
Parenteral Nutrition, Sepsis, Acute Heart Failure and Hepatotoxic Drugs Are Related to Liver Test Disturbances in Critically Ill Patients
 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Selection Criteria
2.3. Collected Data
2.4. Co-Morbidities
2.5. Hepatotoxic Drugs
2.6. Statistical Analysis
3. Results
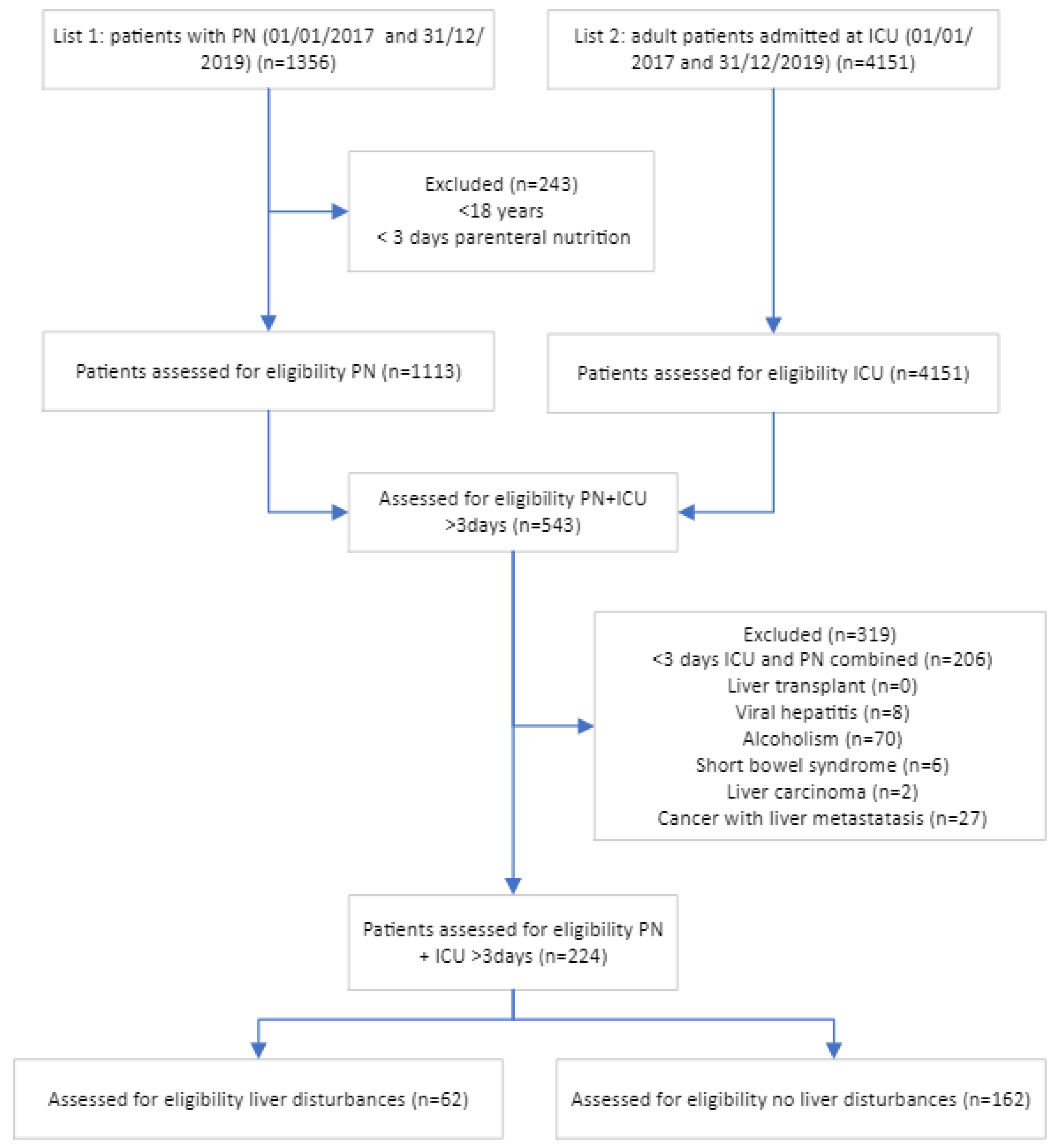
3.1. Study Population
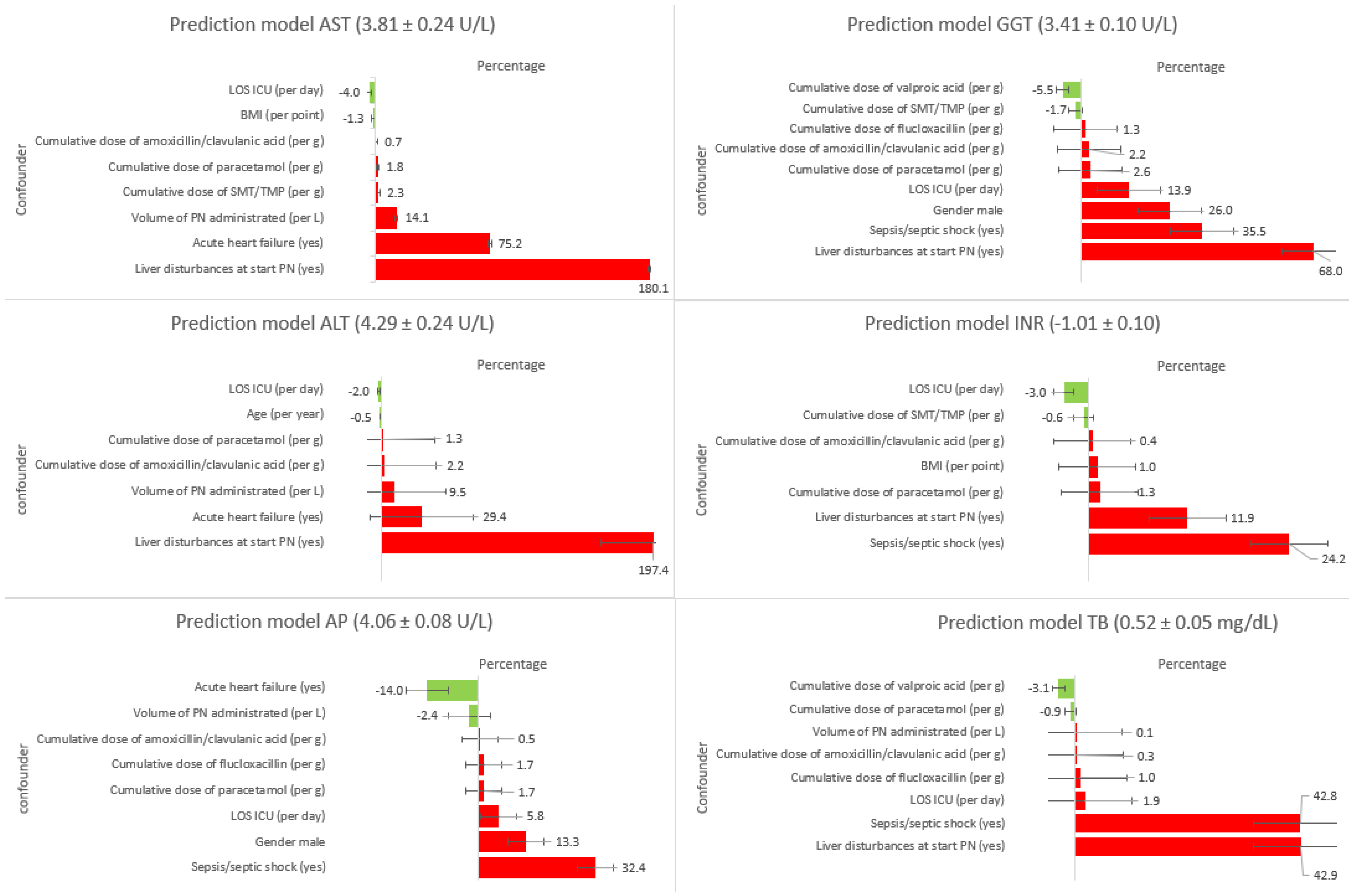
3.2. Liver Test Abnormalities Associated with PN, Drugs, AHF, and Sepsis
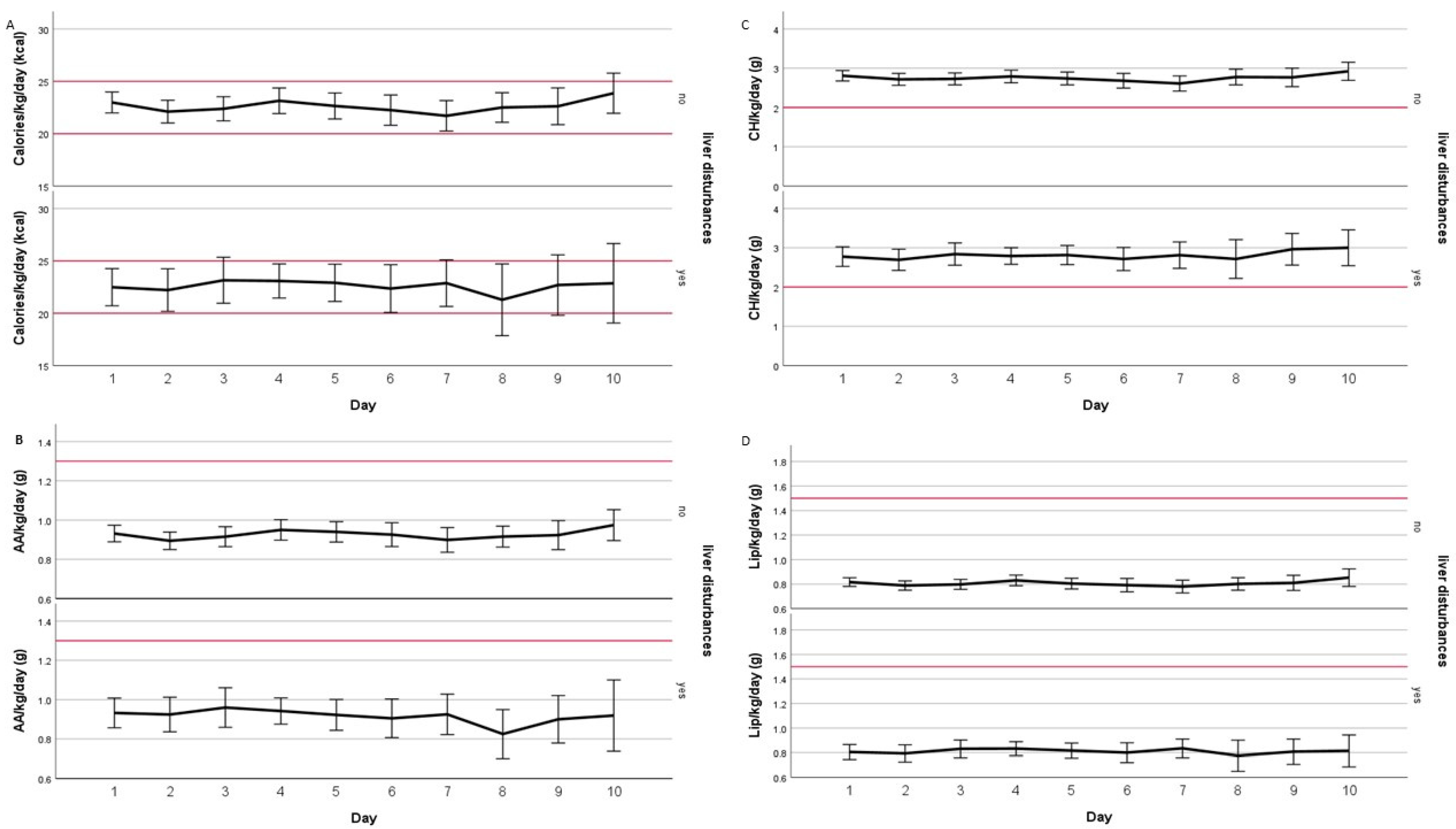
3.3. Feeding Adequacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Estimate (SE) | Increase/Decrease (%) | t Value | p Value | |
|---|---|---|---|---|
| AST (U/L) (3.81 ± 0.24 U/L) | ||||
| Duration on ICU (per day) | −0.041 (0.009) | −4.0 | −4.377 | <0.001 |
| Acute heart failure vs. no acute heart failure | 0.561 (0.128) | 75.2 | 4.377 | <0.001 |
| Cumulative dose of paracetamol (per g) | 0.018 (0.004) | 1.8 | 4.131 | <0.001 |
| Cumulative dose of amoxicillin/clavulanic acid (per g) | 0.007 (0.005) | 0.7 | 1.580 | 0.114 |
| Cumulative dose of SMT/TMP (per g) | 0.023 (0.010) | 2.3 | 2.299 | 0.022 |
| Liver dist at start PN vs. no liver dist at start PN | 1.030 (0.106) | 180.1 | 9.739 | <0.001 |
| Volume of PN (per L) | 0.132 (0.059) | 14.1 | 2.252 | 0.025 |
| BMI (per point) | −0.013 (0.009) | −1.3 | −1.574 | 0.117 |
| ALT (U/L) (4.29 ± 0.24 U/L) | ||||
| Duration on ICU (per day) | −0.020 (0.008) | −2.0 | −2.590 | 0.009 |
| Age (per year) | −0.005 (0.003) | −0.5 | −1.660 | 0.097 |
| Cumulative dose of paracetamol (per g) | 0.013 (0.004) | 1.3 | 3.700 | <0.001 |
| Cumulative dose of amoxicillin/clavulanic acid (per g) | 0.022 (0.004) | 2.2 | 5.530 | <0.001 |
| Volume of PN (per L) | 0.091 (0.050) | 9.5 | 1.860 | 0.063 |
| Acute heart failure vs. no acute heart failure | 0.258 (0126) | 29.4 | 2.040 | 0.043 |
| Liver dist at start PN vs. no liver dist at start PN | 1.090 (0.106) | 197.4 | 10.300 | <0.001 |
| AP (U/L) (4.06 ± 0.08 U/L) | ||||
| Acute heart failure vs. no acute heart failure | −0.151 (0.093) | −14.0 | −1.620 | 0.107 |
| Duration on ICU (per day) | 0.056 (0.005) | 5.8 | 11.100 | <0.001 |
| Liver dist at start PN vs. no liver dist at start PN | 0.371 (0.078) | 44.9 | 4.760 | <0.001 |
| Cumulative dose of flucloxacillin (per g) | 0.017 (0.004) | 1.7 | 4.200 | <0.001 |
| Cumulative dose of amoxicillin/clavulanic acid (per g) | 0.005 (0.003) | 0.5 | 1.940 | 0.053 |
| Cumulative dose of paracetamol (per g) | 0.017 (0.002) | 1.7 | 6.930 | <0.001 |
| Sepsis/septic shock vs. no sepsis/septic shock | 0.281 (0.079) | 32.4 | 3.580 | <0.001 |
| Male | 0.125 (0.071) | 13.3 | 1.770 | 0.077 |
| Volume of PN (per L) | −0.024 (0.033) | −2.4 | −0.742 | 0.458 |
| GGT (U/L) (3.41 ± 0.10 U/L) | ||||
| Sepsis/septic shock vs. no sepsis/septic shock | 0.304 (0.129) | 35.5 | 2.360 | 0.019 |
| Male | 0.231 (0.115) | 26.0 | 2.000 | 0.046 |
| Liver dist at start PN vs. no liver dist at start PN | 0.519 (0.125) | 68.0 | 4.150 | <0.001 |
| Cumulative dose of SMT/TMP (per g) | −0.017 (0.009) | −1.7 | −1.810 | 0.071 |
| Cumulative dose of valproic acid (per g) | −0.057 (0.041) | −5.5 | −1.390 | 0.164 |
| Cumulative dose of flucloxacillin (per g) | 0.013 (0.006) | 1.3 | 2.230 | 0.026 |
| Cumulative dose of amoxicillin/clavulanic acid (per g) | 0.022 (0.004) | 2.2 | 4.930 | <0.001 |
| Cumulative dose of paracetamol (per g) | 0.026 (0.004) | 2.6 | 6.760 | <0.001 |
| Duration on ICU (per day) | 0.130 (0.008) | 13.9 | 16.200 | <0.001 |
| INR (−1.01 ± 0.10) | ||||
| Duration on ICU (per day) | −0.030 (0.004) | −3.0 | −8.250 | <0.001 |
| Liver dist at start PN vs. no liver dist at start PN | 0.112 (0.047) | 11.9 | 2.380 | 0.018 |
| Sepsis/septic shock vs. no sepsis/septic shock | 0.217 (0.048) | 24.2 | 4.520 | <0.001 |
| BMI (per point) | 0.010 (0.004) | 1.0 | 2.620 | 0.010 |
| Cumulative dose of SMT/TMP (per g) | −0.006 (0.004) | −0.6 | −1.540 | 0.123 |
| Cumulative dose of amoxicillin/clavulanic acid (per g) | 0.004 (0.002) | 0.4 | 2.260 | 0.024 |
| Cumulative dose of paracetamol (per g) | 0.013 (0.002) | 1.3 | 7.440 | <0.001 |
| TB (mg/dL) (0.52 ± 0.05 mg/dL) | ||||
| Duration on ICU (per day) | 0.019 (0.003) | 1.9 | 5.860 | <0.001 |
| Cumulative dose of valproic acid (per g) | −0.031 (0.020) | −3.1 | −1.540 | 0.125 |
| Cumulative dose of flucloxacillin (per g) | 0.010 (0.003) | 1.0 | 3.840 | <0.001 |
| Cumulative dose of amoxicillin/clavulanic acid (per g) | 0.003 (0.002) | 0.3 | 1.680 | 0.094 |
| Cumulative dose of paracetamol (per g) | −0.009 (0.002) | −0.9 | −5.540 | <0.001 |
| Liver dist at start PN vs. no liver dist at start PN | 0.357 (0.061) | 42.9 | 5.770 | <0.001 |
| Sepsis/septic shock vs. no sepsis/septic shock | 0.356 (0.063) | 42.8 | 5.600 | <0.001 |
| Volume of PN (per L) | 0.001 (0.021) | 0.1 | 0.049 | 0.961 |
Appendix B
| Situation 1 | Situation 2 | Situation 3 | Situation 4 | ||||
|---|---|---|---|---|---|---|---|
| Parameter | =e(estimate) | Parameter | =e(estimate) | Parameter | =e(estimate) | Parameter | =e(estimate) |
| AST | =e(3.81) | AST | =e(3.81) | AST | =e(3.81) | AST | =e(3.81) |
| AHF (yes) | =e(0.561) | AHF (yes) | =e(0.561) | AHF (no) | N/A | AHF (no) | N/A |
| LD (yes) | =e(1.03) | LD (yes) | =e(1.03) | LD (yes) | =e(1.03) | LD (no) | N/A |
| PCT (g) | =e(4 × 0.018) | PCT (g) | =e(4 × 0.018) | PCT (g) | =e(4 × 0.018) | PCT (g) | =e(4 × 0.018) |
| BMI | =e(−0.013 × 25) | BMI | =e(−0.013 × 25) | BMI | =e(−0.013 × 25) | BMI | =e(−0.013 × 25) |
| Day ICU | =e(−0.041 × 3) | Day ICU | =e(−0.041 × 3) | Day ICU | =e(−0.041 × 3) | Day ICU | =e(−0.041 × 3) |
| PN (L) | N/A | PN (L) | =e(2 × 0.132) | PN (L) | =e(2 × 0.132) | PN (L) | =e(2 × 0.132) |
| AST | 152.2 U/L | AST | 198.1 U/L | AST | 113.1 U/L | AST | 40.4 U/L |
References
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, S.E.; Parrott, F.; Harrison, D.A.; Bear, D.E.; Segaran, E.; Beale, R.; Bellingan, G.; Leonard, R.; Mythen, M.G.; Rowan, K.M.; et al. Trial of the Route of Early Nutritional Support in Critically Ill Adults. N. Engl. J. Med. 2014, 371, 1673–1684. [Google Scholar] [CrossRef] [PubMed]
- Wischmeyer, P.E.; Hasselmann, M.; Kummerlen, C.; Kozar, R.; Kutsogiannis, D.J.; Karvellas, C.J.; Besecker, B.; Evans, D.K.; Preiser, J.-C.; Gramlich, L.; et al. A randomized trial of supplemental parenteral nutrition in underweight and overweight critically ill patients: The TOP-UP pilot trial. Crit. Care 2017, 21, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.M.; Pichard, C. Development and current use of parenteral nutrition in critical care—An opinion paper. Crit. Care 2014, 18, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zusman, O.; Theilla, M.; Cohen, J.; Kagan, I.; Bendavid, I.; Singer, P. Resting energy expenditure, calorie and protein consumption in critically ill patients: A retrospective cohort study. Crit. Care 2016, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Achamrah, N.; Delsoglio, M.; De Waele, E.; Berger, M.M.; Pichard, C. Indirect calorimetry: The 6 main issues. Clin. Nutr. 2020, 40, 4–14. [Google Scholar] [CrossRef]
- Grau, T.; Bonet, A.; Rubio, M.; Mateo, D.; Farré, M.; Acosta, J.; Blesa, A.; Montejo, J.; De Lorenzo, A.; Mesejo, A. Liver dysfunction associated with artificial nutrition in critically ill patients. Crit. Care 2007, 11, R10. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.-W.; Li, Y.-S. Pathogenesis and treatment of parenteral nutrition-associated liver disease. Hepatobiliary Pancreat. Dis. Int. 2012, 11, 586–593. [Google Scholar] [CrossRef]
- Żalikowska-Gardocka, M.; Przybyłkowski, A. Review of parenteral nutrition-associated liver disease. Clin. Exp. Hepatol. 2020, 6, 65–73. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of cholestatic liver diseases. J. Hepatol. 2009, 51, 237–267. [Google Scholar] [CrossRef]
- Woźnica, E.; Inglot, M.; Woźnica, R.; Łysenko, L. Liver dysfunction in sepsis. Adv. Clin. Exp. Med. 2018, 27, 547–552. [Google Scholar] [CrossRef]
- Kobashi, H.; Toshimori, J.; Yamamoto, K. Sepsis-associated liver injury: Incidence, classification and the clinical significance. Hepatol. Res. 2012, 43, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Laribi, S.; Mebazaa, A. Cardiohepatic Syndrome: Liver Injury in Decompensated Heart Failure. Curr. Heart Fail. Rep. 2014, 11, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, E.S. Hepatotoxicity by Drugs: The Most Common Implicated Agents. Int. J. Mol. Sci. 2016, 17, 224. [Google Scholar] [CrossRef] [Green Version]
- Dev, K.; Sumita, V. Drug-induced liber injury. R. Collage Physicians 2016, 16, 104–109. [Google Scholar]
- Lemmens, H.J.M.; Brodsky, J.B.; Bernstein, D.P. Estimating Ideal Body Weight—A New Formula. Obes. Surg. 2005, 15, 1082–1083. [Google Scholar] [CrossRef] [PubMed]
- Gotts, J.E.; Matthay, M.A. Sepsis: Pathophysiology and clinical management. BMJ 2016, 353, i1585. [Google Scholar] [CrossRef] [Green Version]
- Napolitano, L.M. Sepsis 2018: Definitions and Guideline Changes. Surg. Infect. 2018, 19, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Kurmani, S.; Squire, I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr. Heart Fail. Rep. 2017, 14, 385–392. [Google Scholar] [CrossRef] [Green Version]
- Mebazaa, A.; Nieminen, M.S.; Packer, M.; Cohen-Solal, A.; Kleber, F.X.; Pocock, S.J.; Thakkar, R.; Padley, R.J.; Põder, P.; Kivikko, M.; et al. Levosimendan vs Dobutamine for Patients With Acute Decompensated Heart Failure. JAMA 2007, 297, 1883–1891. [Google Scholar] [CrossRef] [Green Version]
- Shan, S.; Shen, Z.; Song, F. Autophagy and acetaminophen-induced hepatotoxicity. Arch. Toxicol. 2018, 92, 2153–2161. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, E.S.; Hoofnagle, J.H. Categorization of drugs implicated in causing liver injury: Critical assessment based on published case reports. Hepatology 2015, 63, 590–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badia-Tahull, M.B.; Leiva-Badosa, E.; Llop-Talaverón, J.; Figueras-Suriol, A.; Quirante-Cremades, A.; Tubau-Molas, M.; Jódar-Masanés, R. Alteraciones de los parámetros hepáticos asociados con la administración de utrición parenteral en pacientes adultos hospitalizados; incidencia y factores de riesgo. Nutr. Hosp. 2012, 27, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Xanthopoulos, A.; Starling, R.C.; Kitai, T.; Triposkiadis, F. Heart Failure and Liver Disease: Cardiohepatic Interactions. JACC Heart Fail. 2018, 7, 87–97. [Google Scholar] [CrossRef]
- Cogger, V.C.; Fraser, R.; Le Couteur, D.G. Liver dysfunction and heart failure. Am. J. Cardiol. 2003, 91, 1399. [Google Scholar] [CrossRef]
- Lau, G.T.; Tan, H.C.; Kritharides, L. Type of liver dysfunction in heart failure and its relation to the severity of tricuspid regurgitation. Am. J. Cardiol. 2002, 90, 1405–1409. [Google Scholar] [CrossRef]
- Vasconcelos, L.A.B.A.; de Almeida, E.A.; Bachur, L.F. Clinical evaluation and hepatic laboratory assessment in individuals with congestive heart failure. Arq. Bras. Cardiol. 2007, 88, 590–595. [Google Scholar] [CrossRef] [Green Version]
- Clarke, P.; Ball, M.; Kettlewell, M. Liver Function Tests in Patients Receiving Parenteral Nutrition. J. Parenter. Enter. Nutr. 1991, 15, 54–59. [Google Scholar] [CrossRef]
- Messing, B.; Colombel, J.F.; Heresbach, D.; Chazouillères, O.; Galian, A. Chronic cholestasis and macronutrient excess in patients treated with prolonged parenteral nutrition. Nutrition 1992, 8, 30–36. Available online: https://europepmc.org/article/med/1562786 (accessed on 20 January 2023).
- Ito, Y.; Shils, M.E. Liver Dysfunction Associated with Long-Term Total Parenteral Nutrition in Patients with Massive Bowel Resection. J. Parenter. Enter. Nutr. 1991, 15, 271–276. [Google Scholar] [CrossRef]
- Quigley, E.M.M.; Marsh, M.N.; Shaffer, J.L.; Markin, R.S. Special Reports and Reviews hepatobiliary complications of Total Parenteral Nutrition. Gastroenterology 1993, 104, 286–301. [Google Scholar] [CrossRef] [PubMed]
- Ellegård, L.; Sunesson, Å.; Bosaeus, I. High serum phytosterol levels in short bowel patients on parenteral nutrition support. Clin. Nutr. 2005, 24, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Hallikainen, M.; Huikko, L.; Kontra, K.; Nissinen, M.; Piironen, V.; Miettinen, T.; Gylling, H. Effect of Parenteral Serum Plant Sterols on Liver Enzymes and Cholesterol Metabolism in a Patient With Short Bowel Syndrome. Nutr. Clin. Pract. 2008, 23, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Llop, J.M.; Virgili, N.; Moreno-Villares, J.M.; García-Peris, P.; Serrano, T.; Forga, M.; Solanich, J.; Pita, A.M. Phytosterolemia in parenteral nutrition patients: Implications for liver disease development. Nutrition 2008, 24, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Plauth, M. ESPEN practical guideline: Clinical nutrition in liver disease. Clin. Nutr. 2020, 39, 3533–3562. [Google Scholar] [CrossRef]
- Cai, W.; Calder, P.C.; Cury-Boaventura, M.F.; De Waele, E.; Jakubowski, J.; Zaloga, G. Biological and Clinical Aspects of an Olive Oil-Based Lipid Emulsion—A Review. Nutrients 2018, 10, 776. [Google Scholar] [CrossRef] [Green Version]
- Manzanares, W.; Langlois, P.L.; Hardy, G. Intravenous lipid emulsions in the critically ill. Curr. Opin. Crit. Care 2016, 22, 308–315. [Google Scholar] [CrossRef]
- De Waele, E.; Malbrain, M.L.; Spapen, H. Nutrition in Sepsis: A Bench-to-Bedside Review. Nutrients 2020, 12, 395. [Google Scholar] [CrossRef] [Green Version]
- Sungurtekin, H.; Değirmenci, S.; Sungurtekin, U.; Oguz, B.E.; Sabir, N.; Kaptanoglu, B. Comparison of the Effects of Different Intravenous Fat Emulsions in Patients With Systemic Inflammatory Response Syndrome and Sepsis. Nutr. Clin. Pract. 2011, 26, 665–671. [Google Scholar] [CrossRef]
- Nagai, T.; Honda, Y.; Sugano, Y.; Nishimura, K.; Nakai, M.; Honda, S.; Iwakami, N.; Okada, A.; Asaumi, Y.; Aiba, T.; et al. Circulating Omega-6, But Not Omega-3 Polyunsaturated Fatty Acids, Are Associated with Clinical Outcomes in Patients with Acute Decompensated Heart Failure. PLoS ONE 2016, 11, e0165841. [Google Scholar] [CrossRef] [Green Version]
- Green, P.; Theilla, M.; Singer, P. Lipid metabolism in critical illness. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 111–115. [Google Scholar] [CrossRef]
- Hall, T.C.; Bilku, D.K.; Al-Leswas, D.; Neal, C.P.; Horst, C.; Cooke, J.; Metcalfe, M.S.; Dennison, A.R. A Randomized Controlled Trial Investigating the Effects of Parenteral Fish Oil on Survival Outcomes in Critically Ill Patients With Sepsis. J. Parenter. Enter. Nutr. 2014, 39, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.-J.; Sun, L.-L.; Li, M.-Y.; Ding, C.-L.; Su, Y.-C.; Xue, S.-H.; Yan, F.; Zhao, C.-H.; Wang, W. Comparison of Formulas Based on Lipid Emulsions of Olive Oil, Soybean Oil, or Several Oils for Parenteral Nutrition: A Systematic Review and Meta-Analysis. Adv. Nutr. Int. Rev. J. 2016, 7, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hara, M.; Sakata, Y.; Nakatani, D.; Suna, S.; Usami, M.; Matsumoto, S.; Hamasaki, T.; Doi, Y.; Nishino, M.; Sato, H.; et al. Low levels of serum n-3 polyunsaturated fatty acids are associated with worse heart failure-free survival in patients after acute myocardial infarction. Circ. J. 2013, 77, 153–162. [Google Scholar] [CrossRef] [Green Version]
- Marchioli, R.; Barzi, F.; Bomba, E.; Chieffo, C.; Di Gregorio, D.; Di Mascio, R.; Franzosi, M.G.; Geraci, E.; Levantesi, G.; Maggioni, A.P.; et al. Early protection against sudden death by n-3 polyunsaturated fatty acids after myocardial infarction. Circulation 2002, 105, 1897–1903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishizaki, Y.; Shimada, K.; Tani, S.; Ogawa, T.; Ando, J.; Takahashi, M.; Yamamoto, M.; Shinozaki, T.; Miyazaki, T.; Miyauchi, K.; et al. Association between the docosahexaenoic acid to arachidonic acid ratio and acute coronary syndrome: A multicenter observational study. BMC Cardiovasc. Disord. 2016, 16, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gourd, N.M.; Nikitas, N. Multiple Organ Dysfunction Syndrome. J. Intensiv. Care Med. 2019, 35, 1564–1575. [Google Scholar] [CrossRef]
- D’angelo, S.; Motti, M.L.; Meccariello, R. ω-3 and ω-6 Polyunsaturated Fatty Acids, Obesity and Cancer. Nutrients 2020, 12, 2751. [Google Scholar] [CrossRef]
- Iyer, K.; Spitz, L.; Clayton, P. New insight into mechanisms of parenteral nutrition—Associated cholestasis: Role of plant sterols. J. Pediatr. Surg. 1998, 33, 1–6. [Google Scholar] [CrossRef]
- Guthrie, G.; Tackett, B.; Stoll, B.; Martin, C.; Olutoye, O.; Burrin, D.G. Phytosterols Synergize With Endotoxin to Augment Inflammation in Kupffer Cells but Alone Have Limited Direct Effect on Hepatocytes. J. Parenter. Enter. Nutr. 2017, 42, 37–48. [Google Scholar] [CrossRef]
- Manzanares, W.; Dhaliwal, R.; Jurewitsch, B.; Stapleton, R.D.; Jeejeebhoy, K.N.; Heyland, D.K. Parenteral fish oil lipid emulsions in the critically Ill. J. Parenter. Enter. Nutr. 2013, 38, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Deutz, N.E.P.; Biolo, G.; Bischoff, S.; Boirie, Y.; Cederholm, T.; Cuerda, C.; Delzenne, N.; Leon Sanz, M.; Ljungqvist, O.; et al. Carbohydrates and insulin resistance in clinical nutrition: Recommendations from the ESPEN expert group. Clin. Nutr. 2017, 36, 355–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakananurak, N.; Tienchai, K. Incidence and risk factors of parenteral nutrition-associated liver disease in hospitalized adults: A prospective cohort study. Clin. Nutr. ESPEN 2019, 34, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.M. Acetaminophen (APAP) hepatotoxicity—Isn’t it time for APAP to go away? J. Hepatol. 2017, 67, 1324–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| No liver Disturbances (N = 162) | Liver Disturbances (N = 62) | Total (N = 224) | p-Value | |
|---|---|---|---|---|
| Baseline characteristics | ||||
| Sex female—no. (%) | 62 (38.3) | 23 (37.1) | 85 (37.9) | 0.871 |
| Age (y) | 65 ± 16 | 60 ± 17 | 63 ± 17 | 0.040 |
| Height (cm) | 169 ± 10 | 172 ± 10 | 171 ± 10 | 0.196 |
| Weight (kg) | 76 ± 20 | 78 ± 15 | 77 ± 19 | 0.221 |
| BMI | 26 ± 6 | 26 ± 5 | 26 ± 6 | 0.700 |
| Body Mass Index—no. (%) | 0.224 | |||
| <18.5 | 12 (7.4) | 1 (1.6) | 13 (5.8) | |
| 18.5–25 | 61 (37.7) | 27 (43.5) | 88 (39.3) | |
| >25 | 89 (54.9) | 34 (54.8) | 123 (54.9) | |
| ABW (kg) | 68 ± 10 | 71 ± 9 | 69 ± 10 | 0.078 |
| LOS ICU (days) | 16 [9–26] | 18 [9–33] | 19 [10–31] | 0.243 |
| APACHE II score | 21 ± 11 | 24 ± 11 | 22 ± 11 | 0.048 |
| 28 days mortality—no. (%) | 43 (26.5) | 23 (37.1) | 66 (29.5) | 0.121 |
| Nutritional characteristics | ||||
| PN therapy duration at ICU (days) | 6 [4–12] | 6 [4–11] | 8 [5–14] | 0.540 |
| Tube feeding—no. (%) | 93 (57.4) | 41 (66.1) | 134 (59.8) | 0.234 |
| TF therapy duration at ICU (days) | 12 [6–23] | 7 [4–28] | 12 [6–23] | 0.219 |
| REE (Kcal) | 1772 [1349–2225] | 1877 [1689–2180] | 1834 [1492–2139] | 0.533 |
| Calorie requirement (Kcal) | 1708 ± 261 | 1764 ± 232 | 1732 ± 251 | 0.078 |
| Amino acid requirement (g) | 89 ± 14 | 92 ± 12 | 90 ± 13 | 0.078 |
| Carbohydrate requirement (g) | 137 ± 21 | 141 ±19 | 139 ± 20 | 0.078 |
| Lipid requirement (g) | 102 ± 16 | 106 ± 14 | 104 ± 15 | 0.078 |
| IC performed—no. (%) | 20 (12.3) | 6 (9.7) | 26 (11.6) | 0.577 |
| PN intake | ||||
| Volume of PN administered daily (mL) | 1450 ± 388 | 1572 ± 439 | 1482 ± 406 | <0.001 |
| PN Calories administered daily (kcal) | 1603 ± 548 | 1767 ± 499 | 1642 ± 472 | <0.001 |
| PN AA administered daily (g) | 64 ± 22 | 71 ± 21 | 66 ± 18 | <0.001 |
| PN CH administered daily (g) | 197 ± 69 | 217 ± 60 | 201 ± 62 | <0.001 |
| PN lipids administered daily (g) | 58 ± 22 | 62 ± 17 | 59 ± 16 | <0.001 |
| Co-morbidities | ||||
| Sepsis/septic shock—no. (%) | 35 (21.6) | 22 (35.5) | 57 (25.4) | 0.033 |
| Acute Heart Failure—no. (%) | 19 (11.7) | 18 (29) | 37 (16.5) | 0.002 |
| Hepatotoxic drugs | ||||
| Paracetamol prescribed—no. (%) | 151 (93.2) | 59 (95.2) | 210 (93.8) | 0.589 |
| Paracetamol therapy (days) | 22 [14–36] | 19 [9–35] | 21 [12–36] | 0.250 |
| AC prescribed—no. (%) | 114 (70.4) | 40 (64.5) | 154 (68.8) | 0.398 |
| AC therapy (days) | 5 ± 4 | 4 ± 3 | 5 ± 4 | 0.157 |
| Flucloxacillin prescribed—no. (%) | 15 (9.3) | 2 (3.2) | 17 (7.6) | 0.127 |
| Flucloxacillin therapy (days) | 10 ± 12 | 11 ± 8 | 9 ± 10 | 0.618 |
| Valproic acid prescribed—no. (%) | 11 (6.8) | 2 (3.2) | 13 (5.8) | 0.307 |
| Valproic acid therapy (days) | 4 [4–24] | 7 [4–7] | 7 [4–20] | 0.923 |
| SMT/TMP prescribed—no. (%) | 20 (16.1) | 10 (16.1) | 30 (13.4) | 0.457 |
| SMT/TMP therapy (days) | 6 [2–9] | 13 [4–22] | 7 [2–13] | 0.143 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosseel, Z.; Cortoos, P.-J.; Jonckheer, J.; Cools, W.; Vinken, M.; Reynaert, H.; De Waele, E. Parenteral Nutrition, Sepsis, Acute Heart Failure and Hepatotoxic Drugs Are Related to Liver Test Disturbances in Critically Ill Patients. Nutrients 2023, 15, 2612. https://doi.org/10.3390/nu15112612
Rosseel Z, Cortoos P-J, Jonckheer J, Cools W, Vinken M, Reynaert H, De Waele E. Parenteral Nutrition, Sepsis, Acute Heart Failure and Hepatotoxic Drugs Are Related to Liver Test Disturbances in Critically Ill Patients. Nutrients. 2023; 15(11):2612. https://doi.org/10.3390/nu15112612
Chicago/Turabian StyleRosseel, Zenzi, Pieter-Jan Cortoos, Joop Jonckheer, Wilfried Cools, Mathieu Vinken, Hendrik Reynaert, and Elisabeth De Waele. 2023. "Parenteral Nutrition, Sepsis, Acute Heart Failure and Hepatotoxic Drugs Are Related to Liver Test Disturbances in Critically Ill Patients" Nutrients 15, no. 11: 2612. https://doi.org/10.3390/nu15112612