
Adherence to the DASH Diet and Risk of Hypertension: A Systematic Review and Meta-Analysis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias in Individual Studies
2.6. Data Synthesis
2.7. Quality of the Evidence
3. Results
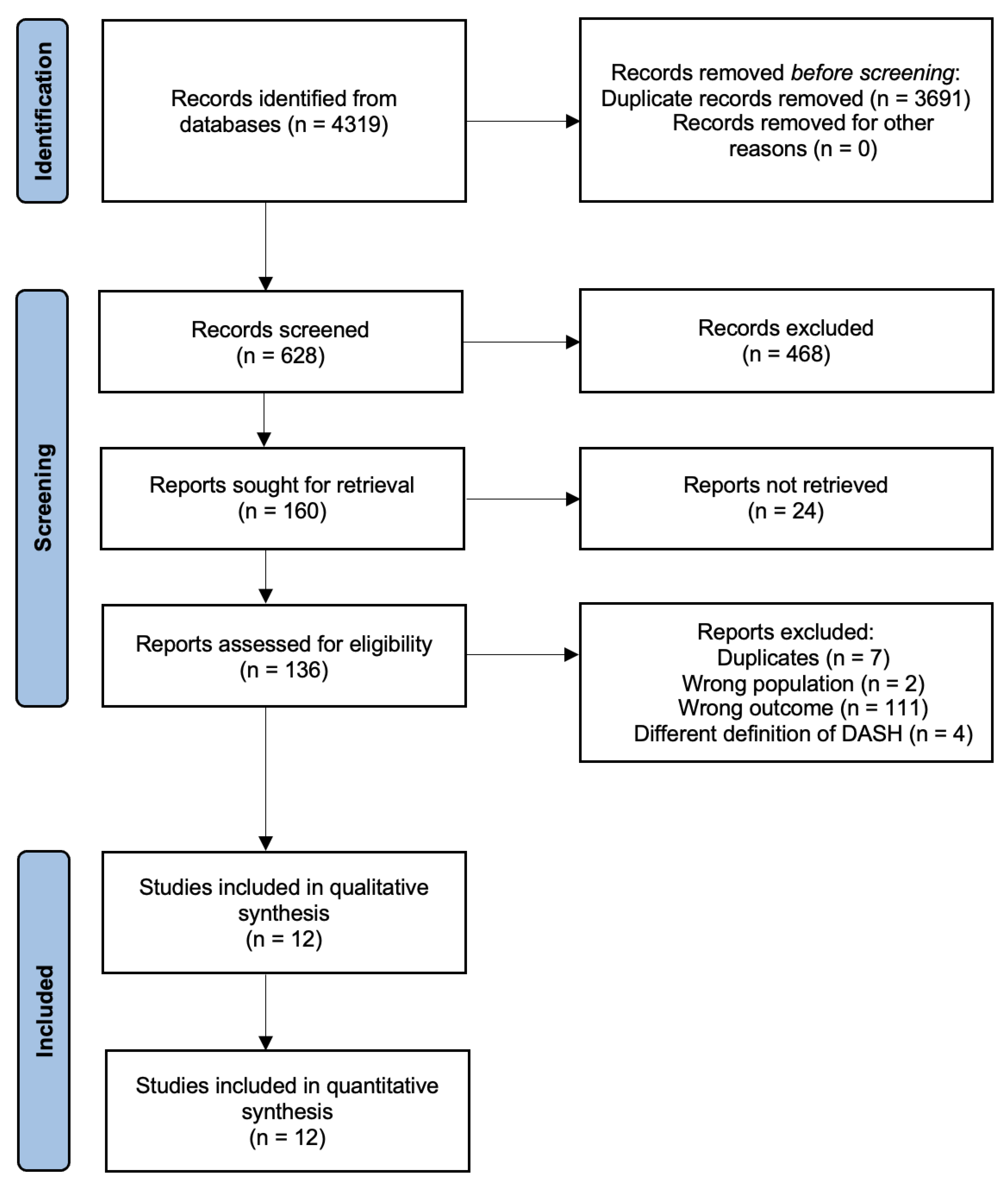
3.1. Database Search and Study Characteristics
3.2. Definitions of the DASH Diet
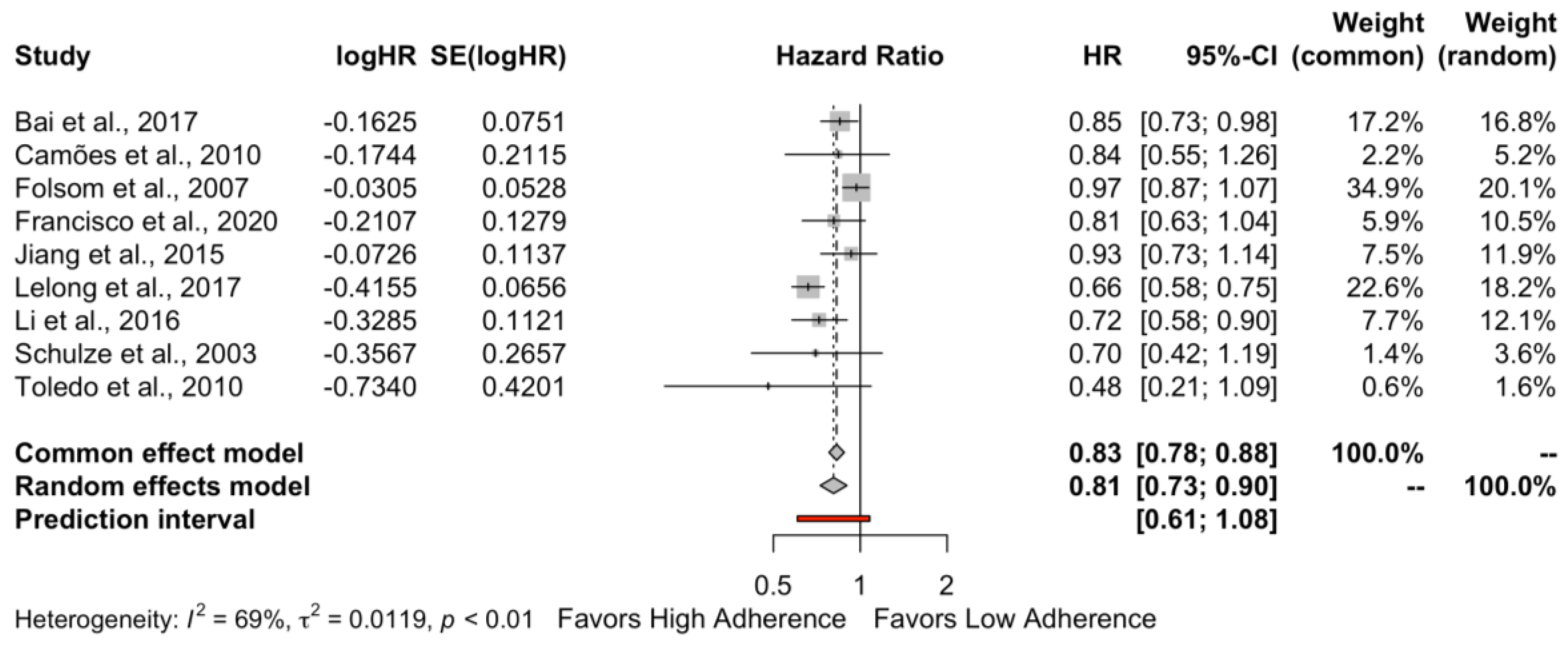
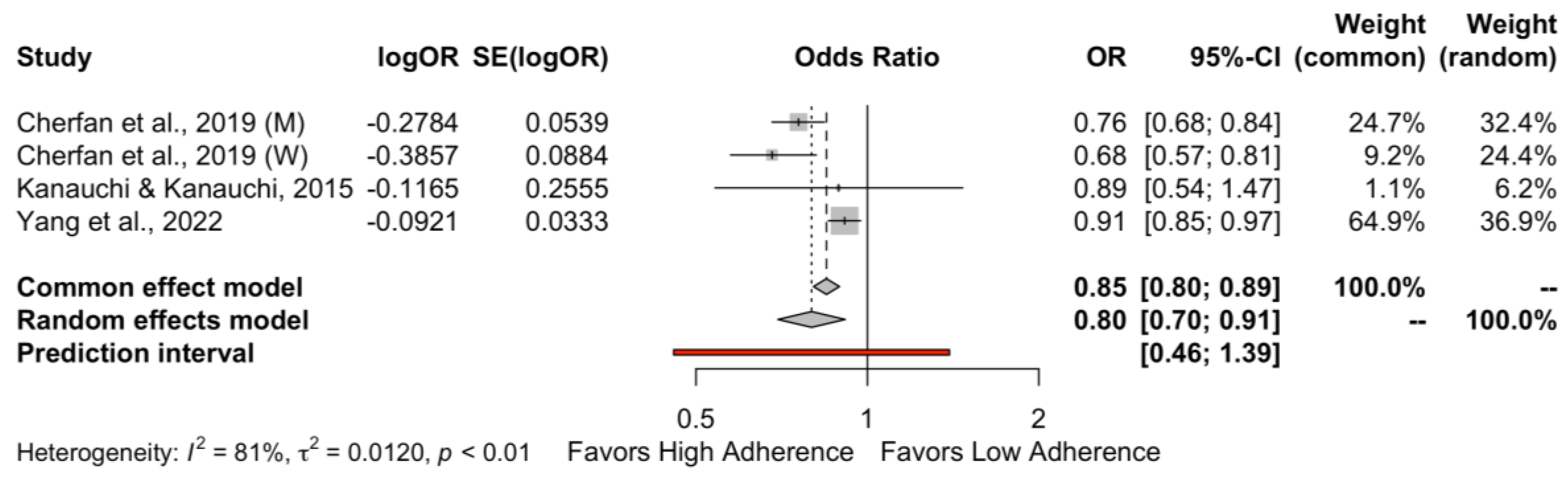
3.3. Outcome of Interest
3.4. Risk of Bias Assessment
3.5. Subgroup and Sensitivity Analysis
3.6. Certainty of the Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide Trends in Hypertension Prevalence and Progress in Treatment and Control from 1990 to 2019: A Pooled Analysis of 1201 Population-Representative Studies with 104 Million Participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- World Health Organization. Hypertension. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 27 November 2022).
- Heidenreich, P.A.; Trogdon, J.G.; Khavjou, O.A.; Butler, J.; Dracup, K.; Ezekowitz, M.D.; Finkelstein, E.A.; Hong, Y.; Johnston, S.C.; Khera, A.; et al. Forecasting the Future of Cardiovascular Disease in the United States. Circulation 2011, 123, 933–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, S. Hypertension Management in 2030: A Kaleidoscopic View. J. Hum. Hypertens. 2020, 35, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Mensah, G.A. Epidemiology and Global Burden of Hypertension. In The ESC Textbook of Cardiovascular Medicine; Came, J., Lüscher, T., Maurer, G., Serruys, P., Eds.; Oxford University Press: Oxford, UK, 2018; pp. 290–297. [Google Scholar]
- Carey, R.M.; Muntner, P.; Bosworth, H.B.; Whelton, P.K. Prevention and Control of Hypertension: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1278. [Google Scholar] [CrossRef] [PubMed]
- Campbell, N.R.C.; Whelton, P.K.; Orias, M.; Wainford, R.D.; Cappuccio, F.P.; Ide, N.; Neal, B.; Cohn, J.; Cobb, L.K.; Webster, J.; et al. 2022 World Hypertension League, Resolve to Save Lives and International Society of Hypertension Dietary Sodium (Salt) Global Call to Action. J. Hum. Hypertens. 2022, 37, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial HypertensionThe Task Force for the Management of Arterial Hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, E13–E115. [Google Scholar] [CrossRef]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary Approaches to Stop Hypertension (DASH) Diet and Blood Pressure Reduction in Adults with and without Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2020, 11, 1150. [Google Scholar] [CrossRef]
- Günther, A.L.B.; Liese, A.D.; Bell, R.A.; Dabelea, D.; Lawrence, J.M.; Rodriguez, B.L.; Standiford, D.A.; Mayer-Davis, E.J. Association between the Dietary Approaches to Hypertension Diet and Hypertension in Youth with Diabetes Mellitus. Hypertension 2009, 53, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Hassani Zadeh, S.; Salehi-Abargouei, A.; Mirzaei, M.; Nadjarzadeh, A.; Hosseinzadeh, M. The Association between Dietary Approaches to Stop Hypertension Diet and Mediterranean Diet with Metabolic Syndrome in a Large Sample of Iranian Adults: YaHS and TAMYZ Studies. Food Sci. Nutr. 2021, 9, 3932. [Google Scholar] [CrossRef]
- Jiang, J.; Liu, M.; Troy, L.M.; Bangalore, S.; Hayes, R.B.; Parekh, N. Concordance with DASH Diet and Blood Pressure Change: Results from the Framingham Offspring Study (1991–2008). J. Hypertens. 2015, 33, 2223–2230. [Google Scholar] [CrossRef]
- Kanauchi, M.; Kanauchi, K. Diet Quality and Adherence to a Healthy Diet in Japanese Male Workers with Untreated Hypertension. BMJ Open 2015, 5, e008404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-Analysis of Observational Studies in Epidemiology: A Proposal for Reporting. Meta-Analysis of Observational Studies in Epidemiology (MOOSE) Group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Veroniki, A.A.; Jackson, D.; Viechtbauer, W.; Bender, R.; Bowden, J.; Knapp, G.; Kuss, O.; Higgins, J.P.; Langan, D.; Salanti, G. Methods to Estimate the Between-Study Variance and Its Uncertainty in Meta-Analysis. Res. Synth. Methods 2016, 7, 55–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; ISBN 9781119536604. [Google Scholar]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for Routinely Presenting Prediction Intervals in Meta-Analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; Sterne, J.A.C.; Higgins, J.P.T.; Egger, M. Investigating and Dealing with Publication Bias and Other Reporting Biases in Meta-Analyses of Health Research: A Review. Res. Synth. Methods 2021, 12, 248–259. [Google Scholar] [CrossRef] [PubMed]
- Bai, G.; Zhang, J.; Zhao, C.; Wang, Y.; Qi, Y.; Zhang, B. Adherence to a Healthy Lifestyle and a DASH-Style Diet and Risk of Hypertension in Chinese Individuals. Hypertens. Res. 2017, 40, 196–202. [Google Scholar] [CrossRef]
- Camões, M.; Oliveira, A.; Pereira, M.; Severo, M.; Lopes, C. Role of Physical Activity and Diet in Incidence of Hypertension: A Population-Based Study in Portuguese Adults. Eur. J. Clin. Nutr. 2010, 64, 1441–1449. [Google Scholar] [CrossRef] [Green Version]
- Folsom, A.R.; Parker, E.D.; Harnack, L.J. Degree of Concordance with DASH Diet Guidelines and Incidence of Hypertension and Fatal Cardiovascular Disease. Am. J. Hypertens. 2007, 20, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francisco, S.C.; Araújo, L.F.; Griep, R.H.; Chor, D.; Molina, M.D.C.B.; Mil, J.G.; Bensenor, I.M.; Matos, S.M.A.; Barreto, S.M.; Giatti, L. Adherence to the Dietary Approaches to Stop Hypertension (DASH) and Hypertension Risk: Results of the Longitudinal Study of Adult Health (ELSA-Brasil). Br. J. Nutr. 2020, 123, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Lelong, H.; Blacher, J.; Baudry, J.; Adriouch, S.; Galan, P.; Fezeu, L.; Hercberg, S.; Kesse-Guyot, E. Individual and Combined Effects of Dietary Factors on Risk of Incident Hypertension Prospective Analysis from the Nutrinet-Santé Cohort. Hypertension 2017, 70, 712–720. [Google Scholar] [CrossRef]
- Li, S.; Zhu, Y.; Chavarro, J.E.; Bao, W.; Tobias, D.K.; Ley, S.H.; Forman, J.P.; Liu, A.; Mills, J.; Bowers, K.; et al. Healthful Dietary Patterns and the Risk of Hypertension among Women with a History of Gestational Diabetes Mellitus: A Prospective Cohort Study. Hypertension 2016, 67, 1157–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze, M.B.; Hoffmann, K.; Kroke, A.; Boeing, H. Risk of Hypertension among Women in the EPIC-Potsdam Study: Comparison of Relative Risk Estimates for Exploratory and Hypothesis-Oriented Dietary Patterns. Am. J. Epidemiol. 2003, 158, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Toledo, E.; Carmona-Torre, F.D.A.; Alonso, A.; Puchau, B.; Zulet, M.A.; Martinez, J.A.; Martinez-Gonzalez, M.A. Hypothesis-Oriented Food Patterns and Incidence of Hypertension: 6-Year Follow-up of the SUN (Seguimiento Universidad de Navarra) Prospective Cohort. Public Health Nutr. 2010, 13, 338–349. [Google Scholar] [CrossRef] [Green Version]
- Cherfan, M.; Vallée, A.; Kab, S.; Salameh, P.; Goldberg, M.; Zins, M.; Blacher, J. Unhealthy Behavior and Risk of Hypertension: The CONSTANCES Population-Based Cohort. J. Hypertens. 2019, 37, 2180–2189. [Google Scholar] [CrossRef]
- Yang, Y.; Yu, D.; Piao, W.; Huang, K.; Zhao, L. Nutrient-Derived Beneficial for Blood Pressure Dietary Pattern Associated with Hypertension Prevention and Control: Based on China Nutrition and Health Surveillance 2015–2017. Nutrients 2022, 14, 3108. [Google Scholar] [CrossRef]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-Style Diet and Risk of Coronary Heart Disease and Stroke in Women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Bazzano, L.A.; Green, T.; Harrison, T.N.; Reynolds, K. Dietary Approaches to Prevent Hypertension. Curr. Hypertens. Rep. 2013, 15, 694–702. [Google Scholar] [CrossRef] [Green Version]
- Tarray, R.; Saleem, S.; Afroze, D.; Yousuf, I.; Gulnar, A.; Laway, B.; Verma, S. Role of Insulin Resistance in Essential Hypertension. Cardiovasc. Endocrinol. 2014, 3, 129–133. [Google Scholar] [CrossRef]
- Rodrigo, R.; González, J.; Paoletto, F. The Role of Oxidative Stress in the Pathophysiology of Hypertension. Hypertens. Res. 2011, 34, 431–440. [Google Scholar] [CrossRef] [Green Version]
- Guyton, A.C. Blood Pressure Control—Special Role of the Kidneys and Body Fluids. Science 1991, 252, 1813–1816. [Google Scholar] [CrossRef] [PubMed]
- Boegehold, M.A. The Effect of High Salt Intake on Endothelial Function: Reduced Vascular Nitric Oxide in the Absence of Hypertension. J. Vasc. Res. 2013, 50, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.S. Arterial Stiffness and Hypertension. Clin. Hypertens. 2018, 24, 17. [Google Scholar] [CrossRef]
- Salvi, P.; Giannattasio, C.; Parati, G. High Sodium Intake and Arterial Stiffness. J. Hypertens. 2018, 36, 754–758. [Google Scholar] [CrossRef]
- García-Ortiz, L.; Recio-Rodríguez, J.I.; Rodríguez-Sánchez, E.; Patino-Alonso, M.C.; Agudo-Conde, C.; Rodríguez-Martín, C.; Castaño-Sánchez, C.; Runkle, I.; Gómez-Marcos, M.A. Sodium and Potassium Intake Present a J-Shaped Relationship with Arterial Stiffness and Carotid Intima-Media Thickness. Atherosclerosis 2012, 225, 497–503. [Google Scholar] [CrossRef]
- Kaess, B.M.; Rong, J.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S.; Mitchell, G.F. Aortic Stiffness, Blood Pressure Progression, and Incident Hypertension. JAMA 2012, 308, 875–881. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, A.N.; Akerman, A.; Kumar, S.; Diep Pham, H.T.; Coffey, S.; Mann, J. Dietary Fibre in Hypertension and Cardiovascular Disease Management: Systematic Review and Meta-Analyses. BMC Med. 2022, 20, 139. [Google Scholar] [CrossRef]
- Fu, L.; Zhang, G.; Qian, S.; Zhang, Q.; Tan, M. Associations between Dietary Fiber Intake and Cardiovascular Risk Factors: An Umbrella Review of Meta-Analyses of Randomized Controlled Trials. Front. Nutr. 2022, 9, 972399. [Google Scholar] [CrossRef]
- Aljuraiban, G.S.; Griep, L.M.O.; Chan, Q.; Daviglus, M.L.; Stamler, J.; van Horn, L.; Elliott, P.; Frost, G.S. Total, Insoluble and Soluble Dietary Fibre Intake in Relation to Blood Pressure: The INTERMAP Study. Br. J. Nutr. 2015, 114, 1480–1486. [Google Scholar] [CrossRef] [Green Version]
- Guo, R.; Li, N.; Yang, R.; Liao, X.Y.; Zhang, Y.; Zhu, B.F.; Zhao, Q.; Chen, L.; Zhang, Y.G.; Lei, Y. Effects of the Modified DASH Diet on Adults with Elevated Blood Pressure or Hypertension: A Systematic Review and Meta-Analysis. Front Nutr. 2021, 8, 621. [Google Scholar] [CrossRef]
- Soltani, S.; Arablou, T.; Jayedi, A.; Salehi-Abargouei, A. Adherence to the Dietary Approaches to Stop Hypertension (DASH) Diet in Relation to All-Cause and Cause-Specific Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Nutr. J. 2020, 19, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murad, M.H.; Asi, N.; Alsawas, M.; Alahdab, F. New Evidence Pyramid. BMJ Evid. Based Med. 2016, 21, 125–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramachandran, K.M.; Tsokos, C.P. Mathematical Statistics with Applications in R, 3rd ed.; Ramachandran, K.M., Tsokos, C.P., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; ISBN 9780128178157. [Google Scholar]
- Dobrescu, A.I.; Nussbaumer-Streit, B.; Klerings, I.; Wagner, G.; Persad, E.; Sommer, I.; Herkner, H.; Gartlehner, G. Restricting Evidence Syntheses of Interventions to English-Language Publications Is a Viable Methodological Shortcut for Most Medical Topics: A Systematic Review. J. Clin. Epidemiol. 2021, 137, 209–217. [Google Scholar] [CrossRef]
- Morrison, A.; Polisena, J.; Husereau, D.; Moulton, K.; Clark, M.; Fiander, M.; Mierzwinski-Urban, M.; Clifford, T.; Hutton, B.; Rabb, D. The Effect of English-Language Restriction on Systematic Review-Based Meta-Analyses: A Systematic Review of Empirical Studies. Int. J. Technol. Assess. Health Care 2012, 28, 138–144. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study ID, Country | Study Design, Effect Size | Population | No of Participants (Low/High Adherence) | Mean Age ± SD | Exclusion Criteria | DASH Assessment Tool | Hypertension Diagnosis |
|---|---|---|---|---|---|---|---|
| Bai et al., 2017 [22], China | Longitudinal-cohort, HR | Chinese adults | - | 42 ± 9.3 | Younger than 18 years old, missing average SBP or DBP, identified hypertension, antihypertensive medication, existing diagnosis of diabetes, myocardial infarction, or apoplexy | DASH diet score Fung et al. (2008) [32] | SBP ≥ 140 or DBP ≥ 90 or antihypertensive medication use |
| Camões et al., 2010 [23], Portugal | Longitudinal cohort study, HR | Portuguese adults, resident in Porto and at risk of developing hypertension | 246/256 | - | Age < 39 years old, missing information on BP measurements, hypertensive | Developed DASH diet score | SBP ≥ 140 or DBP ≥ 90 or antihypertensive medication use |
| Cherfan et al., 2019 [30], France | Cross-sectional analysis, OR | Adult workers or retired | 3709/29,342 | - | BMI < 18 kg/m2 | Constructed DASH diet score according to Fung et al. (2008) [32] | SBP ≥ 140 or DBP ≥ 90 or antihypertensive medication use |
| Folsom et al., 2007 [24], U.S. | Cohort study, HR | Adult women | 5017/4041 | 61.0 | History of physician-diagnosed hypertension, heart attack, angina, heart disease, diabetes, more than 29 blank items on FFQ, EI < 500 kcal or >5000 kcal, missing covariates | Developed DASH diet index score | Self-report of hypertension |
| Francisco et al., 2020 [25], Brazil | Longitudinal cohort study, HR | Adults active or retired civil services of higher research institutions located in Brazil | 4987/645 | 49.9 ± 8.3 | Hypertension, antihypertensive drugs, CVD, changed dietary habits in the last 6 months, self-reported their race/skin color as Asian, Brazilian indigenous, missing information on BP values | Dash diet score calculated by National Institutes of Health, National Heart Lung and Blood Institute | SBP ≥ 140 or DBP ≥ 90 or antihypertensive medication use |
| Jiang et al., 2015 [14], U.S. | Longitudinal cohort study, HR | U.S. adults | 585/331 | 52.5 ± 9.4 | Medication, no SBP or DPB recorded at follow-ups, no valid FFQ, missing information for hypertension medication | Developed DASH diet score using score by Folsom et al. (2007) [24] | SBP ≥ 140 or DBP ≥ 90 or antihypertensive medication use |
| Kanauchi et al., 2015 [15], Japan | Cross-sectional, OR | Male workers | - | 45.3 ± 6.9 | Diabetes, CKD, implausibly low or high estimated EI, missing information | Developed DASH diet score | SBP ≥ 140 or DBP ≥ 90 |
| Lelong et al., 2017 [26], France | Prospective cohort study, HR | Adults internet user volunteer | 19,967/ 19,323 | 41.9 ± 14.0 | Energy under reporters, with < 3 24 h valid recalls, prevalent hypertension, cancer, diabetes mellitus, and cardiovascular disease, pregnant women, missing or invalid data on health status, anthropometric measurements, or physical activity | DASH diet score Fung et al. (2008) [32] | Self-report of hypertension |
| Li et al., 2016 [27], U.S. | Cohort study, HR | Adult women | 706/747 | 36.5 ± 4.3 | History of cardiovascular disease, cancer, multiple gestations or pregnancies lasting <6 months, history of GDM, history of hypertension beforethe diagnosis of GDM or with missing data on post-pregnancy diet | DASH diet score Fung et al. (2008) [32] | Self-report of hypertension |
| Schulze et al., 2003 [28], Germany | Cohort study, HR | Women in the EPIC-Potsdam Study | - | - | Previous diagnosis of hypertension, antihypertensive medication within a 4-week period prior to the baseline examination, missing information on dietary intake, estimated basal metabolic rate, physical activity, lifestyle characteristics, and anthropometric measurements; current pregnancy or breastfeeding, outlying total energy intake, with no follow-up, possible hypertension for whom we did not have completed verification, prevalent or secondary hypertension | DASH diet score based on hypothesis-oriented pattern variable | - |
| Toledo et al., 2010 [29], Spain | Prospective cohort study, HR | University graduates | 6487/158 | 36.3 ± 11.0 | Self-reported prevalent hypertension with extreme total EI, prevalent CVD at baseline | Developed DASH diet score | Self-report of hypertension |
| Yang et al., 2022 [31], China | Cross-sectional, OR | Chinese adults | 12,298/11,862 | - | Incomplete dietary information, incomplete basic information, incomplete physical examination and laboratory test, implausible dietary EI < 500 kcal/d or >5000 kcal/d, and pre-diagnosed coronary heart disease or stroke | Developed DASH diet score | SBP ≥ 140 or DBP ≥ 90 or antihypertensive medication use |
| First Author, Year | BMI | SBP | DBP | Physical Activity | Smoking Status | Sodium Intake | Potassium Intake (Low/High) |
|---|---|---|---|---|---|---|---|
| (Low/High) | (Low/High) | (Low/High) | (Low/High) | (Low/High) | (Low/High) | ||
| Bai et al., 2017 [22] | NA | NA | NA | NA | NA | NA | NA |
| Camões et al., 2010 [23] | NA | NA | NA | NA | NA | NA | NA |
| Cherfan et al., 2019 [30] | NA | NA | NA | NA | NA | NA | NA |
| Folsom et al., 2007 [24] | 26.3/25.3 | NA | NA | 16.0%/40.0% | Current smokers = 22.0%/10.0% | 2124.0 mg/d 2275.0 mg/d | 1147.0 mg/d 1437.0 mg/d |
| high PA * | |||||||
| Francisco et al., 2020 [25] | 25.8 ± 4.2/ 24.9 ± 3.8 | 114.5 ± 11.5/ 114.5 ± 11.8 | 72.7 ± 8.1/ 71.4 ± 8.2 | Low Adherence: | Low Adherence: | 4.6 ± 14.4 g/d 3.5 ± 3.0 g/d | 3982.0 ± 1607.0 mg/d 5260.0 ± 1664.0 mg/d |
| Light = 78.6% | Non-smoker = 58.8% | ||||||
| Moderate = 14.1% | Former smoker = 25.8% | ||||||
| High = 7.3% | Smoker = 15.4% | ||||||
| High Adherence: | High Adherence: | ||||||
| Light = 62.8% | Non-smoker = 65.3% | ||||||
| Moderate = 24.8% | Former smoker = 25.4% | ||||||
| High = 12.4% | Smoker = 9.3% | ||||||
| Jiang et al., 2015 [14] | 27.1/25.9 | 121.1/119.0 | 73.6/71.7 | 35.6/34.6 PAI | 35.9%/7.0% | 1145.3/1000 kcal | 1468.3/1000 kcal |
| 1146.0/1000 kcal | 1902.2/1000 kcal | ||||||
| Kanauchi et al., 2015 [15] | NA | NA | NA | NA | NA | NA | NA |
| Lelong et al., 2017 [26] | 23.8 ± 4.7/ 22.7 ± 3.6 | NA | NA | Low Adherence: | Low Adherence: | 2907.0 ± 958.0 mg/d 2454.0 ± 857.0 mg/d | 2623.0 ± 726.0 mg/d 3409.0 ± 884.0 mg/d |
| Low = 31.3% | Never = 48.7% | ||||||
| Moderate = 41.5% | Former Smoker = 25.8% | ||||||
| High = 27.3% | Current = 25.6% | ||||||
| High Adherence: | High Adherence: | ||||||
| Low = 17.4% | Never = 53.6% | ||||||
| Moderate = 44.1% | Former Smoker = 36.1% | ||||||
| High = 38.5% | Current = 38.5% | ||||||
| Li et al., 2016 [27] | 26.8 ± 6.5/ 25.8 ± 5.7 | NA | NA | 12.5 ± 18.3/21.9 ± 25.4 | 19.0%/7.0% | NA | NA |
| (MET × h/week) | |||||||
| Schulze et al., 2003 [28] | NA | NA | NA | NA | NA | NA | NA |
| Toledo et al., 2010 [29] | 23.0 ± 3.0/ 23.0 ± 3.0 | NA | NA | 23.5 ± 20.9/32.1 ± 30.1 (MET × h/week) | Low Adherence: | 3.4 ± 2.2 g/d 3.1 ± 1.5 g/d | 4.3 ± 1.2 g/d 7.3 ± 2.1 g/d |
| Current = 25.0% | |||||||
| Ex-smokers = 25.0% | |||||||
| High Adherence: | |||||||
| Current = 15.0% | |||||||
| Ex-smokers = 30.0% | |||||||
| Yang et al., 2022 [31] | NA | NA | NA | NA | NA | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Theodoridis, X.; Chourdakis, M.; Chrysoula, L.; Chroni, V.; Tirodimos, I.; Dipla, K.; Gkaliagkousi, E.; Triantafyllou, A. Adherence to the DASH Diet and Risk of Hypertension: A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 3261. https://doi.org/10.3390/nu15143261
Theodoridis X, Chourdakis M, Chrysoula L, Chroni V, Tirodimos I, Dipla K, Gkaliagkousi E, Triantafyllou A. Adherence to the DASH Diet and Risk of Hypertension: A Systematic Review and Meta-Analysis. Nutrients. 2023; 15(14):3261. https://doi.org/10.3390/nu15143261
Chicago/Turabian StyleTheodoridis, Xenophon, Michail Chourdakis, Lydia Chrysoula, Violeta Chroni, Ilias Tirodimos, Konstantina Dipla, Eugenia Gkaliagkousi, and Areti Triantafyllou. 2023. "Adherence to the DASH Diet and Risk of Hypertension: A Systematic Review and Meta-Analysis" Nutrients 15, no. 14: 3261. https://doi.org/10.3390/nu15143261