
Sex-Specific Associations between Serum IL-16 Levels and Sarcopenia in Older Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Collection and Handling of Serum Samples
2.3. Measurement of Candidate Biomarkers
2.4. Analysis of the Appendicular Skeletal Muscle Mass
2.5. Grip Strength Measurement
2.6. Physical Assessment and Evaluation
2.7. Statistical Analysis
3. Results
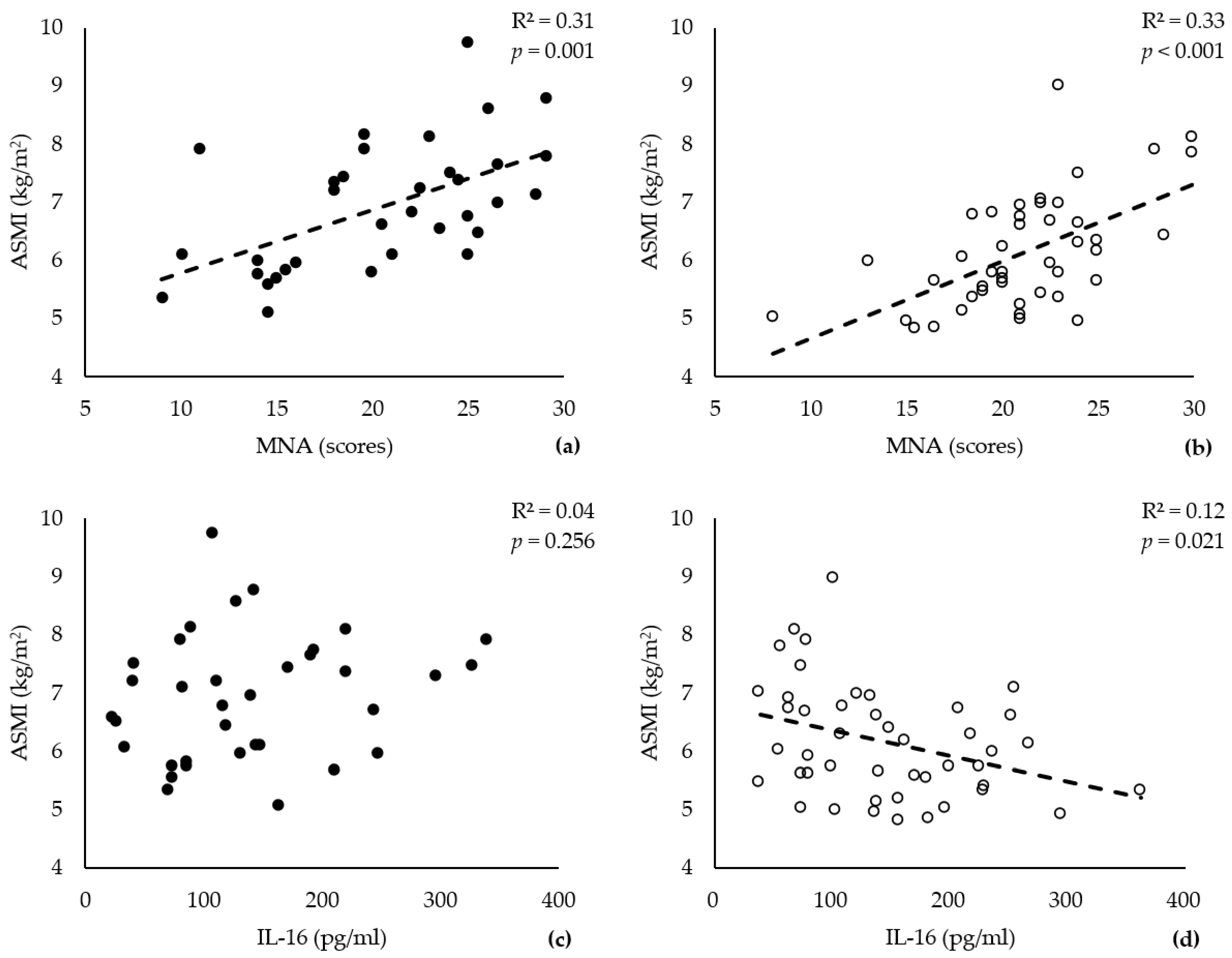
3.1. ASMI and Serum Levels of IL-16 Correlate Exclusively in Older Females
3.2. BFR and IL-16 Are Influencing Factors in Older Female Patients with Sarcopenia
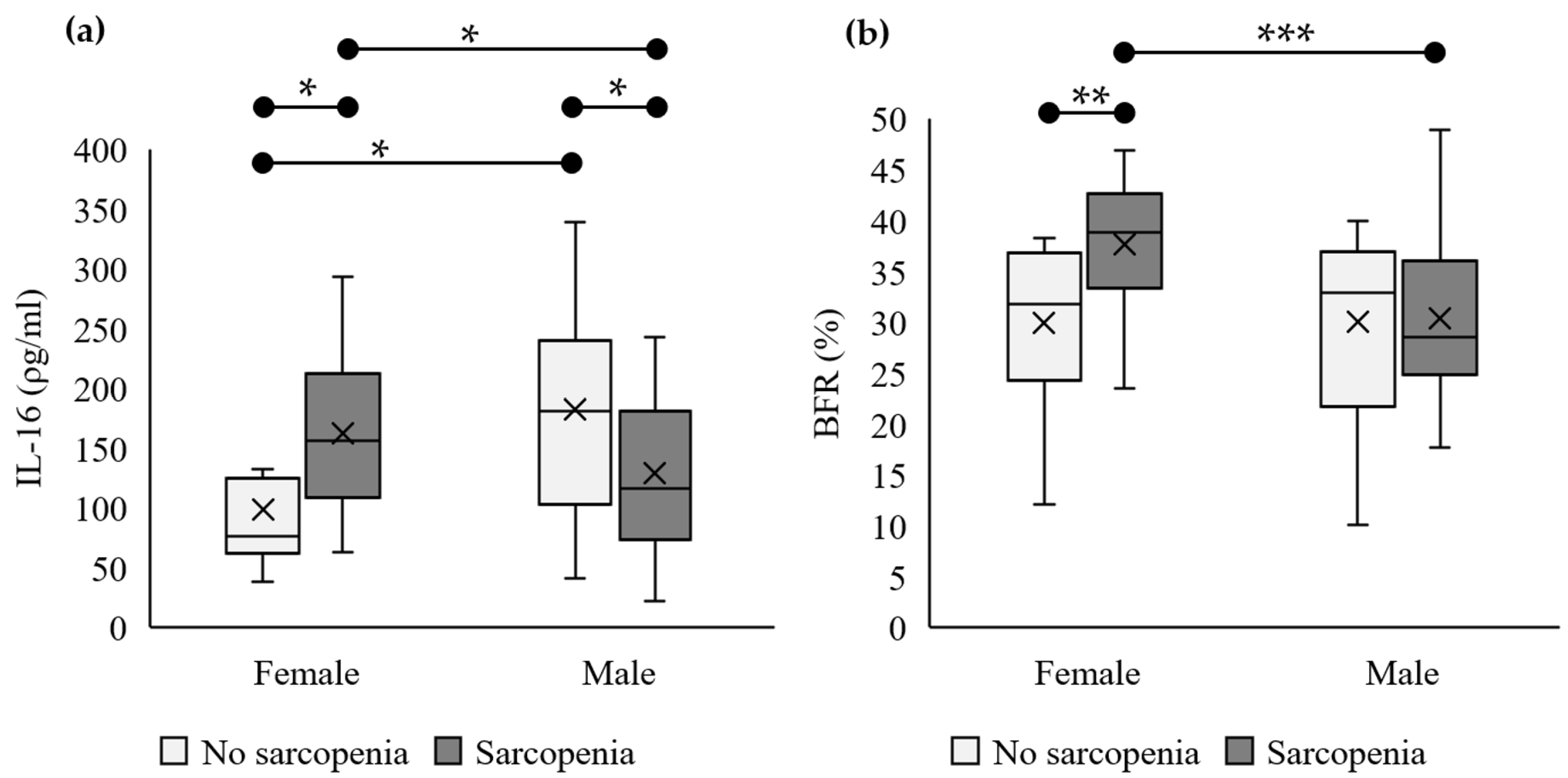
3.3. IL-16 Serum Levels and BFRs Are Significantly Higher in Older Females
3.4. High IL-16 Serum Levels Serve Exclusively as a Risk Factor for Sarcopenia in Older Females
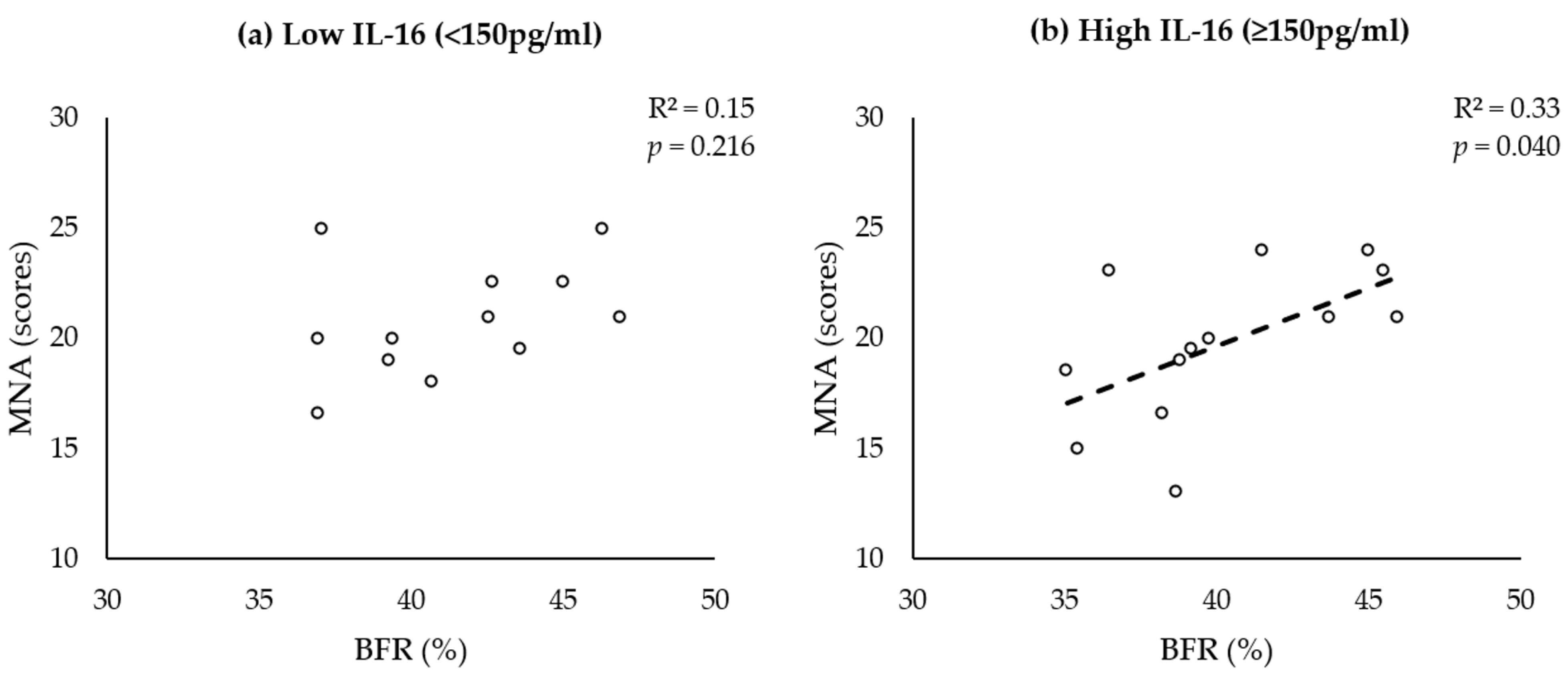
3.5. BFR and MNA Correlate in Women with Sarcopenia with High IL-16 Serum Levels
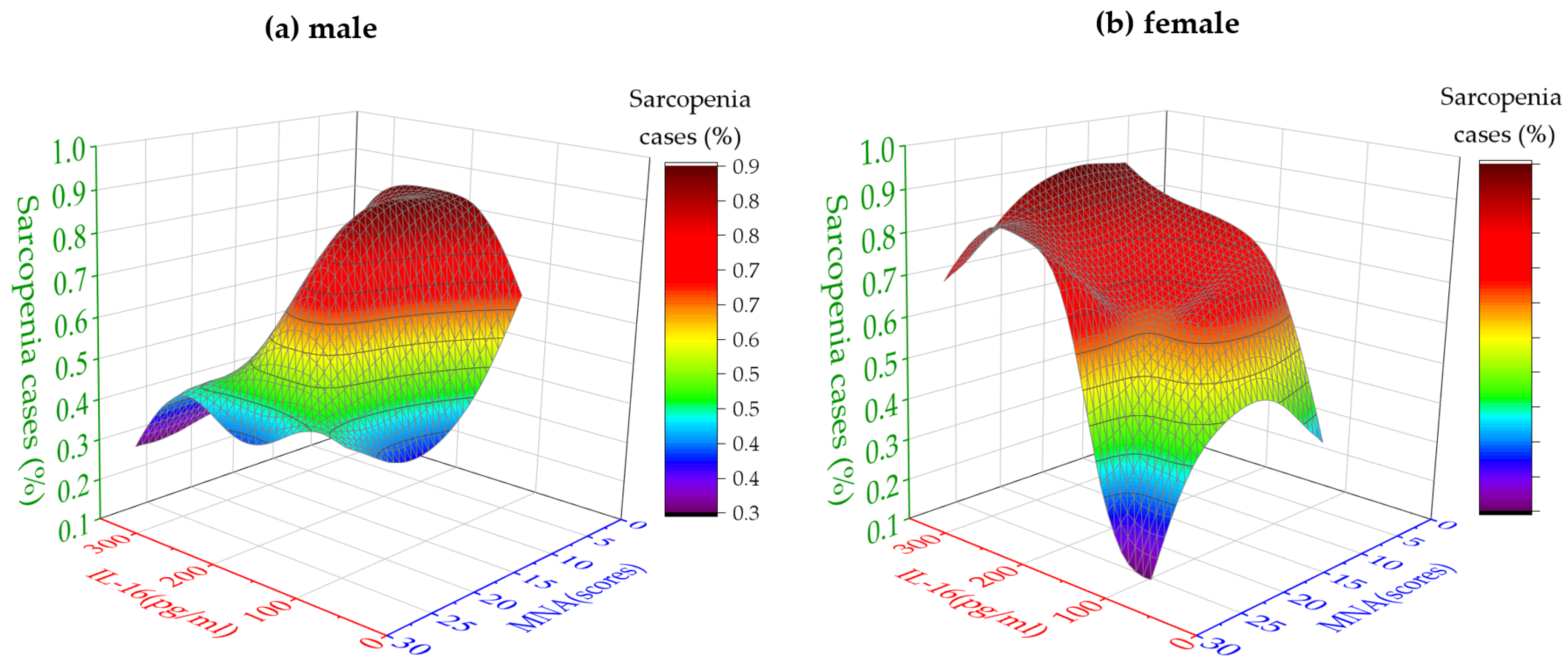
3.6. High IL-16 Serum Levels Are the Primary Factor Influencing the Probability of Sarcopenia in Older Females
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Coletta, G.; Phillips, S.M. An elusive consensus definition of sarcopenia impedes research and clinical treatment: A narrative review. Ageing Res. Rev. 2023, 86, 101883. [Google Scholar] [CrossRef] [PubMed]
- Agostini, D.; Gervasi, M.; Ferrini, F.; Bartolacci, A.; Stranieri, A.; Piccoli, G.; Barbieri, E.; Sestili, P.; Patti, A.; Stocchi, V.; et al. An Integrated Approach to Skeletal Muscle Health in Aging. Nutrients 2023, 15, 1802. [Google Scholar] [CrossRef] [PubMed]
- Li, C.W.; Yu, K.; Shyh-Chang, N.; Li, G.-X.; Jiang, L.-J.; Yu, S.-L.; Xu, L.-Y.; Liu, R.-J.; Guo, Z.-J.; Xie, H.-Y.; et al. Circulating factors associated with sarcopenia during ageing and after intensive lifestyle intervention. J. Cachexia Sarcopenia Muscle 2019, 10, 586–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picca, A.; Calvani, R. Molecular Mechanism and Pathogenesis of Sarcopenia: An Overview. Int. J. Mol. Sci. 2021, 22, 3032. [Google Scholar] [CrossRef]
- Giovannini, S.; Brau, F.; Forino, R.; Berti, A.; D’ignazio, F.; Loreti, C.; Bellieni, A.; D’angelo, E.; Di Caro, F.; Biscotti, L.; et al. Sarcopenia: Diagnosis and Management, State of the Art and Contribution of Ultrasound. J. Clin. Med. 2021, 10, 5552. [Google Scholar] [CrossRef]
- Cesari, M.; Fielding, R.A.; Pahor, M.; Goodpaster, B.; Hellerstein, M.; Van Kan, G.A.; Anker, S.D.; Rutkove, S.; Vrijbloed, J.W.; Isaac, M.; et al. Biomarkers of sarcopenia in clinical trials-recommendations from the International Working Group on Sarcopenia. J. Cachexia Sarcopenia Muscle 2012, 3, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Saeki, C.; Tsubota, A. Influencing Factors and Molecular Pathogenesis of Sarcopenia and Osteosarcopenia in Chronic Liver Disease. Life 2021, 11, 899. [Google Scholar] [CrossRef]
- Xiong, J.; Hu, H.; Kang, W.; Shao, X.; Li, Y.; Jin, P.; Tian, Y. Association of Sarcopenia and Expression of Interleukin-16 in Gastric Cancer Survival. Nutrients 2022, 14, 838. [Google Scholar] [CrossRef]
- Park, S.S.; Kwon, E.S.; Kwon, K.S. Molecular mechanisms and therapeutic interventions in sarcopenia. Osteoporos Sarcopenia 2017, 3, 117–122. [Google Scholar] [CrossRef]
- Lee, J.H.; Jun, H.S. Role of Myokines in Regulating Skeletal Muscle Mass and Function. Front. Physiol. 2019, 10, 42. [Google Scholar] [CrossRef]
- Blaschke, S.; Schulz, H.; Schwarz, G.; Blaschke, V.; Müller, G.A.; Reuss-Borst, M. Interleukin 16 expression in relation to disease activity in rheumatoid arthritis. J. Rheumatol. 2001, 28, 12–21. [Google Scholar]
- Qin, G.; Wei, L.; Jiang, F.; Li, J.; Zhang, B.; Pan, D.; Lu, X. LncRNA NR024118 is downregulated in sepsis and inhibits LPS-induced apoptosis of cardiomyocytes. Mol. Med. Rep. 2021, 23, 434. [Google Scholar] [CrossRef]
- Gao, L.B.; Rao, L.; Wang, Y.-Y.; Liang, W.-B.; Li, C.; Xue, H.; Bin Zhou, B.; Sun, H.; Li, Y.; Lv, M.-L.; et al. The association of interleukin-16 polymorphisms with IL-16 serum levels and risk of colorectal and gastric cancer. Carcinogenesis 2009, 30, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, J.; Bitterman, P.; Basu, S.; Barua, A. Changes in IL-16 Expression in the Ovary during Aging and Its Potential Consequences to Ovarian Pathology. J. Immunol. Res. 2022, 2022, 2870389. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Uriz-Otano, F.; Malafarina, C.; Martinez, J.A.; Zulet, M.A. Effectiveness of nutritional supplementation on sarcopenia and recovery in hip fracture patients. A multi-centre randomized trial. Maturitas 2017, 101, 42–50. [Google Scholar] [CrossRef]
- Zhu, L.Y.; Chan, R.; Kwok, T.; Cheng, K.C.-C.; Ha, A.; Woo, J. Effects of exercise and nutrition supplementation in community-dwelling older Chinese people with sarcopenia: A randomized controlled trial. Age Ageing 2019, 48, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Carbone, L.; Petro, J.L.; Cione, E.; Vargas, S.; Angulo, H.; Forero, D.A.; Odriozola-Martínez, A.; Kreider, R.B.; Bonilla, D.A. Sarcopenia: Etiology, Nutritional Approaches, and miRNAs. Int. J. Mol. Sci. 2021, 22, 9724. [Google Scholar] [CrossRef]
- Misra, D. Sarcopenic obesity: An undefined dilemma. Osteoarthr. Cartil. 2019, 27, 1729–1730. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Busetto, L.; Bauer, J.M.; Bischoff, S.; Boirie, Y.; Cederholm, T.; Cruz-Jentoft, A.J.; Dicker, D.; Frühbeck, G.; Giustina, A.; et al. Critical appraisal of definitions and diagnostic criteria for sarcopenic obesity based on a systematic review. Clin. Nutr. 2020, 39, 2368–2388. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Li, Y.; Ma, L. Sarcopenic Obesity: An Emerging Public Health Problem. Aging Dis. 2022, 13, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Laurentius, T.; Fait, Y.; Müller, A.; Mückter, E.; Bollheimer, L.C.; Nourbakhsh, M. Associations of Serum CXCL12α and CK Levels with Skeletal Muscle Mass in Older Adults. J. Clin. Med. 2023, 12, 3800. [Google Scholar] [CrossRef]
- Della Peruta, C.; Lozanoska-Ochser, B.; Renzini, A.; Moresi, V.; Riera, C.S.; Bouché, M.; Coletti, D. Sex Differences in Inflammation and Muscle Wasting in Aging and Disease. Int. J. Mol. Sci. 2023, 24, 4651. [Google Scholar] [CrossRef] [PubMed]
- Kokura, Y.; Momosaki, R. Rehabilitation Nutrition in Older People. Nutrients 2023, 15, 1893. [Google Scholar] [CrossRef]
- Wen, Z.; Gu, J.; Chen, R.; Wang, Q.; Ding, N.; Meng, L.; Wang, X.; Liu, H.; Sheng, Z.; Zheng, H. Handgrip Strength and Muscle Quality: Results from the National Health and Nutrition Examination Survey Database. J. Clin. Med. 2023, 12, 3184. [Google Scholar] [CrossRef]
- Strand, R.; Kullberg, J.; Ahlström, H.; Lind, L. Relationships between plasma levels and six proinflammatory interleukins and body composition using a new magnetic resonance imaging voxel-based technique. Cytokine X 2021, 3, 100050. [Google Scholar] [CrossRef] [PubMed]
- Lichtenauer, M.; Franz, M.; Fritzenwanger, M.; Figulla, H.-R.; Gerdes, N.; Jung, C. Elevated plasma levels of interleukin-12p40 and interleukin-16 in overweight adolescents. Biomed Res. Int. 2015, 2015, 940910. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male (n = 35) | Female (n = 45) | p | |
|---|---|---|---|
| Age (years) | 80.34 ± 7.05 | 82.31 ± 5.81 | 0.232 |
| ASMI (kg/m2) | 6.93 ± 1.07 | 6.15 ± 0.97 | 0.001 |
| Weight (kg) | 76.27 ± 16.45 | 67.14 ± 13.55 | 0.008 |
| Grip Strength (kg) | 20.64 ± 10.04 | 13.84 ± 5.61 | 0.001 |
| BFR (%) | 30.24 ± 8.00 | 35.93 ± 7.36 | 0.001 |
| MNA (score) | 20.69 ± 5.74 | 21.36 ± 4.36 | 0.782 |
| IL-16 (pg/mL) | 140.19 ± 83.40 | 145.91 ± 76.21 | 0.731 |
| Control Group Male ≥ 7.3 kg/m2 Female ≥ 6.8 kg/m2 (n = 24) | Patient Group Male < 7.3 kg/m2 Female < 6.8 kg/m2 (n = 56) | p | ||
|---|---|---|---|---|
| Sex (F/M) | 10/14 | 35/21 | 0.087 | |
| Age (years) | Male | 77.79 ± 6.67 | 82.05 ± 6.92 | 0.098 |
| Female | 81.80 ± 3.39 | 82.46 ± 6.37 | 0.520 | |
| Weight (kg) | Male | 86.86 ± 12.12 | 69.21 ± 15.29 | 0.001 |
| Female | 74.75 ± 12.29 | 64.97 ± 13.26 | 0.043 | |
| ASMM (kg) | Male | 23.54 ± 3.45 | 17.97 ± 2.82 | <0.001 |
| Female | 20.26 ± 1.99 | 15.54 ± 2.23 | <0.001 | |
| FM (kg) | Male | 26.52 ± 9.21 | 21.88 ± 10.43 | 0.051 |
| Female | 23.14 ± 8.76 | 25.02 ± 8.34 | 0.682 | |
| BFR (%) | Male | 29.98 ± 8.87 | 30.40 ± 7.59 | 0.840 |
| Female | 29.91 ± 8.10 | 37.64 ± 6.24 | 0.002 | |
| MNA (score) | Male | 23.11 ± 5.28 | 19.07 ± 5.56 | 0.039 |
| Female | 25.30 ± 3.74 | 20.23 ± 3.88 | 0.001 | |
| IL-16 (pg/mL) | Male | 181.99 ± 92.25 | 112.33 ± 65.24 | 0.013 |
| Female | 98.77 ± 62.20 | 159.38 ± 75.18 | 0.025 |
| OR | 95% CI | p | |||
|---|---|---|---|---|---|
| MNA (score) | Male | Low (scores < 17) | 9.75 | 1.07–88.87 | 0.028 |
| High (scores ≥ 17) | |||||
| Female | Low (scores < 17) | 4.63 | 0.24–89.42 | 0.312 | |
| High (scores ≥ 17) | |||||
| BFR (%) | Male | Obesity (≥25.0%) | 1.28 | 0.28–5.93 | 0.752 |
| Normal (<25.0%) | |||||
| Female | Obesity (≥35.0%) | 5.83 | 1.25–27.17 | 0.027 | |
| Normal (<35.0%) | |||||
| IL-16 (pg/mL) | Male | High (≥150 pg/mL) | 0.18 | 0.04–0.81 | 0.031 |
| Low (<150 pg/mL) | |||||
| Female | High (≥150 pg/mL) | 9.53 | 1.09–83.44 | 0.029 | |
| Low (<150 pg/mL) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Laurentius, T.; Fait, Y.; Müller, A.; Mückter, E.; Hao, D.; Bollheimer, L.C.; Nourbakhsh, M. Sex-Specific Associations between Serum IL-16 Levels and Sarcopenia in Older Adults. Nutrients 2023, 15, 3529. https://doi.org/10.3390/nu15163529
Chen Z, Laurentius T, Fait Y, Müller A, Mückter E, Hao D, Bollheimer LC, Nourbakhsh M. Sex-Specific Associations between Serum IL-16 Levels and Sarcopenia in Older Adults. Nutrients. 2023; 15(16):3529. https://doi.org/10.3390/nu15163529
Chicago/Turabian StyleChen, Ze, Thea Laurentius, Yvonne Fait, Aline Müller, Eva Mückter, Dandan Hao, Leo Cornelius Bollheimer, and Mahtab Nourbakhsh. 2023. "Sex-Specific Associations between Serum IL-16 Levels and Sarcopenia in Older Adults" Nutrients 15, no. 16: 3529. https://doi.org/10.3390/nu15163529