
Association of Fried Food Intake with Gastric Cancer Risk: A Systemic Review and Meta-Analysis of Case–Control Studies

Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Literature Selection Criteria
2.2. Literature Evaluation and Selection
2.3. Risk of Bias Assessment of the Research Literature
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
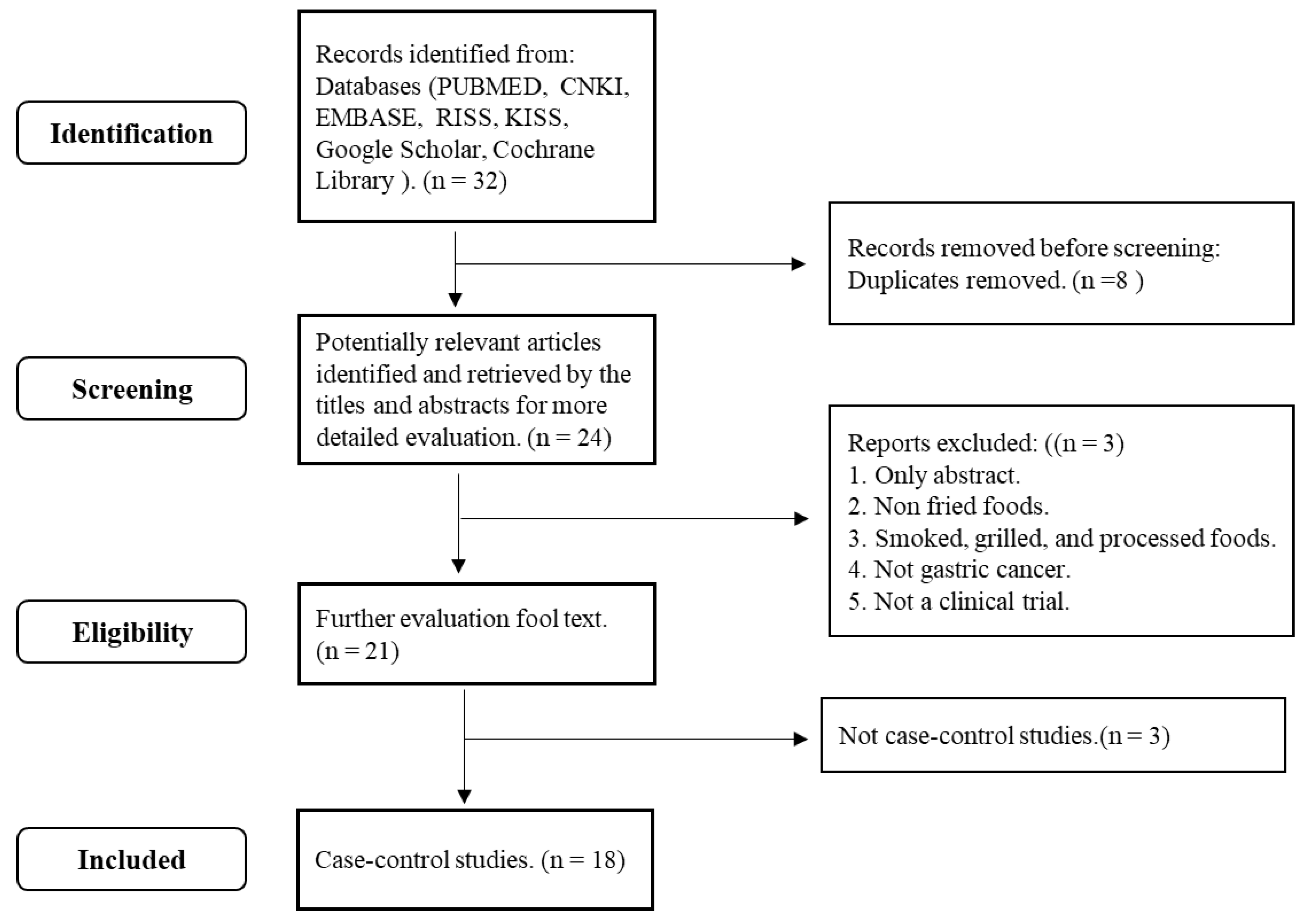
3.1. Study Selection and Study Characteristics
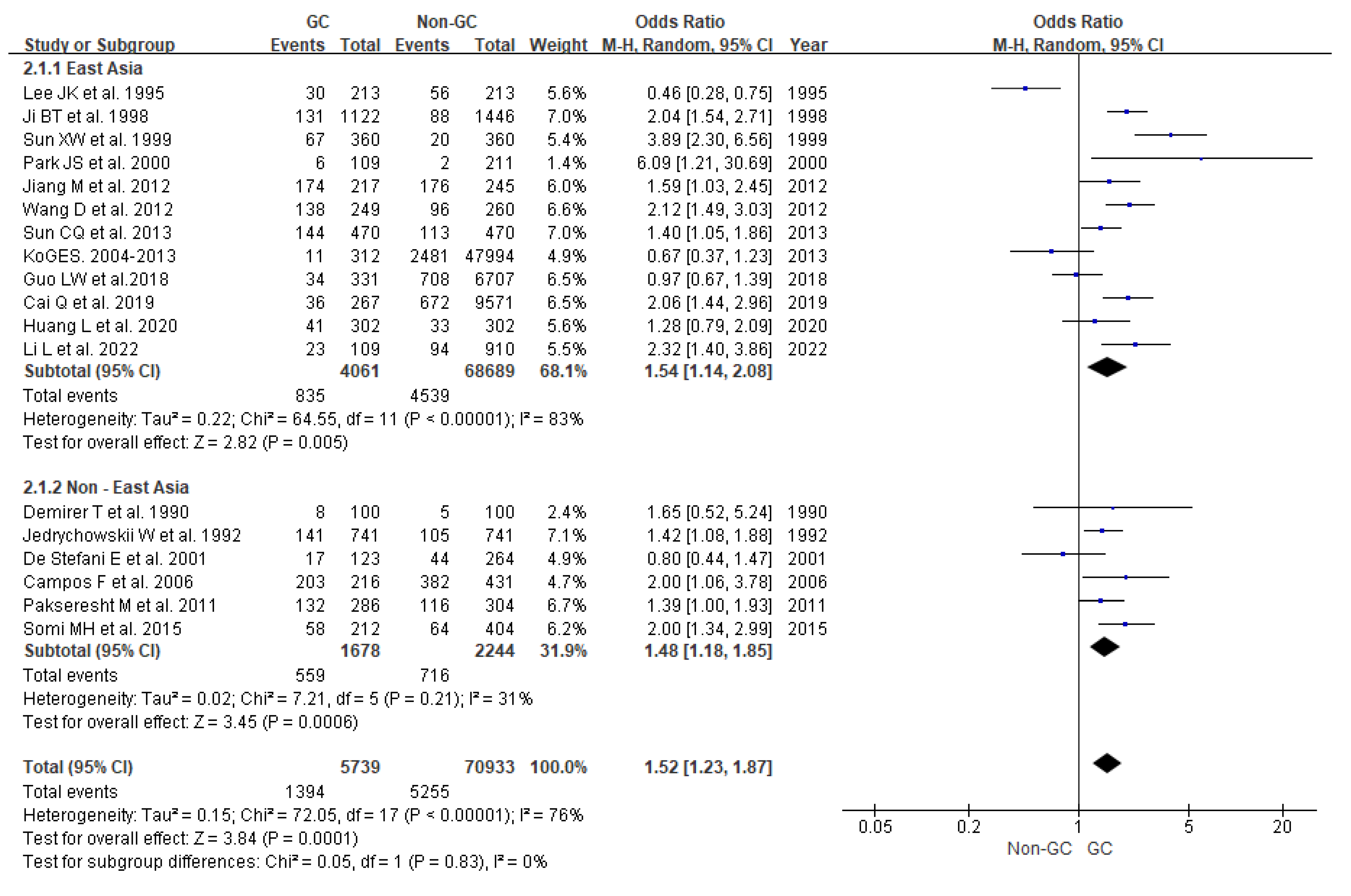
3.2. High Intake of Fried Foods
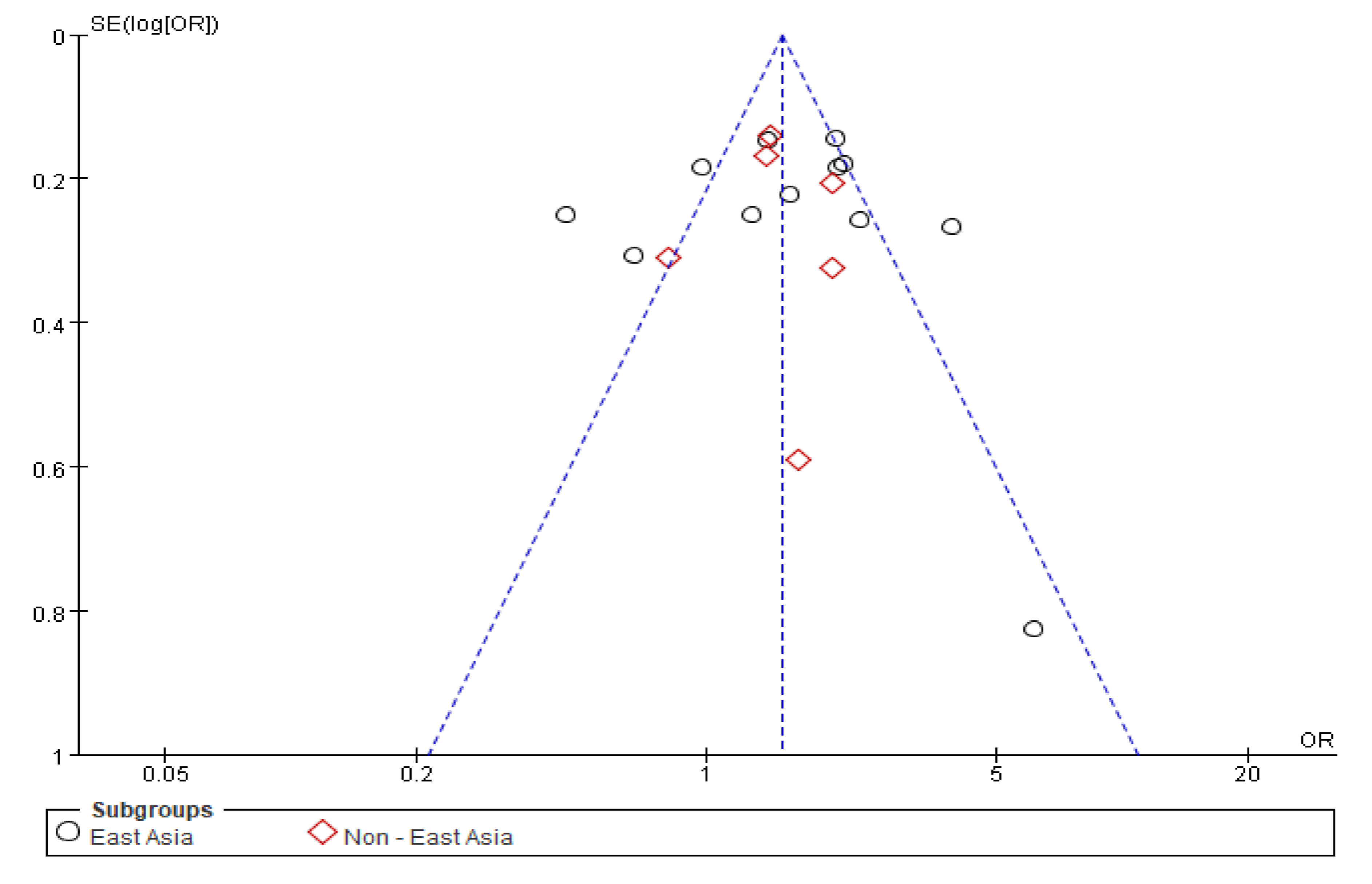
3.3. Sensitivity Analysis and Publication Bias
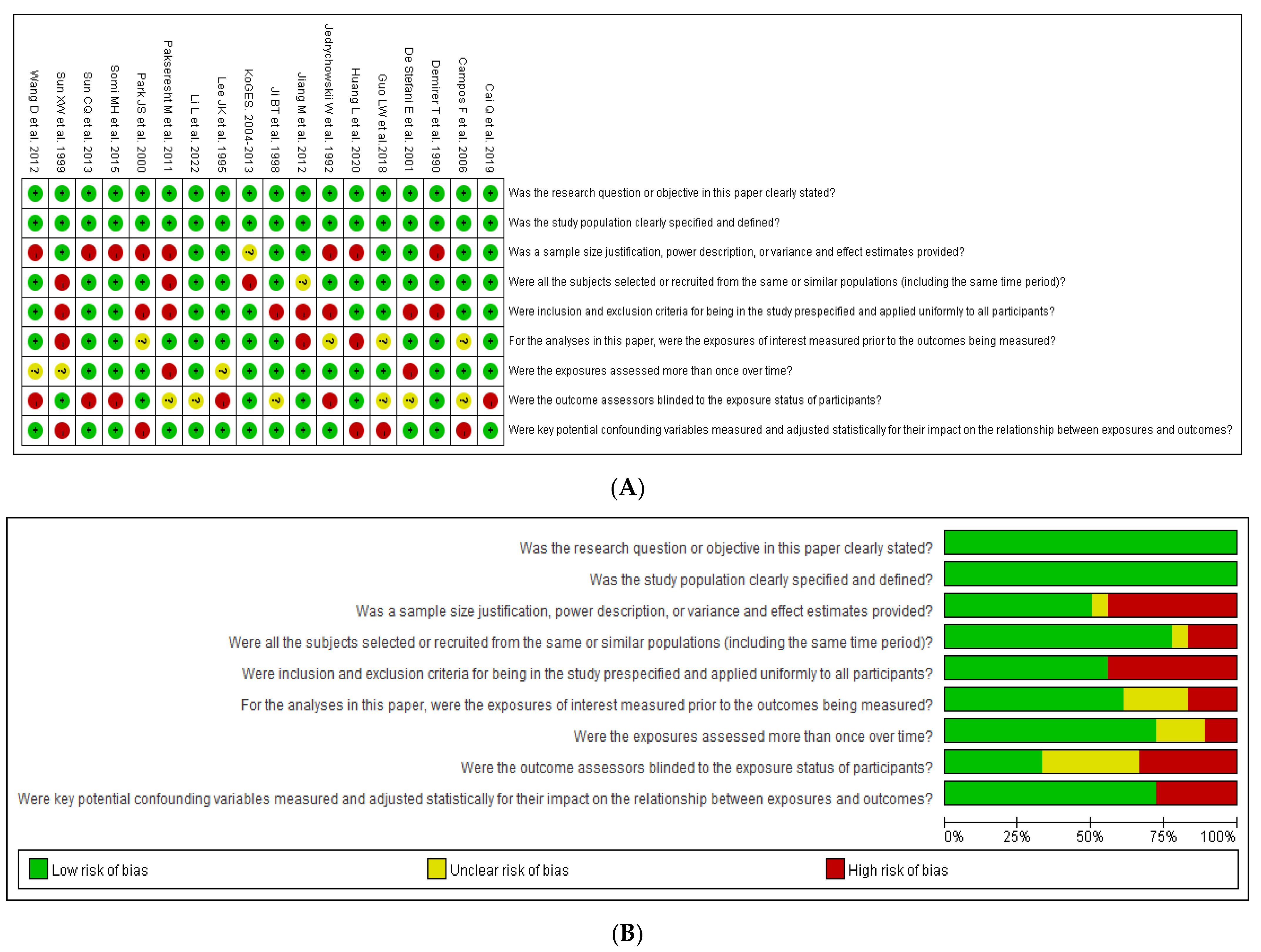
3.4. Risk of Bias (ROB)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Kim, I.H.; Kang, S.J.; Choi, M.; Kim, B.H.; Eom, B.W.; Kim, B.J.; Min, B.H.; Choi, C.I.; Shin, C.M.; et al. Korean Practice Guidelines for Gastric Cancer 2022: An Evidence-based, Multidisciplinary Approach. J. Gastric Cancer 2023, 23, 3–106. [Google Scholar] [CrossRef]
- World Cancer Research Fund International; American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective: A Summary of the Third Expert Report; World Cancer Research Fund International: London, UK, 2018. [Google Scholar]
- Dobarganes, C.; Márquez-Ruiz, G. Possible adverse effects of frying with vegetable oils. Br. J. Nutr. 2015, 113 (Suppl. S2), S49–S57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uzcudun, A.E.; Retolaza, I.R.; Fernández, P.B.; Sánchez Hernández, J.J.; Grande, A.G.; García, A.G.; Olivar, L.M.; De Diego Sastre, I.; Barón, M.G.; Bouzas, J.G. Nutrition and pharyngeal cancer: Results from a case-control study in Spain. Head Neck 2002, 24, 830–840. [Google Scholar] [CrossRef]
- Bosetti, C.; Talamini, R.; Levi, F.; Negri, E.; Franceschi, S.; Airoldi, L.; La Vecchia, C. Fried foods: A risk factor for laryngeal cancer? Br. J. Cancer 2002, 87, 1230–1233. [Google Scholar] [CrossRef]
- Jain, K.; Sreenivas, V.; Velpandian, T.; Kapil, U.; Garg, P.K. Risk factors for gallbladder cancer: A case-control study. Int. J. Cancer 2013, 132, 1660–1666. [Google Scholar] [CrossRef]
- Li, M.L.; Lin, J.; Hou, J.G.; Xu, L.; Cui, X.G.; Xu, X.X.; Yu, Y.W.; Han, X.; Wang, G.M.; Guo, J.M.; et al. Environmental and psycho-social factors related to prostate cancer risk in the Chinese population: A case-control study. Biomed. Environ. Sci. 2014, 27, 707–717. [Google Scholar]
- Zhong, G.C.; Zhu, Q.; Gong, J.P.; Cai, D.; Hu, J.J.; Dai, X.; Gong, J.H. Fried food consumption and the risk of pancreatic cancer: A large prospective multicenter study. Front. Nutr. 2022, 9, 889303. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.K.; Park, B.J.; Yoo, K.Y.; Ahn, Y.O. Dietary factors and stomach cancer: A case-control study in Korea. Int. J. Epidemiol. 1995, 24, 33–41. [Google Scholar] [CrossRef]
- Campos, F.; Carrasquilla, G.; Koriyama, C.; Serra, M.; Carrascal, E.; Itoh, T.; Nomoto, M.; Akiba, S. Risk factors of gastric cancer-specific for tumor location and histology in Cali, Colombia. World J. Gastroenterol. 2006, 12, 5772–5779. [Google Scholar] [CrossRef]
- Cai, Q.; Zhu, C.; Yuan, Y.; Feng, Q.; Feng, Y.; Hao, Y.; Li, J.; Zhang, K.; Ye, G.; Ye, L.; et al. Development and validation of a prediction rule for estimating gastric cancer risk in the Chinese high-risk population: A nationwide multicentre study. Gut 2019, 68, 1576–1587. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-S.; Kim, H.; Song, Y.-J.; Yun, H.-Y.; Kang, J.-W.; Kim, Y.-D.; Nan, H.-M. Effects of environmental carcinogens and genetic polymorphisms of CYP2E1 and NAT2 on gastric carcinogenesis. J. Korean Surg. Sci. 2000, 59, 488–499. [Google Scholar]
- Sun, C.Q.; Chang, Y.B.; Cui, L.L.; Chen, J.J.; Sun, N.; Zhang, W.J.; Jia, X.C.; Tian, Y.; Dai, L.P. A population-based case-control study on risk factors for gastric cardia cancer in rural areas of Linzhou. Asian Pac. J. Cancer Prev. 2013, 14, 2897–2901. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Zhou, J.; Wang, T.; Li, X.; Li, S.; Chen, S.; Ma, G.; Li, J.; Zhang, X. Polymorphisms in MSH2 gene and risk of gastric cancer, and interactions with lifestyle factors in a Chinese population. Cancer Epidemiol. 2012, 36, e171–e176. [Google Scholar] [CrossRef] [PubMed]
- Demirer, T.; Icli, F.; Uzunalimoglu, O.; Kucuk, O. Diet and stomach cancer incidence. A case-control study in Turkey. Cancer 1990, 65, 2344–2348. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.; Boeing, H.; Popiela, T.; Wahrendorf, J.; Tobiasz-Adamczyk, B.; Kulig, J. Dietary practices in households as risk factors for stomach cancer: A familial study in Poland. Eur. J. Cancer Prev. 1992, 1, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Ji, B.T.; Chow, W.H.; Yang, G.; McLaughlin, J.K.; Zheng, W.; Shu, X.O.; Jin, F.; Gao, R.N.; Gao, Y.T.; Fraumeni, J.F., Jr. Dietary habits and stomach cancer in Shanghai, China. Int. J. Cancer 1998, 76, 659–664. [Google Scholar] [CrossRef]
- Sun, X.W.; Dai, X.D.; Jia, L.Y.; Bai, S.Y.; Sun, J.J. Study on the relationship between dietary factors and gastric cancer. J. Practical Oncol. 1999, 13, 16–19. [Google Scholar]
- Guo, L.W.; Liu, S.Z.; Zhang, M.; Chen, Q.; Zhang, S.K.; Sun, X.B. Multivariate analysis of the association between consumption of fried food and gastric cancer and precancerous lesions. Chin. J. Prev. Med. 2018, 52, 170–174. [Google Scholar]
- Jiang, M.; Li, T.; Yang, L.P.; Wang, Y.; Yin, J.; Wu, Y.Z.; Wang, J.H. A case- control study on the relationship between diet habit and gastric cancer in Xian, China. Modern Oncol. 2012, 20, 1453–1456. [Google Scholar]
- De Stefani, E.; Ronco, A.; Brennan, P.; Boffetta, P. Meat consumption and risk of stomach cancer in Uruguay: A case-control study. Nutr. Cancer 2001, 40, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Chen, L.; Gui, Z.X.; Liu, S.; Wei, Z.J.; Xu, A.M. Preventable lifestyle and eating habits associated with gastric adenocarcinoma: A case-control study. J. Cancer 2020, 11, 1231–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Ni, J.; Sun, S.; Zha, X.; Li, R.; He, C. Clinical applicability of a new scoring system for population-based screening and risk factors of gastric cancer in the Wannan region. BMC Gastroenterol. 2022, 22, 306. [Google Scholar] [CrossRef] [PubMed]
- Pakseresht, M.; Forman, D.; Malekzadeh, R.; Yazdanbod, A.; West, R.M.; Greenwood, D.C.; Crabtree, J.E.; Cade, J.E. Dietary habits and gastric cancer risk in north-west Iran. Cancer Causes Control 2011, 22, 725–736. [Google Scholar] [CrossRef] [Green Version]
- Somi, M.H.; Mousavi, S.M.; Naghashi, S.; Faramarzi, E.; Jafarabadi, M.A.; Ghojazade, M.; Majdi, A.; Naseri Alavi, S.A. Is there any relationship between food habits in the last two decades and gastric cancer in North-Western Iran? Asian Pac. J. Cancer Prev. 2015, 16, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Song, S.S. Genetic Factors, Dietary Intake, and the Risk of Gastric Cancer: Genetic Interaction between Polygenetic Risk Scores for Gastric Cancer and Dietary Intake; Hoseo University: Cheonan, Republic of Korea, 2023. [Google Scholar]
- Cochrane committee. Cochrane Review Manager (RevMan) 5.3. 2008, p. 373. Available online: https://training.cochrane.org/online-learning/core-software/revman (accessed on 27 June 2023).
- Higgins, J.P.; Thompson, S.G.; Spiegelhalter, D.J. A re-evaluation of random-effects meta-analysis. J. R. Stat. Soc. Ser. A Stat. Soc. 2009, 172, 137–159. [Google Scholar] [CrossRef] [Green Version]
- Savović, J.; Weeks, L.; Sterne, J.A.; Turner, L.; Altman, D.G.; Moher, D.; Higgins, J.P. Evaluation of the Cochrane Collaboration’s tool for assessing the risk of bias in randomized trials: Focus groups, online survey, proposed recommendations and their implementation. Syst. Rev. 2014, 3, 37. [Google Scholar] [CrossRef] [Green Version]
- Lang, N.P.; Butler, M.A.; Massengill, J.; Lawson, M.; Stotts, R.C.; Hauer-Jensen, M.; Kadlubar, F.F. Rapid metabolic phenotypes for acetyltransferase and cytochrome P4501A2 and putative exposure to food-borne heterocyclic amines increase the risk for colorectal cancer or polyps. Cancer Epidemiol. Biomark. Prev. 1994, 3, 675–682. [Google Scholar]
- Sinha, R.; Chow, W.H.; Kulldorff, M.; Denobile, J.; Butler, J.; Garcia-Closas, M.; Weil, R.; Hoover, R.N.; Rothman, N. Well-done, grilled red meat increases the risk of colorectal adenomas. Cancer Res. 1999, 59, 4320–4324. [Google Scholar]
- Salehzadeh, H.; Maleki, A.; Rezaee, R.; Shahmoradi, B.; Ponnet, K. The nitrate content of fresh and cooked vegetables and their health-related risks. PLoS ONE 2020, 15, e0227551. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Chetty, A.A. Nitrate-N determination in leafy vegetables: Study of the effects of cooking and freezing. Food Chem. 2008, 106, 772–780. [Google Scholar] [CrossRef]
- Mihoubi, A.; Alloui-Lombarkia, O.; Zitouni, B. Food consumption and digestive cancers in the province of batna. Ann. Food Sci. Technol. 2018, 19, 135–145. [Google Scholar]
- Augustsson, K.; Skog, K.; Jägerstad, M.; Dickman, P.W.; Steineck, G. Dietary heterocyclic amines and cancer of the colon, rectum, bladder, and kidney: A population-based study. Lancet 1999, 353, 703–707. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary acrylamide intake is not associated with gastrointestinal cancer risk. J. Nutr. 2008, 138, 2229–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelucchi, C.; Franceschi, S.; Levi, F.; Trichopoulos, D.; Bosetti, C.; Negri, E.; La Vecchia, C. Fried potatoes and human cancer. Int. J. Cancer 2003, 105, 558–560. [Google Scholar] [CrossRef]
- Chang, W.K.; Kim, D.J.; Kim, H.Y.; Kim, J.H.; Kim, J.B.; Park, C.K.; Yoo, J.Y.; Kim, H.J.; Kim, M.K.; Choi, B.Y.; et al. A case-control study on the risk factors of Helicobacter pylori infection in Korea. J. Prev. Med. Public. Health 2000, 36, 137–147. [Google Scholar]
- Yan, S.; Li, B.; Bai, Z.Z.; Wu, J.Q.; Xie, D.W.; Ma, Y.C.; Ma, X.X.; Zhao, J.H.; Guo, X.J. Clinical epidemiology of gastric cancer in Hehuang valley of China: A 10-year epidemiological study of gastric cancer. World J. Gastroenterol. 2014, 20, 10486–10494. [Google Scholar] [CrossRef]
- Lim, S.L.; Canavarro, C.; Zaw, M.H.; Zhu, F.; Loke, W.C.; Chan, Y.H.; Yeoh, K.G. Irregular Meal Timing Is Associated with Helicobacter pylori Infection and Gastritis. ISRN Nutr. 2013, 2013, 714970. [Google Scholar] [CrossRef] [Green Version]
- Duan, F.; Song, C.; Shi, J.; Wang, P.; Ye, H.; Dai, L.; Zhang, J.; Wang, K. Identification and epidemiological evaluation of gastric cancer risk factors: Based on a field synopsis and meta-analysis in Chinese population. Aging 2021, 13, 21451–21469. [Google Scholar] [CrossRef]



 Low risk of bias;
Low risk of bias;  Uncertain risk of bias;
Uncertain risk of bias;  High risk of bias.
Low risk of bias; Uncertain risk of bias; High risk of bias.
High risk of bias.
Low risk of bias; Uncertain risk of bias; High risk of bias.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, (Year), Country Ref. No | Region, Study Design | Study Period (Years) | Population, Age | Inclusion Criteria (Exclusion Criteria Indicated) | Dietary Assessment |
|---|---|---|---|---|---|
| Demirer et al. (1990) Turkey [17] | Ankara, Turkey Case–control (Hospital-based) | 1987–1988 (0.3) | 100 cases and 100 controls (matched age, sex, patients; 29–78, healthy; 28–73) | Histologically proven adenocarcinoma of gastric cancer (cases) and same hospitals with no cancer or gastrointestinal disease (controls) | Frequency of consumption of specific food items past 15 years |
| Jedrychowski et al. (1992) Poland [18] | Poland Case–control (Hospital-based) | 1986–1990 (5) | 741 cases (histologically confirmed adenocarcinoma) and 741 controls (patients admitted to the surgical ward) <75 years | Not stated | Structured questionnaire |
| Lee et al. (1995) Korea [11] | Seoul, Korea Case–control (Hospital-based) | 1990–1991 (1.3) | 213 cases (histologically confirmed) and 213 matched (age, sex) controls 25–64 years, ≥65 years | Not diagnosed within 6 months preceding interview, aged >70, with other coexisting chronic systemic diseases affecting dietary patterns or communication problems, non-adenocarcinoma, recurrent cancers (cases), and hospitalized patients (controls) | Semiquantitative food frequency questionnaire with 64 food items, 3 years prior to the interview |
| Ji et al. (1998) China [19] | Shanghai, China Case–control (Population-based) | 1988–1989 (1) | 1124 cases and 1451 matched (age, sex) controls (randomly selected among Shanghai residents) 20–69 years | Not stated | Comprehensive food frequency questionnaire, 74 items assessing usual food intake 10 years before diagnosis |
| Sun et al. (1999) China [20] | Haerbin, China Case–control (Hospital-based) | 1990–1996 (6.11) | 360 cases and 360 healthy controls Average age: 57.94 years and 57.44 years | Not stated | Interview survey |
| Park et al. (2000) Korea [14] | Chungcheong province, Korea Case–control (Hospital-based) | Not stated | 109 cases and 211 controls (matched age and sex) | Same hospitals without cancer | Direct interview with a structured questionnaire |
| De Stefani et al. (2001) Uruguay [23] | Montevideo, Uruguay Case–control (Hospital-based) | 1997–1999 (2) | 123 cases and 282 controls (patients with nonneoplastic diseases) 30–89 years | All newly diagnosed and histologically verified (cases) and same hospitals as the cases, not excessively ill patients (controls) | FFQ 64 items assessing intake 5 years before the onset of symptoms or interview |
| KoGES (2004–2013) Korea [28] | City-Cohort Korea Case–control (Hospital-based) | 2004–2013 (9) | n = 48,306 312 cases and 47,994 controls ≥40 years | Without any history of cancer or disease of the digestive system | Semiquantitative food frequency questionnaire (SQFFQ) 106 items |
| Campos et al. (2006) Colombia [12] | Cali, Colombia Case–control (Hospital-based) | 2000–2002 (2) | 216 cases and 431 controls (noncancer patients matching in age, gender, and hospital) 49–75 years | Without recurrent GC, lived in Valle del Cauca for fewer than five years (cases) and malignant diseases, gastric illnesses, lived in Valle del Cauca for fewer than 5 years, severe clinical conditions, diagnosed with GC 15 years before (controls) | FFQ |
| Pakseresht, et al. (2011) Iran [26] | North-west Iran resided in Ardabil for over 20 years Case–control (Population-based) | 2005–2007 (2) | 286 cases and 304 noncancer controls ≥40 years | Without other malignancies (case) | QFFQ 117 items, assessing usual diet over the last year or 1 year before the diagnosis |
| Wang et al. (2012) China [16] | Jiangsu Province China Case–control (Population-based) | 2004 (1) | 249 cases and 260 healthy controls of the same geographic origins 57.6 ± 9.2 years | Without a history of other cancers or chronic diseases caused by dietary intake or communication problems (cases) | Semiquantitative food frequency table, last 10 years |
| Jiang et al. (2012) China [22] | Xian, China Permanent Resident (≥20 years) Case–control (Hospital-based) | 2007–2010 (2.6) | 217 cases and 245 healthy controls <45 years 45–64 years ≥65 years | Not stated | Epidemiological questionnaire |
| Sun et al. (2013) China [15] | Rural Areas of Linzhou, China Case–control (Population-based) | 2005–2007 (2) | 470 cases (newly diagnosed) and 470 healthy controls (matched age, sex) 40–69 years | Without any disease of the digestive system, living in the nearby Linzhou for more than 10 years (case) | Face-to-face interviews with a uniform questionnaire one year before the diagnosis |
| Somi et al. (2015) Iran [27] | East Azerbaijan of Iran Case–control (Hospital-based) | 2009–2011 (2) | 212 cases (21–84 years, Residents of East Azarbaijan for more than 20 years), 404 controls (cancer-free patients) 61.17 ± 11.72 years | Without other malignancies and a history of cancer, family history of cancer, and other gastrointestinal diseases (case) | Structured questionnaire, over the past two decades |
| Guo et al. (2018) China [21] | Henan Province, China Case–control (Population-based) | 2005–2013 (8) | Endoscopic screening objects (n = 82,367) 331 cases and 6707 matched healthy controls 40–69 years Average age: (53.46 ± 8.07) | Inclusion: participating in the upper gastrointestinal cancer screening project for the first time; Exclusion: participants with missing pathological or endoscopic diagnosis information | Questionnaire |
| Cai et al. (2019) China [13] | China Cohort Case–control (Hospital-based) | 2015–2017 (1.8) | Individuals with a high risk prior to gastroscopy (n = 14,929) 267 cases and 9571 controls 40–80 years | Exclusion: previous gastric operations, H. pylori eradication, taking H2 blockers or proton pump inhibitors in the past 2 weeks, a disorder of renal function, pregnancy, a history of any type of cancer, and a gastroscopy examination within 1 year | Pre-validated self-reported questionnaire |
| Huang et al. (2020) China [24] | Anhui, China Case–control (Hospital-based) | 2016–2018 (2) | 302 cases and 302 matched healthy controls Average 60 ± 11 and 59 ± 11 years | Without other malignancies, benign gastric diseases, dementia, severe dysfunction of organs, severe systematic unfitness, or first-degree relative having gastric cancer (cases) | Frequency score (FS) |
| Li et al. (2022) China [25] | Wannan, China Cohort Case–control (Hospital-based) | 2019–2021 (2.5) | Prospectively enrolled asymptomatic participants (n = 25,194) 109 cases and 910 controls ≥40 years | Exclusion: taking H2 blockers or proton pump inhibitors in the past 2 weeks, H. pylori eradication, pregnant or lactating, chemotherapy or radiotherapy, mental symptoms, or other severe systemic diseases | Questionnaire survey |
| First Author, (Year), Country Ref. No | Sex | Types of Fried Foods or Cooking Methods | Fried Foods: High and Low Case/Control | Types of Gastric Cancer | Comparison (High vs. Low) | Adjusted OR, RR (95% CI) | Adjusted Covariates | Author’s Conclusion |
|---|---|---|---|---|---|---|---|---|
| Demirer et al. (1990) Turkey [17] | M/F | Fried (potatoes, meat, fish) | High: 8 (100)/ 5 (100) Low: 92 (100)/ 95 (100) | GC | Three to four times a week; Daily vs. No consumption; Rare consumption; Once or twice a month; Once or twice a week | not significant | Age, sex, blood group, Residential area | No difference in fried food consumption between the cases and controls |
| Jedrychowski et al. (1992) Poland [18] | M/F | Fried meat (usually served at home) | High: 141 (741)/ 105 (741) Low: 600 (741)/ 636 (741) | GC | Fried vs. No | RR 2.06 (1.48–2.87) | Age, sex, education, occupation of the index person, and residency | Fried or stewed food was associated with a significantly higher risk for GC compared to boiling |
| Lee et al. (1995) Korea [11] | M/F | Fried (meat, fish) | High: 30 (213)/ 56 (213) Low: 183 (213)/ 157 (213) | GC | High, vs. Intermediate Low | 0.4 (0 2–0.8) 0.8 (0.5–1.3) 1.0 (p < 0.001) | Age, sex, education, economic status, and residence areas | Frying (fried meat, fish) was associated with a decreased GC risk |
| Ji et al. (1998) China [19] | M/F | Fried food | High: 131 (1122)/88 (1446) Low: 991 (1122)/ 1358 (1446) | Overall GC (Cardia, Distal) | Frequently Sometimes vs. Occasionally | 2.3 (1.6–3.2) 1.1 (0.9–1.4) 1.0 (p = 0.0001) | Age, sex, income, education, smoking, and alcohol drinking | Risks for both cardia and non-cardia tumors increased by 2-fold with frequent consumption of fried foods |
| Sun et al. (1999) China [20] | M/F | Fried food | High: 67 (360)/ 20 (360) Low: 293 (360)/ 340 (360) | GC | Frequently vs. Occasionally; Do not eat; Rarely eat | 1.20 (0.67–2.16) 3.02 (1.41–6.47) 1.00 1.31 (0.73–1.77) | Age, sex, education, and others | Regular fried food consumption can increase the RR of gastric cancer by 3 times. Regularly consuming garlic, vinegar, and soy products can reduce the GC risk. |
| Park et al. (2000) Korea [14] | M/F | Fried potatoes | High: 6 (109)/ 2 (211) Low: 99 (109)/ 205 (211) | GC | 4 times or more per month, vs. Less than twice per month, 2 or 3 times per month, or 2 or 3 times per week, | p = 0.019 | Age, sex, smoking, drinking, BMI | Eating more fried potatoes was associated with a lower risk of GC |
| De Stefani et al. (2001) Uruguay [23] | M/F | Frying cooking method | High: 17 (123)/ 44 (264) Low: 106 (123)/ 220 (264) | Overall GC | Fried vs. No | 0.9 (0.4–1.8) | Age, gender, education, residence, urban/rural status, smoking, alcohol, mate drinking, energy, and meat intake. | No association |
| KoGES. (2004–2013) Korea [28] | M/F | Fried foods | High: 11 (312)/ 2481 (47,994) Low: 300 (312)/ 45,184 (47,994) | GC | ≥1 time/week vs. <1 time/week or Never | 0.933 (0.493–1.766) 1.0 | Age, gender, BMI, residence area, physical activity, education, income, smoking, intake of alcohol and energy | Not significance |
| Campos et al. (2006) Colombia [12] | M/F | Fried foods | High: 203 (216)/ 382 (431) Low: 13 (216)/ 49 (431) | GC | Yes vs. No | 1.9 (1.0–3.6) (p = 0.039) | Age, gender | A significant association between GC risk and fried foods |
| Pakseresht et al. (2011) Iran [26] | M/F | Fried foods | High: 132 (286)/ 116 (304) Low: 154 (286)/ 188 (304) | Total GC Cardia Non-cardia Intestinal Diffuse | Yes vs. No | 2.21 (1.45–3.37) 4.91 (2.19–11.06) 2.17 (1.34–3.50) 3.33 (1.90–5.82) 3.96 (1.83–8.56) | Age, sex, education, income, living area, smoking, total energy intake, gastric symptoms, H. pylori infection, owning a refrigerator, period of using a refrigerator, frying method | Positive associations with people who prefer fried foods |
| Wang D et al. (2012) China [16] | M/F | Fried foods (beef, pork, lamb, fish, egg, vegetables) | High: 138 (249)/ 96 (260) Low: 111 (249)/ 164 (260) | Genotypes of GC IVS10 + 12G > A IVS12-6T > C | ≥2.5 portions per week vs. less | 2.88 (1.70–4.94) (p < 0.001) 2.48 (1.42–4.13) (p = 0.007) | Age, gender, smoking, drinking, and pickled food intake | High intake of fried foods was positively correlated among participants, particularly with the IVS12-6T > C or IVS10 + 12G > A |
| Jiang M et al. (2012) China [22] | M/F | Fried foods | High: 174 (217)/ 176 (245) Low: 43 (217)/ 69 (245) | GC | ≥3 times/week <3 times/week | 4.372 (1.633–11.706) p = 0.003 | Age, sex, level of education, family history of GC or HP infection | Barbecued food, fried food, overheating diet, and salty food were risk factors for GC, while green tea and garlic intake were protective factors. |
| Sun et al. (2013) China [15] | M/F | Fried foods | High: 144 (470)/ 113 (470) Low: 326 (470)/ 357 (470) | Cardia GC | ≥2 times/week 1–2 times/week Never | 1.46 (0.91–2.33) (p = 0.038) 1.06 (0.69–1.63) (p = 0.578) 1 | Age, sex, nationality, marital status, per capita income, education level | Fried food intake was a risk factor for GC cancer |
| Somi et al. (2015) Iran [27] | M/F | Deep-fried meat (Ghorme), high-fat food | High: 58 (212)/ 64 (404) Low: 145 (212)/ 315 (404) | GC | Yes vs. No | 2.47 (1.5–4.07) (p < 0.001) | Sex, age, education, BMI, smoking | There were positive associations between high-fat foods and GC risk. |
| Guo et al. (2018) China [21] | M/F | Fried food | High: 34 (331)/ 708 (6707) Low: 297 (331)/ 5999 (6707) | GC | Frequently (≥2 times/week), occasionally (1~2 times/week) do not eat (<1 time/week), | 1.91 (1.66–2.20) (p < 0.001) 1.89 (1.57–2.28) (p < 0.001) 1.00 | Age, gender, BMI, marital status, education, smoking, intake of alcohol | Eating fried food is a risk factor for GC and precancerous lesions. Reducing the intake of fried food can prevent the occurrence of gastric carcinoma and precancerous lesions. |
| Cai et al. (2019) China [13] | M/F | Fried foods | High: 36 (267)/ 672 (9571) Low: 231 (267)/ 8899 (9571) | GC | Regular (at least three times/week) vs. occasional (<3 times/week) | 1.71 (1.15–2.54) (p = 0.008) | Age, sex, anti-H. pylori, PG I/II ratio, IgG status, G-17 concentration, pickled food, fried food | Fried food consumption is a predictor of gastric cancer |
| Huang et al. (2020) China [24] | M/F | Fried foods | High: 41 (302)/ 33 (302) Low: 264 (302)/ 269 (302) | GC | Food frequency scores: 1 score ≤1 time per month; 2 scores 2–3 times per month; 0 scores Never | 1.07 (0.95–1.21) (p = 0.265) | Age, sex, height, weight, education level, marital status, alcohol drinking, smoking, and passive smoking | The habit of cooking fried food was associated with higher GC incidence |
| Li et al. (2022) China [25] | M/F | Fried foods | High: 23 (109)/ 94 (910) Low: 86 (109)/ 816 (910) | GC and precancerous lesions | Yes vs. No | 2.322 (1.398–3.855) (p = 0.001) | GC, H. pylori infection | Frequent consumption of fried foods was an independent risk factor for GC and precancerous lesions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, T.; Song, S.S.; Liu, M.; Park, S. Association of Fried Food Intake with Gastric Cancer Risk: A Systemic Review and Meta-Analysis of Case–Control Studies. Nutrients 2023, 15, 2982. https://doi.org/10.3390/nu15132982
Zhang T, Song SS, Liu M, Park S. Association of Fried Food Intake with Gastric Cancer Risk: A Systemic Review and Meta-Analysis of Case–Control Studies. Nutrients. 2023; 15(13):2982. https://doi.org/10.3390/nu15132982
Chicago/Turabian StyleZhang, Ting, Sang Shin Song, Meiling Liu, and Sunmin Park. 2023. "Association of Fried Food Intake with Gastric Cancer Risk: A Systemic Review and Meta-Analysis of Case–Control Studies" Nutrients 15, no. 13: 2982. https://doi.org/10.3390/nu15132982