

Is Health Education among the Decisive Factors for the Diet Quality of Pregnant Women in Poland?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Design and Sample
2.2. Analysis
3. Results
3.1. Group Characteristics
3.2. Diet Characteristics
3.3. Food Determinants of Diet Quality
3.4. Sociodemographic and Maternal Lifestyle-Related Determinants of Diet Quality
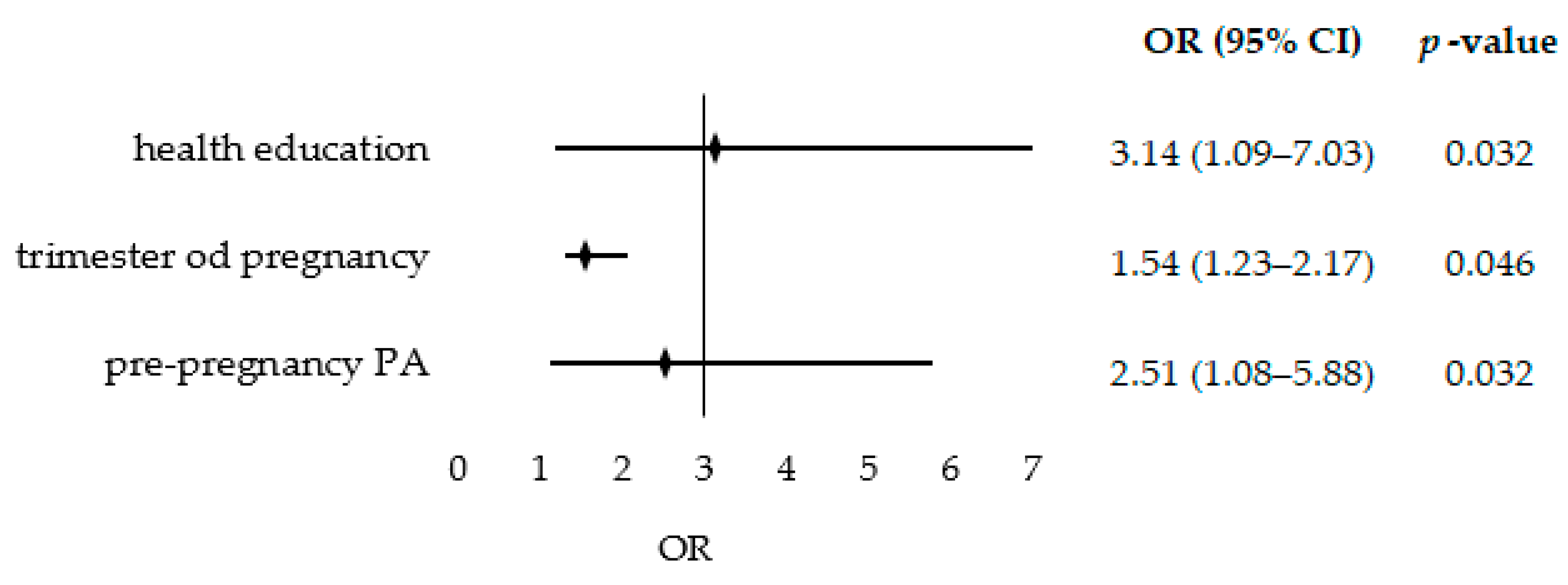
3.5. The Odds Ratio of Higher-Quality Diet
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forbes, L.E.; Graham, J.E.; Berglund, C.; Bell, R.C. Dietary change during pregnancy and women’s reasons for change. Nutrients 2018, 10, 1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, C.L.; Lombard, C.B.; Teede, H.J. Understanding health behaviours in a cohort of pregnant women at risk of gestational diabetes mellitus: An observational study. BJOG Int. J. Gynaecol. Obstet. 2012, 119, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Olander, E.K.; Smith, D.M.; Darwin, Z. Health behaviour and pregnancy: A time for change. J. Reprod. Infant. Psychol. 2018, 36, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Chia, A.R.; Chen, L.W.; Lai, J.S.; Wong, C.H.; Neelakantan, N.; van Dam, R.M.; Chong, M.F. Maternal Dietary Patterns and Birth Outcomes: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 685–695. [Google Scholar] [CrossRef] [Green Version]
- Teruel Camargo, J.; Taylor, M.K.; Gajewski, B.J.; Carlson, S.E.; Sullivan, D.K.; Gibbs, H.D. Higher Diet Quality in Latina Women during Pregnancy May Be Associated with Sociodemographic Factors. Int. J. Environ. Res. Public Health 2022, 19, 13895. [Google Scholar] [CrossRef]
- Wesołowska, E.; Jankowska, A.; Trafalska, E.; Kałużny, P.; Grzesiak, M.; Dominowska, J.; Hanke, W.; Calamandrei, G.; Polańska, K. Sociodemographic, Lifestyle, Environmental and Pregnancy-Related Determinants of Dietary Patterns during Pregnancy. Int. J. Environ. Res. Public Health 2019, 16, 754. [Google Scholar] [CrossRef] [Green Version]
- Cucó, G.; Fernández-Ballart, J.; Sala, J.; Viladrich, C.; Iranzo, R.; Vila, J.; Arija, V. Dietary patterns and associated lifestyles in preconception, pregnancy and postpartum. Eur. J. Clin. Nutr. 2006, 60, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Laraia, B.A.; Bodnar, L.M.; Siega-Riz, A.M. Pregravid body mass index is negatively associated with diet quality during pregnancy. Public Health Nutr. 2007, 10, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Gollenberg, A.; Pekow, P.; Markenson, G.; Tucker, K.L.; Chasan-Taber, L. Dietary behaviors, physical activity, and cigarette smoking among pregnant Puerto Rican women. Am. J. Clin. Nutr. 2008, 87, 1844–1851. [Google Scholar] [CrossRef] [Green Version]
- Northstone, K.; Emmett, P.; Rogers, I. Dietary patterns in pregnancy and associations with socio-demographic and lifestyle factors. Eur. J. Clin. Nutr. 2008, 62, 471–479. [Google Scholar] [CrossRef]
- Fowler, J.K.; Evers, S.E.; Campbell, M.K. Inadequate dietary intakes among pregnant women. Can. J. Diet. Pract. Res. 2012, 73, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Nash, D.M.; Gilliland, J.A.; Evers, S.E.; Wilk, P.; Campbell, M.K. Determinants of diet quality in pregnancy: Sociodemographic, pregnancy-specific, and food environment influences. J. Nutr. Educ. Behav. 2013, 45, 627–634. [Google Scholar] [CrossRef]
- Central Statistical Office. Percentage of People Aged 15 and Over by Body Mass Index (BMI). 2020. Available online: https://stat.gov.pl/obszary-tematyczne/zdrowie/zdrowie/odsetek-osob-w-wieku-powyzej-15-lat-wedlug-indeksu-masy-ciala-bmi,23,1.html (accessed on 21 May 2023). (In Polish)
- Deierlein, A.L.; Ghassabian, A.; Kahn, L.G.; Afanasyeva, Y.; Mehta-Lee, S.S.; Brubaker, S.G.; Trasande, L. Dietary Quality and Sociodemographic and Health Behavior Characteristics Among Pregnant Women Participating in the New York University Children’s Health and Environment Study. Front. Nutr. 2021, 8, 639425. [Google Scholar] [CrossRef] [PubMed]
- Antosiak-Cyrak, K.Z.; Demuth, A. A study of physical activity levels of pregnant women using the Polish version of Pregnancy Physical Activity Questionnaire (PPAQ-Pl). Ginekol. Pol. 2019, 90, 250–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pick, M.E.; Edwards, M.; Moreau, D.; Ryan, E.A. Assessment of diet quality in pregnant women using the Healthy Eating Index. J. Am. Diet. Assoc. 2005, 105, 240–246. [Google Scholar] [CrossRef]
- Rojhani, A.; Ouyang, P.; Gullon-Rivera, A.; Dale, T.M. Dietary Quality of Pregnant Women Participating in the Special Supplemental Nutrition Program for Women, Infants, and Children. Int. J. Environ. Res. Public Health 2021, 18, 8370. [Google Scholar] [CrossRef]
- Walsh, J.M.; McAuliffe, F.M. Impact of maternal nutrition on pregnancy outcome—Does it matter what pregnant women eat? Best. Pract. Res. Clin. Obs. Gynaecol. 2015, 29, 63–78. [Google Scholar] [CrossRef]
- Yamashita, T.; Roces, R.E.D.; Ladines-Llave, C.; Tuliao, M.T.R.; Yamada, C.; Tanaka, T.; Shimazawa, K.; Iwamoto, S.; Matsuo, H. Dietary Intake Quality Is Affected by Knowledge and Dietary Intake Frequency among Pregnant Women in Muntinlupa, Philippines: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12306. [Google Scholar] [CrossRef]
- Kebbe, M.; Flanagan, E.M.; Sparks, J.R.; Redman, L.M. Eating Behaviors and Dietary Patterns of Women during Pregnancy: Optimizing the Universal ‘Teachable Moment’. Nutrients 2021, 13, 3298. [Google Scholar] [CrossRef]
- Ministry of Education and Science. Health Education. 2013. Available online: https://www.gov.pl/web/edukacja-i-nauka/edukacja-zdrowotna (accessed on 21 May 2023). (In Polish)
- Wolny, B. Edukacja Zdrowotna w Szkole. Poradnik dla Dyrektorów Szkół i Nauczycieli; Ośrodek Rozwoju Edukacji: Warszawa, Poland, 2019. [Google Scholar]
- Bloomingdale, A.; Guthrie, L.B.; Price, S.; Wright, R.O.; Platek, D.; Haines, J.; Oken, E. A qualitative study of fish consumption during pregnancy. Am. J. Clin. Nutr. 2010, 92, 1234–1240. [Google Scholar] [CrossRef] [Green Version]
- De Jersey, S.J.; Nicholson, J.M.; Callaway, L.K.; Daniels, L.A. An observational study of nutrition and physical activity behaviours, knowledge, and advice in pregnancy. BMC Pregnancy Childbirth 2013, 13, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woynarowska, B. Edukacja zdrowotna w szkole w Polsce. Zmiany w ostatnich dekadach i nowa propozycja. Probl. Hig. Epidemiol. 2008, 89, 445–452. [Google Scholar]
- Education Law. Compulsory Schooling. Dz.U.2023.900 [In Polish]. 2023. Available online: https://sip.lex.pl/akty-prawne/dzu-dziennik-ustaw/prawo-oswiatowe-18558680/art-35?_ga=2.42963813.1518331979.1684747071-432803955.1684747070 (accessed on 21 May 2023).
- Tejada, J.J.; Punzalan, J.R.B. On the misuse of Slovin’s formula. Philipp. Stat. 2012, 61, 129–136. [Google Scholar]
- Jeżewska-Zychowicz, M.; Gawecki, J.; Wadolowska, L.; Czarnocinska, J.; Galinski, G.; Kollajtis Dolowy, A.; Roszkowski, W.; Wawrzyniak, A.; Przybylowicz, K.; Stasiewicz, B.; et al. KomPAN® Dietary Habits and Nutrition Beliefs Questionnaire and the Manual for Developing of Nutritional Data; Gawecki, J., Ed.; The Committee of Human Nutrition, Polish Academy of Sciences: Olsztyn, Poland, 2020; Available online: http://www.knozc.pan.pl/ (accessed on 20 January 2023).
- Krzepota, J.; Sadowska, D. Kwestionariusz aktywności fizycznej kobiet w ciąży—Wersja polska (PPAQ-PL). Med. Ogólna Nauk. Zdrowiu 2017, 23, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sport. Exerc. 2000, 32 (Suppl. S9), 498–504. [Google Scholar] [CrossRef] [Green Version]
- Stanisz, A. Basics of korrelation and regression. In Accessible Course of Statistics with Application of Statistica PL Using Medical Examples; Basics Statistics; StatSoft: Kraków, Poland, 2007; Volume 1, pp. 203–219. [Google Scholar]
- Szwajcer, E.; Hiddink, G.J.; Maas, L.; Koelen, M.; van Woerkum, C. Nutrition awareness before and throughout different trimesters in pregnancy: A quantitative study among dutch women. Fam. Pract. 2012, 29, i82–i88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Blondin, J.H.; LoGiudice, J.A. Pregnant women’s knowledge and awareness of nutrition. Appl. Nurs. Res. 2018, 39, 167–174. [Google Scholar] [CrossRef]
- Lee, A.; Newton, M.; Radcliffe, J.; Belski, R. Pregnancy nutrition knowledge and experiences of pregnant women and antenatal care clinicians: A mixed methods approach. Women Birth 2018, 31, 269–277. [Google Scholar] [CrossRef]
- Lucas, C.; Charlton, K.E.; Yeatman, H. Nutrition advice during pregnancy: Do women receive it and can health professionals provide it? Matern. Child. Health 2014, 18, 2465–2478. [Google Scholar] [CrossRef] [Green Version]
- Doyle, I.M.; Borrmann, B.; Grosser, A.; Razum, O.; Spallek, J. Determinants of dietary patterns and diet quality during pregnancy: A systematic review with narrative synthesis. Public Health Nutr. 2017, 20, 1009–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arkkola, T.; Uusitalo, U.; Kronberg-Kippilä, C.; Männistö, S.; Virtanen, M.; Kenward, M.G.; Veijola, R.; Knip, M.; Ovaskainen, M.L.; Virtanen, S.M. Seven distinct dietary patterns identified among pregnant Finnish women—Associations with nutrient intake and sociodemographic factors. Public Health Nutr. 2008, 11, 176–182. [Google Scholar] [CrossRef] [Green Version]
- Bojar, I.; Owoc, A.; Humeniuk, E.; Wierzba, W.; Fronczak, A. Inappropriate consumption of vitamins and minerals by pregnant women in Poland. Ann. Agric. Environ. Med. 2012, 19, 263–266. [Google Scholar] [PubMed]
- Jardí, C.; Aparicio, E.; Bedmar, C.; Aranda, N.; Abajo, S.; March, G.; Basora, J.; Arija, V.; Study Group, T.E. Food Consumption during Pregnancy and Post-Partum. ECLIPSES Study. Nutrients 2019, 14, 2447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodnar, L.M.; Simhan, H.N.; Parker, C.B.; Meier, H.; Mercer, B.M.; Grobman, W.A.; Haas, D.M.; Wing, D.A.; Hoffman, M.K.; Parry, S.; et al. Racial or ethnic and socioeconomic inequalities in adherence to national dietary guidance in a large cohort of US pregnant women. J. Acad. Nutr. Diet. 2017, 117, 867–877. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, L.M.; Siega-Riz, A.M. A diet quality index for pregnancy detects variation in diet and differences by sociodemographic factors. Public Health Nutr. 2002, 5, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Delbaere, I.; Verstraelen, H.; Goetgeluk, S.; Martens, G.; De Backer, G.; Temmerman, M. Pregnancy outcome in primiparae of advanced maternal age. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 135, 41–46. [Google Scholar] [CrossRef]
- Emond, J.A.; Karagas, M.R.; Baker, E.R.; Gilbert-Diamond, D. Better diet quality during pregnancy is associated with a reduced likelihood of an infant born small for gestational age: An analysis of the prospective new hampshire birth cohort study. J. Nutr. 2018, 148, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Dietary quality during pregnancy varies by maternal characteristics in project viva: A US cohort. J. Am. Diet. Assoc. 2009, 109, 1004–1011. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, A.L.; Kaar, J.L.; Crume, T.L.; Starling, A.P.; Siega-Riz, A.M.; Ringham, B.M.; Glueck, D.H.; Norris, J.M.; A Barbour, L.; Friedman, J.E.; et al. Maternal diet quality in pregnancy and neonatal adiposity: The healthy start study. Int. J. Obes. 2016, 40, 1056–1062. [Google Scholar] [CrossRef] [Green Version]
- Thomson, J.L.; Tussing-Humphreys, L.M.; Goodman, M.H.; Olender, S. Baseline demographic, anthropometric, psychosocial, and behavioral characteristics of rural, Southern women in early pregnancy. Matern. Child. Health J. 2016, 20, 1980–1988. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.A.; McAuliffe, F.M. Maternal dietary patterns and associated nutrient intakes during each trimester of pregnancy. Public Health Nutr. 2013, 16, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Gómez, E.; Luque-Vara, T.; Moya-Fernández, P.J.; López-Olivares, M.; Gallardo-Vigil, M.Á.; Enrique-Mirón, C. Factors Influencing Dietary Patterns during Pregnancy in a Culturally Diverse Society. Nutrients 2020, 23, 3242. [Google Scholar] [CrossRef] [PubMed]
- Aittasalo, M.; Pasanen, M.; Fogelholm, M.; Kinnunen, T.I.; Ojala, K.; Luoto, R. Physical activity counseling in maternity and child health care—A controlled trial. BMC Womens Health 2008, 8, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skouteris, H.; Hartley-Clark, L.; McCabe, M.; Milgrom, J.; Kent, B.; Herring, S.J.; Gale, J. Preventing excessive gestational weight gain: A systematic review of interventions. Obes. Rev. 2010, 11, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi-Khoigani, M.; Baghiani Moghadam, M.H.; Nadjarzadeh, A.; Mardanian, F.; Fallahzadeh, H.; Mazloomy-Mahmoodabad, S. Impact of Nutrition Education in Improving Dietary Pattern During Pregnancy Based on Pender’s Health Promotion Model: A Randomized Clinical Trial. Iran. J. Nurs. Midwifery Res. 2018, 23, 18–25. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Healthy Diet; World Health Organization: Geneva, Switzerland, 2018. Available online: https://www.who.int/publications/m/item/healthy-diet-factsheet394 (accessed on 20 March 2023).
- IFN—Institute of Food and Nutrition, Pyramid of Healthy Nutrition and Physical Activity for Adults. 2019. Available online: https://ncez.pzh.gov.pl/aktywnosc-fizyczna/piramida-zdrowego-zywienia-i-aktywnosci-fizycznej-dla-osob-doroslych-2/ (accessed on 26 April 2023). (In Polish)
- Skreden, M.; Bere, E.; Sagedal, L.R.; Vistad, I.; Øverby, N.C. Changes in fruit and vegetable consumption habits from pre-pregnancy to early pregnancy among Norwegian women. BMC Pregnancy Childbirth 2017, 17, 107. [Google Scholar] [CrossRef] [Green Version]
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef] [Green Version]
- Prasadi, N.V.P.; Joye, I.J. Dietary Fibre from Whole Grains and Their Benefits on Metabolic Health. Nutrients 2020, 12, 3045. [Google Scholar] [CrossRef]
- Tosh, S.M.; Bordenave, N. Emerging science on benefits of whole grain oat and barley and their soluble dietary fibers for heart health, glycemic response, and gut microbiota. Nutr. Rev. 2020, 78, 13–20. [Google Scholar] [CrossRef]
- Semba, R.D.; Ramsing, R.; Rahman, N.; Kraemer, K.; Bloem, M.W. Legumes as a sustainable source of protein in human diets. Glob. Food Sec. 2021, 28, 100520. [Google Scholar] [CrossRef]
- Miyahira, R.F.; Lopes, J.O.; Antunes, A.E.C. The Use of Sprouts to Improve the Nutritional Value of Food Products: A Brief Review. Plant. Foods Hum. Nutr. 2021, 76, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Cater, M.; Gaitan, A.; Drewery, M.; Gravois, R.; Lammi-Keffe, C.J. Awareness of Listeria and high-risk food consumption behavior among pregnant women in Louisiana. Food Control. 2017, 76, 62–66. [Google Scholar] [CrossRef]
- Barlik, M.; Seremak-Mrozikiewicz, A.; Drews, K. Listerioza w ciąży—Opis przypadku. Ginekol. Pol. 2014, 85, 309–313. [Google Scholar]
- Bauer, P.W.; Broman, C.L.; Pivarnik, J.M. Exercise and pregnancy knowledge among healthcare providers. J. Womens Health 2010, 19, 335–341. [Google Scholar] [CrossRef]
- Evenson, K.R.; Pompeii, L.A. Obstetrician practice patterns and recommendations for physical activity during pregnancy. J. Womens Health 2010, 19, 1733–1740. [Google Scholar] [CrossRef]
- Burdick, L.; Mielke, G.I.; Parra, D.C.; Gomes, G.; Florindo, A.; Bracco, M.; Lobelo, F.; Simoes, E.J.; Pratt, M.; Ramos, L.R.; et al. Physicians’, nurses’ and community health workers’ knowledge about physical activity in Brazil: A cross-sectional study. Prev. Med. Rep. 2015, 2, 467–472. [Google Scholar] [CrossRef] [Green Version]
- Wise, N.J.; Arcamone, A.A. Survey of adolescent views of healthy eating during pregnancy. MCN Am. J. Matern. Child. Nurs. 2011, 36, 381–386. [Google Scholar] [CrossRef]
- Thornton, P.L.; Kieffer, E.C.; Salabarría-Peña, Y.; Odoms-Young, A.; Willis, S.K.; Kim, H.; Salinas, M.A. Weight, diet, and physical activity-related beliefs and practices among pregnant and postpartum Latino women: The role of social support. Matern. Child. Health J. 2006, 10, 95–104. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total n = 122 | HEG n = 33 | nHEG n = 89 | p-Value |
|---|---|---|---|---|
| age (years) | 27.7 ± 3.7 | 23.4 ± 1.5 | 29.3 ± 2.9 | <0.001 |
| educational level (%) (n) | ||||
| 5.7 (7) | 12.1 (4) | 3.4 (3) | 0.037 |
| 23.8 (29) | 33.3 (11) | 20.2 (18) | |
| 70.5 (86) | 54.6 (18) | 76.4 (68) | |
| place of residence (%) (n) | ||||
| 31.1 (38) | 33.3 (11) | 30.3 (27) | 0.751 |
| 68.9 (84) | 66.7 (22) | 69.7 (62) | |
| trimester of pregnancy (%) (n) | ||||
| 9.8 (12) | 18.2 (6) | 6.7 (6) | 0.161 |
| 41.0 (50) | 39.4 (13) | 41.6 (37) | |
| 49.2 (60) | 42.4 (14) | 51.7 (46) | |
| pre-pregnancy weight (kg) (mean± SD) | 66.3 ± 14.3 | 63.5 ± 13.8 | 67.3 ± 14.4 | 0.110 |
| pre-pregnancy PA (%) (n) | ||||
| 41.8 (51) | 54.5 (18) | 37.1 (33) | 0.082 |
| 58.2 (71) | 45.5 (15) | 62.9 (56) | |
| pregnancy PA (METs; mean ± SD) | ||||
| 191.0 ± 118.7 | 187.6 ± 156.8 | 192.4 ± 102.1 | 0.177 |
| 41.1 ± 31.6 | 41.2 ± 31.7 | 41.1 ± 31.5 | 0.977 |
| 71.7 ± 38.9 | 69.2 ± 42.5 | 72.6 ± 37.6 | 0.536 |
| 72.9 ± 75.8 | 68.6 ± 92.8 | 74.6 ± 68.9 | 0.132 |
| 5.3 ± 22.3 | 8.6 ± 33.7 | 4.1 ± 16.2 | 0.762 |
| r | p-Value | |
|---|---|---|
| 1. pHDI | 0.27 | 0.002 |
| 2. wholemeal bread | 0.25 | 0.005 |
| 3. grains and coarse-ground groats | 0.23 | 0.012 |
| 4. milk | 0.10 | 0.269 |
| 5. fermented milk beverages | 0.14 | 0.111 |
| 6. curd | 0.16 | 0.082 |
| 7. white meat | 0.14 | 0.112 |
| 8. fish | 0.19 | 0.039 |
| 9. legumes | 0.19 | 0.033 |
| 10. fruits | 0.21 | 0.019 |
| 11. vegetables | 0.18 | 0.044 |
| Variables | HEG | nHEG |
|---|---|---|
| 0.58 * | 0.50 * |
| 0.74 * | 0.42 * |
| 0.60 * | 0.26 |
| 0.62 * | 0.60 * |
| 0.62 * | 0.37 * |
| 0.35 * | 0.28 |
| 0.45 * | 0.33 * |
| 0.47 * | 0.53 * |
| 0.75 * | 0.61 * |
| 0.81 * | 0.73 * |
| Variables | R2 | β | F | p-Value |
|---|---|---|---|---|
| Model 1: HEG | 0.996 | 2297.2 | <0.001 | |
| vegetables | 0.28 | <0.001 | ||
| fermented milk beverages | 0.16 | <0.001 | ||
| milk | 0.23 | <0.001 | ||
| wholemeal bread | 0.20 | <0.001 | ||
| fruits | 0.22 | <0.001 | ||
| grains and coarse-ground groats | 0.20 | <0.001 | ||
| curd | 0.16 | <0.001 | ||
| white meat | 0.06 | <0.001 | ||
| Model 2: nHEG | 0.939 | 79.5 | <0.001 | |
| vegetables | 0.21 | 0.004 | ||
| fermented milk beverages | 0.34 | <0.001 | ||
| grains and coarse-ground groats | 0.16 | 0.002 | ||
| fruits | 0.38 | <0.001 | ||
| legumes | 0.25 | <0.001 | ||
| wholemeal bread | 0.26 | <0.001 |
| Variable | R2 | β | F | p Value |
|---|---|---|---|---|
| 0.208 | 7.69 | <0.001 | ||
| health education | 0.25 | 0.003 | ||
| trimester of pregnancy | 0.21 | 0.028 | ||
| moderate PA | 0.19 | 0.013 | ||
| pre-pregnancy PA | 0.18 | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demuth, A.; Ratajczak, J.; Czerniak, U.; Antosiak-Cyrak, K. Is Health Education among the Decisive Factors for the Diet Quality of Pregnant Women in Poland? Nutrients 2023, 15, 2627. https://doi.org/10.3390/nu15112627
Demuth A, Ratajczak J, Czerniak U, Antosiak-Cyrak K. Is Health Education among the Decisive Factors for the Diet Quality of Pregnant Women in Poland? Nutrients. 2023; 15(11):2627. https://doi.org/10.3390/nu15112627
Chicago/Turabian StyleDemuth, Anna, Joanna Ratajczak, Urszula Czerniak, and Katarzyna Antosiak-Cyrak. 2023. "Is Health Education among the Decisive Factors for the Diet Quality of Pregnant Women in Poland?" Nutrients 15, no. 11: 2627. https://doi.org/10.3390/nu15112627