
Translation of the Satter’s Division of Responsibility in Feeding Questionnaire into Brazilian Portuguese: A Cross-Sectional Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
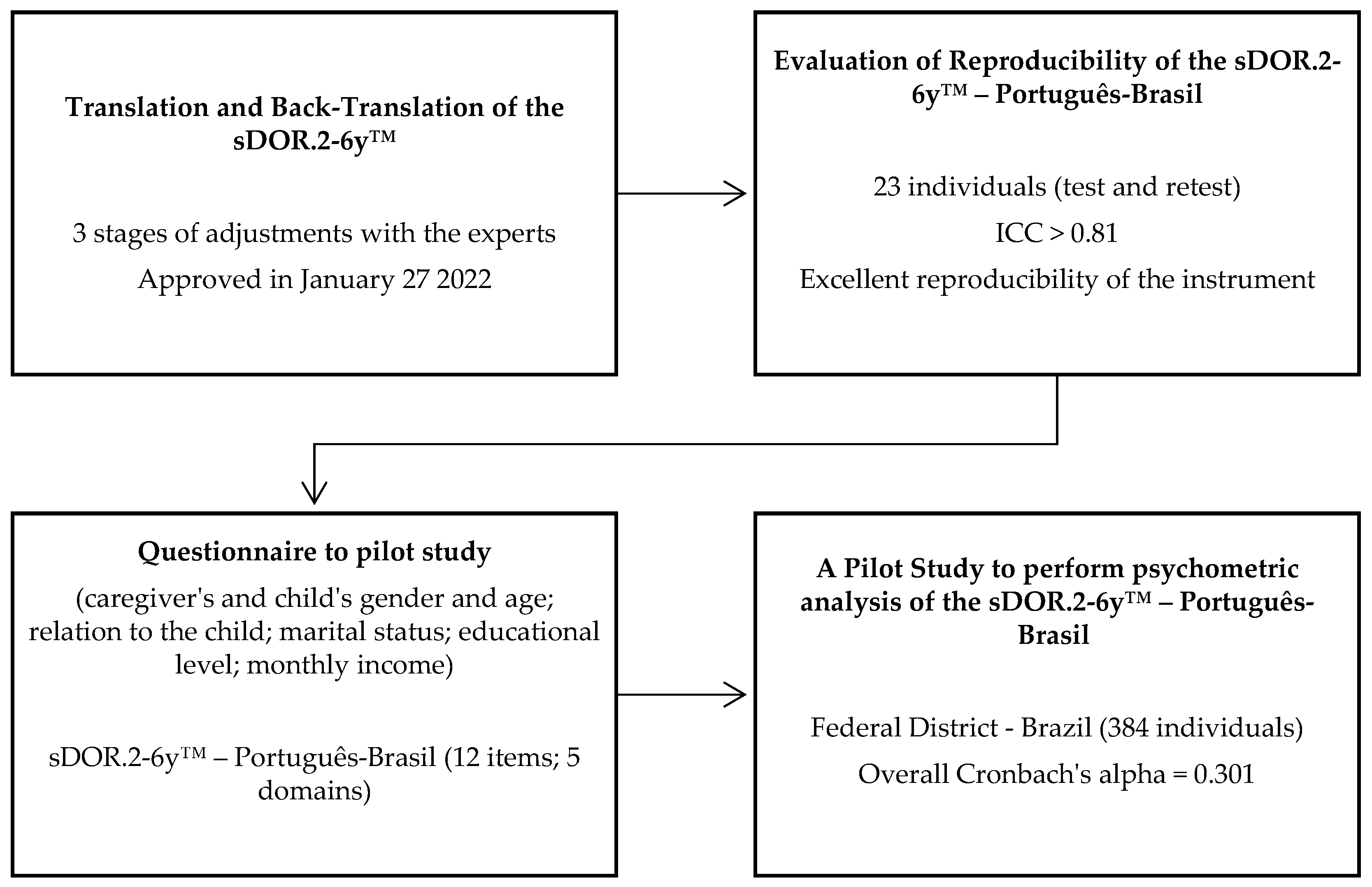
2.1. Translation and Back-Translation of the sDOR.2-6y™
2.2. Evaluation of Reproducibility of the sDOR.2-6y™—Português-Brasil
2.3. A Pilot Study to Perform a Psychometric Analysis of the sDOR.2-6y™—Português-Brasil
2.4. Statistical Analysis
3. Results
3.1. Translation and Back-Translation of the sDOR.2-6y™
3.2. Evaluation of Reproducibility of the sDOR.2-6y™—Português-Brasil
3.3. A Pilot Study to Perform a Psychometric Analysis of the sDOR.2-6y™—Português-Brasil
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Nutrition. Available online: https://www.who.int/health-topics/nutrition (accessed on 21 July 2022).
- World Health Organization Infant Nutrition. Available online: https://www.who.int/health-topics/infant-nutrition#tab=tab_1 (accessed on 21 July 2022).
- Ministério da Saúde. Brasil Dietary Guidelines for Brazilian Children under Two Years of Age; Ministério da Saúde: Brasília, Brazil, 2019; ISBN 978-85-334-2737-2.
- Haines, J.; Haycraft, E.; Lytle, L.; Nicklaus, S.; Kok, F.J.; Merdji, M.; Fisberg, M.; Moreno, L.A.; Goulet, O.; Hughes, S.O. Nurturing Children’s Healthy Eating: Position Statement. Appetite 2019, 137, 124–133. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.; Holub, S. Comprehensive Feeding Practices Questionnaire: Validation of a New Measure of Parental Feeding Practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory Factor Analysis of the Child Feeding Questionnaire: A Measure of Parental Attitudes, Beliefs and Practices about Child Feeding and Obesity Proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry Allied Discip. 2001, 42, 963–970. [Google Scholar] [CrossRef]
- Jansen, E.; Williams, K.E.; Mallan, K.M.; Nicholson, J.M.; Daniels, L.A. The Feeding Practices and Structure Questionnaire (FPSQ-28): A Parsimonious Version Validated for Longitudinal Use from 2 to 5 Years; Elsevier: Amsterdam, The Netherlands, 2016; Volume 100, ISBN 1260800005639. [Google Scholar]
- Satter, E. The Feeding Relationship: Problems and Interventions. J. Pediatr. 1990, 117, S181–S189. [Google Scholar] [CrossRef]
- Satter, E. The Feeding Relationship. J. Am. Diet. Assoc. 1986, 86, 352–356. [Google Scholar] [CrossRef]
- Satter, E. Feeding Dynamics: Helping Children to Eat Well. J. Pediatr. Health Care 1995, 9, 178–184. [Google Scholar] [CrossRef]
- Satter, E. Adjusting the Eneli et Al. Feeding Dynamic Intervention to Make It Consistent with Satter Feeding and Eating Models. Contemp. Clin. Trials 2015, 43, 279–280. [Google Scholar] [CrossRef]
- Lohse, B.; Mitchell, D.C. Valid and Reliable Measure of Adherence to Satter Division of Responsibility in Feeding. J. Nutr. Educ. Behav. 2021, 53, 211–222. [Google Scholar] [CrossRef]
- Lohse, B.; Satter, E.; Arnold, K. Development of a Tool to Assess Adherence to a Model of the Division of Responsibility in Feeding Young Children: Using Response Mapping to Capacitate Validation Measures. Child. Obes. 2014, 10, 153–168. [Google Scholar] [CrossRef]
- Lohse, B.; Satter, E. Use of an Observational Comparative Strategy Demonstrated Construct Validity of a Measure to Assess Adherence to the Satter Division of Responsibility in Feeding. J. Acad. Nutr. Diet. 2021, 121, 1143–1156.e6. [Google Scholar] [CrossRef]
- Borsa, J.C. Cross-Cultural Adaptation and Validation of Psychological Instruments: Adaptação e Validação de Instrumentos Psicológicos Entre Culturas: Algumas Considerações Adaptación y Validación de Instrumentos Psicológicos Entre Culturas: Algunas Consideraciones. Paidéia 2012, 22, 423–432. [Google Scholar] [CrossRef]
- Galdeano, L.E.; Furuya, R.K.; Delacio, M.C.B.; Dantas, R.A.S.; Rossi, L.A. Validação Semântica Do Cardiac Patients Learning Needs Inventory Para Brasileiros e Portugueses. Rev. Gaúcha Enferm. 2011, 32, 602–610. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Gjersing, L.; Caplehorn, J.R.; Clausen, T. Cross-Cultural Adaptation of Research Instruments: Language, Setting, Time and Statistical Considerations. BMC Med. Res. Methodol. 2010, 10, 13. [Google Scholar] [CrossRef]
- NEEDs Center. NEEDs Center: Using SDOR.2-6yTM. Available online: https://www.needscenter.org/satter-eating-competence-model-ecsatter/sdor-2-6y/ (accessed on 21 July 2022).
- de Queiroz, F.L.N.; Nakano, E.Y.; Ginani, V.C.; Botelho, R.B.A.; Araújo, W.M.C.; Zandonadi, R.P. Eating Competence among a Select Sample of Brazilian Adults: Translation and Reproducibility Analyses of the Satter Eating Competence Inventory. Nutrients 2020, 12, 2145. [Google Scholar] [CrossRef]
- Yasuzato, M.; Kikuchi, R.; Kawahara, T.; Nakayama, Y.; Yamazaki, A. Psychometric Examination of the Japanese Translation of the Satter Eating Competence Inventory-2.0TM for Parents of Fifth and Sixth Grade Students. Jpn. J. Nurs. Sci. 2021, 18, e12393. [Google Scholar] [CrossRef]
- NEEDs Center. NEEDs Center: Using EcSI 2.0TM. Available online: https://www.needscenter.org/satter-eating-competence-model-ecsatter/eating-competence/ (accessed on 21 July 2022).
- Zou, G.Y. Sample Size Formulas for Estimating Intraclass Correlation Coefficients with Precision and Assurance. Stat. Med. 2012, 31, 3972–3981. [Google Scholar] [CrossRef]
- Cicchetti, D. V Interreliability Standards in Psychological Evaluations. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Leighton, K.; Kardong-Edgren, S.; Schneidereith, T.; Foisy-Doll, C. Using Social Media and Snowball Sampling as an Alternative Recruitment Strategy for Research. Clin. Simul. Nurs. 2021, 55, 37–42. [Google Scholar] [CrossRef]
- Webber-Ritchey, K.J.; Aquino, E.; Ponder, T.N.; Lattner, C.; Soco, C.; Spurlark, R.; Simonovich, S.D. Recruitment Strategies to Optimize Participation by Diverse Populations. Nurs. Sci. Q. 2021, 34, 235–243. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 7th ed.; Bookman: Englewood Cliffs, NJ, USA, 2009; ISBN 978-0-02-349020-. [Google Scholar]
- Damásio, B.F. Uso Da Análise Fatorial Exploratória Em Psicologia. Avaliação Psicológica 2012, 11, 213–228. [Google Scholar]
- Pedroso, J.; Gubert, M.B. Cross-Cultural Adaptation and Validation of the Infant Feeding Style Questionnaire in Brazil. PLoS ONE 2021, 16, e0257991. [Google Scholar] [CrossRef]
- Evans, C.; Paz, C.; Mascialino, G. “Infeliz” or “Triste”: A Paradigm for Mixed Methods Exploration of Outcome Measures Adaptation Across Language Variants. Front. Psychol. 2021, 12, 695893. [Google Scholar] [CrossRef]
- Polit, D.F. Getting Serious about Test-Retest Reliability: A Critique of Retest Research and Some Recommendations. Qual. Life Res. 2014, 23, 1713–1720. [Google Scholar] [CrossRef]
- Miller, L.A.; Lovler, R.L.; McIntire, S.A. Foundations of Psychological Testing; SAGE Publications: Los Angeles, CA, USA, 2016; ISBN 9781483369259. [Google Scholar]
- Bruton, A.; Conway, J.H.; Holgate, S.T. Reliability: What Is It, and How Is It Measured? Physiotherapy 2000, 86, 94–99. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying Test-Retest Reliability Using the Intraclass Correlation Coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231. [Google Scholar] [CrossRef]
- Zanella, C.P.; de Sampaio, H.A.C.; de Lima, J.W.O.; Moreira, T.M.M. Cultural Adaptation and Content Validity Evidence of the Nutritional Literacy Scale Brazilian Version. Rev. Bras. Enferm. 2022, 75, e20210657. [Google Scholar] [CrossRef]
- de Almeida, P.C.; Vasconcelos, I.A.L.; Zandonadi, R.P.; Nakano, E.Y.; Raposo, A.; Han, H.; Araya-Castillo, L.; Ariza-Montes, A.; Botelho, R.B.A. Food Neophobia among Brazilian Children: Prevalence and Questionnaire Score Development. Sustainability 2022, 14, 975. [Google Scholar] [CrossRef]
- Davidson, D.J.; Freudenburg, W.R. Gender and Environmental Risk Concerns: A Review and Analysis of Available Research. Environ. Behav. 1996, 28, 302–339. [Google Scholar] [CrossRef]
- Sax, L.J.; Gilmartin, S.K.; Bryant, A.N. Assessing Response Rates and Nonresponse Bias in Web. High. Educ. 2011, 44, 409–432. [Google Scholar]
- Hamilton, R.J.; Bowers, B.J. Internet Recruitment and E-Mail Interviews in Qualitative Studies. Qual. Health Res. 2006, 16, 821–835. [Google Scholar] [CrossRef]
- Cortina, J.M. What Is Coefficient Alpha? An Examination of Theory and Applications. J. Appl. Psychol. 1993, 78, 98–104. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making Sense of Cronbach’s Alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Gadermann, A.M.; Guhn, M.; Zumbo, B.D. Estimating Ordinal Reliability for Likert-Type and Ordinal Item Response Data: A Conceptual, Empirical, and Practical Guide. Pract. Assess. Res. Eval. 2012, 17, 3. [Google Scholar]
- Streiner, D.L. Starting at the Beginning: An Introduction to Coefficient Alpha and Internal Consistency. J. Pers. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Schmitt, N. Uses and Abuses of Coefficient Alpha. Psychol. Assess. 1996, 8, 350–353. [Google Scholar] [CrossRef]
- Vyas, K.; Bano, S.; Islamia, J.M. Child’s Gender and Parenting Styles. Delhi Psychiatry J. 2016, 19, 289–293. [Google Scholar]
- Powell, F.C.; Farrow, C.V.; Meyer, C. Food Avoidance in Children. The Influence of Maternal Feeding Practices and Behaviours. Appetite 2011, 57, 683–692. [Google Scholar] [CrossRef]
- Braden, A.; Rhee, K.; Peterson, C.B.; Rydell, S.A.; Zucker, N.; Boutelle, K. Associations between Child Emotional Eating and General Parenting Style, Feeding Practices, and Parent Psychopathology. Appetite 2014, 80, 35–40. [Google Scholar] [CrossRef]
- Hittner, J.B.; Johnson, C.; Tripicchio, G.; Faith, M.S. Infant Emotional Distress, Maternal Restriction at a Home Meal, and Child BMI Gain through Age 6 Years in the Colorado Adoption Project. Eat. Behav. 2016, 21, 135–141. [Google Scholar] [CrossRef]
- Devall, E. Promoting Healthy Feeding Relationships and Nurturing Parenting Practices; New Mexico WIC Program Final Report; WIC: Washington, DC, USA, 2006.
- Ministério da Educuation FNDE. BRASIL Programa Nacional de Alimentação Escolae—PNAE; Caderno de Legislação 2018; Ministério da Educuation FNDE: Brasília, Brasil, 2018; p. 353.
- Fisberg, M.; Duarte Batista, L. Nutrition Related-Practices in Brazilian Preschoolers: Identifying Challenges and Addressing Barriers. Nestle Nutr. Inst. Workshop Ser. 2020, 95, 23–32. [Google Scholar] [CrossRef]
- Gaglianone, C.P.; Taddei, J.A.D.A.C.; Colugnati, F.A.B.; Magalhães, C.G.; Davanço, G.M.; De Macedo, L.; Lopez, F.A. Nutrition Education in Public Elementary Schools of São Paulo, Brazil: The Reducing Risks of Illness and Death in Adulthood Project. Rev. Nutr. 2006, 19, 309–320. [Google Scholar] [CrossRef]
- Diep, C.S.; Chen, T.A.; Davies, V.F.; Baranowski, J.C.; Baranowski, T. Influence of Behavioral Theory on Fruit and Vegetable Intervention Effectiveness Among Children: A Meta-Analysis. J. Nutr. Educ. Behav. 2014, 46, 506–546. [Google Scholar] [CrossRef]


{kind=link}
| sDOR.2-6y™ Domains | Tests Means (SD 1) | Retest Means (SD) | ICC 2 |
|---|---|---|---|
| Mealtime structure | 4.61(1.16) | 4.57 (1.08) | 0.894 |
| What is available to the child | 3.70 (1.89) | 3.87 (1.77) | 0.814 |
| How food is available to the child | 6.09 (1.12) | 6.13 (1.01) | 0.832 |
| Respect for child autonomy in eating | 5.09 (1.59) | 5.48 (1.20) | 0.700 |
| Who controls what, when, and how much is eaten | 3.96 (1.40) | 4.00 (1.21) | 0.825 |
| Total | 23.43 (4.18) | 24.04 (3.71) | 0.945 |
| Frequency Sample = 384 | % | ||
|---|---|---|---|
| Caregiver’s gender | Female | 325 | 84.6% |
| Male | 59 | 15.4% | |
| Caregiver’s age | 21 to 30 years | 18 | 4.7% |
| 31 to 40 years | 275 | 71.6% | |
| 41 to 50 years | 83 | 21.6% | |
| 51 to 60 years | 6 | 1.6% | |
| 61 to 70 years | 2 | 0.5% | |
| Relation to the child | Mother | 317 | 82.6% |
| Father | 60 | 15.6% | |
| Aunt | 2 | 0.5% | |
| Grandma | 5 | 1.3% | |
| Marital status | Married or common-law marriage | 340 | 88.8% |
| Single | 22 | 5.7% | |
| Divorced | 20 | 5.2% | |
| Widowed | 2 | 0.5% | |
| Educational level | High School | 15 | 3.9% |
| Undergraduate | 78 | 20.3% | |
| Graduate | 291 | 75.8% | |
| Monthly income 1 | Up to BRL 3000 | 14 | 3.6% |
| BRL 3001 to BRL 5000 | 17 | 4.4% | |
| BRL 5001 to BRL 10,000 | 59 | 15.3% | |
| BRL 10,001 to BRL 15,000 | 76 | 19.8% | |
| More than BRL 15,000 | 186 | 48.4% | |
| Prefer not to inform | 32 | 8.3% | |
| Child’s gender | Female | 200 | 52.1% |
| Male | 184 | 47.9% | |
| Child’s age | 2 years to 2 years and 11 months | 109 | 28.4% |
| 3 years to 3 years and 11 months | 89 | 23.2% | |
| 4 years to 4 years and 11 months | 79 | 20.6% | |
| 5 years to 5 years and 11 months | 58 | 15.1% | |
| 6 years exactly | 49 | 12.7% |
| D1 | D2 | D3 | D4 | D5 | Total | |
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Caregiver’s gender * | ||||||
| Female (n = 325) | 4.52 (1.10) A | 2.57 (1.41) A | 5.90 (1.36) A | 2.07 (1.38) A | 4.96 (1.92) A | 20.02 (3.53) A |
| Male (n = 59) | 4.49 (1.10) A | 2.64 (1.46) A | 5.59 (1.54) A | 2.20 (1.23) A | 5.24 (2.01) A | 20.17 (3.85) A |
| p | 0.871 | 0.709 | 0.120 | 0.490 | 0.317 | 0.766 |
| Caregiver’s age * | ||||||
| Up to 40 years (n = 293) | 4.50 (1.08) A | 2.56 (1.38) A | 5.85 (1.36) A | 2.08 (1.37) A | 4.96 (1.85) A | 19.95 (3.47) A |
| More than 40 years (n = 91) | 4.55 (1.16) A | 2.65 (1.53) A | 5.86 (1.49) A | 2.14 (1.30) A | 5.14 (2.18) A | 20.34 (3.90) A |
| p | 0.718 | 0.602 | 0.965 | 0.678 | 0.437 | 0.361 |
| Relation to the child * | ||||||
| Mother (n = 317) | 4.51 (1.10) A | 2.56 (1.40) A | 5.90 (1.36) A | 2.06 (1.39) A | 4.98 (1.92) A | 20.02 (3.54) A |
| Other (n = 67) | 4.52 (1.09) A | 2.69 (1.47) A | 5.61 (1.49) A | 2.22 (1.19) A | 5.10 (1.99) A | 20.15 (3.76) A |
| p | 0.939 | 0.501 | 0.120 | 0.378 | 0.644 | 0.787 |
| Marital status * | ||||||
| Married or common-law marriage (n = 340) | 4.51 (1.11) A | 2.56 (1.41) A | 5.87 (1.38) A | 2.09 (1.35) A | 5.07 (1.95) A | 20.10 (3.61) A |
| Others (n = 44) | 4.57 (1.00) A | 2.77 (1.43) A | 5.70 (1.49) A | 2.09 (1.39) A | 4.48 (1.72) A | 19.61 (3.24) A |
| p | 0.724 | 0.339 | 0.456 | 0.999 | 0.054 | 0.399 |
| Educational level * | ||||||
| High School/Undergraduate (n = 93) | 4.69 (1.03) A | 2.76 (1.36) A | 5.78 (1.29) A | 2.10 (1.23) A | 4.91 (1.67) A | 20.25 (3.47) A |
| Graduate (n = 291) | 4.46 (1.12) A | 2.52 (1.43) A | 5.87 (1.42) A | 2.09 (1.40) A | 5.03 (2.01) A | 19.98 (3.61) A |
| p | 0.078 | 0.152 | 0.596 | 0.963 | 0.602 | 0.524 |
| Monthly income 1,** | ||||||
| Up to BRL 5000 (n = 31) | 4.84 (0.86) A | 3.13 (1.57) A | 5.77 (1.31) A | 2.16 (1.34) A | 5.13 (1.75) A | 21.03 (3.74) A |
| BRL 5001 to BRL 10,000 (n = 59) | 4.54 (0.99) A | 2.66 (1.25) A | 5.85 (1.40) A | 1.93 (1.35) A | 5.14 (1.91) A | 20.12 (3.13) A |
| BRL 10,001 to BRL 15,000 (n = 76) | 4.66 (1.17) A | 2.76 (1.33) A | 5.87 (1.32) A | 2.07 (1.43) A | 5.32 (2.02) A | 20.67 (3.58) A |
| More than BRL 15,000 (n = 186) | 4.38 (1.08) A | 2.44 (1.47) A | 5.83 (1.46) A | 2.11 (1.31) A | 4.87 (1.87) A | 19.62 (3.55) A |
| Prefer not to inform (n = 32) | 4.59 (1.36) A | 2.28 (1.30) A | 6.00 (1.22) A | 2.28 (1.49) A | 4.72 (2.25) A | 19.88 (4.06) A |
| p | 0.129 | 0.052 | 0.973 | 0.815 | 0.403 | 0.116 |
| Child’s gender * | ||||||
| Female (n = 200) | 4.55 (1.07) A | 2.68 (1.45) A | 5.84 (1.43) A | 2.15 (1.37) A | 4.78 (2.00) A | 20.00 (3.81) A |
| Male (n = 184) | 4.48 (1.13) A | 2.47 (1.37) A | 5.86 (1.35) A | 2.03 (1.34) A | 5.25 (1.84) B | 20.09 (3.30) A |
| p | 0.553 | 0.152 | 0.865 | 0.376 | 0.017 | 0.790 |
| Child’s age ** | ||||||
| 2 years (n = 109) | 4.34 (1.21) A | 2.60 (1.51) A | 6.00 (1.41) A | 2.07 (1.41) A | 5.14 (1.73) A | 20.15 (3.50) A |
| 3 years (n = 89) | 4.56 (1.16) A | 2.55 (1.42) A | 5.78 (1.29) A | 2.20 (1.24) A | 5.18 (1.93) A | 20.27 (3.40) A |
| 4 years (n = 79) | 4.61 (0.98) A | 2.59 (1.33) A | 5.52 (1.32) A | 2.05 (1.38) A | 5.00 (1.97) A | 19.77 (3.50) A |
| 5 years (n = 58) | 4.60 (0.99) A | 2.64 (1.28) A | 6.02 (1.63) A | 2.21 (1.47) A | 4.88 (2.26) A | 20.34 (4.24) A |
| 6 years (n = 49) | 4.55 (1.04) A | 2.51 (1.52) A | 6.00 (1.27) A | 1.86 (1.27) A | 4.55 (1.86) A | 19.47 (3.32) A |
| p | 0.419 A | 0.991 | 0.114 | 0.634 | 0.382 | 0.632 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dusi, R.; Botelho, R.B.A.; Nakano, E.Y.; Queiroz, F.L.N.d.; Zandonadi, R.P. Translation of the Satter’s Division of Responsibility in Feeding Questionnaire into Brazilian Portuguese: A Cross-Sectional Study. Nutrients 2023, 15, 2575. https://doi.org/10.3390/nu15112575
Dusi R, Botelho RBA, Nakano EY, Queiroz FLNd, Zandonadi RP. Translation of the Satter’s Division of Responsibility in Feeding Questionnaire into Brazilian Portuguese: A Cross-Sectional Study. Nutrients. 2023; 15(11):2575. https://doi.org/10.3390/nu15112575
Chicago/Turabian StyleDusi, Rafaella, Raquel Braz Assunção Botelho, Eduardo Yoshio Nakano, Fabiana Lopes Nalon de Queiroz, and Renata Puppin Zandonadi. 2023. "Translation of the Satter’s Division of Responsibility in Feeding Questionnaire into Brazilian Portuguese: A Cross-Sectional Study" Nutrients 15, no. 11: 2575. https://doi.org/10.3390/nu15112575