
Comparison of the Potential Relative Bioaccessibility of Zinc Supplements—In Vitro Studies

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Samples, Reagents, and Standards
2.2. Determination of Zn Content Using the FAAS Method
2.3. Bioaccessibility of Zn
2.4. Preparation of Dialysis Membranes
2.5. In Vitro Gastrointestinal Digestion Simulation
2.6. Mineralization
2.7. Method Validation
2.8. Evaluation of Dietary Supplements according to Polish and European Regulations and the Requirements of the United States Pharmacopoeia (USP 43-NF 38)
3. Results and Discussion
3.1. Bioaccessibility of Zn and Influence of Its Form
3.2. Realisation of Reference Intake of Zn
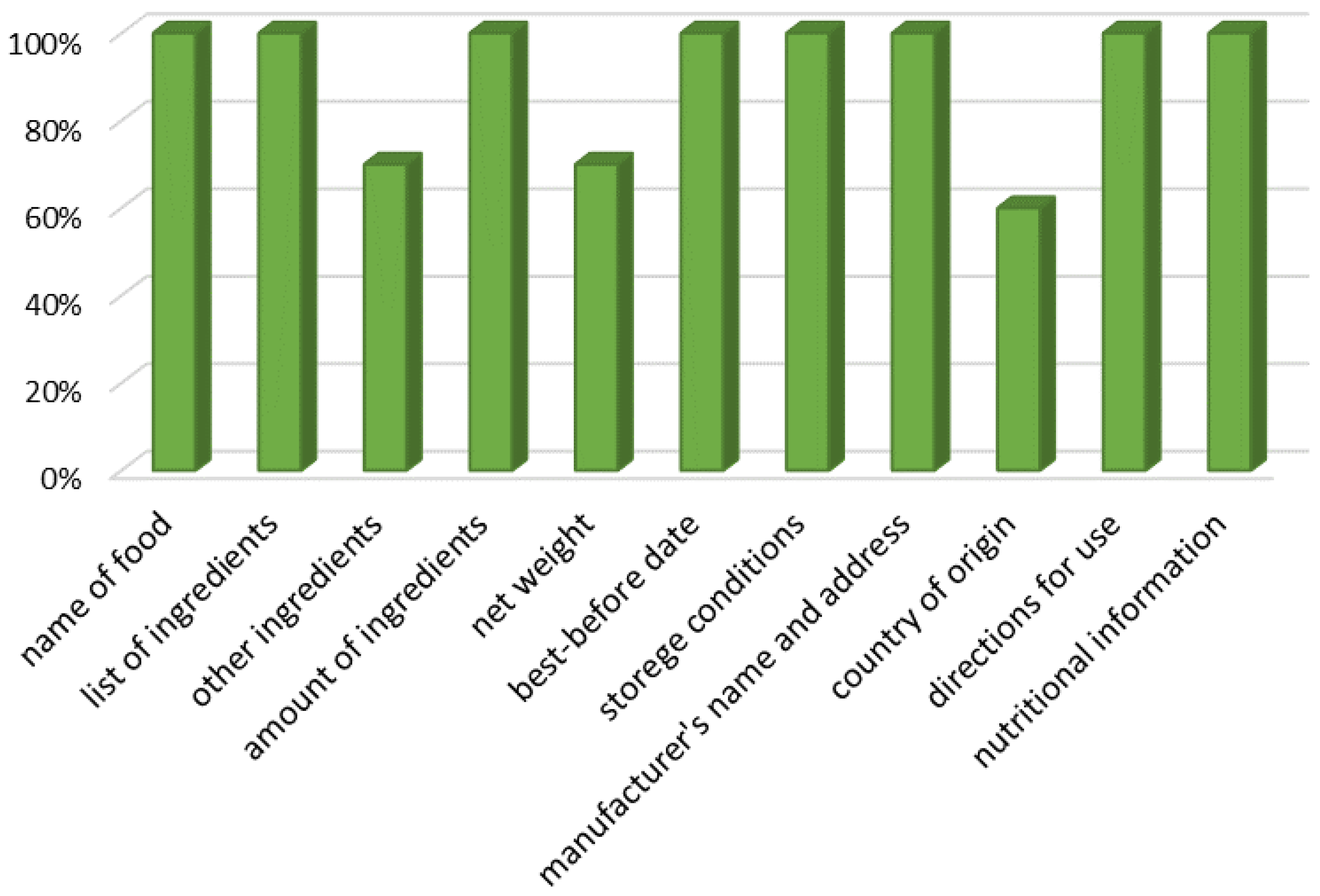
3.3. Assessment of the Manufacturer’s Declaration in Light of Current Legislation
3.4. Evaluation of Dietary Supplements against the Requirements of the FDA and the United States Pharmacopoeia (USP 43-NF 38)
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, K.H.; Riddell, L.J.; Nowson, C.A.; Booth, A.O.; Szymlek-Gay, E.A. Iron and zinc nutrition in the economically-developed world: A review. Nutrients 2003, 5, 3184–3211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maret, W. Zinc in cellular regulation: The nature and significance of “zinc signals”. Int. J. Mol. Sci. 2007, 18, 2285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rink, L.; Gabriel, P. Zinc and the immune system. Proc. Nutr. Soc. 2000, 59, 541–552. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.H.; Prasad, A.S.; Brewer, G.J.; Owyang, C. Zinc absorption in human small intestine. Am. J. Physiol. 1989, 256, G87–G91. [Google Scholar] [CrossRef] [PubMed]
- Maares, M.; Haase, H.A. Guide to human zinc absorption: General overview and recent advances of in vitro intestinal models. Nutrients 2020, 12, 762. [Google Scholar] [CrossRef] [Green Version]
- Davies, N.T. Studies on the absorption of zinc by rat intestine. Br. J. Nutr. 1980, 43, 189–203. [Google Scholar] [CrossRef] [Green Version]
- Antonson, D.L.; Barak, A.J.; Vanderhoof, J.A. Determination of the site of zinc absorption in rat small intestine. J. Nutr. 1979, 109, 142–147. [Google Scholar] [CrossRef]
- Steinhardt, H.J.; Adibi, S.A. Interaction between transport of zinc and other solutes in human intestine. Am. J. Physiol. 1984, 247, G176–G182. [Google Scholar] [CrossRef]
- Krebs, N.F. Overview of zinc absorption and excretion in the human gastrointestinal tract. J. Nutr. 2000, 130, 1374S–1377S. [Google Scholar] [CrossRef] [Green Version]
- Maret, W.; Sandstead, H.H. Zinc requirements and the risks and benefits of zinc supplementation. J. Trace Elem. Med. Biol. 2006, 20, 3–18. [Google Scholar] [CrossRef]
- World Health Organization (WHO); Food and Agricultural Organization. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004.
- Marreiro, D.D.N.; Cruz, K.J.C.; Morais, J.B.S.; Beserra, J.B.; Severo, J.S.; De Oliveira, A.R.S. Zinc and Oxidative Stress: Current Mechanisms. Antioxidants 2017, 6, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruz, M.; Carrasco, F. Zinc as a potential coadjuvant in therapy for type 2 diabetes. Food Nutr. Bull. 2013, 34, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Chasapis, C.T.; Loutsidou, A.C. Zinc and human health: An update. Arch. Toxicol. 2012, 86, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, M.; Olbert, M.; Wyszogrodzka, G.; Młyniec, K.; Librowski, T. Antioxidant and anti-inflammatory effects of zinc. Zinc-dependent NF-κB signaling. Inflammopharmacology 2017, 25, 11–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunt, J.R.; Beiseigel, J.M.; Johnson, L.K. Adaptation in human zinc absorption as influenced by dietary zinc and bioavailability. Am. J. Clin. Nutr. 2008, 87, 1336–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lönnerdal, B. Dietary factors influencing zinc absorption. J. Nutr. 2000, 130, 1378S–1383S. [Google Scholar] [CrossRef] [Green Version]
- FAO; WHO. Expert Consultation on Human Vitamin and Mineral Requirements, Vitamin and Mineral Requirements in Human Nutrition: Report of Joint FAO/WHO Expert Consolation, 2nd ed.; FAO: Bangkok, Thailand, 2004; p. 341.
- Morris, E.R.; Ellis, R. Usefulness of the dietary phytic acid/zinc molar ratio as an index of zinc bioavailability to rats and humans. Biol. Trace Elem. Res. 1989, 19, 107–117. [Google Scholar] [CrossRef]
- Turnlund, J.R.; King, J.C.; Keyes, W.R.; Gong, B.; Michel, M.C. A stable isotope study of zinc absorption in young men: Effects of phytate and alpha-cellulose. Am. J. Clin. Nutr. 1984, 40, 1071–1077. [Google Scholar] [CrossRef]
- Hunt, J.R. Bioavailability of iron, zinc, and other trace minerals from vegetarian diets. Am. J. Clin. Nutr. 2003, 78, 633S–639S. [Google Scholar] [CrossRef] [Green Version]
- Hambidge, K.M.; Miller, L.V.; Westcott, J.E.; Sheng, X.; Krebs, N.F. Zinc bioavailability and homeostasis. Am. J. Clin. Nutr. 2010, 91, 1478S–1483S. [Google Scholar] [CrossRef] [Green Version]
- International Zinc Nutrition Consultative Group; Brown, K.H.; Rivera, J.A.; Bhutta, Z.; Gibson, R.S.; King, J.C.; Lonnerdal, B.; Ruel, M.T.; Sandtrom, B.; Wasantwisut, E.; et al. International zinc nutrition consultative group (izincg) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr. Bull. 2004, 25, S99–S203. [Google Scholar]
- Haase, H.; Overbeck, S.; Rink, L. Zinc supplementation for the treatment or prevention of disease: Current status and future perspectives. Exp. Gerontol. 2008, 43, 394–408. [Google Scholar] [CrossRef]
- Trame, S.; Wessels, I.; Haase, H.; Rink, L. A short 18 items food frequency questionnaire biochemically validated to estimate zinc status in humans. J. Trace Elem. Med. Biol. 2018, 49, 285–295. [Google Scholar] [CrossRef]
- Etcheverry, P.; Grusak, M.A.; Fleige, L.E. Application of in vitro bioaccessibility and bioavailability methods for calcium, carotenoids, folate, iron, magnesium, polyphenols, zinc, and vitamins B6, B12, D, and E. Front. Physiol. 2012, 3, 317. [Google Scholar] [CrossRef] [Green Version]
- Chiplonkar, S.A.; Agte, V.V.; Tarwadi, K.V.; Kavadia, R. In vitro dialyzability using meal approach as an index for zinc and iron absorption in humans. Biol. Trace Elem. Res. 1999, 67, 249–256. [Google Scholar] [CrossRef]
- Dosh, R.H.; Essa, A.; Jordan-Mahy, N.; Sammon, C.; Le Maitre, C.L. Use of hydrogel scaffolds to develop an in vitro 3d culture model of human intestinal epithelium. Acta Biomater. 2017, 62, 128–143. [Google Scholar] [CrossRef]
- Langerholc, T.; Maragkoudakis, P.A.; Wollgast, J.; Gradisnik, L.; Cencic, A. Novel and established intestinal cell line models—An indispensable tool in food science and nutrition. Trends Food Sci. Technol. 2011, 22, S11–S20. [Google Scholar] [CrossRef]
- Brodkorb, A.; Egger, L.; Alminger, M.; Alvito, P.; Assunção, R.; Balance, S.; Bohn, T.; Bourlieu-Lacanal, C.; Boutrou, R.; Carrière, F.; et al. INFOGEST static in vitro simulation of gastrointestinal food digestion. Nat. Protoc. 2019, 14, 991–1014. [Google Scholar] [CrossRef]
- Grossblatt, N.; National Research Council (US) Committee on Methods of Producing Monoclonal Antibodies. Monoclonal Antibody Production; National Academies Press (US): Washington, DC, USA, 2019; pp. 22–23. Available online: https://www.ncbi.nlm.nih.gov/books/NBK100199/ (accessed on 7 May 2023).
- EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific Opinion on Dietary Reference Values for zinc. EFSA J. 2014, 12, 3844. [Google Scholar] [CrossRef] [Green Version]
- European Parliament. Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers. Off. J. Eur. Union 2011, 304, 18–46. Available online: https://eur-lex.europa.eu/legal-content/EN/ALL/?uri=CELEX:32011R1169 (accessed on 7 May 2023).
- Dziennik, U. Ustawa z dnia 25 sierpnia 2006 r. o bezpieczeństwie żywności i żywienia (z późn. zm.). In 2006 Nr 171 Poz. 1225; ISAP: Warsaw, Poland, 2006. [Google Scholar]
- ISAP. Rozporządzenie Ministra Zdrowia z dnia 9 października 2007 r. w sprawie składu oraz oznakowania suplementów diety. In 2007 Nr 196 Poz. 1425; ISAP: Warsaw, Poland, 2007. [Google Scholar]
- The United States Pharmacopeial Convention. Weight variation of dietary supplements. In United States Pharmacopeia and National Formulary (USP 43-NF 38); United States Pharmacopeial Convention: Rockville, MD, USA, 2021. [Google Scholar]
- FDA. Dietary Supplement Health and Education Act of 1994; FDA: Montgomery, MD, USA, 1994.
- Overgaard, A.B.A.; Hojsted, J.; Hansen, R.; Moller-Sonnergaard, J.; Christrup, L.L. Patients’ evaluation of shape, size and colour of solid dosage forms. Pharm. World Sci. 2001, 23, 185–188. [Google Scholar] [CrossRef]
- Schmidt, L.; Figueroa, J.A.L.; Vecchia, P.D.; Duarte, F.A.; Mello, P.A.; Caruso, J.A.; Flores, E.M. Bioavailability of Hg and Se from seafood after culinary treatments. Microchem. J. 2018, 139, 363–371. [Google Scholar] [CrossRef]
- Domínguez-González, R.; Romarís-Hortas, V.; García-Sartal, C.; Moreda-Piñeiro, A.; del Carmen Barciela-Alonso, M.; Bermejo-Barrera, P. Evaluation of an in vitro method to estimate trace elements bioavailability in edible seaweeds. Talanta 2010, 82, 1668–1673. [Google Scholar] [CrossRef]
- Alnaimat, A.S.; Barciela-Alonso, M.C.; Herbello-Hermelo, P.; Domínguez-González, R.; Bermejo-Barrera, P. In vitro assessment of major and trace element bioaccessibility in tea samples. Talanta 2021, 225, 122083. [Google Scholar] [CrossRef]
- Brzezicha-Cirocka, J.; Grembecka, M.; Szefer, P. Monitoring of essential and heavy metals in green tea from different geographical origins. Environ. Monit. Assess. 2016, 188, 183. [Google Scholar] [CrossRef] [Green Version]
- Konieczka, P.; Namieśnik, J. Quality Assurance and Quality Control in the Analytical Chemical Laboratory: A Practical Approach; CRC Press—Taylor & Francis Group: Boca Raton, FL, USA, 2009. [Google Scholar]
- Sandström, B.; Davidsson, L.; Cederblad, A.; Lönnerdal, B. Oral iron, dietary ligands and zinc absorption. J. Nutr. 1985, 115, 411–414. [Google Scholar] [CrossRef]
- Davies, N.T.; Olpin, S.E. Studies on the phytate:zinc molar contents in diets as a determinant of Zn availability to young rats. Br. J. Nutr. 1979, 41, 590–603. [Google Scholar] [CrossRef] [Green Version]
- Wegmüller, R.; Tay, F.; Zeder, C.; Brnic, M.; Hurrell, R.F. Zinc absorption by young adults from supplemental zinc citrate is comparable with that from zinc gluconate and higher than from zinc oxide. J. Nutr. 2014, 144, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Guillem, A.; Alegría, A.; Barberá, R.; Farré, R.; Lagarda, M.J.; Clemente, G. In vitro dialyzability of zinc from different salts used in the supplementation of infant formulas. Biol. Trace Elem. Res. 2000, 75, 11–19. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, C.; Wu, W.; Qu, Y.; Zhang, W.; Li, D.; Zhu, L.; Gao, F.; Wu, B.; Zhang, L.; et al. Organic zinc with moderate chelation strength enhances zinc absorption in the small intestine and expression of related transporters in the duodenum of broilers. Front Physiol. 2022, 13, 952941. [Google Scholar] [CrossRef]
- Schlegel, P.; Windisch, W. Bioavailability of zinc glycinate in comparison with zinc sulphate in the presence of dietary phytate in an animal model with 65Zn labelled rats. J. Anim. Physiol. Anim. Nutr. 2006, 90, 216–222. [Google Scholar] [CrossRef]
- Sapota, A.; Daragó, A.; Skrzypińska-Gawrysiak, M.; Nasiadek, M.; Klimczak, M.; Kilanowicz, A. The bioavailability of different zinc compounds used as human dietary supplements in rat prostate: A comparative study. Biometals 2014, 27, 495–505. [Google Scholar] [CrossRef]
- Roohani, N.; Hurrell, R.; Kelishadi, R.; Schulin, R. Zinc and its importance for human health: An integrative review. J. Res. Med. Sci. 2013, 18, 144–157. [Google Scholar]
- Müller, O.; Becher, H.; van Zweeden, A.B.; Ye, Y.; Diallo, D.A.; Konate, A.T.; Gbangou, A.; Kouyate, B.; Garenne, M. Effect of zinc supplementation on malaria and other causes of morbidity in west African children: Randomised double blind placebo controlled trial. BMJ 2001, 322, 1567. [Google Scholar] [CrossRef] [Green Version]
- Shankar, A.H.; Genton, B.; Baisor, M.; Paino, J.; Tamja, S.; Adiguma, T.; Wu, L.; Rare, L.; Bannon, D.; Tielsch, J.M.; et al. The influence of zinc supplementation on morbidity due to Plasmodium falciparum: A randomized trial in preschool children in Papua New Guinea. Am. J. Trop. Med. Hyg. 2000, 62, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Tabatabaeizadeh, S.A. Zinc supplementation and COVID-19 mortality: A meta-analysis. Eur. J. Med. Res. 2022, 27, 70. [Google Scholar] [CrossRef]
- Younes, M.; Aquilina, G.; Castle, L.; Engel, K.; Fowler, P.; Fernandez, M.J.F.; Fürst, P.; Gundert-Remy, U.; Gürtler, R.; Husøy, T.; et al. Safety assessment of titanium dioxide (E171) as a food additive. EFSA J. 2021, 19, 6585. [Google Scholar]
- Channer, K.S.; Virjee, J.P. The effect of size and shape of tablets on their esophageal transit. J. Clin. Pharmacol. 1986, 26, 141–146. [Google Scholar] [CrossRef]
- Kelly, J.; D’Cruz, G.; Wright, D. Patients with dysphagia: Experiences of taking medication. J. Adv. Nurs. 2010, 66, 82–91. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pharmaceutical Form | Zn Content Declared by Producer | Chemical Form | Dosage | |
|---|---|---|---|---|
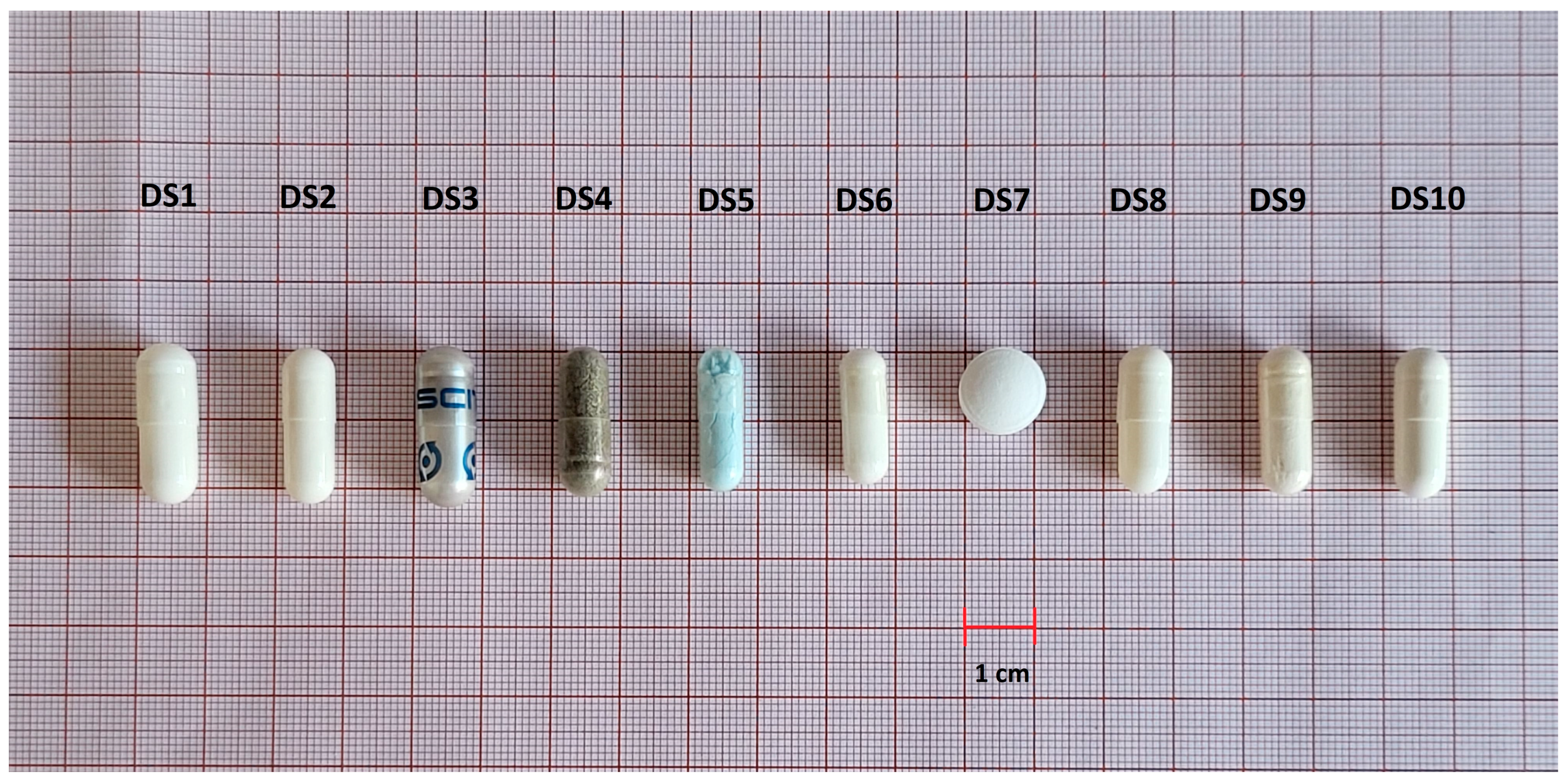
| DS1 | Capsules | 25 mg | zinc bisglycinate | 1 capsule/day |
| DS2 | Capsules | 10 mg | zinc bisglycinate | 1 capsule/day |
| DS3 | Capsules | 30 mg | zinc sulfate | 2 capsules/day |
| DS4 | Capsules | 15 mg | zinc picolinate | 1 capsule/day |
| DS5 | Capsules | 25 mg | zinc citrate | 1 capsule/day |
| DS6 | Capsules | 30 mg | zinc methionine | 1 capsule/day |
| DS7 | Tablets | 24.6 mg | zinc gluconate | 1 tablet/day |
| DS8 | Capsules | 15 mg | zinc gluconate | 1 capsule/day |
| DS9 | Capsules | 30 mg | zinc bisglycinate | 1 capsule/day |
| DS10 | Capsules | 15 mg | zinc bisglycinate | 1 capsule/day |
| Code | Fraction | Average Content [mg/Capsule] (Range) | Total Content a [mg] | Potential Relative Bioaccessibility [%] | Percentage of UL (for 1 Capsule/Tablet) b [%] |
|---|---|---|---|---|---|
| DS1 | A | 28.4 ± 4.90 (21.8–33.6) | 30.8 | 7.86 | 123 |
| B | 2.42 ± 0.008 (2.42–2.43) | ||||
| DS2 | A | 10.2 ± 1.11 (8.81–11.5) | 11.3 | 9.38 | 45.2 |
| B | 1.06 ± 0.24 (0.80–1.38) | ||||
| DS3 | A | 16.6 ± 1.64 (14.3–18.2) | 16.8 | 1.13 | 67.2 |
| B | 0.19 ± 0.12 (0.05–0.33) | ||||
| DS4 | A | 23.3 ± 2.29 (20.5–26.1) | 24.1 | 3.15 | 96.4 |
| B | 0.76 ± 0.05 (0.72–0.83) | ||||
| DS5 | A | 35.9 ± 10.8 (25.1–46.7) | 36.6 | 1.99 | 146 |
| B | 0.73 ± 0.01 (0.72–0.75) | ||||
| DS6 | A | 30.0 ± 0.67 (29.4–30.9) | 31.1 | 3.38 | 124 |
| B | 1.05 ± 0.003 (1.04–1.05) | ||||
| DS7 | A | 32.2 ± 4.03 (26.7–36.0) | 33.7 | 4.48 | 135 |
| B | 1.51 ± 0.002 (1.50–1.51) | ||||
| DS8 | A | 12.6 ± 1.09 (11.7–14.1) | 13.4 | 6.19 | 53.6 |
| B | 0.83 ± 0.13 (0.65–0.96) | ||||
| DS9 | A | 31.7 ± 0.77 (31.0–32.8) | 33.6 | 5.77 | 134 |
| B | 1.94 ± 0.10 (1.82–2.05) | ||||
| DS10 | A | 16.2 ± 0.71 (15.2–16.8) | 17.3 | 6.59 | 69.2 |
| B | 1.14 ± 0.13 (0.97–1.30) |
| Code | Length ± SD [mm] | Width ± SD [mm] | Depth ± SD [mm] | L + W + D 1 | Shape | FDA Recommendation 2 |
|---|---|---|---|---|---|---|
| DS1 | 23.1 ± 0.05 | 8.40 ± 0.08 | 8.40 ± 0.08 | 39.9 | cylindrical capsule | acceptable |
| DS2 | 22.0 ± 0.36 | 7.53 ± 0.03 | 7.53 ± 0.03 | 37.1 | cylindrical capsule | acceptable |
| DS3 | 23.3 ± 0.10 | 8.46 ± 0.06 | 8.46 ± 0.06 | 40.2 | cylindrical capsule | acceptable |
| DS4 | 21.6 ± 0.17 | 7.63 ± 0.02 | 7.63 ± 0.02 | 36.9 | cylindrical capsule | acceptable |
| DS5 | 20.51 ± 0.53 | 6.84 ± 0.05 | 6.84 ± 0.05 | 34.2 | cylindrical capsule | acceptable |
| DS6 | 19.52 ± 0.32 | 6.90 ± 0.05 | 6.90 ± 0.05 | 33.3 | cylindrical capsule | acceptable |
| DS7 | 12.3 ± 0.02 | 12.3 ± 0.02 | 6.83 ± 0.16 | 31.4 | round tablet | acceptable |
| DS8 | 21.09 ± 0.10 | 7.57 ± 0.04 | 7.57 ± 0.04 | 36.2 | cylindrical capsule | acceptable |
| DS9 | 21.13 ± 0.12 | 7.61 ± 0.03 | 7.61 ± 0.03 | 36.4 | cylindrical capsule | acceptable |
| DS10 | 21.52 ± 0.05 | 7.56 ± 0.06 | 7.56 ± 0.06 | 36.6 | cylindrical capsule | acceptable |
| Code | Average Weight ± SD [mg] | Declared Weight [mg] | Percentage of Declaration [%] | Min 1–Max 2 [%] | Pharmacopeia Criteria |
|---|---|---|---|---|---|
| DS1 | 507 ± 6.97 | 500 | 101 | 98–102 | passed |
| DS2 | 383 ± 8.59 | NA | ND | 95–105 | passed |
| DS3 | 846 ± 44.2 | NA | ND | 94–110 | passed |
| DS4 | 504 ± 13.3 | NA | ND | 95–105 | passed |
| DS5 | 428 ± 13.7 | NA | ND | 94–105 | passed |
| DS6 | 458 ± 10.0 | NA | ND | 96–105 | passed |
| DS7 | 649 ± 48.8 | NA | ND | 87–120 | failed |
| DS8 | 234 ± 9.70 | 200 | 117 | 93–109 | passed |
| DS9 | 500 ± 8.36 | ND | ND | 96–104 | passed |
| DS10 | 520 ± 3.97 | 490 | 106 | 99–101 | passed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ośko, J.; Pierlejewska, W.; Grembecka, M. Comparison of the Potential Relative Bioaccessibility of Zinc Supplements—In Vitro Studies. Nutrients 2023, 15, 2813. https://doi.org/10.3390/nu15122813
Ośko J, Pierlejewska W, Grembecka M. Comparison of the Potential Relative Bioaccessibility of Zinc Supplements—In Vitro Studies. Nutrients. 2023; 15(12):2813. https://doi.org/10.3390/nu15122813
Chicago/Turabian StyleOśko, Justyna, Wiktoria Pierlejewska, and Małgorzata Grembecka. 2023. "Comparison of the Potential Relative Bioaccessibility of Zinc Supplements—In Vitro Studies" Nutrients 15, no. 12: 2813. https://doi.org/10.3390/nu15122813