
Foundational Nutrition: Implications for Human Health
 , ,
, ,
Abstract
:1. Introduction: The Nutritional Health Problem
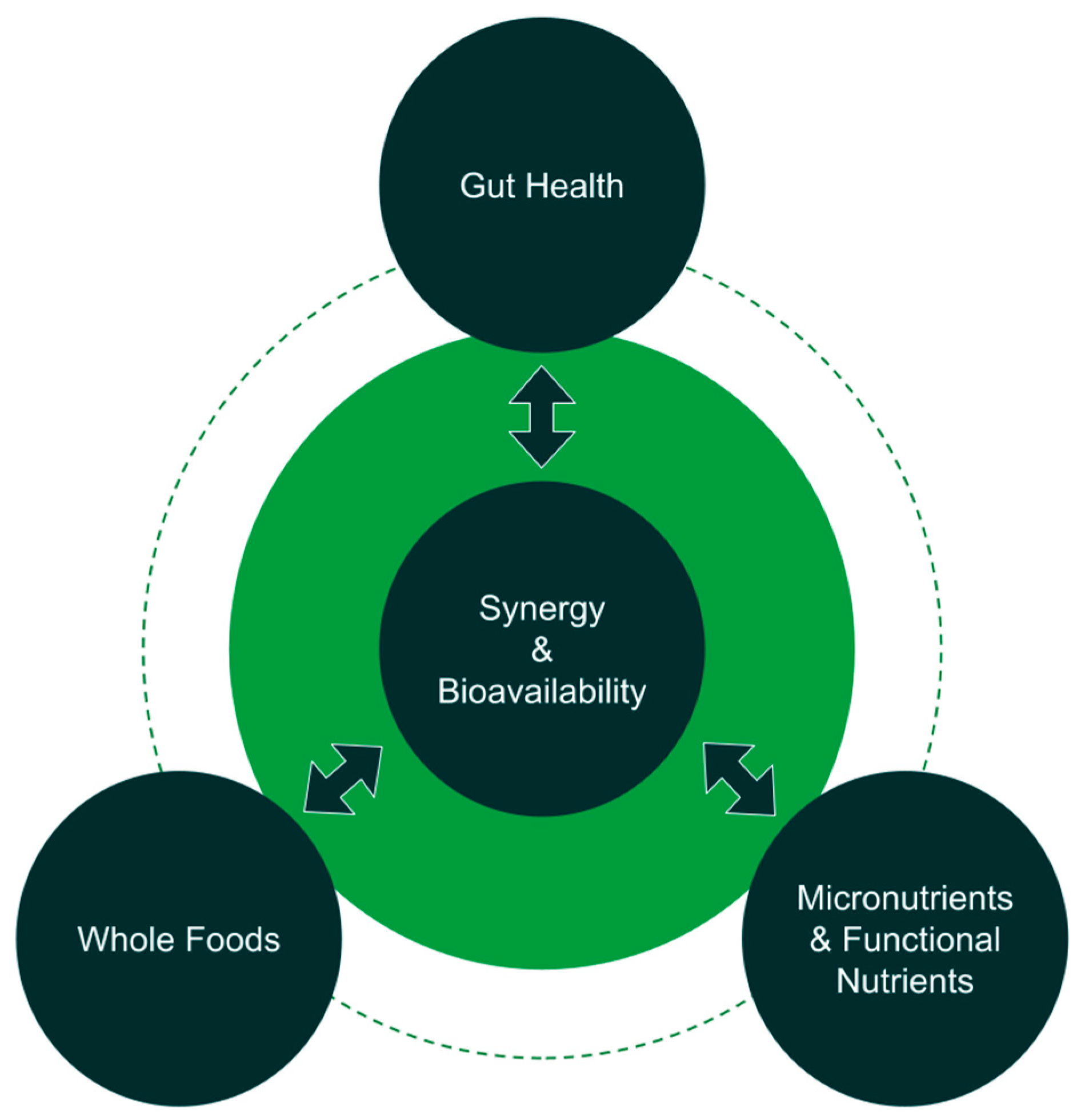
2. Foundational Nutrition Definition
2.1. Leveraging Nutrient Synergy and Bioavailability
2.2. Nutrient Quality, Quantity, and Essential Nutrients
2.3. An Emphasis on Supporting Nutrient Absorption through Gut Health
3. Challenges to an Exclusively Macronutrient-Focused Approach to Nutrition
4. History of Nutrient Recommendations and Further Needs
5. Nutrients and Foundational Nutrition
6. Importance of Gut Health
7. Merely the Beginning
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Fact Sheet: Malnutrition; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Doll, R.; Peto, R. The Causes of Cancer: Quantitative Estimates of Avoidable Risks of Cancer in the United States Today. J. Natl. Cancer Inst. 1981, 66, 1191–1308. [Google Scholar] [CrossRef]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Firth, J.; Gangwisch, J.E.; Borsini, A.; Wootton, R.E.; Mayer, E.A. Food and Mood: How Do Diet and Nutrition Affect Mental Wellbeing? BMJ 2020, 369, m2382. [Google Scholar] [CrossRef]
- Owen, L.; Corfe, B. The Role of Diet and Nutrition on Mental Health and Wellbeing. Proc. Nutr. Soc. 2017, 76, 425–426. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, U.; Mishra, S.; Xu, J.; Levin, S.; Gonzales, J.; Barnard, N.D. A Multicenter Randomized Controlled Trial of a Nutrition Intervention Program in a Multiethnic Adult Population in the Corporate Setting Reduces Depression and Anxiety and Improves Quality of Life: The GEICO Study. Am. J. Health Promot. 2015, 29, 245–254. [Google Scholar] [CrossRef]
- Conner, T.S.; Brookie, K.L.; Richardson, A.C.; Polak, M.A. On Carrots and Curiosity: Eating Fruit and Vegetables Is Associated with Greater Flourishing in Daily Life. Br. J. Health Psychol. 2015, 20, 413–427. [Google Scholar] [CrossRef]
- Coppen, A.; Bailey, J. Enhancement of the Antidepressant Action of Fluoxetine by Folic Acid: A Randomised, Placebo Controlled Trial. J. Affect. Disord. 2000, 60, 121–130. [Google Scholar] [CrossRef]
- Mech, A.W.; Farah, A. Correlation of Clinical Response with Homocysteine Reduction during Therapy with Reduced B Vitamins in Patients with MDD Who Are Positive for MTHFR C677T or A1298C Polymorphism: A Randomized, Double-Blind, Placebo-Controlled Study. J. Clin. Psychiatry 2016, 77, 668–671. [Google Scholar] [CrossRef] [Green Version]
- Mozaffari-Khosravi, H.; Nabizade, L.; Yassini-Ardakani, S.M.; Hadinedoushan, H.; Barzegar, K. The Effect of 2 Different Single Injections of High Dose of Vitamin D on Improving the Depression in Depressed Patients with Vitamin D Deficiency: A Randomized Clinical Trial. J. Clin. Psychopharmacol. 2013, 33, 378. [Google Scholar] [CrossRef]
- Spasov, A.A.; Wikman, G.K.; Mandrikov, V.B.; Mironova, I.A.; Neumoin, V.V. A Double-Blind, Placebo-Controlled Pilot Study of the Stimulating and Adaptogenic Effect of Rhodiola Rosea SHR-5 Extract on the Fatigue of Students Caused by Stress during an Examination Period with a Repeated Low-Dose Regimen. Phytomedicine 2000, 7, 85–89. [Google Scholar] [CrossRef]
- James, W.P.; Nelson, M.; Ralph, A.; Leather, S. Socioeconomic Determinants of Health. The Contribution of Nutrition to Inequalities in Health. BMJ 1997, 314, 1545–1549. [Google Scholar] [CrossRef] [Green Version]
- Darmon, N.; Drewnowski, A. Contribution of Food Prices and Diet Cost to Socioeconomic Disparities in Diet Quality and Health: A Systematic Review and Analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef]
- Gundersen, C.; Ziliak, J.P. Food Insecurity And Health Outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [Green Version]
- Marti-Soler, H.; Guessous, I.; Gaspoz, J.-M.; Metcalf, P.; Deschamps, V.; Castetbon, K.; Malyutina, S.; Bobak, M.; Ruidavets, J.-B.; Bongard, V.; et al. Seasonality of Nutrient Intake—An Analysis Including over 44,000 Participants in 4 Countries. Clin. Nutr. ESPEN 2017, 21, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Marshak, A.; Venkat, A.; Young, H.; Naumova, E.N. How Seasonality of Malnutrition Is Measured and Analyzed. Int. J. Environ. Res. Public Health 2021, 18, 1828. [Google Scholar] [CrossRef]
- Fardet, A.; Rock, E. Toward a New Philosophy of Preventive Nutrition: From a Reductionist to a Holistic Paradigm to Improve Nutritional Recommendations. Adv. Nutr. 2014, 5, 430–446. [Google Scholar] [CrossRef] [Green Version]
- Messina, M.; Lampe, J.W.; Birt, D.F.; Appel, L.J. Reductionism and the Narrowing Nutrition Perspective: Time for Reevaluation and Emphasis on Food Synergy. J. Acad. Nutr. Diet. 2001, 101, 1416. [Google Scholar]
- Yeum, K.-J.; Beretta, G.; Krinsky, N.I.; Russell, R.M.; Aldini, G. Synergistic Interactions of Antioxidant Nutrients in a Biological Model System. Nutrition 2009, 25, 839–846. [Google Scholar] [CrossRef]
- Christian, P.; West, K.P. Interactions between Zinc and Vitamin A: An Update. Am. J. Clin. Nutr. 1998, 68, 435S–441S. [Google Scholar] [CrossRef] [Green Version]
- Fardet, A.; Rock, E. The Search for a New Paradigm to Study Micronutrient and Phytochemical Bioavailability: From Reductionism to Holism. Med. Hypotheses 2014, 82, 181–186. [Google Scholar] [CrossRef]
- Yang, Q.; Liang, Q.; Balakrishnan, B.; Belobrajdic, D.P.; Feng, Q.-J.; Zhang, W. Role of Dietary Nutrients in the Modulation of Gut Microbiota: A Narrative Review. Nutrients 2020, 12, 381. [Google Scholar] [CrossRef] [Green Version]
- Zhan, Q.; Wang, R.; Thakur, K.; Feng, J.-Y.; Zhu, Y.-Y.; Zhang, J.-G.; Wei, Z.-J. Unveiling of Dietary and Gut-Microbiota Derived B Vitamins: Metabolism Patterns and Their Synergistic Functions in Gut-Brain Homeostasis. Crit. Rev. Food Sci. Nutr. 2022, 1–13. [Google Scholar] [CrossRef]
- Van Campen, D.R.; Glahn, R.P. Micronutrient Bioavailability Techniques: Accuracy, Problems and Limitations. Field Crops Res. 1999, 60, 93–113. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluationof Dietary Reference Intakes. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press (US): Washington, DC, USA, 1997; ISBN 978-0-309-06350-0. [Google Scholar]
- Pardo, M.R.; Garicano Vilar, E.; San Mauro Martín, I.; Camina Martín, M.A. Bioavailability of Magnesium Food Supplements: A Systematic Review. Nutrition 2021, 89, 111294. [Google Scholar] [CrossRef] [PubMed]
- Mattar, G.; Haddarah, A.; Haddad, J.; Pujola, M.; Sepulcre, F. New Approaches, Bioavailability and the Use of Chelates as a Promising Method for Food Fortification. Food Chem. 2022, 373, 131394. [Google Scholar] [CrossRef]
- Melse-Boonstra, A. Bioavailability of Micronutrients from Nutrient-Dense Whole Foods: Zooming in on Dairy, Vegetables, and Fruits. Front. Nutr. 2020, 7, 101. [Google Scholar] [CrossRef] [PubMed]
- Rowland, I.; Gibson, G.; Heinken, A.; Scott, K.; Swann, J.; Thiele, I.; Tuohy, K. Gut Microbiota Functions: Metabolism of Nutrients and Other Food Components. Eur. J. Nutr. 2018, 57, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Oh, R.; Brown, D.L. Vitamin B12 Deficiency. Am. Fam. Physician 2003, 67, 979–986. [Google Scholar] [PubMed]
- Hill, M.J. Intestinal Flora and Endogenous Vitamin Synthesis. Eur. J. Cancer Prev. 1997, 6 (Suppl. S1), S43–S45. [Google Scholar] [CrossRef] [PubMed]
- Judkins, T.C.; Archer, D.L.; Kramer, D.C.; Solch, R.J. Probiotics, Nutrition, and the Small Intestine. Curr. Gastroenterol. Rep. 2020, 22, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Torras, S.; Iglesias, I.; Llopis, M.; Lozano, J.J.; Antolín, M.; Guarner, F.; Pastor-Anglada, M. Transportome Profiling Identifies Profound Alterations in Crohn’s Disease Partially Restored by Commensal Bacteria. J. Crohn’s Colitis 2016, 10, 850–859. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.C.; Spiegel, B.M.R.; Talley, N.J.; Moayyedi, P. Small Intestinal Bacterial Overgrowth in Irritable Bowel Syndrome: Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2009, 7, 1279–1286. [Google Scholar] [CrossRef]
- Dukowicz, A.C.; Lacy, B.E.; Levine, G.M. Small Intestinal Bacterial Overgrowth. Gastroenterol. Hepatol. 2007, 3, 112–122. [Google Scholar]
- Singh, R.; Zogg, H.; Wei, L.; Bartlett, A.; Ghoshal, U.C.; Rajender, S.; Ro, S. Gut Microbial Dysbiosis in the Pathogenesis of Gastrointestinal Dysmotility and Metabolic Disorders. J. Neurogastroenterol. Motil. 2021, 27, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Wedlake, L.; A’Hern, R.; Russell, D.; Thomas, K.; Walters, J.R.F.; Andreyev, H.J.N. Systematic Review: The Prevalence of Idiopathic Bile Acid Malabsorption as Diagnosed by SeHCAT Scanning in Patients with Diarrhoea-Predominant Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2009, 30, 707–717. [Google Scholar] [CrossRef]
- Wei, Y.; Zhang, H.; Zhang, S.; Li, H. The Influence of Diet upon Liver Function Indices of Healthy Volunteers Resident in a Phase I Clinical Trail. Am. J. Transl. Res. 2019, 11, 3187–3194. [Google Scholar]
- World Health Organization. Obesity and Overweight Fact Sheet; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction: The American Heart Association’s Strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [Green Version]
- Rehm, C.D.; Peñalvo, J.L.; Afshin, A.; Mozaffarian, D. Dietary Intake among US Adults, 1999–2012. JAMA 2016, 315, 2542–2553. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet: A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [Green Version]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.-E.; Moreiras-Varela, O.; Menotti, A.; Van Staveren, W.A. Mediterranean Diet, Lifestyle Factors, and 10-Year Mortality in Elderly European Men and Women: The HALE Project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Tuso, P.J.; Ismail, M.H.; Ha, B.P.; Bartolotto, C. Nutritional Update for Physicians: Plant-Based Diets. Perm. J. 2013, 17, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; December 2015. Available online: https://health.gov/our-work/food-nutrition/previous-dietary-guidelines/2015 (accessed on 3 March 2023).
- Steele, E.M.; Baraldi, L.G.; da Costa Louzada, M.L.; Moubarac, J.-C.; Mozaffarian, D.; Monteiro, C.A. Ultra-Processed Foods and Added Sugars in the US Diet: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [Green Version]
- Martini, D.; Godos, J.; Bonaccio, M.; Vitaglione, P.; Grosso, G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients 2021, 13, 3390. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C.; McBurney, M.; Fulgoni, V.L. Multivitamin/Mineral Supplement Contribution to Micronutrient Intakes in the United States, 2007–2010. J. Am. Coll. Nutr. 2014, 33, 94–102. [Google Scholar] [CrossRef]
- Davis, D.R.; Epp, M.D.; Riordan, H.D. Changes in USDA Food Composition Data for 43 Garden Crops, 1950 to 1999. J. Am. Coll. Nutr. 2004, 23, 669–682. [Google Scholar] [CrossRef]
- Mayer, A.-M. Historical Changes in the Mineral Content of Fruits and Vegetables. Br. Food J. 1997, 99, 207–211. [Google Scholar] [CrossRef]
- Mayer, A.-M.B.; Trenchard, L.; Rayns, F. Historical Changes in the Mineral Content of Fruit and Vegetables in the UK from 1940 to 2019: A Concern for Human Nutrition and Agriculture. Int. J. Food Sci. Nutr. 2022, 73, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D. A Study on the Mineral Depletion of the Foods Available to Us as a Nation over the Period 1940 to 1991. Nutr. Health 2003, 17, 85–115. [Google Scholar] [CrossRef]
- White, P.J.; Broadley, M.R. Historical Variation in the Mineral Composition of Edible Horticultural Products. J. Hortic. Sci. Biotechnol. 2005, 80, 660–667. [Google Scholar] [CrossRef]
- Tirado, M.C.; Crahay, P.; Mahy, L.; Zanev, C.; Neira, M.; Msangi, S.; Brown, R.; Scaramella, C.; Coitinho, D.C.; Müller, A. Climate Change and Nutrition: Creating a Climate for Nutrition Security. Food Nutr. Bull. 2013, 34, 533–547. [Google Scholar] [CrossRef]
- Black, M.M. Micronutrient Deficiencies and Cognitive Functioning. J. Nutr. 2003, 133, 3927S–3931S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cascino, T.M.; Hummel, S.L. Nutrient Deficiencies in Heart Failure: A Micro Problem with Macro Effects? J. Am. Heart Assoc. 2018, 7, e010447. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Garach, A.; García-Fontana, B.; Muñoz-Torres, M. Nutrients and Dietary Patterns Related to Osteoporosis. Nutrients 2020, 12, 1986. [Google Scholar] [CrossRef] [PubMed]
- Reider, C.A.; Chung, R.-Y.; Devarshi, P.P.; Grant, R.W.; Hazels Mitmesser, S. Inadequacy of Immune Health Nutrients: Intakes in US Adults, the 2005–2016 NHANES. Nutrients 2020, 12, 1735. [Google Scholar] [CrossRef]
- Haidar, Y.M.; Cosman, B.C. Obesity Epidemiology. Clin. Colon. Rectal Surg. 2011, 24, 205–210. [Google Scholar] [CrossRef]
- Khanna, D.; Welch, B.S.; Rehman, A. Pathophysiology of Obesity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kobylińska, M.; Antosik, K.; Decyk, A.; Kurowska, K. Malnutrition in Obesity: Is It Possible? Obes. Facts 2021, 15, 19–25. [Google Scholar] [CrossRef]
- Xanthakos, S.A. Nutritional Deficiencies in Obesity and After Bariatric Surgery. Pediatr. Clin. 2009, 56, 1105–1121. [Google Scholar] [CrossRef] [Green Version]
- Kaidar-Person, O.; Person, B.; Szomstein, S.; Rosenthal, R.J. Nutritional Deficiencies in Morbidly Obese Patients: A New Form of Malnutrition? Part A: Vitamins. Obes. Surg. 2008, 18, 870–876. [Google Scholar] [CrossRef]
- Strohmayer, E.; Via, M.A.; Yanagisawa, R. Metabolic Management Following Bariatric Surgery. Mt. Sinai J. Med. 2010, 77, 431–445. [Google Scholar] [CrossRef]
- Banach, W.; Nitschke, K.; Krajewska, N.; Mongiałło, W.; Matuszak, O.; Muszyński, J.; Skrypnik, D. The Association between Excess Body Mass and Disturbances in Somatic Mineral Levels. Int. J. Mol. Sci. 2020, 21, 7306. [Google Scholar] [CrossRef]
- Via, M. The Malnutrition of Obesity: Micronutrient Deficiencies That Promote Diabetes. ISRN Endocrinol. 2012, 2012, 103472. [Google Scholar] [CrossRef] [Green Version]
- García, O.P.; Ronquillo, D.; Caamaño, M.d.C.; Martínez, G.; Camacho, M.; López, V.; Rosado, J.L. Zinc, Iron and Vitamins A, C and E Are Associated with Obesity, Inflammation, Lipid Profile and Insulin Resistance in Mexican School-Aged Children. Nutrients 2013, 5, 5012–5030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cigerli, O.; Parildar, H.; Dogruk Unal, A.; Tarcin, O.; Kut, A.; Eroglu, H.; Guvener, N. Vitamin deficiency and insulin resistance in nondiabetic obese patients. Acta Endocrinol. 2016, 12, 319–327. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Recommended Dietary Allowances; National Research Council-National Academy Press: Washington, DC, USA, 1989.
- Leitch, I. The Evolution of Dietary Standards. Nutr. Abstr. Rev. 1942, 11, 509–521. [Google Scholar]
- Roberts, L.J. Beginnings of the Recommended Dietary Allowances. J. Am. Diet. Assoc. 1958, 34, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Saltos, E. Over Time. Am. Eat. Habits Changes Conseq. 1999, 750, 33. [Google Scholar]
- Murphy, S.P.; Yates, A.A.; Atkinson, S.A.; Barr, S.I.; Dwyer, J. History of Nutrition: The Long Road Leading to the Dietary Reference Intakes for the United States and Canada. Adv. Nutr. 2016, 7, 157–168. [Google Scholar] [CrossRef] [Green Version]
- National Research Council. Diet and Health: Implications for Reducing Chronic Disease Risk; National Academies Press: Washington, DC, USA, 1989.
- Campbell, S. Dietary Reference Intakes: Water, Potassium, Sodium, Chloride, and Sulfate. Clin. Nutr. Insight 2004, 30, 1–4. [Google Scholar]
- Institute of Medicine (US) Food & Nutrition Board. Dietary Reference Intakes: A Risk Assessment Model for Establishing Upper Intake Levels for Nutrients; National Academies Press: Washington, DC, USA, 1998; ISBN 0-309-06348-5. [Google Scholar]
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes F N B. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academies Press (US): Washington, DC, USA, 1998. [Google Scholar]
- Institute of Medicine (US). Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids: A Report. of the Panel on Dietary Antioxidants and Related Compounds, Subcommittees on Upper Reference Levels of Nutrients; National Academies Press: Washington, DC, USA, 2000; ISBN 0-309-06949-1. [Google Scholar]
- Institute of Medicine; Panel on Micronutrients; Nutrition Board; Subcommittees on Upper Reference Levels of Nutrients, of Interpretation; Use of Dietary Reference Intakes. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; Dietary Reference Intakes; National Academies Press (US): Washington, DC, USA, 2002; ISBN 0-309-07290-5. [Google Scholar]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids.(Commentary). J. Am. Diet. Assoc. 2002, 102, 1621–1631. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes: Applications in Dietary Planning; National Academies Press (US): Washington, DC, USA, 2003. [Google Scholar]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. DRI Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press (US): Washington, DC, USA, 2000. [Google Scholar]
- Institute of Medicine (US). Panel on Dietary Reference Intakes for Electrolytes, & Water. DRI, Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; National Academies Press (US): Washington, DC, USA, 2004; ISBN 0-309-09170-5. [Google Scholar]
- Del Valle, H.B.; Yaktine, A.L.; Taylor, C.L.; Ross, A.C. Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Kohlmeier, M. Nutrient Metabolism: Structures, Functions, and Genes; Academic Press: Cambridge, MA, USA, 2015; ISBN 0-12-387788-1. [Google Scholar]
- De Lauzon, B.; Volatier, J.L.; Martin, A. A Monte Carlo Simulation to Validate the EAR Cut-Point Method for Assessing the Prevalence of Nutrient Inadequacy at the Population Level. Public Health Nutr. 2004, 7, 893–900. [Google Scholar] [CrossRef] [Green Version]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Food and Nutrition Board; Committee on the Development of Guiding Principles for the Inclusion of Chronic Disease Endpoints in Future Dietary Reference Intakes. Guiding Principles for Developing Dietary Reference Intakes Based on Chronic Disease; Oria, M.P., Kumanyika, S., Eds.; National Academies Press (US): Washington, DC, USA, 3 August 2017. Available online: https://www.ncbi.nlm.nih.gov/books/NBK465016/ (accessed on 3 March 2023).
- Yaktine, A.L.; Ross, A.C. Milestones in DRI Development: What Does the Future Hold? Adv. Nutr. 2019, 10, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Yetley, E.A.; MacFarlane, A.J.; Greene-Finestone, L.S.; Garza, C.; Ard, J.D.; Atkinson, S.A.; Bier, D.M.; Carriquiry, A.L.; Harlan, W.R.; Hattis, D. Options for Basing Dietary Reference Intakes (DRIs) on Chronic Disease Endpoints: Report from a Joint US-/Canadian-Sponsored Working Group. Am. J. Clin. Nutr. 2017, 105, 249S–285S. [Google Scholar] [CrossRef] [Green Version]
- MacFarlane, A.J.; Cogswell, M.E.; de Jesus, J.M.; Greene-Finestone, L.S.; Klurfeld, D.M.; Lynch, C.J.; Regan, K.; Yamini, S.; Group, J.C.-U.D.R.I.W. A Report of Activities Related to the Dietary Reference Intakes from the Joint Canada-US Dietary Reference Intakes Working Group. Am. J. Clin. Nutr. 2019, 109, 251–259. [Google Scholar] [CrossRef] [Green Version]
- Flock, M.R.; Harris, W.S.; Kris-Etherton, P.M. Long-Chain Omega-3 Fatty Acids: Time to Establish a Dietary Reference Intake. Nutr. Rev. 2013, 71, 692–707. [Google Scholar] [CrossRef]
- Racey, M.; MacFarlane, A.; Carlson, S.E.; Stark, K.D.; Plourde, M.; Field, C.J.; Yates, A.A.; Wells, G.; Grantham, A.; Bazinet, R.P. Dietary Reference Intakes Based on Chronic Disease Endpoints: Outcomes from a Case Study Workshop for Omega 3’s EPA and DHA. Appl. Physiol. Nutr. Metab. 2021, 46, 530–539. [Google Scholar] [CrossRef]
- Williamson, G.; Holst, B. Dietary Reference Intake (DRI) Value for Dietary Polyphenols: Are We Heading in the Right Direction? Br. J. Nutr. 2008, 99, S55–S58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, W.S.; Mozaffarian, D.; Lefevre, M.; Toner, C.D.; Colombo, J.; Cunnane, S.C.; Holden, J.M.; Klurfeld, D.M.; Morris, M.C.; Whelan, J. Towards Establishing Dietary Reference Intakes for Eicosapentaenoic and Docosahexaenoic Acids. J. Nutr. 2009, 139, 804S–819S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupton, J.R.; Atkinson, S.A.; Chang, N.; Fraga, C.G.; Levy, J.; Messina, M.; Richardson, D.P.; van Ommen, B.; Yang, Y.; Griffiths, J.C.; et al. Exploring the Benefits and Challenges of Establishing a DRI-like Process for Bioactives. Eur. J. Nutr. 2014, 53, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pressman, P.; Clemens, R.A.; Hayes, A.W. Bioavailability of Micronutrients Obtained from Supplements and Food: A Survey and Case Study of the Polyphenols. Toxicol. Res. Appl. 2017, 1, 2397847317696366. [Google Scholar] [CrossRef] [Green Version]
- Hambidge, K.M. Micronutrient Bioavailability: Dietary Reference Intakes and a Future Perspective. Am. J. Clin. Nutr. 2010, 91, 1430S–1432S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, C.; Prakash, D. Phytonutrients as Therapeutic Agents. J. Complement. Integr. Med. 2014, 11, 151–169. [Google Scholar] [CrossRef] [PubMed]
- Blekkenhorst, L.C.; Sim, M.; Bondonno, C.P.; Bondonno, N.P.; Ward, N.C.; Prince, R.L.; Devine, A.; Lewis, J.R.; Hodgson, J.M. Cardiovascular Health Benefits of Specific Vegetable Types: A Narrative Review. Nutrients 2018, 10, 595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beecher, G.R. Phytonutrients’ Role in Metabolism: Effects on Resistance to Degenerative Processes. Nutr. Rev. 1999, 57, 3–6. [Google Scholar] [CrossRef]
- Carlsen, M.H.; Halvorsen, B.L.; Holte, K.; Bøhn, S.K.; Dragland, S.; Sampson, L.; Willey, C.; Senoo, H.; Umezono, Y.; Sanada, C.; et al. The Total Antioxidant Content of More than 3100 Foods, Beverages, Spices, Herbs and Supplements Used Worldwide. Nutr. J. 2010, 9, 3. [Google Scholar] [CrossRef]
- Cardona, F.; Andrés-Lacueva, C.; Tulipani, S.; Tinahones, F.J.; Queipo-Ortuño, M.I. Benefits of Polyphenols on Gut Microbiota and Implications in Human Health. J. Nutr. Biochem. 2013, 24, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- Fraga, C.G.; Galleano, M.; Verstraeten, S.V.; Oteiza, P.I. Basic Biochemical Mechanisms behind the Health Benefits of Polyphenols. Mol. Asp. Med. 2010, 31, 435–445. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.; Samtiya, M.; Dhewa, T.; Mishra, V.; Aluko, R.E. Health Benefits of Polyphenols: A Concise Review. J. Food Biochem. 2022, 46, e14264. [Google Scholar] [CrossRef] [PubMed]
- Rasouli, H.; Farzaei, M.H.; Khodarahmi, R. Polyphenols and Their Benefits: A Review. Int. J. Food Prop. 2017, 20, 1700–1741. [Google Scholar] [CrossRef] [Green Version]
- Ding, S.; Jiang, H.; Fang, J. Regulation of Immune Function by Polyphenols. J. Immunol. Res. 2018, 2018, 1264074. [Google Scholar] [CrossRef] [Green Version]
- Kampa, M.; Nifli, A.-P.; Notas, G.; Castanas, E. Polyphenols and Cancer Cell Growth. Rev. Physiol. Biochem. Pharmacol. 2007, 159, 79–113. [Google Scholar] [CrossRef]
- Scalbert, A.; Johnson, I.T.; Saltmarsh, M. Polyphenols: Antioxidants and Beyond. Am. J. Clin. Nutr. 2005, 81, 215S–217S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, D.E.; Hurst, R.D. Polyphenolic Phytochemicals—Just Antioxidants or Much More? Cell. Mol. Life Sci. 2007, 64, 2900–2916. [Google Scholar] [CrossRef] [PubMed]
- Siard, M.H.; McMurry, K.E.; Adams, A.A. Effects of Polyphenols Including Curcuminoids, Resveratrol, Quercetin, Pterostilbene, and Hydroxypterostilbene on Lymphocyte pro-Inflammatory Cytokine Production of Senior Horses in Vitro. Vet. Immunol. Immunopathol. 2016, 173, 50–59. [Google Scholar] [CrossRef]
- Yahfoufi, N.; Alsadi, N.; Jambi, M.; Matar, C. The Immunomodulatory and Anti-Inflammatory Role of Polyphenols. Nutrients 2018, 10, 1618. [Google Scholar] [CrossRef] [Green Version]
- Yao, W.; Zhang, X.; Xu, F.; Cao, C.; Liu, T.; Xue, Y. The Therapeutic Effects of Naringenin on Bronchial Pneumonia in Children. Pharmacol. Res. Perspect. 2021, 9, e00825. [Google Scholar] [CrossRef]
- Nieto-Vazquez, I.; Fernández-Veledo, S.; Krämer, D.K.; Vila-Bedmar, R.; Garcia-Guerra, L.; Lorenzo, M. Insulin Resistance Associated to Obesity: The Link TNF-Alpha. Arch. Physiol. Biochem. 2008, 114, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Azizi, G.; Mirshafiey, A. The Potential Role of Proinflammatory and Antiinflammatory Cytokines in Alzheimer Disease Pathogenesis. Immunopharmacol. Immunotoxicol. 2012, 34, 881–895. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Arik, F.; Smith, L.; Jackson, S.E.; Isik, A.T. Inflammation, Frailty and Cardiovascular Disease. Adv. Exp. Med. Biol. 2020, 1216, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.; Zhang, Y.; Wang, X.-Z.; Zhao, J.; Yang, Z.-J.; Lin, Y.-P.; Sun, L.; Lu, Q.-Y.; Fan, G.-J. Flavonoids for Treating Viral Acute Respiratory Tract Infections: A Systematic Review and Meta-Analysis of 30 Randomized Controlled Trials. Front. Public Health 2022, 10, 814669. [Google Scholar] [CrossRef]
- Rizza, S.; Muniyappa, R.; Iantorno, M.; Kim, J.; Chen, H.; Pullikotil, P.; Senese, N.; Tesauro, M.; Lauro, D.; Cardillo, C. Citrus Polyphenol Hesperidin Stimulates Production of Nitric Oxide in Endothelial Cells While Improving Endothelial Function and Reducing Inflammatory Markers in Patients with Metabolic Syndrome. J. Clin. Endocrinol. Metab. 2011, 96, E782–E792. [Google Scholar] [CrossRef] [PubMed]
- Homayouni, F.; Haidari, F.; Hedayati, M.; Zakerkish, M.; Ahmadi, K. Blood Pressure Lowering and Anti-inflammatory Effects of Hesperidin in Type 2 Diabetes; a Randomized Double-blind Controlled Clinical Trial. Phytother. Res. 2018, 32, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Morand, C.; Dubray, C.; Milenkovic, D.; Lioger, D.; Martin, J.F.; Scalbert, A.; Mazur, A. Hesperidin Contributes to the Vascular Protective Effects of Orange Juice: A Randomized Crossover Study in Healthy Volunteers. Am. J. Clin. Nutr. 2011, 93, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bérubé-Parent, S.; Pelletier, C.; Doré, J.; Tremblay, A. Effects of Encapsulated Green Tea and Guarana Extracts Containing a Mixture of Epigallocatechin-3-Gallate and Caffeine on 24 h Energy Expenditure and Fat Oxidation in Men. Br. J. Nutr. 2005, 94, 432–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maki, K.C.; Reeves, M.S.; Farmer, M.; Yasunaga, K.; Matsuo, N.; Katsuragi, Y.; Komikado, M.; Tokimitsu, I.; Wilder, D.; Jones, F.; et al. Green Tea Catechin Consumption Enhances Exercise-Induced Abdominal Fat Loss in Overweight and Obese Adults. J. Nutr. 2009, 139, 264–270. [Google Scholar] [CrossRef] [Green Version]
- Vázquez Cisneros, L.C.; López-Uriarte, P.; López-Espinoza, A.; Navarro Meza, M.; Espinoza-Gallardo, A.C.; Guzmán Aburto, M.B. Effects of green tea and its epigallocatechin (EGCG) content on body weight and fat mass in humans: A systematic review. Nutr. Hosp. 2017, 34, 731–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuby, J.; Gravestock, I.; Wolfram, E.; Pichierri, G.; Steurer, J.; Burgstaller, J.M. Appetite-Suppressing and Satiety-Increasing Bioactive Phytochemicals: A Systematic Review. Nutrients 2019, 11, 2238. [Google Scholar] [CrossRef] [Green Version]
- Bentinger, M.; Tekle, M.; Dallner, G. Coenzyme Q–Biosynthesis and Functions. Biochem. Biophys. Res. Commun. 2010, 396, 74–79. [Google Scholar] [CrossRef]
- Thomas, S.R.; Neuzil, J.; Stocker, R. Inhibition of LDL Oxidation by Ubiquinol-10. A Protective Mechanism for Coenzyme Q in Atherogenesis? Mol. Asp. Med. 1997, 18, 85–103. [Google Scholar] [CrossRef]
- Gao, L.; Mao, Q.; Cao, J.; Wang, Y.; Zhou, X.; Fan, L. Effects of Coenzyme Q10 on Vascular Endothelial Function in Humans: A Meta-Analysis of Randomized Controlled Trials. Atherosclerosis 2012, 221, 311–316. [Google Scholar] [CrossRef]
- Tabrizi, R.; Akbari, M.; Sharifi, N.; Lankarani, K.B.; Moosazadeh, M.; Kolahdooz, F.; Taghizadeh, M.; Asemi, Z. The Effects of Coenzyme Q10 Supplementation on Blood Pressures Among Patients with Metabolic Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. High Blood Press. Cardiovasc. Prev. 2018, 25, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Žmitek, K.; Pogačnik, T.; Mervic, L.; Žmitek, J.; Pravst, I. The Effect of Dietary Intake of Coenzyme Q10 on Skin Parameters and Condition: Results of a Randomised, Placebo-Controlled, Double-Blind Study. BioFactors 2017, 43, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.; Feng, Y.; Chen, G.-C.; Qin, L.-Q.; Fu, C.; Chen, L.-H. Effects of Coenzyme Q10 Supplementation on Inflammatory Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pharmacol. Res. 2017, 119, 128–136. [Google Scholar] [CrossRef]
- Calder, P.C.; Yaqoob, P. Understanding Omega-3 Polyunsaturated Fatty Acids. Postgrad. Med. 2009, 121, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Das, U.N. Essential Fatty Acids: Biochemistry, Physiology and Pathology. Biotechnol. J. Healthc. Nutr. Technol. 2006, 1, 420–439. [Google Scholar] [CrossRef]
- U.S. Department of Agriculture, Agricultural Research Service. What We Eat in America, 2011–2012; National Academies Press (US): Washington, DC, USA, 2015.
- Brenna, J.T.; Salem Jr, N.; Sinclair, A.J.; Cunnane, S.C. α-Linolenic Acid Supplementation and Conversion to n-3 Long-Chain Polyunsaturated Fatty Acids in Humans. Prostaglandins Leukot. Essent. Fat. Acids 2009, 80, 85–91. [Google Scholar] [CrossRef]
- Barry, A.R.; Dixon, D.L. Omega-3 Fatty Acids for the Prevention of Atherosclerotic Cardiovascular Disease. Pharmacotherapy 2021, 41, 1056–1065. [Google Scholar] [CrossRef]
- NIH Office of Dietary Supplements—Omega-3 Fatty Acids. Available online: https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/ (accessed on 3 March 2023).
- Murphy, R.A.; Devarshi, P.P.; Ekimura, S.; Marshall, K.; Mitmesser, S.H. Long-Chain Omega-3 Fatty Acid Serum Concentrations across Life Stages in the USA: An Analysis of NHANES 2011–2012. BMJ Open 2021, 11, e043301. [Google Scholar] [CrossRef]
- De Caterina, R.; Liao, J.K.; Libby, P. Fatty Acid Modulation of Endothelial Activation. Am. J. Clin. Nutr. 2000, 71, 213S–223S. [Google Scholar] [CrossRef] [Green Version]
- Goodfellow, J.; Bellamy, M.F.; Ramsey, M.W.; Jones, C.J.; Lewis, M.J. Dietary Supplementation with Marine Omega-3 Fatty Acids Improve Systemic Large Artery Endothelial Function in Subjects with Hypercholesterolemia. J. Am. Coll. Cardiol. 2000, 35, 265–270. [Google Scholar] [CrossRef] [Green Version]
- Jain, A.P.; Aggarwal, K.K.; Zhang, P.-Y. Omega-3 Fatty Acids and Cardiovascular Disease. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 441–445. [Google Scholar] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef]
- Hu, Y.; Hu, F.B.; Manson, J.E. Marine Omega-3 Supplementation and Cardiovascular Disease: An Updated Meta-Analysis of 13 Randomized Controlled Trials Involving 127 477 Participants. J. Am. Heart Assoc. 2019, 8, e013543. [Google Scholar] [CrossRef]
- Mazereeuw, G.; Lanctôt, K.L.; Chau, S.A.; Swardfager, W.; Herrmann, N. Effects of Omega-3 Fatty Acids on Cognitive Performance: A Meta-Analysis. Neurobiol. Aging 2012, 33, 1482.e17–1482.e29. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.; Summerbell, C.D.; Worthington, H.V.; Song, F.; et al. Omega-3 Fatty Acids for the Primary and Secondary Prevention of Cardiovascular Disease. Cochrane Database Syst. Rev. 2020, 3, CD003177. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Cook, N.R.; Lee, I.-M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Albert, C.M.; Gordon, D.; Copeland, T.; et al. Marine N-3 Fatty Acids and Prevention of Cardiovascular Disease and Cancer. N. Engl. J. Med. 2019, 380, 23–32. [Google Scholar] [CrossRef]
- van Gelder, B.M.; Tijhuis, M.; Kalmijn, S.; Kromhout, D. Fish Consumption, n-3 Fatty Acids, and Subsequent 5-y Cognitive Decline in Elderly Men: The Zutphen Elderly Study. Am. J. Clin. Nutr. 2007, 85, 1142–1147. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Liu, X.; Zhang, D. Fish Consumption and Risk of Depression: A Meta-Analysis. J. Epidemiol. Community Health 2016, 70, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Sköldstam, L.; Börjesson, O.; Kjällman, A.; Seiving, B.; Akesson, B. Effect of Six Months of Fish Oil Supplementation in Stable Rheumatoid Arthritis. A Double-Blind, Controlled Study. Scand. J. Rheumatol. 1992, 21, 178–185. [Google Scholar] [CrossRef]
- Swanson, D.; Block, R.; Mousa, S.A. Omega-3 Fatty Acids EPA and DHA: Health Benefits throughout Life. Adv. Nutr. 2012, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Alonso, M.; Aguirre Camorlinga, A.; Messiah, S.E.; Marroquin, E. Effect of Adding Probiotics to an Antibiotic Intervention on the Human Gut Microbial Diversity and Composition: A Systematic Review. J. Med. Microbiol. 2022, 71, 001625. [Google Scholar] [CrossRef]
- Sánchez, B.; Delgado, S.; Blanco-Míguez, A.; Lourenço, A.; Gueimonde, M.; Margolles, A. Probiotics, Gut Microbiota, and Their Influence on Host Health and Disease. Mol. Nutr. Food Res. 2017, 61, 1600240. [Google Scholar] [CrossRef] [Green Version]
- Chávarri, M.; Diez-Gutiérrez, L.; Marañón, I.; del Carmen Villarán, M.; Barrón, L.J.R. The Role of Probiotics in Nutritional Health: Probiotics as Nutribiotics. In Probiotics in the Prevention and Management of Human. Diseases; Elsevier: Amsterdam, The Netherlands, 2022; pp. 397–415. [Google Scholar]
- Czech, M.P. Insulin Action and Resistance in Obesity and Type 2 Diabetes. Nat. Med. 2017, 23, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Lavie, C.J.; Blair, S.N. Obesity and Cardiovascular Disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and Nonalcoholic Fatty Liver Disease: From Pathophysiology to Therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Parnell, J.A.; Raman, M.; Rioux, K.P.; Reimer, R.A. The Potential Role of Prebiotic Fibre for Treatment and Management of Non-Alcoholic Fatty Liver Disease and Associated Obesity and Insulin Resistance. Liver Int. 2012, 32, 701–711. [Google Scholar] [CrossRef]
- Cerdó, T.; García-Santos, J.A.; Bermúdez, M.G.; Campoy, C. The Role of Probiotics and Prebiotics in the Prevention and Treatment of Obesity. Nutrients 2019, 11, 635. [Google Scholar] [CrossRef] [Green Version]
- Ben Othman, R.; Ben Amor, N.; Mahjoub, F.; Berriche, O.; El Ghali, C.; Gamoudi, A.; Jamoussi, H. A Clinical Trial about Effects of Prebiotic and Probiotic Supplementation on Weight Loss, Psychological Profile and Metabolic Parameters in Obese Subjects. Endocrinol. Diabetes Metab. 2023, 6, e402. [Google Scholar] [CrossRef]
- Wiciński, M.; Gębalski, J.; Gołębiewski, J.; Malinowski, B. Probiotics for the Treatment of Overweight and Obesity in Humans—A Review of Clinical Trials. Microorganisms 2020, 8, 1148. [Google Scholar] [CrossRef]
- Nicolucci, A.C.; Hume, M.P.; Martínez, I.; Mayengbam, S.; Walter, J.; Reimer, R.A. Prebiotics Reduce Body Fat and Alter Intestinal Microbiota in Children Who Are Overweight or With Obesity. Gastroenterology 2017, 153, 711–722. [Google Scholar] [CrossRef] [Green Version]
- She, J.; Wong, C.C.; Yu, J. Targeted Prebiotics Alter the Obese Gut Microbiome in Humans. Signal. Transduct. Target. Ther. 2021, 6, 363. [Google Scholar] [CrossRef] [PubMed]
- Bilal, M.; Ashraf, S.; Zhao, X. Dietary Component-Induced Inflammation and Its Amelioration by Prebiotics, Probiotics, and Synbiotics. Front. Nutr. 2022, 9, 931458. [Google Scholar] [CrossRef] [PubMed]
- Cristofori, F.; Dargenio, V.N.; Dargenio, C.; Miniello, V.L.; Barone, M.; Francavilla, R. Anti-Inflammatory and Immunomodulatory Effects of Probiotics in Gut Inflammation: A Door to the Body. Front. Immunol. 2021, 12, 578386. [Google Scholar] [CrossRef] [PubMed]
- Parmar, R.M.; Can, A.S. Dietary Approaches To Obesity Treatment. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Keyes, K.M.; Gary, D.; O’Malley, P.M.; Hamilton, A.; Schulenberg, J. Recent Increases in Depressive Symptoms among US Adolescents: Trends from 1991 to 2018. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 987–996. [Google Scholar] [CrossRef]
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef] [Green Version]
- Lipson, S.K.; Lattie, E.G.; Eisenberg, D. Increased Rates of Mental Health Service Utilization by U.S. College Students: 10-Year Population-Level Trends (2007–2017). Psychiatr. Serv. 2019, 70, 60–63. [Google Scholar] [CrossRef]
- Durrani, D.; Idrees, R.; Idrees, H.; Ellahi, A. Vitamin B6: A New Approach to Lowering Anxiety, and Depression? Ann. Med. Surg. 2022, 82, 104663. [Google Scholar] [CrossRef]
- Donoso, F.; Schverer, M.; Rea, K.; Pusceddu, M.M.; Roy, B.L.; Dinan, T.G.; Cryan, J.F.; Schellekens, H. Neurobiological Effects of Phospholipids in Vitro: Relevance to Stress-Related Disorders. Neurobiol. Stress 2020, 13, 100252. [Google Scholar] [CrossRef]
- Komori, T. The Effects of Phosphatidylserine and Omega-3 Fatty Acid-Containing Supplement on Late Life Depression. Ment. Illn. 2015, 7, 5647. [Google Scholar] [CrossRef]
- Konstantinos, F.; Heun, R. The Effects of Rhodiola Rosea Supplementation on Depression, Anxiety and Mood–A Systematic Review. Glob. Psychiatry 2020, 3, 72–82. [Google Scholar] [CrossRef] [Green Version]
- Trexler, E.T.; Smith-Ryan, A.E.; Stout, J.R.; Hoffman, J.R.; Wilborn, C.D.; Sale, C.; Kreider, R.B.; Jäger, R.; Earnest, C.P.; Bannock, L. International Society of Sports Nutrition Position Stand: Beta-Alanine. J. Int. Soc. Sport. Nutr. 2015, 12, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barkhidarian, B.; Khorshidi, M.; Shab-Bidar, S.; Hashemi, B. Effects of L-Citrulline Supplementation on Blood Pressure: A Systematic Review and Meta-Analysis. Avicenna J. Phytomed. 2019, 9, 10. [Google Scholar]
- Mousavi, S.M.; Shab-Bidar, S.; Kord-Varkaneh, H.; Khorshidi, M.; Djafarian, K. Effect of Alpha-Lipoic Acid Supplementation on Lipid Profile: A Systematic Review and Meta-Analysis of Controlled Clinical Trials. Nutrition 2019, 59, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Jackson, J.K.; Patterson, A.J.; MacDonald-Wicks, L.K.; Oldmeadow, C.; McEvoy, M.A. The Role of Inorganic Nitrate and Nitrite in Cardiovascular Disease Risk Factors: A Systematic Review and Meta-Analysis of Human Evidence. Nutr. Rev. 2018, 76, 348–371. [Google Scholar] [CrossRef]
- Anghelescu, I.-G.; Edwards, D.; Seifritz, E.; Kasper, S. Stress Management and the Role of Rhodiola Rosea: A Review. Int. J. Psychiatry Clin. Pract. 2018, 22, 242–252. [Google Scholar] [CrossRef] [Green Version]
- Cheah, K.L.; Norhayati, M.N.; Husniati Yaacob, L.; Abdul Rahman, R. Effect of Ashwagandha (Withania Somnifera) Extract on Sleep: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0257843. [Google Scholar] [CrossRef]
- Serban, M.-C.; Sahebkar, A.; Zanchetti, A.; Mikhailidis, D.P.; Howard, G.; Antal, D.; Andrica, F.; Ahmed, A.; Aronow, W.S.; Muntner, P. Effects of Quercetin on Blood Pressure: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2016, 5, e002713. [Google Scholar] [CrossRef] [Green Version]
- Hernandez-Garcia, D.; Granado-Serrano, A.B.; Martín-Gari, M.; Naudi, A.; Serrano, J.C. Efficacy of Panax Ginseng Supplementation on Blood Lipid Profile. A Meta-Analysis and Systematic Review of Clinical Randomized Trials. J. Ethnopharmacol. 2019, 243, 112090. [Google Scholar] [CrossRef]
- Kreider, R.B.; Stout, J.R. Creatine in Health and Disease. Nutrients 2021, 13, 447. [Google Scholar] [CrossRef]
- Belvoncikova, P.; Splichalova, P.; Videnska, P.; Gardlik, R. The Human Mycobiome: Colonization, Composition and the Role in Health and Disease. J. Fungi 2022, 8, 1046. [Google Scholar] [CrossRef]
- Cao, Z.; Sugimura, N.; Burgermeister, E.; Ebert, M.P.; Zuo, T.; Lan, P. The Gut Virome: A New Microbiome Component in Health and Disease. eBioMedicine 2022, 81, 104113. [Google Scholar] [CrossRef] [PubMed]
- Chibani, C.M.; Mahnert, A.; Borrel, G.; Almeida, A.; Werner, A.; Brugère, J.-F.; Gribaldo, S.; Finn, R.D.; Schmitz, R.A.; Moissl-Eichinger, C. A Catalogue of 1,167 Genomes from the Human Gut Archaeome. Nat. Microbiol. 2022, 7, 48–61. [Google Scholar] [CrossRef]
- Ghosh, T.S.; Shanahan, F.; O’Toole, P.W. The Gut Microbiome as a Modulator of Healthy Ageing. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 565–584. [Google Scholar] [CrossRef]
- Laforest-Lapointe, I.; Arrieta, M.-C. Microbial Eukaryotes: A Missing Link in Gut Microbiome Studies. mSystems 2018, 3, e00201-17. [Google Scholar] [CrossRef] [Green Version]
- Said, H.M.; Mohammed, Z.M. Intestinal Absorption of Water-Soluble Vitamins: An Update. Curr. Opin. Gastroenterol. 2006, 22, 140–146. [Google Scholar] [CrossRef]
- Leeming, E.R.; Johnson, A.J.; Spector, T.D.; Le Roy, C.I. Effect of Diet on the Gut Microbiota: Rethinking Intervention Duration. Nutrients 2019, 11, 2862. [Google Scholar] [CrossRef] [Green Version]
- Kumar, M.; Ji, B.; Babaei, P.; Das, P.; Lappa, D.; Ramakrishnan, G.; Fox, T.E.; Haque, R.; Petri, W.A.; Bäckhed, F.; et al. Gut Microbiota Dysbiosis Is Associated with Malnutrition and Reduced Plasma Amino Acid Levels: Lessons from Genome-Scale Metabolic Modeling. Metab. Eng. 2018, 49, 128–142. [Google Scholar] [CrossRef] [Green Version]
- Böhmer, C.; Bröer, A.; Munzinger, M.; Kowalczuk, S.; Rasko, J.E.J.; Lang, F.; Bröer, S. Characterization of Mouse Amino Acid Transporter B0AT1 (Slc6a19). Biochem. J. 2005, 389, 745–751. [Google Scholar] [CrossRef] [Green Version]
- Ferraris, R.P. Nutrient Transport, Regulation Of. In Encyclopedia of Gastroenterology; Johnson, L.R., Ed.; Elsevier: New York, NY, USA, 2004; pp. 754–759. ISBN 978-0-12-386860-2. [Google Scholar]
- Licata, A.; Zerbo, M.; Como, S.; Cammilleri, M.; Soresi, M.; Montalto, G.; Giannitrapani, L. The Role of Vitamin Deficiency in Liver Disease: To Supplement or Not Supplement? Nutrients 2021, 13, 4014. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Nikolova, D.; Bjelakovic, M.; Gluud, C. Vitamin D Supplementation for Chronic Liver Diseases in Adults. Cochrane Database Syst. Rev. 2017, 2017, CD011564. [Google Scholar] [CrossRef]
- Abdul-Muneer, P.M.; Alikunju, S.; Schuetz, H.; Szlachetka, A.M.; Ma, X.; Haorah, J. Impairment of Thiamine Transport at the GUT-BBB-AXIS Contributes to Wernicke’s Encephalopathy. Mol. Neurobiol. 2018, 55, 5937–5950. [Google Scholar] [CrossRef]
- Breton, J.; Galmiche, M.; Déchelotte, P. Dysbiotic Gut Bacteria in Obesity: An Overview of the Metabolic Mechanisms and Therapeutic Perspectives of Next-Generation Probiotics. Microorganisms 2022, 10, 452. [Google Scholar] [CrossRef]
- Kim, M.-H.; Yun, K.E.; Kim, J.; Park, E.; Chang, Y.; Ryu, S.; Kim, H.-L.; Kim, H.-N. Gut Microbiota and Metabolic Health among Overweight and Obese Individuals. Sci. Rep. 2020, 10, 19417. [Google Scholar] [CrossRef]
- Sanmiguel, C.; Gupta, A.; Mayer, E.A. Gut Microbiome and Obesity: A Plausible Explanation for Obesity. Curr. Obes. Rep. 2015, 4, 250–261. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Sun, H.; Jiang, F.; Shen, Y.; Li, X.; Hu, X.; Shen, X.; Wei, P. Alteration of the Gut Microbiota Associated with Childhood Obesity by 16S RRNA Gene Sequencing. PeerJ 2020, 8, e8317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaner, O.; Goday, A.; Park, Y.-M.; Lee, S.-H.; Magkos, F.; Shiow, S.-A.T.E.; Schröder, H. The Gut Microbiome Profile in Obesity: A Systematic Review. Int. J. Endocrinol. 2018, 2018, 4095789. [Google Scholar] [CrossRef]
- Pinart, M.; Dötsch, A.; Schlicht, K.; Laudes, M.; Bouwman, J.; Forslund, S.K.; Pischon, T.; Nimptsch, K. Gut Microbiome Composition in Obese and Non-Obese Persons: A Systematic Review and Meta-Analysis. Nutrients 2021, 14, 12. [Google Scholar] [CrossRef]
- Davis, C.D. The Gut Microbiome and Its Role in Obesity. Nutr. Today 2016, 51, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Aoun, A.; Darwish, F.; Hamod, N. The Influence of the Gut Microbiome on Obesity in Adults and the Role of Probiotics, Prebiotics, and Synbiotics for Weight Loss. Prev. Nutr. Food Sci. 2020, 25, 113–123. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Nutrients in Current RDA and DRI | Nutrients for Foundational Nutrition | ||
|---|---|---|---|
| Macromolecules | |||
|
| ||
| Vitamins and Minerals | |||
|
|
|
|
| Phytonutrients | |||
| |||
| Prebiotics and Probiotics | |||
| |||
| Functional Nutrients | |||
| |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Townsend, J.R.; Kirby, T.O.; Marshall, T.M.; Church, D.D.; Jajtner, A.R.; Esposito, R. Foundational Nutrition: Implications for Human Health. Nutrients 2023, 15, 2837. https://doi.org/10.3390/nu15132837
Townsend JR, Kirby TO, Marshall TM, Church DD, Jajtner AR, Esposito R. Foundational Nutrition: Implications for Human Health. Nutrients. 2023; 15(13):2837. https://doi.org/10.3390/nu15132837
Chicago/Turabian StyleTownsend, Jeremy R., Trevor O. Kirby, Tess M. Marshall, David D. Church, Adam R. Jajtner, and Ralph Esposito. 2023. "Foundational Nutrition: Implications for Human Health" Nutrients 15, no. 13: 2837. https://doi.org/10.3390/nu15132837