
Osteosarcopenic Adiposity and Nutritional Status in Older Nursing Home Residents during the COVID-19 Pandemic

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometric and Bioimpedance Measurements
2.3. Mini Nutritional Assessment (MNA)
2.4. Statistical Analysis
Power Analysis
3. Results
3.1. General and Body Composition Data
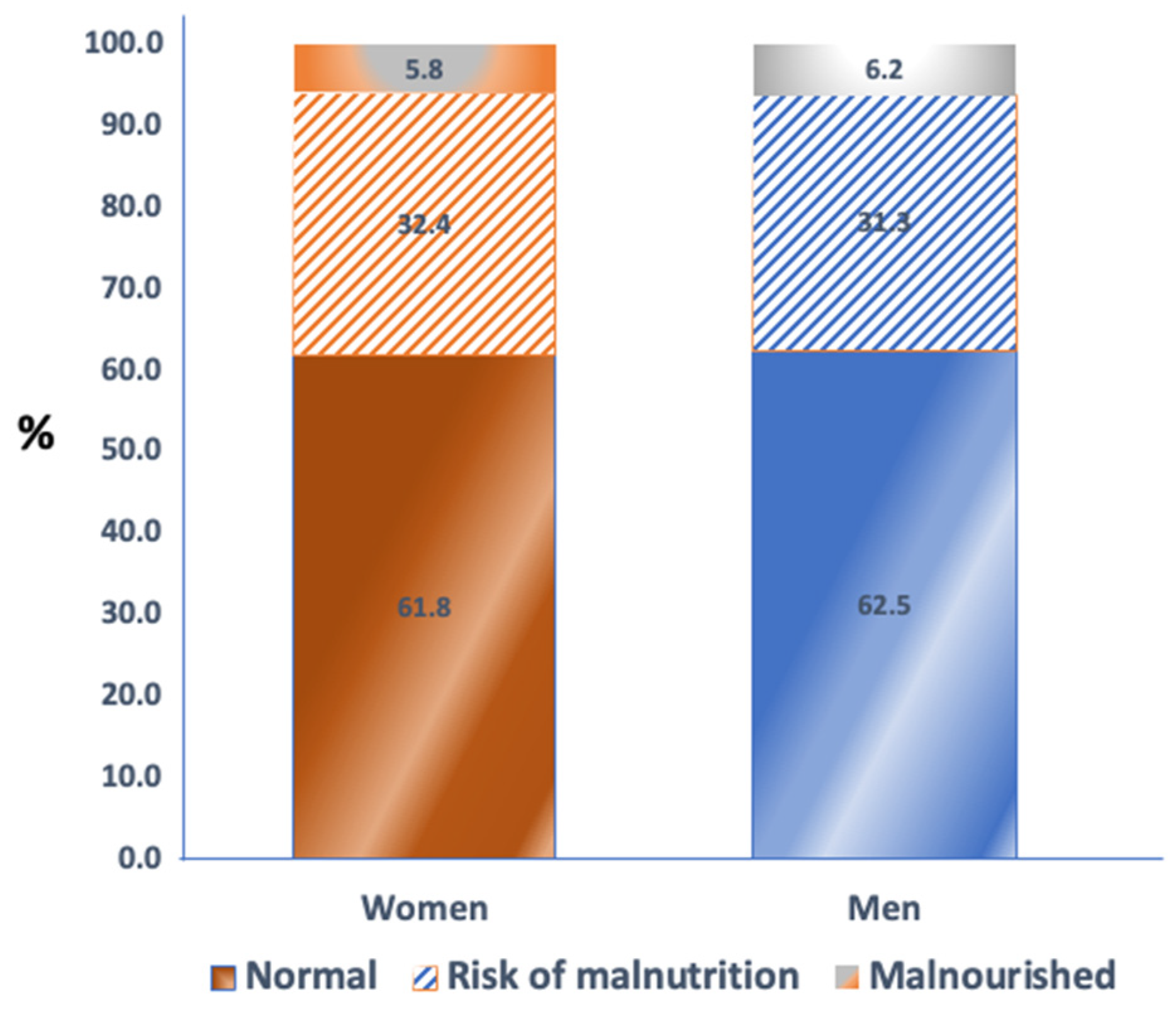
3.2. Nutritional Assessment
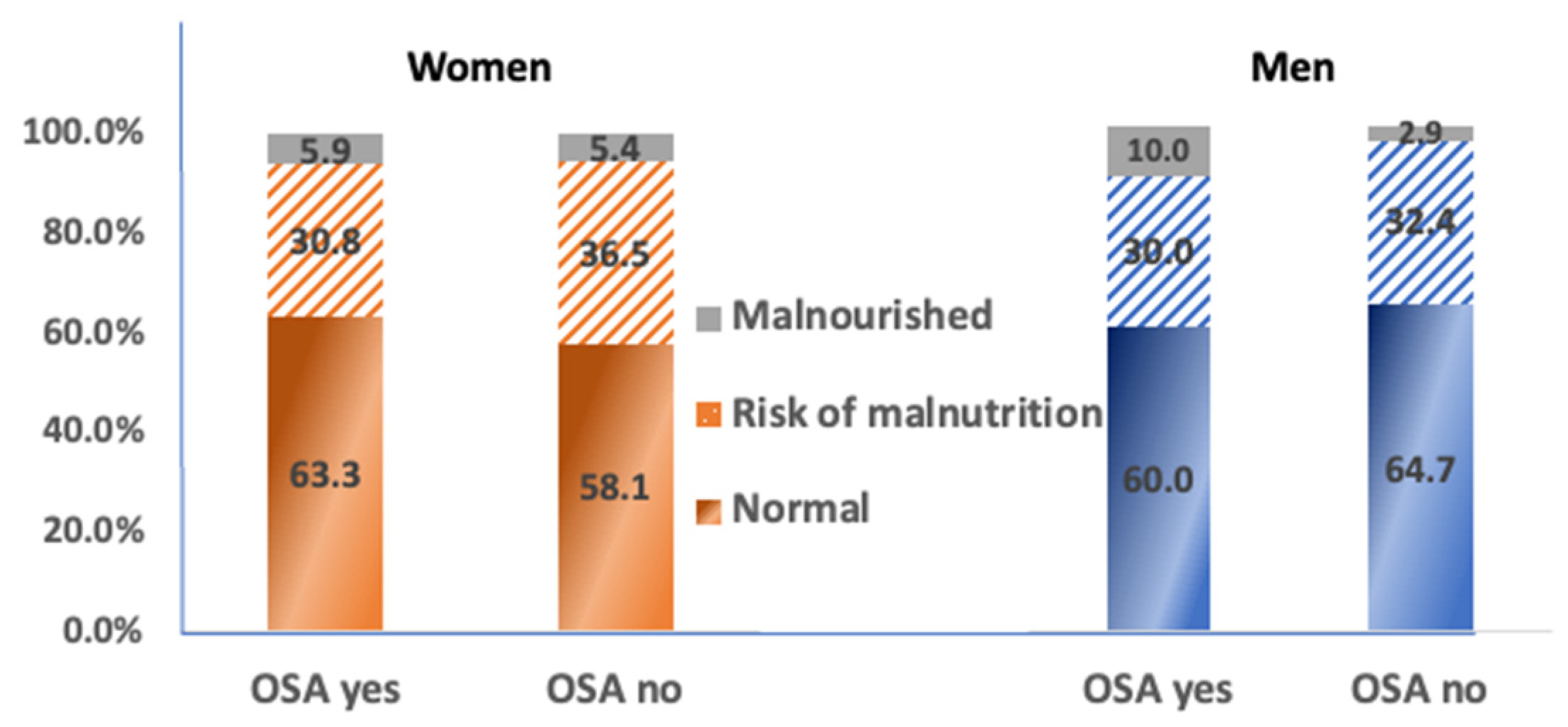
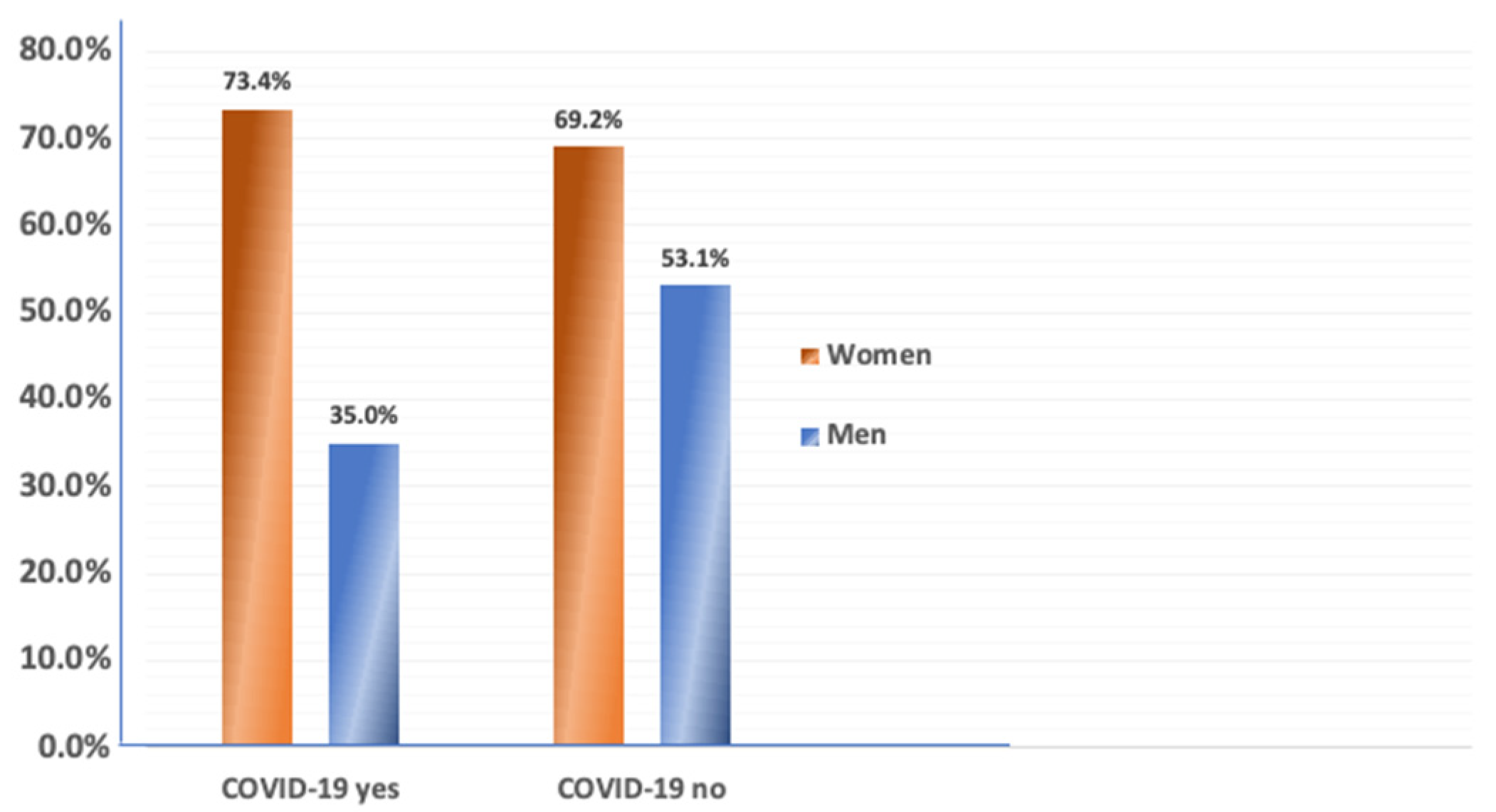
3.3. Body Composition, Nutrition and COVID-19
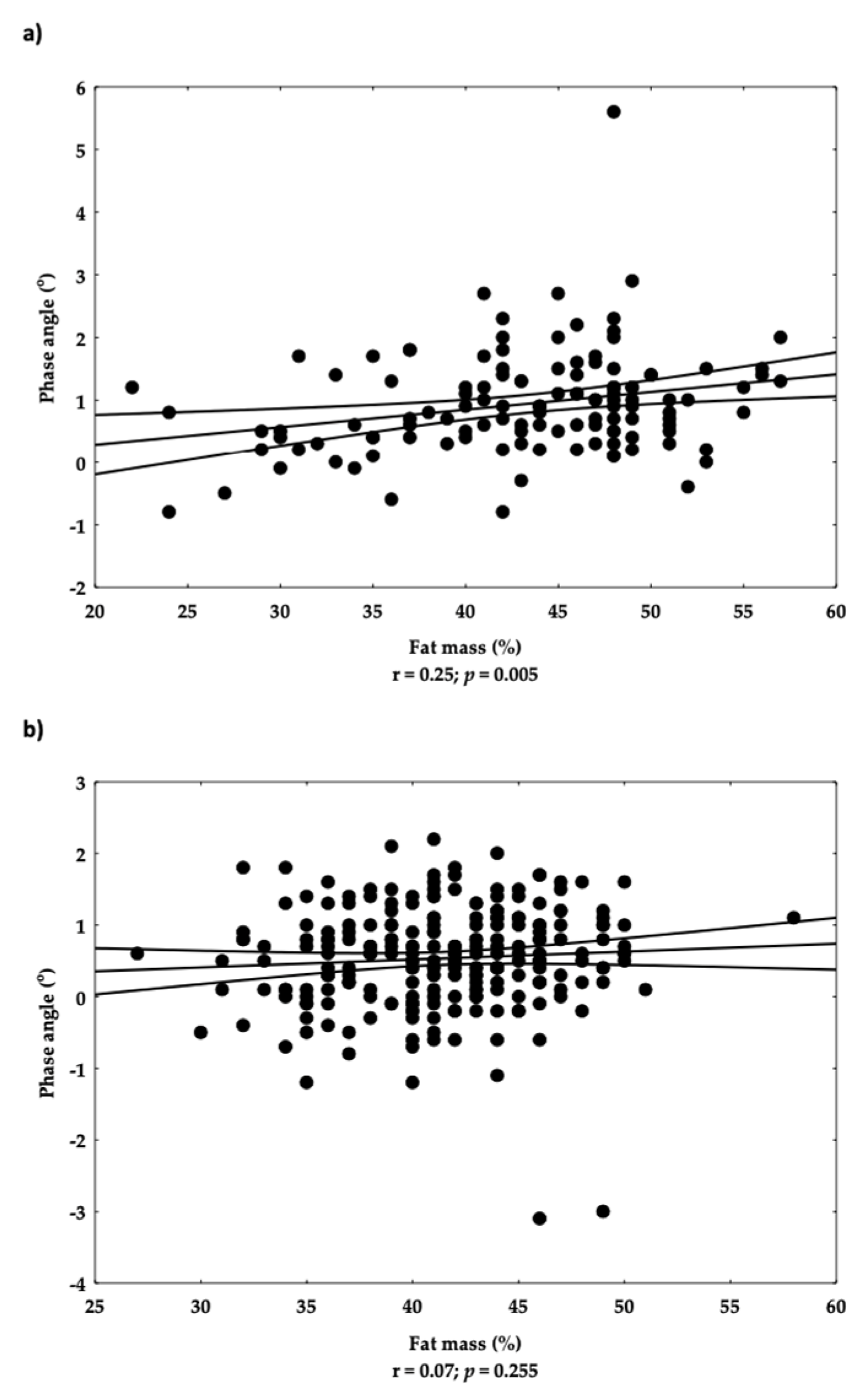
3.4. Analyses of Associations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, D.Y.; Shin, S. Association of sarcopenia with osteopenia and osteoporosis in community-dwelling older Korean adults: A cross-sectional study. J. Clin. Med. 2021, 11, 129. [Google Scholar] [CrossRef] [PubMed]
- Ilich, J.Z.; Gilman, J.C.; Cvijetic, S.; Boschiero, D. Chronic stress contributes to osteosarcopenic adiposity via inflammation and immune modulation: The case for more precise nutritional investigation. Nutrients 2020, 12, 989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, D.; Johansson, J.; Ebeling, P.R.; Nordstrom, P.; Nordstrom, A. Adiposity without obesity: Associations with osteoporosis, sarcopenia, and falls in the Healthy Ageing Initiative Cohort Study. Obesity 2020, 28, 2232–2241. [Google Scholar] [CrossRef]
- Ilich, J.Z. Nutritional and behavioral approaches to body composition and low-grade chronic inflammation management for older adults in the ordinary and COVID-19 times. Nutrients 2020, 12, 3898. [Google Scholar] [CrossRef] [PubMed]
- de França, N.A.G.; Peters, B.S.E.; dos Santos, E.A.; Lima, M.M.S.; Fisberg, R.M.; Martini, L.A. Obesity associated with low lean mass and low bone density has higher impact on general health in middle-aged and older adults. J. Obes. 2020, 2020, 8359616. [Google Scholar] [CrossRef]
- Kelly, O.; Gilman, J.; Boschiero, D.; Ilich, J. Osteosarcopenic obesity: Current knowledge, revised identification criteria and treatment principles. Nutrients 2019, 11, 747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilich, J.Z.; Kelly, O.J.; Inglis, J.E.; Panton, L.P.; Duque, G.; Ormsbee, M.J. Interrelationship among muscle, fat, and bone: Connecting the dots on cellular, hormonal, and whole-body levels. Ageing Res. Rev. 2014, 15, 51–60. [Google Scholar] [CrossRef]
- Ilich, J.Z. Osteosarcopenic adiposity syndrome update and the role of associated minerals and vitamins. Proc. Nutr. Soc. 2021, 80, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.A.; Kurniawan, A.A. Dreadful consequences of sarcopenia and osteoporosis due to COVID-19 containment. Geriatr. Orthop. Surg. Rehabil. 2021, 12, 2151459321992746. [Google Scholar] [CrossRef] [PubMed]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in patients younger than 60 years is a risk factor for COVID-19 hospital admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [PubMed]
- Welch, C.; Greig, C.; Masud, T.; Wilson, D.; Jackson, T.A. COVID-19 and acute sarcopenia. Aging Dis. 2020, 11, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Molfino, A.; Imbimbo, G.; Rizzo, V.; Muscaritoli, M.; Alampi, D. The link between nutritional status and outcomes in COVID-19 patients in ICU: Is obesity or sarcopenia the real problem? Eur. J. Intern. Med. 2021, 91, 93–95. [Google Scholar] [CrossRef]
- Hernández-Martínez, P.; Olmos, J.M.; Llorca, J.; Hernández, J.L.; González-Macías, J. Sarcopenic osteoporosis, sarcopenic obesity, and sarcopenic osteoporotic obesity in the Camargo cohort (Cantabria, Spain). Arch. Osteoporos. 2022, 17, 105. [Google Scholar] [CrossRef] [PubMed]
- Kolbaşı, E.N.; Demirdağ, F. Prevalence of osteosarcopenic obesity in community-dwelling older adults: A cross-sectional retrospective study. Arch. Osteoporos. 2020, 15, 166. [Google Scholar] [CrossRef]
- Szlejf, C.; Parra-Rodríguez, L.; Rosas-Carrasco, O. Osteosarcopenic obesity: Prevalence and relation with frailty and physical performance in middle-aged and older women. J. Am. Med. Dir. Assoc. 2017, 18, 733.e1–733.e5. [Google Scholar] [CrossRef]
- Keser, I.; Cvijetić, S.; Ilić, A.; Colić Barić, I.; Boschiero, D.; Ilich, J.Z. Assessment of body composition and dietary intake in nursing-home residents: Could lessons learned from the COVID-19 pandemic be used to prevent future casualties in older individuals? Nutrients 2021, 13, 1510. [Google Scholar] [CrossRef]
- White, E.M.; Wetle, T.F.; Reddy, A.; Baier, R.R. Front-line nursing home staff experiences during the COVID-19 pandemic. J. Am. Med. Dir. Assoc. 2021, 22, 199–203. [Google Scholar] [CrossRef]
- Akamatsu, Y.; Kusakabe, T.; Arai, H.; Yamamoto, Y.; Nakao, K.; Ikeue, K.; Ishihara, Y.; Tagami, T.; Yasoda, A.; Ishii, K.; et al. Phase angle from bioelectrical impedance analysis is a useful indicator of muscle quality. J. Cachexia Sarcopenia Muscle 2022, 13, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Santana, N.D.M.; Pinho, C.P.S.; da Silva, C.P.; dos Santos, N.F.; Mendes, R.M.L. Phase angle as a sarcopenia marker in hospitalized elderly patients. Nutr. Clin. Pract. 2018, 33, 232–237. [Google Scholar] [CrossRef]
- Stobaus, N.; Pirlich, M.; Valentini, L.; Schulzke, J.D.; Norman, K. Determinants of bioelectrical phase angle in disease. Br. J. Nutr. 2012, 107, 1217–1220. [Google Scholar] [CrossRef]
- Lee, Y.; Kwon, O.; Shin, C.S.; Lee, S.M. Use of bioelectrical impedance analysis for the assessment of nutritional status in critically ill patients. Clin. Nutr. Res. 2015, 4, 32. [Google Scholar] [CrossRef] [Green Version]
- Vellas, B.; Guigoz, Y.; Garry, P.J.; Nourhashemim, F.; Bennahum, D.; Lauque, S.; Albarede, J.L. The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Vellas, B.; Villars, H.; Abellan, G.; Soto, M.E.; Rolland, Y.; Guigoz, Y.; Morley, J.E.; Chumlea, W.; Salva, A.; Rubenstein, L.Z.; et al. Overview of the MNA®—Its history and challenges. J. Nutr. Health Aging 2006, 10, 456–463. [Google Scholar]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. MNA-International Group. Validation of the Mini Nutritional Assessment short-form (MNA-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Zhang, W.; Han, P.; Kohzuki, M.; Guo, Q. Ostesarrcopenic obesity associated with poor physical performance in the elderly Chinese community. Clin. Interv. Aging 2020, 15, 1343–1352. [Google Scholar] [CrossRef]
- Perna, S.; Spadaccini, D.; Nichetti, M.; Avanzato, I.; Faliva, M.A.; Rondanelli, M. Osteosarcopenic visceral obesity and osteosarcopenic subcutaneous obesity, two new phenotypes of sarcopenia: Prevalence, metabolic profile, and risk factors. J. Aging Res. 2018, 16, 2018:6147426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salech, F.; Marquez, C.; Lera, L.; Angel, B.; Saguez, R.; Albala, C. Osteosrcopenia predicts falls, fractures, and mortality in chilean community-dwelling older adults. J. Am. Med. Dir. Assoc. 2021, 22, 853–858. [Google Scholar] [CrossRef] [PubMed]
- Tsigos, C.; Stefanaki, C.; Lambrou, G.I.; Boschiero, D.; Chrousos, G.P. Stress and inflammatory biomarkers and symptoms are associated with bioimpedance measures. Eur. J. Clin. Investig. 2015, 45, 126–134. [Google Scholar] [CrossRef]
- Peppa, M.; Stefanaki, C.; Papaefstathiou, A.; Boschiero, D.; Dimitriadis, G.; Chrousos, G.P. Bioimpedance analysis vs. DEXA as a screening tool for osteosarcopenia in lean, overweight and obese Caucasian postmenopausal females. Hormones 2017, 16, 181–193. [Google Scholar]
- Straub, R.H.; Ehrenstein, B.; Günther, F.; Rauch, L.; Trendafilova, N.; Boschiero, D.; Grifka, J.; Fleck, M. Increased extracellular water measured by bioimpedance and by increased serum levels of atrial natriuretic peptide in RA patients-signs of volume overload. Clin. Rheumatol. 2017, 36, 1041–1051. [Google Scholar] [CrossRef]
- Chang, K.P.; Center, J.R.; Nguyen, T.V.; Eisman, J.A. Incidence of hip and other osteoporotic fractures in elderly men and women: Dubbo Osteoporosis Epidemiology Study. J. Bone Miner. Res. 2004, 19, 532–536. [Google Scholar] [CrossRef]
- Orsso, C.E.; Mackenzie, M.; Alberga, A.S.; Sharma, A.M.; Richer, L.; Rubin, D.A.; Prado, C.M.; Haqq, A.M. The use of magnetic resonance imaging to characterize abnormal body composition phenotypes in youth with Prader–Willi syndrome. Metabolism 2017, 69, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Parrish, A.R. The impact of aging on epithelial barriers. Tissue Barriers 2017, 5, e1343172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.S.; Lee, G.Y.; Seo, Y.M.; Seo, S.H.; Yoo, J.I. The relationship between extracellular water-to-body water ratio and sarcopenia according to the newly revised Asian Working Group for Sarcopenia: 2019 Consensus Update. Aging Clin. Exp. Res. 2021, 33, 2471–2477. [Google Scholar] [CrossRef]
- Tanaka, S.; Ando, K.; Kobayashi, K.; Nakashima, H.; Seki, T.; Ishizuka, S.; Machino, M.; Morozumi, M.; Kanbara, S.; Ito, S.; et al. Higher extracellular water-to-total body water ratio more strongly reflects the locomotive syndrome risk and frailty than sarcopenia. Arch. Gerontol. Geriatr. 2020, 88, 104042. [Google Scholar] [CrossRef]
- Bian, A.L.; Hu, H.Y.; Rong, Y.D.; Wang, J.; Wang, J.X.; Zhou, X.Z. A study on relationship between elderly sarcopenia and inflammatory factors IL-6 and TNF. Eur. J. Med. Res. 2017, 22, 25. [Google Scholar] [CrossRef] [Green Version]
- Doumit, J.H.; Nasser, R.N.; Hanna, D.R. Nutritional and health status among nursing home residents in Lebanon: Comparison across gender in a national cross sectional study. BMC Public Health 2014, 14, 629. [Google Scholar] [CrossRef] [Green Version]
- Madeira, T.; Peixoto-Plácido, C.; Sousa-Santos, N.; Santos, O.; Alarcão, V.; Goulão, B.; Mendonça, N.; Nicola, P.J.; Yngve, A.; Bye, A.; et al. Malnutrition among older adults living in Portuguese nursing homes: The PEN-3S study. Public Health Nutr. 2018, 15, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauly, L.; Stehle, P.; Volkert, D. Nutritional situation of elderly nursing home residents. Z. Gerontol. Geriatr. 2007, 40, 3–12. [Google Scholar] [CrossRef]
- JafariNasabian, P.; Inglis, J.E.; Reilly, W.; Kelly, O.J.; Ilich, J.Z. Aging human body: Changes in bone, muscle and body fat with consequent changes in nutrient intake. J. Endocrinol. 2017, 234, R37–R51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Groot, L.C.; Beck, A.M.; Schroll, M.; van Staveren, W.A. Evaluating the DETERMINE Your Nutritional Health Checklist and the Mini Nutritional Assessment as tools to identify nutritional problems in elderly Europeans. Eur. J. Clin. Nutr. 1998, 52, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Vranešić Bender, D.; Kovačević, M.; Hanževački, M.; Vrabec, B.; Benković, V.; Domislović, V.; Krznarić, Ž. Nutritional issues and nutrition support in older home care patients in the city of Zagreb. Acta Clin. Croat. 2017, 56, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Souto Barreto, P.; Zanandrea, V.; Lapeyre-Mestre, M.; Cesari, M.; Vellas, B.; Rolland, Y. Obesity in nursing home residents: A cross-sectional study. J. Nurs. Home Res. 2015, 1, 6–10. [Google Scholar] [CrossRef]
- Marihart, C.L.; Brunt, A.R.; Geraci, A.A. The high price of obesity in nursing homes. Care Manag. J. 2015, 16, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Abadía Otero, J.; Briongos Figuero, L.S.; Gabella Mattín, M.; Usategui Martín, I.; Cubero Morais, P.; Cuellar Olmedo, L.; Inglada Galiana, L.; Dueñas Gutiérrez, C.; Carretero Gómez, J.; Corral Gudino, L.; et al. The nutritional status of the elderly patient infected with COVID-19: The forgotten risk factor? Curr. Med. Res. Opin. 2021, 37, 549–554. [Google Scholar] [CrossRef]
- Pérez-Rodríguez, P.; Díaz de Bustamante, M.; Aparicio Mollá, S.; Arenas, M.C.; Jiménez-Armero, S.; Lacosta Esclapez, P.; González-Espinoza, L.; Bermejo Boixareu, C. Functional, cognitive, and nutritional decline in 435 elderly nursing home residents after the first wave of the COVID-19 Pandemic. Eur. Geriatr. Med. 2021, 12, 1137–1145. [Google Scholar] [CrossRef]
- Ngadiarti, I.; Muntikah, M.; Nurkolis, F.; Gunawan, W.B. Malnutrition during pandemic among home-nursed and community-dwelling elderly. Nutr. Clín. Diet. Hosp. 2022, 42, 134–145. [Google Scholar]
- Alvarez-Altamirano, K.; Bejarano-Rosales, M.P.; Gonzalez-Rosas, E.A.; Gallardo, A.G.; Ruiz-Lara, E.; Loza-Muro, A.; Fuchs-Tarlovsky, V.; Cruz, D.N.; Lee-Orozco, K.P. Body composition in recovered COVID-19 patients. Clin. Nutr. ESPEN 2021, 46, S594. [Google Scholar] [CrossRef]
- Czeck, M.A.; Roelofs, E.J.; Evanoff, N.G.; Dengel, D.R. No Changes in Body Composition in NCAA Division I Collegiate Football Players because of COVID-19 Restrictions. J. Strength Cond. Res. 2022, 36, 1749–1752. [Google Scholar] [CrossRef]
- Del Brutto, O.H.; Mera, R.M.; Rumbea, D.A.; Pérez, P.; Recalde, B.Y.; Sedler, M.J. Body Composition in Community-Dwelling Older Adults Before and After SARS-CoV-2 Infection: A Longitudinal Prospective Study in a Rural Village Struck by the Pandemic. J. Prim. Care Community Health 2021, 12, 21501327211047781. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895.e20. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Chen, D.; Yuan, D.; Lausted, C.; Choi, J.; Dai, C.L.; Voillet, V.; Duvvuri, V.R.; Scherler, K.; Troisch, P.; et al. Multi-Omics Resolves a Sharp Disease-State Shift between Mild and Moderate COVID-19. Cell 2020, 183, 1479–1495.e20. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Su, Y.; Baloni, P.; Chen, D.; Pavlovitch-Bedzyk, A.J.; Yuan, D.; Duvvuri, V.R.; Ng, R.H.; Choi, J.; Xie, J.; et al. Integrated analysis of plasma and single immune cells uncovers metabolic changes in individuals with COVID-19. Nat. Biotechnol. 2022, 40, 110–120. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Women (n = 296) | Men (n = 69) | p (t-Test) |
|---|---|---|---|
| Age (years) | 84.3 ± 5.6 | 83.1 ± 7.3 | 0.699 |
| Height (cm) | 156.0 ± 6.1 | 171.2 ± 7.6 | <0.001 |
| Weight (kg) | 70.7 ± 12.8 | 80.7 ± 11.3 | <0.001 |
| Time in NH (mos.) | 48.3 ± 40.1 | 42.1 ± 43.3 | 0.256 |
| BMI (kg/m2) | 29.0 ± 5.1 | 27.5 ± 3.8 | 0.027 |
| FM (%) | 43.0 ± 5.4 | 37.7 ± 5.6 | <0.001 |
| AAT (cm2) | 489.8 ± 150.8 | 529.5 ± 148.7 | 0.048 |
| IMAT (%) | 2.8 ± 0.4 | 2.8 ± 0.3 | 0.286 |
| SM (%) | 24.5 ± 4.9 | 34.8 ± 5.6 | <0.001 |
| S-score | −1.7 ± 1.4 | −1.2 ± 1.0 | 0.010 |
| hSMI | 4.0 ± 1.1 | 5.9 ± 1.0 | <0.001 |
| Phase angle (o) | 0.68 ± 0.69 | 0.60 ± 0.74 | 0.400 |
| Bone mass (kg) | 2.5 ± 0.4 | 3.8 ± 0.5 | <0.001 |
| T-score | −1.6 ± 0.8 | −0.9 ± 0.6 | <0.001 |
| ECW (%) | 55.7 ± 5.0 | 48.7 ± 3.1 | <0.001 |
| ECW/TBW | 0.52 ± 0.07 | 0.47 ± 0.04 | <0.001 |
| Parameter | Women | Men | ||||
|---|---|---|---|---|---|---|
| OSA (n = 209) | No OSA (n = 87) | p (t-Test) | OSA (n = 33) | No OSA (n = 36) | p (t-Test) | |
| Age (years) | 84.3 ± 5.4 | 81.1 ± 5.5 | <0.001 | 84.4 ± 7.9 | 81.9 ± 6.5 | 0.146 |
| Time in NH (mos.) | 48.1 ± 37.7 | 48.5 ± 39.0 | 0.697 | 44.7 ± 44.3 | 39.6 ± 42.8 | 0.155 |
| BMI (kg/m2) | 27.0 ± 3.1 | 33.8 ± 5.7 | <0.001 | 25.9 ± 2.9 | 29.1 ± 3.9 | <0.001 |
| FM (%) | 41.8 ± 4.3 | 45.8 ± 6.7 | <0.001 | 37.9 ± 6.5 | 37.6 ± 4.9 | 0.918 |
| AAT (cm2) | 438.7 ± 98.1 | 613.5 ± 181.2 | <0.001 | 481.5 ± 107.1 | 573.5 ± 168.3 | 0.009 |
| IMAT (%) | 2.8 ± 0.4 | 3.0 ± 0.4 | <0.001 | 2.8 ± 0.3 | 2.7 ± 0.2 | 0.899 |
| SM (%) | 22.5 ± 3.5 | 29.4 ± 4.4 | <0.001 | 32.4 ± 2.3 | 37.0 ± 6.1 | <0.001 |
| S-score | −2.3 ± 0.8 | −0.1 ± 1.3 | <0.001 | −1.9 ± 0.4 | −0.6 ± 1.0 | <0.001 |
| hSMI | 3.5 ± 0.7 | 5.3 ± 1.1 | <0.001 | 5.3 ± 0.4 | 6.6 ± 1.0 | <0.001 |
| Phase angle (o) | 0.56 ± 0.72 | 1.01 ± 0.83 | <0.001 | 0.39 ± 0.61 | 0.79 ± 0.80 | <0.027 |
| Bone mass (kg) | 2.3 ± 0.3 | 3.0 ± 0.4 | <0.001 | 3.4 ± 0.3 | 4.2 ± 0.4 | <0.001 |
| T-score | −2.0 ± 0.5 | −0.8 ± 0.7 | <0.001 | −1.3 ± 0.3 | −0.5 ± 0.5 | <0.001 |
| ECW (%) | 57.5 ± 3.9 | 51.4 ± 4.9 | <0.001 | 50.0 ± 3.3 | 47.7 ± 2.5 | 0.001 |
| ECW/TBW | 0.54 ± 0.08 | 0.49 ± 0.06 | <0.001 | 0.48 ± 0.05 | 0.47 ± 0.03 | 0.129 |
| Questions | Answers | Women (%) | Men (%) |
|---|---|---|---|
| Decrease in food intake |
| 6.1 26.0 67.9 | 1.9 23.9 74.2 |
| Loss of body weight |
| 12.1 12.1 63.7 12.1 | 12.6 12.6 65.1 9.7 |
| Number of meals per day |
| 0.4 9.2 90.4 | 0 6.3 93.7 |
| Protein intake |
| 80.4 67.0 67.4 | 79.6 65.6 68.7 |
| More than 2 servings of fruit/vegetables/day |
| 65.9 34.1 | 57.8 42.2 |
| Fluid intake |
| 8.9 51.7 39.4 | 6.2 50.0 43.8 |
| Independence in feeding |
| 0.00 4.6 95.4 | 0 14.1 * 85.9 |
| Self-assessment of nutritional status |
| 4.2 14.9 80.9 | 6.1 9.1 84.8 |
| Variables | β | Standard Error | Wald Stat. | Lower CL 95.00% | Upper CL 95.00% | p |
|---|---|---|---|---|---|---|
| Intercept | 15.27 | 3.72 | 16.79 | 7.96 | 22.57 | <0.001 |
| Age | −0.01 | 0.03 | 0.03 | −0.07 | 0.06 | 0.855 |
| Sex (level of effect: female) | −2.19 | 0.4 | 29.42 | −2.98 | −1.40 | <0.001 |
| IMAT% | 1.06 | 0.53 | 3.97 | −0.02 | 2.1 | 0.046 |
| Phase angle | −0.12 | 0.29 | 0.15 | −0.69 | 0.46 | 0.696 |
| Bone mass | −2.05 | 0.95 | 4.71 | −3.91 | −0.19 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cvijetić, S.; Keser, I.; Boschiero, D.; Ilich, J.Z. Osteosarcopenic Adiposity and Nutritional Status in Older Nursing Home Residents during the COVID-19 Pandemic. Nutrients 2023, 15, 227. https://doi.org/10.3390/nu15010227
Cvijetić S, Keser I, Boschiero D, Ilich JZ. Osteosarcopenic Adiposity and Nutritional Status in Older Nursing Home Residents during the COVID-19 Pandemic. Nutrients. 2023; 15(1):227. https://doi.org/10.3390/nu15010227
Chicago/Turabian StyleCvijetić, Selma, Irena Keser, Dario Boschiero, and Jasminka Z. Ilich. 2023. "Osteosarcopenic Adiposity and Nutritional Status in Older Nursing Home Residents during the COVID-19 Pandemic" Nutrients 15, no. 1: 227. https://doi.org/10.3390/nu15010227