
Midlife Life’s Simple 7, Psychosocial Health, and Physical Frailty, Hospital Frailty, and Comprehensive Frailty 10 Years Later

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Exposure
2.3. Outcome
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
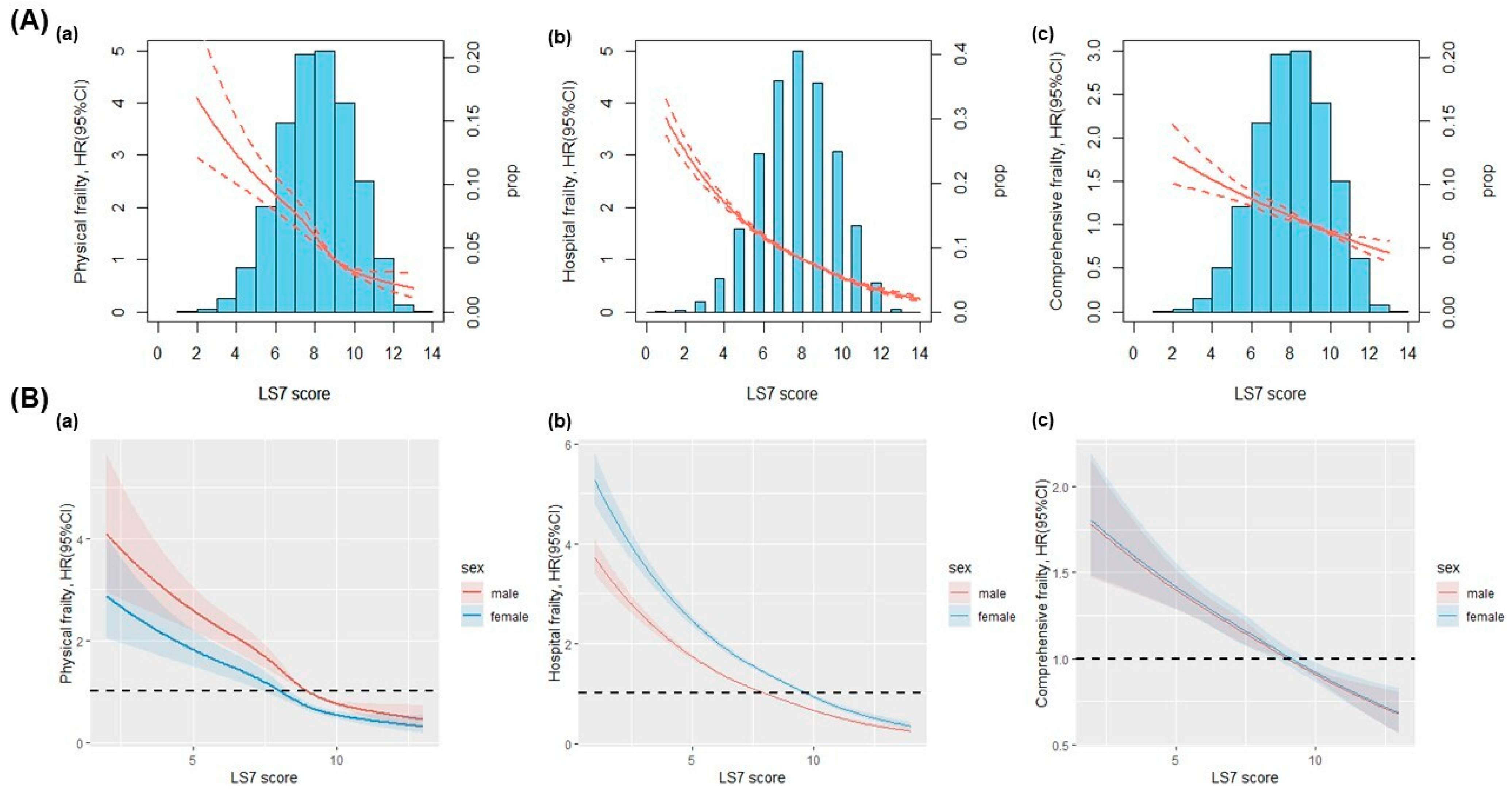
3.2. LS7 Score and Physical Frailty, Hospital Frailty, and Comprehensive Frailty
3.3. Psychosocial Health and Physical Frailty, Hospital Frailty, and Comprehensive Frailty
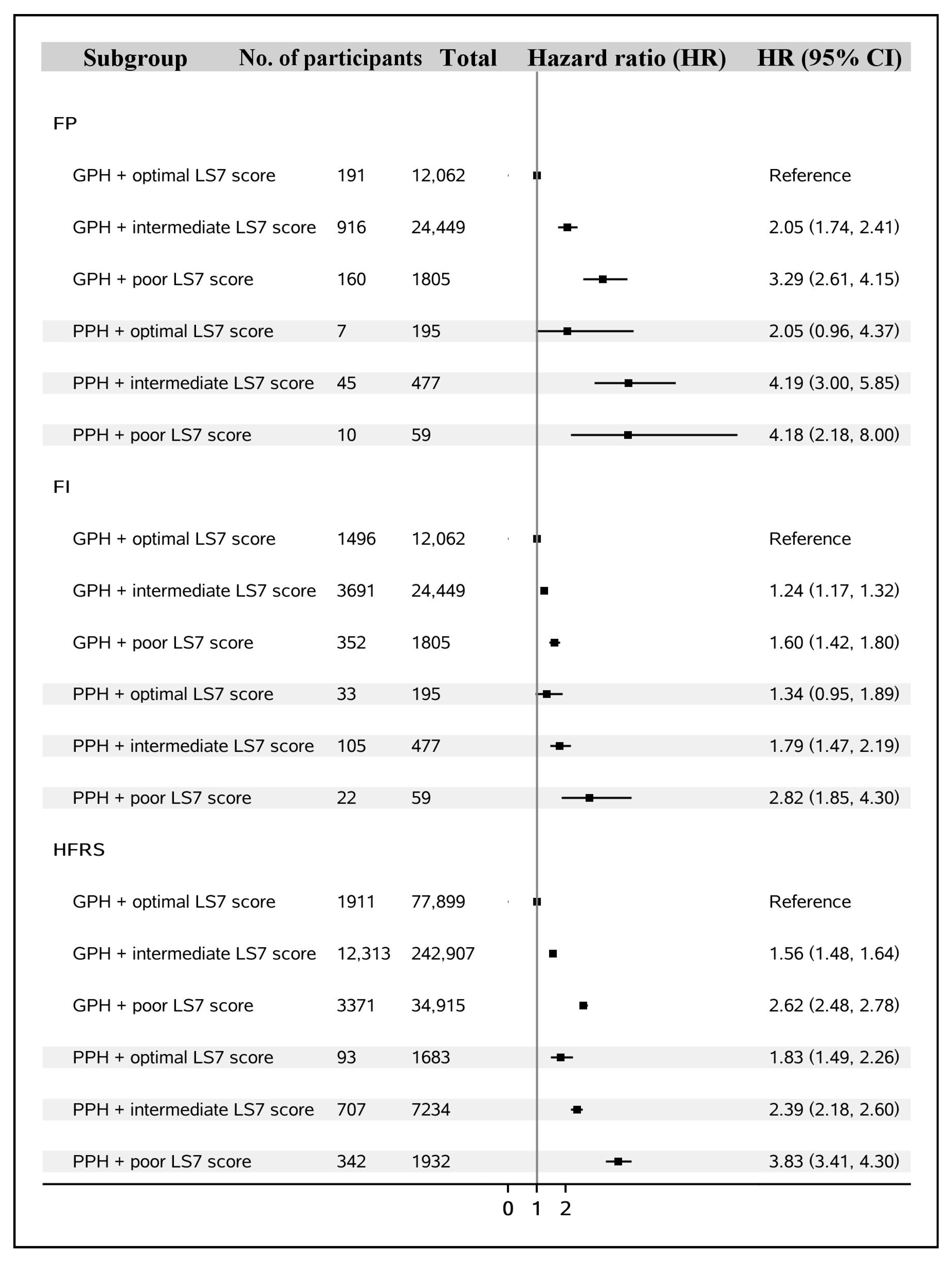
3.4. Synergistic Interactions between LS7 Score and Psychosocial Health Status on Risk of Frailty
4. Discussion
4.1. LS7 Score and Physical Frailty, Hospital Frailty, and Comprehensive Frailty
4.2. Psychosocial Health and Physical Frailty, Hospital Frailty, and Comprehensive Frailty
4.3. Synergistic Interactions between LS7 Score and Psychosocial Health Status on Risk of Frailty
4.4. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Zhong, G.C.; Zhou, X.; Guan, L.; Zhou, L. Frailty and risks of all-cause and cause-specific death in community-dwelling adults: A systematic review and meta-analysis. BMC Geriatr. 2022, 22, 725. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- United Nations. Our World Is Growing Older: UN DESA Releases New Report on Ageing. Available online: https://www.un.org/development/desa/en/news/population/our-world-is-growing-older.html (accessed on 25 January 2023).
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [PubMed]
- Graciani, A.; Garcia-Esquinas, E.; Lopez-Garcia, E.; Banegas, J.R.; Rodriguez-Artalejo, F. Ideal Cardiovascular Health and Risk of Frailty in Older Adults. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 239–245. [Google Scholar] [CrossRef]
- Palta, P.; Griswold, M.; Ranadive, R.; Bandeen-Roche, K.; Folsom, A.R.; Petruski-Ivleva, N.; Burgard, S.; Kucharska-Newton, A.; Windham, B.G. Midlife Cardiovascular Health and Robust Versus Frail Late-Life Status: The Atherosclerosis Risk in Communities Study. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 1222–1229. [Google Scholar] [CrossRef]
- Gale, C.R.; Westbury, L.; Cooper, C. Social isolation and loneliness as risk factors for the progression of frailty: The English Longitudinal Study of Ageing. Age Ageing 2018, 47, 392–397. [Google Scholar] [CrossRef]
- Jarach, C.M.; Tettamanti, M.; Nobili, A.; D’Avanzo, B. Social isolation and loneliness as related to progression and reversion of frailty in the Survey of Health Aging Retirement in Europe (SHARE). Age Ageing 2021, 50, 258–262. [Google Scholar] [CrossRef]
- Mehrabi, F.; Beland, F. Effects of social isolation, loneliness and frailty on health outcomes and their possible mediators and moderators in community-dwelling older adults: A scoping review. Arch. Gerontol. Geriatr. 2020, 90, 104119. [Google Scholar] [CrossRef]
- Bycroft, C.; Freeman, C.; Petkova, D.; Band, G.; Elliott, L.T.; Sharp, K.; Motyer, A.; Vukcevic, D.; Delaneau, O.; O’Connell, J.; et al. The UK Biobank resource with deep phenotyping and genomic data. Nature 2018, 562, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Fayosse, A.; Dumurgier, J.; Schnitzler, A.; Empana, J.P.; Ebmeier, K.P.; Dugravot, A.; Kivimaki, M.; Singh-Manoux, A. Association of ideal cardiovascular health at age 50 with incidence of dementia: 25 year follow-up of Whitehall II cohort study. BMJ 2019, 366, l4414. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.; Georgakis, M.K.; Neitzel, J.; Rannikmae, K.; Ewers, M.; Seshadri, S.; Sudlow, C.L.M.; Dichgans, M. Midlife vascular risk factors and risk of incident dementia: Longitudinal cohort and Mendelian randomization analyses in the UK Biobank. Alzheimers Dement. 2021, 17, 1422–1431. [Google Scholar] [CrossRef]
- Elovainio, M.; Hakulinen, C.; Pulkki-Raback, L.; Virtanen, M.; Josefsson, K.; Jokela, M.; Vahtera, J.; Kivimaki, M. Contribution of risk factors to excess mortality in isolated and lonely individuals: An analysis of data from the UK Biobank cohort study. Lancet Public. Health 2017, 2, e260–e266. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, e323–e332. [Google Scholar] [CrossRef] [PubMed]
- Petermann-Rocha, F.; Lyall, D.M.; Gray, S.R.; Esteban-Cornejo, I.; Quinn, T.J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Associations between physical frailty and dementia incidence: A prospective study from UK Biobank. Lancet Healthy Longev. 2020, 1, e58–e68. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.M.; Jylhava, J.; Pedersen, N.L.; Hagg, S. A Frailty Index for UK Biobank Participants. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Mitnitski, A. Frailty in relation to the accumulation of deficits. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 722–727. [Google Scholar] [CrossRef]
- Mutz, J.; Choudhury, U.; Zhao, J.; Dregan, A. Frailty in individuals with depression, bipolar disorder and anxiety disorders: Longitudinal analyses of all-cause mortality. BMC Med. 2022, 20, 274. [Google Scholar] [CrossRef]
- Mak, J.K.L.; Kuja-Halkola, R.; Wang, Y.; Hagg, S.; Jylhava, J. Frailty and comorbidity in predicting community COVID-19 mortality in the U.K. Biobank: The effect of sampling. J. Am. Geriatr. Soc. 2021, 69, 1128–1139. [Google Scholar] [CrossRef]
- Gilbert, T.; Neuburger, J.; Kraindler, J.; Keeble, E.; Smith, P.; Ariti, C.; Arora, S.; Street, A.; Parker, S.; Roberts, H.C.; et al. Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: An observational study. Lancet 2018, 391, 1775–1782. [Google Scholar] [CrossRef] [PubMed]
- Boreskie, K.F.; Rose, A.V.; Hay, J.L.; Kehler, D.S.; Costa, E.C.; Moffatt, T.L.; Arora, R.C.; Duhamel, T.A. Frailty status and cardiovascular disease risk profile in middle-aged and older females. Exp. Gerontol. 2020, 140, 111061. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, S.E.; Arianayagam, D.S.; Whincup, P.H.; Lennon, L.T.; Cryer, J.; Papacosta, A.O.; Iliffe, S.; Wannamethee, S.G. Cardiovascular risk profile and frailty in a population-based study of older British men. Heart 2015, 101, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Bowling, C.B.; Sloane, R.; Pieper, C.; Luciano, A.; Davis, B.R.; Simpson, L.M.; Einhorn, P.T.; Oparil, S.; Muntner, P. Association of Sustained Blood Pressure Control with Multimorbidity Progression Among Older Adults. J. Am. Geriatr. Soc. 2020, 68, 2059–2066. [Google Scholar] [CrossRef]
- Tajik, B.; Voutilainen, A.; Kauhanen, J.; Mazidi, M.; Lip, G.Y.H.; Tuomainen, T.P.; Isanejad, M. Lipid profile, lipid ratios, apolipoproteins, and risk of cardiometabolic multimorbidity in men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Lipids 2022, 57, 141–149. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Lopez Samaniego, L.; Rodriguez-Manas, L.; Bernabei, R.; Onder, G.; et al. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 659–666. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef]
- Mielke, N.; Schneider, A.; Huscher, D.; Ebert, N.; Schaeffner, E. Gender differences in frailty transition and its prediction in community-dwelling old adults. Sci. Rep. 2022, 12, 7341. [Google Scholar] [CrossRef]
- Abad-Diez, J.M.; Calderon-Larranaga, A.; Poncel-Falco, A.; Poblador-Plou, B.; Calderon-Meza, J.M.; Sicras-Mainar, A.; Clerencia-Sierra, M.; Prados-Torres, A. Age and gender differences in the prevalence and patterns of multimorbidity in the older population. BMC Geriatr. 2014, 14, 75. [Google Scholar] [CrossRef]
- Salive, M.E. Multimorbidity in older adults. Epidemiol. Rev. 2013, 35, 75–83. [Google Scholar] [CrossRef]
- Ding, Y.Y.; Kuha, J.; Murphy, M. Multidimensional predictors of physical frailty in older people: Identifying how and for whom they exert their effects. Biogerontology 2017, 18, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Uno, C.; Okada, K.; Matsushita, E.; Satake, S.; Kuzuya, M. Friendship-related social isolation is a potential risk factor for the transition from robust to prefrailty among healthy older adults: A 1-year follow-up study. Eur. Geriatr. Med. 2021, 12, 285–293. [Google Scholar] [CrossRef]
- De Biasio, J.C.; Mittel, A.M.; Mueller, A.L.; Ferrante, L.E.; Kim, D.H.; Shaefi, S. Frailty in Critical Care Medicine: A Review. Anesth. Analg. 2020, 130, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- Batty, G.D.; Gale, C.R.; Kivimaki, M.; Deary, I.J.; Bell, S. Comparison of risk factor associations in UK Biobank against representative, general population based studies with conventional response rates: Prospective cohort study and individual participant meta-analysis. BMJ 2020, 368, m131. [Google Scholar] [CrossRef] [PubMed]
- Fry, A.; Littlejohns, T.J.; Sudlow, C.; Doherty, N.; Adamska, L.; Sprosen, T.; Collins, R.; Allen, N.E. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants With Those of the General Population. Am. J. Epidemiol. 2017, 186, 1026–1034. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Allen, N.B.; Anderson, C.A.M.; Black, T.; Brewer, L.C.; Foraker, R.E.; Grandner, M.A.; Lavretsky, H.; Perak, A.M.; Sharma, G.; et al. Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct of Cardiovascular Health: A Presidential Advisory From the American Heart Association. Circulation 2022, 146, e18–e43. [Google Scholar] [CrossRef]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- Said, M.A.; Verweij, N.; van der Harst, P. Associations of Combined Genetic and Lifestyle Risks With Incident Cardiovascular Disease and Diabetes in the UK Biobank Study. JAMA Cardiol. 2018, 3, 693–702. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N | LS7 Score | Psychosocial Health | |||||
|---|---|---|---|---|---|---|---|---|
| Poor (0–5) | Intermediate (6–9) | Optimal (10–14) | p * | Good | Poor | p * | ||
| No. of participants | 39,047 | 1864 | 24,926 | 12,257 | 38,316 | 731 | ||
| Age (years, mean ± SD) | 64.0 ± 7.6 | 65.6 ± 6.9 | 65.1 ± 7.3 | 61.7 ± 7.6 | <0.001 | 64.1 ± 7.6 | 62.0 ± 7.5 | 0.506 |
| Sex | <0.001 | 0.105 | ||||||
| Male | 19,138 | 1206 (64.7) | 13,495 (54.1) | 4437 (36.2) | 18,758 (49.0) | 380 (52.0) | ||
| Female | 19,909 | 658 (35.3) | 11,431 (45.9) | 7820 (63.8) | 19,558 (51.0) | 351 (48.0) | ||
| Race/ethnicity | 0.693 | |||||||
| White | 37,984 | 1809 (97.1) | 24,259 (97.3) | 11,916 (97.2) | 37,295 (97.3) | 689 (94.2) | <0.001 | |
| Non-white | 1063 | 55 (2.9) | 667 (2.7) | 341 (2.8) | 1021 (2.7) | 42 (5.8) | ||
| Education level (years) | <0.001 | 0.011 | ||||||
| ≤10 | 13,759 | 839 (45.0) | 9382 (37.7) | 3538 (28.9) | 13,470 (35.1) | 289 (39.5) | ||
| 11–12 | 5197 | 259 (13.9) | 3270 (13.1) | 1668 (13.6) | 5091 (13.3) | 106 (14.5) | ||
| >12 | 20,091 | 766 (41.1) | 12,274 (49.2) | 7051 (57.5) | 19,755 (51.6) | 336 (46.0) | ||
| Income level (£) | <0.001 | <0.001 | ||||||
| Less than 18,000 | 2928 | 187 (10.0) | 1940 (7.8) | 801 (6.5) | 2792 (7.2) | 136 (18.6) | ||
| 18,000 to 30,999 | 7465 | 421 (22.6) | 5045 (20.2) | 1999 (16.3) | 7267 (19.0) | 198 (27.1) | ||
| 31,000 to 51,999 | 11,715 | 606 (32.5) | 7671 (30.8) | 3438 (28.1) | 11,492 (30.0) | 223 (30.5) | ||
| Greater than 52,000 | 16,939 | 650 (34.9) | 10,270 (41.2) | 6019 (49.1) | 16,765 (43.8) | 174 (23.8) | ||
| Alcohol status | <0.001 | <0.001 | ||||||
| Never | 905 | 27 (1.5) | 530 (2.1) | 348 (2.8) | 887 (2.3) | 18 (2.5) | ||
| Previous | 821 | 56 (3.0) | 532 (2.1) | 233 (1.9) | 791 (2.1) | 30 (4.1) | ||
| Current | 37,321 | 1781 (95.5) | 23,864 (95.8) | 11,676 (95.3) | 36,638 (95.6) | 683 (93.4) | ||
| Physical Frailty Phenotype | <0.001 | <0.001 | ||||||
| Non-frail | 15,833 | 502 (26.9) | 9575 (38.4) | 5756 (47.0) | 15,617 (40.8) | 216 (29.6) | ||
| Pre-frail | 21,885 | 1192 (64.0) | 14,390 (57.7) | 6303 (51.4) | 21,432 (55.9) | 453 (62.0) | ||
| Frail | 1329 | 170 (9.1) | 961 (3.9) | 198 (1.6) | 1267 (3.3) | 62 (8.4) | ||
| Frailty Index | <0.001 | <0.001 | ||||||
| Robust | 10,235 | 300 (16.1) | 6090 (24.4) | 3845 (31.4) | 10,144 (26.4) | 91 (12.4) | ||
| Pre-frail | 23,113 | 1190 (63.8) | 15,040 (60.4) | 6883 (56.2) | 22,633 (59.1) | 480 (65.7) | ||
| Frail | 5699 | 374 (20.1) | 3796 (15.2) | 1529 (12.4) | 5539 (14.5) | 160 (21.9) | ||
| Physical Frailty | Comprehensive Frailty | |||||||
|---|---|---|---|---|---|---|---|---|
| Events/N | All Participants | Women | Men | Events/N | All Participants | Women | Men | |
| LS7 score (lifestyle score + biometric score) | ||||||||
| Poor | 170/1864 | 1.00 | 1.00 | 1.00 | 374/1864 | 1.00 | 1.00 | 1.00 |
| Intermediate | 961/24,926 | 0.64 (0.54, 0.77) * | 0.64 (0.49, 0.83) * | 0.65 (0.51, 0.82) * | 3796/24,926 | 0.77 (0.69, 0.86) * | 0.81 (0.68, 0.96) * | 0.75 (0.66, 0.86) * |
| Optimal | 198/12,257 | 0.31 (0.25, 0.39) * | 0.30 (0.22, 0.42) * | 0.31 (0.22, 0.44) * | 1529/12,257 | 0.62 (0.55, 0.69) * | 0.63 (0.52, 0.75) * | 0.62 (0.53, 0.72) * |
| Lifestyle score | ||||||||
| Poor | 112/1253 | 1.00 | 1.00 | 1.00 | 252/1253 | 1.00 | 1.00 | 1.00 |
| Intermediate | 1069/27,162 | 0.57 (0.47, 0.70) * | 0.59 (0.44, 0.80) * | 0.55 (0.42, 0.72) * | 4097/27,162 | 0.78 (0.69, 0.89) * | 0.87 (0.70, 1.08) | 0.73 (0.62, 0.85) * |
| Optimal | 148/10,632 | 0.23 (0.18, 0.30) * | 0.26 (0.18, 0.37) * | 0.19 (0.13, 0.29) * | 1350/10,632 | 0.65 (0.56, 0.74) * | 0.72 (0.58, 0.90) * | 0.60 (0.51, 0.72) * |
| Smoking status | ||||||||
| Poor | 126/2452 | 1.00 | 1.00 | 1.00 | 381/2452 | 1.00 | 1.00 | 1.00 |
| Intermediate | 503/13,049 | 0.80 (0.65, 0.97) * | 0.62 (0.47, 0.82) * | 0.99 (0.74, 1.32) | 2083/13,049 | 1.09 (0.97, 1.21) | 1.14 (0.96, 1.35) | 1.04 (0.90, 1.20) |
| Optimal | 700/23,546 | 0.73 (0.60, 0.88) * | 0.65 (0.50, 0.84) * | 0.79 (0.59, 1.06) | 3235/23,546 | 0.97 (0.87, 1.08) | 1.03 (0.87, 1.22) | 0.91 (0.79, 1.05) |
| BMI | ||||||||
| Poor | 591/7306 | 1.00 | 1.00 | 1.00 | 1317/7306 | 1.00 | 1.00 | 1.00 |
| Intermediate | 495/16,577 | 0.47 (0.42, 0.54) * | 0.46 (0.39, 0.55) * | 0.48 (0.40, 0.58) * | 2395/16,577 | 0.83 (0.77, 0.89) * | 0.77 (0.70, 0.86) * | 0.88 (0.80, 0.97) * |
| Optimal | 243/15,164 | 0.26 (0.22, 0.31) * | 0.24 (0.19, 0.29) * | 0.31 (0.24, 0.41) * | 1987/15,164 | 0.75 (0.69, 0.81) * | 0.70 (0.63, 0.77) * | 0.82 (0.73, 0.91) * |
| Diet | ||||||||
| Poor | 125/3399 | 1.00 | 1.00 | 1.00 | 514/3399 | 1.00 | 1.00 | 1.00 |
| Intermediate | 1118/33,080 | 0.89 (0.74, 1.07) | 0.90 (0.69, 1.18) | 0.86 (0.66, 1.12) | 4808/33,080 | 0.91 (0.83, 0.99) * | 0.94 (0.82, 1.08) | 0.88 (0.78, 0.99) * |
| Optimal | 86/2568 | 0.74 (0.56, 0.98) * | 0.68 (0.45, 1.04) | 0.76 (0.52, 1.10) | 377/2568 | 0.83 (0.73, 0.95) * | 0.90 (0.73, 1.10) | 0.79 (0.66, 0.94) * |
| Physical activity | ||||||||
| Poor | 222/3572 | 1.00 | 1.00 | 1.00 | 618/3572 | 1.00 | 1.00 | 1.00 |
| Intermediate | 1038/31,669 | 0.70 (0.61, 0.81) * | 0.77 (0.63, 0.95) * | 0.64 (0.52, 0.80) * | 4559/31,669 | 0.90 (0.83, 0.98) * | 0.91 (0.80, 1.02) | 0.89 (0.79, 1.00) |
| Optimal | 69/3806 | 0.43 (0.33, 0.57) * | 0.50 (0.34, 0.74) * | 0.39 (0.27, 0.58) * | 522/3806 | 0.90 (0.80, 1.02) | 0.89 (0.75, 1.07) | 0.91 (0.77, 1.06) |
| Biometric score | ||||||||
| Poor | 53/698 | 1.00 | 1.00 | 1.00 | 125/698 | 1.00 | 1.00 | 1.00 |
| Intermediate | 606/14,571 | 0.95 (0.71, 1.28) | 0.99 (0.63, 1.54) | 0.95 (0.64, 1.41) | 2259/14,571 | 0.91 (0.76, 1.09) | 0.88 (0.66, 1.17) | 0.95 (0.75, 1.20) |
| Optimal | 670/23,778 | 0.89 (0.66, 1.21) | 0.87 (0.55, 1.38) | 0.92 (0.61, 1.38) | 3315/23,778 | 0.84 (0.70, 1.01) | 0.79 (0.60, 1.04) | 0.89 (0.71, 1.13) |
| Blood pressure | ||||||||
| Poor | 365/9143 | 1.00 | 1.00 | 1.00 | 1385/9143 | 1.00 | 1.00 | 1.00 |
| Intermediate | 802/23,555 | 1.03 (0.91, 1.18) | 0.91 (0.76, 1.09) | 1.16 (0.97, 1.40) | 3481/23,555 | 1.02 (0.96, 1.09) | 0.98 (0.89, 1.07) | 1.07 (0.98, 1.16) |
| Optimal | 162/6349 | 1.18 (0.96, 1.45) | 1.04 (0.81, 1.34) | 1.27 (0.85, 1.89) | 833/6349 | 0.98 (0.89, 1.07) | 0.95 (0.85, 1.07) | 0.94 (0.80, 1.11) |
| Cholesterol levels (LDL) | ||||||||
| Poor | 325/9363 | 1.00 | 1.00 | 1.00 | 1358/9363 | 1.00 | 1.00 | 1.00 |
| Intermediate | 737/18,068 | 1.07 (0.93, 1.22) | 0.97 (0.81, 1.16) | 1.19 (0.96, 1.47) | 2855/18,068 | 1.07 (1.00, 1.14) | 1.04 (0.94, 1.14) | 1.09 (0.99, 1.20) |
| Optimal | 267/11,616 | 0.91 (0.77, 1.07) | 0.92 (0.74, 1.13) | 0.83 (0.63, 1.11) | 1486/11,616 | 0.94 (0.87, 1.01) | 0.92 (0.83, 1.02) | 0.93 (0.83, 1.04) |
| Glycemic status (HbA1c) | ||||||||
| Poor | 86/780 | 1.00 | 1.00 | 1.00 | 175/780 | 1.00 | 1.00 | 1.00 |
| Intermediate | 255/4356 | 0.97 (0.74, 1.27) | 1.05 (0.68, 1.62) | 0.94 (0.67, 1.34) | 770/4356 | 0.84 (0.71, 0.99) * | 0.90 (0.68, 1.19) | 0.82 (0.67, 1.01) |
| Optimal | 988/33,911 | 0.85 (0.64, 1.14) | 1.06 (0.67, 1.69) | 0.70 (0.48, 1.02) | 4754/33,911 | 0.72 (0.62, 0.84) * | 0.78 (0.60, 1.02) | 0.70 (0.58, 0.85) * |
| Psychosocial health status (social isolation + loneliness) | ||||||||
| Good | 1267/38,316 | 1.00 | 1.00 | 1.00 | 5539/38,316 | 1.00 | 1.00 | 1.00 |
| Poor | 62/731 | 1.87 (1.44, 2.43) * | 1.47 (1.01, 2.15) * | 2.43 (1.68, 3.50) * | 160/731 | 1.46 (1.24, 1.71) * | 1.32 (1.04, 1.67) * | 1.59 (1.28, 1.97) * |
| Social isolation | ||||||||
| No | 1182/36,193 | 1.00 | 1.00 | 1.00 | 5192/36,193 | 1.00 | 1.00 | 1.00 |
| Yes | 147/2854 | 1.29 (1.08, 1.54) * | 1.10 (0.85, 1.43) | 1.48 (1.16, 1.89) * | 507/2854 | 1.19 (1.09, 1.31) * | 1.27 (1.11, 1.45) * | 1.13 (0.99, 1.28) |
| Loneliness | ||||||||
| No | 1013/33,628 | 1.00 | 1.00 | 1.00 | 4771/33,628 | 1.00 | 1.00 | 1.00 |
| Yes | 316/5419 | 1.67 (1.46, 1.90) * | 1.68 (1.42, 1.99) * | 1.65 (1.34, 2.00) * | 928/5419 | 1.20 (1.11, 1.28) * | 1.18 (1.07, 1.30) * | 1.23 (1.11, 1.38) * |
| Events/N | All Participants | Women | Men | |
|---|---|---|---|---|
| LS7 score (lifestyle score + biometric score) | ||||
| Poor | 3713/36,847 | 1.00 | 1.00 | 1.00 |
| Intermediate | 13,020/250,141 | 0.60 (0.58, 0.62) * | 0.59 (0.55, 0.62) * | 0.60 (0.58, 0.63) * |
| Optimal | 2004/79,582 | 0.39 (0.37, 0.41) * | 0.35 (0.32, 0.38) * | 0.43 (0.40, 0.46) * |
| Lifestyle score | ||||
| Poor | 2884/31,907 | 1.00 | 1.00 | 1.00 |
| Intermediate | 13,900/270,879 | 0.64 (0.62, 0.67) * | 0.61 (0.57, 0.65) * | 0.66 (0.63, 0.70) * |
| Optimal | 1953/63,784 | 0.43 (0.41, 0.46) * | 0.42 (0.38, 0.45) * | 0.45 (0.41, 0.49) * |
| Smoking status | ||||
| Poor | 2971/36,987 | 1.00 | 1.00 | 1.00 |
| Intermediate | 7993/129,052 | 0.76 (0.73, 0.80) * | 0.70 (0.66, 0.75) * | 0.82 (0.77, 0.87) * |
| Optimal | 7823/200,531 | 0.58 (0.56, 0.61) * | 0.55 (0.52, 0.59) * | 0.61 (0.58, 0.65) * |
| BMI | ||||
| Poor | 6794/88,695 | 1.00 | 1.00 | 1.00 |
| Intermediate | 7159/154,743 | 0.75 (0.72, 0.78) * | 0.74 (0.70, 0.78) * | 0.76 (0.73, 0.80) * |
| Optimal | 4784/123,132 | 0.77 (0.74, 0.80) * | 0.71 (0.67, 0.75) * | 0.84 (0.79, 0.89) * |
| Diet | ||||
| Poor | 5735/110,620 | 1.00 | 1.00 | 1.00 |
| Intermediate | 12,712/249,819 | 0.94 (0.91, 0.97) * | 0.97 (0.92, 1.02) | 0.92 (0.88, 0.96) * |
| Optimal | 290/6131 | 0.69 (0.62, 0.78) * | 0.81 (0.68, 0.98) * | 0.62 (0.53, 0.72) * |
| Physical activity | ||||
| Poor | 2952/38,506 | 1.00 | 1.00 | 1.00 |
| Intermediate | 13,445/284,383 | 0.76 (0.73, 0.79) * | 0.73 (0.69, 0.78) * | 0.78 (0.74, 0.82) * |
| Optimal | 2340/43,681 | 0.78 (0.73, 0.82) * | 0.81 (0.74, 0.88) * | 0.76 (0.71, 0.82) * |
| Biometric score | ||||
| Poor | 1139/10,126 | 1.00 | 1.00 | 1.00 |
| Intermediate | 9357/150,371 | 0.65 (0.61, 0.69) * | 0.62 (0.57, 0.68) * | 0.67 (0.61, 0.72) * |
| Optimal | 8241/206,073 | 0.55 (0.52, 0.59) * | 0.50 (0.46, 0.55) * | 0.59 (0.55, 0.65) * |
| Blood pressure | ||||
| Poor | 6221/97,863 | 1.00 | 1.00 | 1.00 |
| Intermediate | 11,163/217,499 | 0.93 (0.90, 0.96) * | 0.89 (0.85, 0.93) * | 0.95 (0.91, 0.99) * |
| Optimal | 1353/51,208 | 0.74 (0.70, 0.79) * | 0.65 (0.60, 0.70) * | 0.92 (0.84, 1.01) |
| Cholesterol levels (LDL) | ||||
| Poor | 3538/89,353 | 1.00 | 1.00 | 1.00 |
| Intermediate | 11,043/171,976 | 1.42 (1.36, 1.47) * | 1.32 (1.26, 1.39) * | 1.55 (1.46, 1.64) * |
| Optimal | 4156/105,241 | 1.32 (1.26, 1.38) * | 1.16 (1.08, 1.23) * | 1.51 (1.41, 1.61) * |
| Glycemic status (HbA1c) | ||||
| Poor | 2395/14,867 | 1.00 | 1.00 | 1.00 |
| Intermediate | 4262/53,509 | 0.59 (0.56, 0.62) * | 0.56 (0.51, 0.60) * | 0.62 (0.58, 0.66) * |
| Optimal | 12,080/298,194 | 0.42 (0.40, 0.44) * | 0.41 (0.38, 0.44) * | 0.43 (0.40, 0.45) * |
| Psychosocial health (social isolation + loneliness) | ||||
| Good | 17,595/355,721 | 1.00 | 1.00 | 1.00 |
| Poor | 1142/10,849 | 1.53 (1.44, 1.62) * | 1.52 (1.39, 1.66) * | 1.54 (1.41, 1.68) * |
| Social isolation | ||||
| No | 16,046/334,232 | 1.00 | 1.00 | 1.00 |
| Yes | 2691/32,338 | 1.36 (1.31, 1.42) * | 1.36 (1.28, 1.45) * | 1.37 (1.29, 1.45) * |
| Loneliness | ||||
| No | 14,082/301,219 | 1.00 | 1.00 | 1.00 |
| Yes | 4655/65,351 | 1.40 (1.35, 1.45) * | 1.36 (1.30, 1.43) * | 1.45 (1.38, 1.52) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; Zhou, C.; Dong, C.; Zhang, J.; Xie, Z.; Sun, H.; Fu, C.; Hao, W.; Zhu, D. Midlife Life’s Simple 7, Psychosocial Health, and Physical Frailty, Hospital Frailty, and Comprehensive Frailty 10 Years Later. Nutrients 2023, 15, 2412. https://doi.org/10.3390/nu15102412
Wang Q, Zhou C, Dong C, Zhang J, Xie Z, Sun H, Fu C, Hao W, Zhu D. Midlife Life’s Simple 7, Psychosocial Health, and Physical Frailty, Hospital Frailty, and Comprehensive Frailty 10 Years Later. Nutrients. 2023; 15(10):2412. https://doi.org/10.3390/nu15102412
Chicago/Turabian StyleWang, Qi, Chunmiao Zhou, Caiyun Dong, Jiajun Zhang, Ziwei Xie, Huizi Sun, Chunying Fu, Wenting Hao, and Dongshan Zhu. 2023. "Midlife Life’s Simple 7, Psychosocial Health, and Physical Frailty, Hospital Frailty, and Comprehensive Frailty 10 Years Later" Nutrients 15, no. 10: 2412. https://doi.org/10.3390/nu15102412