
In Underweight Women, Insufficient Gestational Weight Gain Is Associated with Adverse Obstetric Outcomes


Abstract
:1. Introduction
2. Materials and Methods
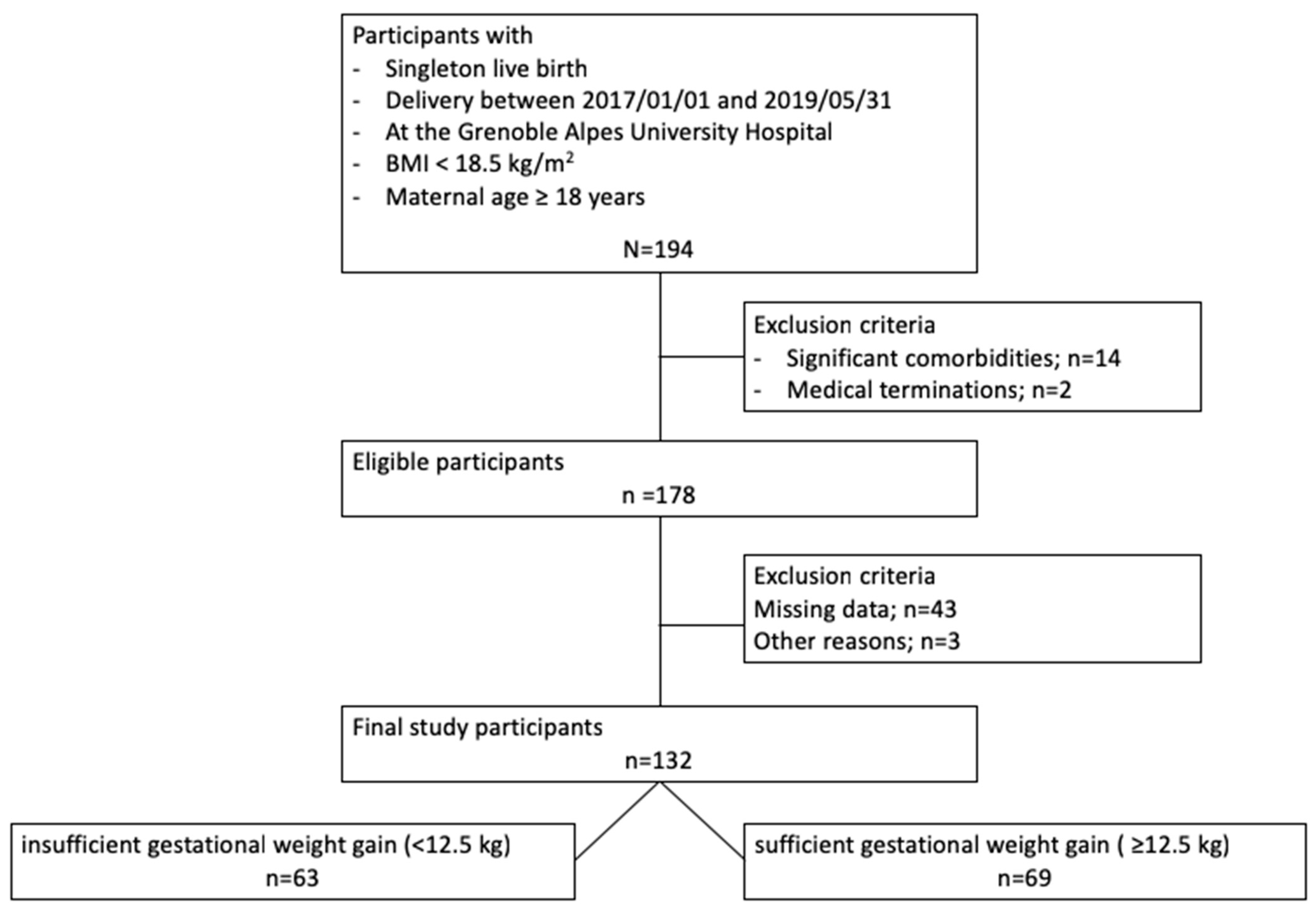
2.1. Study Population
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.1.3. Group Allocation
2.2. Collection of Data
2.2.1. Characteristics of the Participants
2.2.2. Main Outcomes
2.3. Ethics Statement
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Included Participants
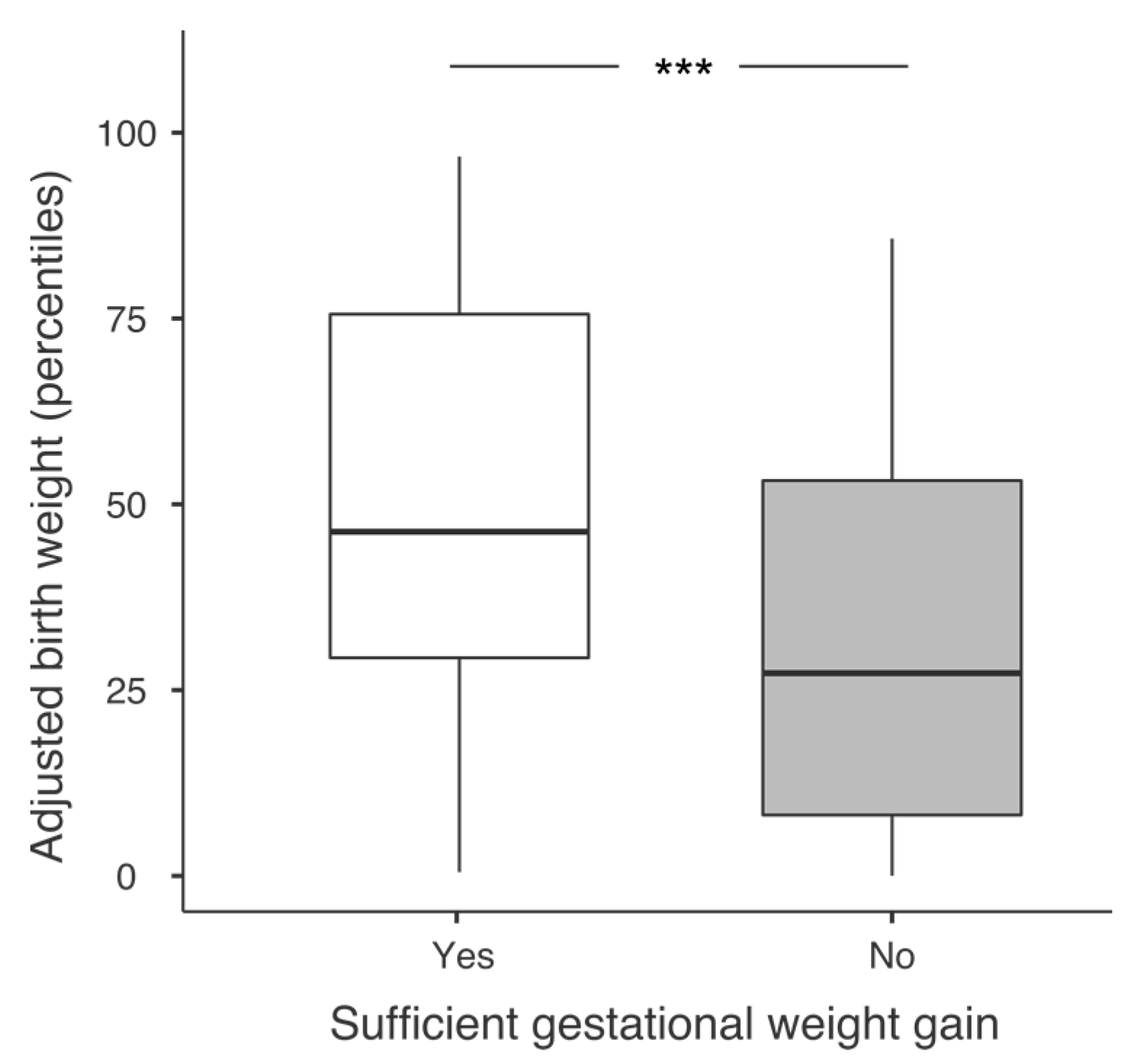
3.2. Primary Outcome: Adjusted Birth Weight and Percentages of SGA Newborns
3.3. Secondary Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siega-Riz, A.M.; Viswanathan, M.; Moos, M.-K.; Deierlein, A.; Mumford, S.; Knaack, J.; Thieda, P.; Lux, L.J.; Lohr, K.N. A Systematic Review of Outcomes of Maternal Weight Gain According to the Institute of Medicine Recommendations: Birthweight, Fetal Growth, and Postpartum Weight Retention. Am. J. Obstet. Gynecol. 2009, 201, 339.e1-14. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, K.M.; Yaktine, A.L.; Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Summary. Weight Gain during Pregnancy; National Academies Press (US): Washington, DC, USA, 2009.
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain with Maternal and Infant Outcomes: A Systematic Review and Meta-Analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Zhu, X.; Chen, Y.; Huang, D.; Tiemeier, H.; Chen, R.; Bao, W.; Zhao, Q. Association of Maternal Pre-Pregnancy Low or Increased Body Mass Index with Adverse Pregnancy Outcomes. Sci. Rep. 2021, 11, 3831. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Yang, W.; Wang, A.; Xiong, L.; Kong, F.; Liu, Z.; Xie, Z.; Wang, H. Effects of Pre-Pregnancy Body Mass Index on Pregnancy and Perinatal Outcomes in Women Based on a Retrospective Cohort. Sci. Rep. 2021, 11, 19863. [Google Scholar] [CrossRef] [PubMed]
- Ratnasiri, A.W.G.; Lee, H.C.; Lakshminrusimha, S.; Parry, S.S.; Arief, V.N.; DeLacy, I.H.; Yang, J.-S.; DiLibero, R.J.; Logan, J.; Basford, K.E. Trends in Maternal Prepregnancy Body Mass Index (BMI) and Its Association with Birth and Maternal Outcomes in California, 2007–2016: A Retrospective Cohort Study. PLoS ONE 2019, 14, e0222458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamelle, N.; Munoz, F.; Grandjean, H. Fetal growth from the AUDIPOG study. I. Establishment of reference curves. J. Gynecol. Obstet. Biol. Reprod. 1996, 25, 61–70. [Google Scholar]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Souche, R.; Mas, S.; Scatton, O.; Fabre, J.-M.; Gimeno, L.; Herrero, A.; Gaujoux, S. French Legislation on Retrospective Clinical Research: What to Know and What to Do. J. Visc. Surg. 2022, 159, 222–228. [Google Scholar] [CrossRef]
- Jeric, M.; Roje, D.; Medic, N.; Strinic, T.; Mestrovic, Z.; Vulic, M. Maternal Pre-Pregnancy Underweight and Fetal Growth in Relation to Institute of Medicine Recommendations for Gestational Weight Gain. Early Hum. Dev. 2013, 89, 277–281. [Google Scholar] [CrossRef]
- Enomoto, K.; Aoki, S.; Toma, R.; Fujiwara, K.; Sakamaki, K.; Hirahara, F. Pregnancy Outcomes Based on Pre-Pregnancy Body Mass Index in Japanese Women. PLoS ONE 2016, 11, e0157081. [Google Scholar] [CrossRef]
- Zilko, C.E.M.; Rehkopf, D.; Abrams, B. Association of Maternal Gestational Weight Gain with Short- and Long-Term Maternal and Child Health Outcomes. Am. J. Obstet. Gynecol. 2010, 202, 574.e1–574.e8. [Google Scholar] [CrossRef]
- Simas, T.A.M.; Waring, M.E.; Liao, X.; Garrison, A.; Sullivan, G.M.T.; Howard, A.E.; Hardy, J.R. Prepregnancy Weight, Gestational Weight Gain, and Risk of Growth Affected Neonates. J. Womens Health 2012, 21, 410–417. [Google Scholar] [CrossRef] [Green Version]
- Hung, T.-H.; Hsieh, T.-T. Pregestational Body Mass Index, Gestational Weight Gain, and Risks for Adverse Pregnancy Outcomes among Taiwanese Women: A Retrospective Cohort Study. Taiwan. J. Obstet. Gynecol. 2016, 55, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Lewandowska, M. Maternal Obesity and Risk of Low Birth Weight, Fetal Growth Restriction, and Macrosomia: Multiple Analyses. Nutrients 2021, 13, 1213. [Google Scholar] [CrossRef]
- Mohammad, N.; Sohaila, A.; Rabbani, U.; Ahmed, S.; Ahmed, S.; Ali, S.R. Maternal Predictors of Intrauterine Growth Retardation. J. Coll. Physicians Surg. Pak. 2018, 28, 681–685. [Google Scholar] [CrossRef] [Green Version]
- Pigatti Silva, F.; Souza, R.T.; Cecatti, J.G.; Passini, R.; Tedesco, R.P.; Lajos, G.J.; Nomura, M.L.; Rehder, P.M.; Dias, T.Z.; Oliveira, P.F.; et al. Role of Body Mass Index and Gestational Weight Gain on Preterm Birth and Adverse Perinatal Outcomes. Sci. Rep. 2019, 9, 13093. [Google Scholar] [CrossRef] [Green Version]
- Vivatkusol, Y.; Thavaramara, T.; Phaloprakarn, C. Inappropriate Gestational Weight Gain among Teenage Pregnancies: Prevalence and Pregnancy Outcomes. Int. J. Womens Health 2017, 9, 347–352. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.; Qi, Y.-N.; He, G.-L.; Yang, H.-M.; Zhang, G.-T.; Zou, K.; Luo, W.; Sun, X.; Liu, X.-H. Association between Maternal Weight Indicators and Iron Deficiency Anemia during Pregnancy: A Cohort Study. Chin. Med. J. 2018, 131, 2566–2574. [Google Scholar] [CrossRef]
- Bodnar, L.M.; Siega-Riz, A.M.; Arab, L.; Chantala, K.; McDonald, T. Predictors of Pregnancy and Postpartum Haemoglobin Concentrations in Low-Income Women. Public Health Nutr. 2004, 7, 701–711. [Google Scholar] [CrossRef]
- Pan, J.R.; Li, T.Y.; Tucker, D.; Chen, K.Y. Pregnancy Outcomes in Women with Active Anorexia Nervosa: A Systematic Review. J. Eat Disord. 2022, 10, 25. [Google Scholar] [CrossRef]
- Stewart, D.E.; Raskin, J.; Garfinkel, P.E.; MacDonald, O.L.; Robinson, G.E. Anorexia Nervosa, Bulimia, and Pregnancy. Am. J. Obstet. Gynecol. 1987, 157, 1194–1198. [Google Scholar] [CrossRef] [PubMed]
- Paulo, M.S.; Abdo, N.M.; Bettencourt-Silva, R.; Al-Rifai, R.H. Gestational Diabetes Mellitus in Europe: A Systematic Review and Meta-Analysis of Prevalence Studies. Front. Endocrinol. 2021, 12, 691033. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Liu, J.; Pujol, I.; López, A.; Martínez, M.J.; García-Patterson, A.; Adelantado, J.M.; Ginovart, G.; Corcoy, R. Inadequate Weight Gain According to the Institute of Medicine 2009 Guidelines in Women with Gestational Diabetes: Frequency, Clinical Predictors, and the Association with Pregnancy Outcomes. J. Clin. Med. 2020, 9, 3343. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sufficient Gestational Weight Gain (n = 69) | Insufficient Gestational Weight Gain (n = 63) | p Value | |
|---|---|---|---|
| Primipara | 31 (45%) | 26 (41%) | p = 0.7 |
| Hyperemesis gravidarium | 3 (4%) | 1 (2%) | p = 0.6 |
| Eating disorders | 2 (3%) | 2 (3%) | p = 1 |
| Toxic exposure during pregnancy | |||
| Smoking | 18 (27%) | 17 (28%) | p = 1 |
| Alcohol use | 0 (0%) | 1 (2%) | p = 0.5 |
| Illegal drugs use | 2 (3%) | 3 (5%) | p = 0.7 |
| Sufficient Gestational Weight Gain (n = 69) | Insufficient Gestational Weight Gain (n = 63) | p Value | |
|---|---|---|---|
| Pregnancy outcomes | |||
| Hypertensive disorder of pregnancy | 3/68 (4%) | 1/63 (2%) | p = 0.5 |
| Gestational diabetes | 3/68 (4%) | 7/61 (12%) | p = 0.3 |
| Anaemia | 18/58 (31%) | 23/46 (50%) | p = 0.026 |
| Premature rupture of membranes | 13/68 (19%) | 25/60 (42%) | p = 0.008 |
| Threatened preterm labor | 9/69 (13%) | 11/63 (18%) | p = 0.4 |
| Intrauterine growth restriction | 3/69 (4%) | 10/59 (17%) | p = 0.036 |
| Gestational age delivery (weeks) | 40.1 (1.5) | 39.3 (2.2) | p = 0.017 |
| Preterm delivery (<37 weeks) | 4/69 (6%) | 8/63 (13%) | p = 0.2 |
| Caesarean delivery | 7/69 (10%) | 7/63 (11%) | p = 0.8 |
| Newborns characteristics | |||
| Umbilical artery pH | 7.26 (0.09) | 7.29 (0.10) | p = 0.08 |
| Apgar Score < 7 (at 5 min) | 0/69 (0%) | 3/63 (5%) | p = 1 |
| Male infants (%) | 29/69 (42%) | 31/63 (49%) | p = 0.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montvignier Monnet, A.; Savoy, D.; Préaubert, L.; Hoffmann, P.; Bétry, C. In Underweight Women, Insufficient Gestational Weight Gain Is Associated with Adverse Obstetric Outcomes. Nutrients 2023, 15, 57. https://doi.org/10.3390/nu15010057
Montvignier Monnet A, Savoy D, Préaubert L, Hoffmann P, Bétry C. In Underweight Women, Insufficient Gestational Weight Gain Is Associated with Adverse Obstetric Outcomes. Nutrients. 2023; 15(1):57. https://doi.org/10.3390/nu15010057
Chicago/Turabian StyleMontvignier Monnet, Alizée, Delphine Savoy, Lise Préaubert, Pascale Hoffmann, and Cécile Bétry. 2023. "In Underweight Women, Insufficient Gestational Weight Gain Is Associated with Adverse Obstetric Outcomes" Nutrients 15, no. 1: 57. https://doi.org/10.3390/nu15010057