
Nationwide Prevalence and Outcomes of Long-Term Nasogastric Tube Placement in Adults

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Outcome Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stroud, M.; Duncan, H.; Nightingale, J.; British Society of Gastroenterology. Guidelines for enteral feeding in adult hospital patients. Gut 2003, 52 (Suppl. 7), vii1–vii12. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, M.; Takada, K.; Shinde, M.; Matsumoto, N.; Tanaka, K.; Kiriya, Y.; Nishimoto, E.; Kuzuya, M. National survey of the prevalence of swallowing difficulty and tube feeding use as well as implementation of swallowing evaluation in long-term care settings in Japan. Geriatr. Gerontol. Int. 2014, 14, 577–581. [Google Scholar] [CrossRef]
- Lee, C.; Im, J.P.; Kim, J.W.; Kim, S.E.; Ryu, D.Y.; Cha, J.M.; Kim, E.Y.; Kim, E.R.; Chang, D.K.; Small Intestine Research Group of the Korean Association for the Study of Intestinal Disease (KASID). Risk factors for complications and mortality of percutaneous endoscopic gastrostomy: A multicenter, retrospective study. Surg. Endosc. 2013, 27, 3806–3815. [Google Scholar] [CrossRef]
- Lin, L.C.; Li, M.H.; Watson, R. A survey of the reasons patients do not chose percutaneous endoscopic gastrostomy/jejunostomy (PEG/PEJ) as a route for long-term feeding. J. Clin. Nurs. 2011, 20, 802–810. [Google Scholar] [CrossRef]
- Mamun, K.; Lim, J. Role of nasogastric tube in preventing aspiration pneumonia in patients with dysphagia. Singap. Med. J. 2005, 46, 627–631. [Google Scholar]
- Jaafar, M.H.; Mahadeva, S.; Tan, K.M.; Chin, A.V.; Kamaruzzaman, S.B.; Khor, H.M.; Saedon, N.I.; Tan, M.P. Long-Term Nasogastric versus Percutaneous Endoscopic Gastrostomy Tube Feeding in Older Asians With Dysphagia: A Pragmatic Study. Nutr. Clin. Pract. 2019, 34, 280–289. [Google Scholar] [CrossRef]
- van der Maarel-Wierink, C.D.; Vanobbergen, J.N.; Bronkhorst, E.M.; Schols, J.M.; de Baat, C. Meta-analysis of dysphagia and aspiration pneumonia in frail elders. J. Dent. Res. 2011, 90, 1398–1404. [Google Scholar] [CrossRef]
- Bonilha, H.S.; Simpson, A.N.; Ellis, C.; Mauldin, P.; Martin-Harris, B.; Simpson, K. The one-year attributable cost of post-stroke dysphagia. Dysphagia 2014, 29, 545–552. [Google Scholar] [CrossRef]
- Ho, C.H.; Lin, W.C.; Hsu, Y.F.; Lee, I.H.; Hung, Y.C. One-Year Risk of Pneumonia and Mortality in Patients with Poststroke Dysphagia: A Nationwide Population-Based Study. J. Stroke Cerebrovasc. Dis. 2018, 27, 1311–1317. [Google Scholar] [CrossRef]
- Lin, L.C.; Wu, S.C.; Chen, H.S.; Wang, T.G.; Chen, M.Y. Prevalence of impaired swallowing in institutionalized older people in taiwan. J. Am. Geriatr. Soc. 2002, 50, 1118–1123. [Google Scholar] [CrossRef]
- Mitchell, S.L.; Teno, J.M.; Roy, J.; Kabumoto, G.; Mor, V. Clinical and organizational factors associated with feeding tube use among nursing home residents with advanced cognitive impairment. JAMA 2003, 290, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Wirth, R.; Bauer, J.M.; Willschrei, H.P.; Volkert, D.; Sieber, C.C. Prevalence of percutaneous endoscopic gastrostomy in nursing home residents--a nationwide survey in Germany. Gerontology 2010, 56, 371–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentur, N.; Sternberg, S.; Shuldiner, J.; Dwolatzky, T. Feeding tubes for older people with advanced dementia living in the community in Israel. Am. J. Alzheimers Dis. Other Dement. 2015, 30, 165–172. [Google Scholar] [CrossRef]
- Adkins, C.; Takakura, W.; Spiegel, B.M.R.; Lu, M.; Vera-Llonch, M.; Williams, J.; Almario, C.V. Prevalence and Characteristics of Dysphagia Based on a Population-Based Survey. Clin. Gastroenterol. Hepatol. 2020, 18, 1970–1979. [Google Scholar] [CrossRef]
- Roden, D.F.; Altman, K.W. Causes of dysphagia among different age groups: A systematic review of the literature. Otolaryngol. Clin. N. Am. 2013, 46, 965–987. [Google Scholar] [CrossRef]
- Bhattacharyya, N. The prevalence of dysphagia among adults in the United States. Otolaryngol. Head Neck Surg. 2014, 151, 765–769. [Google Scholar] [CrossRef]
- Takizawa, C.; Gemmell, E.; Kenworthy, J.; Speyer, R. A systematic review of the prevalence of Oropharyngeal dysphagia in stroke, Parkinson’s disease, Alzheimer’s disease, head injury, and pneumonia. Dysphagia 2016, 31, 434–441. [Google Scholar] [CrossRef]
- Flowers, H.L.; AlHarbi, M.A.; Mikulis, D.; Silver, F.L.; Rochon, E.; Streiner, D.; Martino, R. MRI-based neuroanatomical predictors of dysphagia, dysarthria, and aphasia in patients with first acute ischemic stroke. Cerebrovasc. Dis. Extra 2017, 7, 21–34. [Google Scholar] [CrossRef]
- Yeh, L.; Lo, L.H.; Fetzer, S.; Chen, C.H. Limited PEG tube use: The experience of long-term care directions. J. Clin. Nurs. 2010, 19, 2897–2906. [Google Scholar] [CrossRef]
- Geeganage, C.; Beavan, J.; Ellender, S.; Bath, P.M. Interventions for dysphagia and nutritional support in acute and subacute stroke. Cochrane Database Syst. Rev. 2012, 10, CD000323. [Google Scholar] [CrossRef]
- Gomes, C.A., Jr.; Andriolo, R.B.; Bennett, C.; Lustosa, S.A.; Matos, D.; Waisberg, D.R.; Waisberg, J. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst. Rev. 2015, 2015, CD008096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaafar, M.H.; Mahadeva, S.; Morgan, K.; Tan, M.P. Percutaneous endoscopic gastrostomy versus nasogastric feeding in older individuals with non-stroke dysphagia: A systematic review. J. Nutr. Health Aging 2015, 19, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.S.; Lewis, S.C.; Warlow, C.; FOOD Trial Collaboration. Effect of timing and method of enteral tube feeding for dysphagic stroke patients (FOOD): A multicentre randomised controlled trial. Lancet 2005, 365, 764–772. [Google Scholar] [PubMed]
- Joundi, R.A.; Saposnik, G.; Martino, R.; Fang, J.; Porter, J.; Kapral, M.K. Outcomes among patients with direct enteral vs nasogastric tube placement after acute stroke. Neurology 2018, 90, e544–e552. [Google Scholar] [CrossRef]
- Shinozaki, T.; Ebihara, M.; Iwase, S.; Yamaguchi, T.; Hirakawa, H.; Shimbashi, W.; Kamijo, T.; Okamoto, M.; Beppu, T.; Ohori, J.; et al. Quality of life and functional status of terminally ill head and neck cancer patients: A nation-wide, prospective observational study at tertiary cancer centers in Japan. Jpn. J. Clin. Oncol. 2017, 47, 47–53. [Google Scholar] [CrossRef]
- Takayama, K.; Hirayama, K.; Hirao, A.; Kondo, K.; Hayashi, H.; Kadota, K.; Asaba, H.; Ishizu, H.; Nakata, K.; Kurisu, K.; et al. Survival times with and without tube feeding in patients with dementia or psychiatric diseases in Japan. Psychogeriatrics 2017, 17, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Löser, C.; Aschl, G.; Hébuterne, X.; Mathus-Vliegen, E.M.; Muscaritoli, M.; Niv, Y.; Rollins, H.; Singer, P.; Skelly, R.H. ESPEN guidelines on artificial enteral nutrition--percutaneous endoscopic gastrostomy (PEG). Clin. Nutr. 2005, 24, 848–861. [Google Scholar] [PubMed]
- Dietrich, C.G.; Schoppmeyer, K. Percutaneous endoscopic gastrostomy—Too often? Too late? Who are the right patients for gastrostomy? World J. Gastroenterol. 2020, 26, 2464–2471. [Google Scholar] [CrossRef]
- National Statistics, R.O.C. (Taiwan). Available online: https://www.stat.gov.tw/mp.asp?mp=4 (accessed on 14 April 2022).
- U.S. Bureau of Labor Statistics. Available online: https://www.bls.gov/oes/current/oes291127.htm#nat (accessed on 14 April 2022).
- Di Pede, C.; Mantovani, M.E.; Del Felice, A.; Masiero, S. Dysphagia in the elderly: Focus on rehabilitation strategies. Aging Clin. Exp. Res. 2016, 28, 607–617. [Google Scholar] [CrossRef]
- Wirth, R.; Dziewas, R.; Beck, A.M.; Clavé, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.; Leischker, A.H.; Martino, R.; Pluschinski, P.; et al. Oropharyngeal dysphagia in older persons—From pathophysiology to adequate intervention: A review and summary of an international expert meeting. Clin. Interv. Aging 2016, 11, 189–208. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | NGT Patients | Main Cause | |||||
|---|---|---|---|---|---|---|---|
| Stroke | Head Injury | PD and Parkinsonism | Dementia | Cancer | Something Else | ||
| Number | 2754 | 1202 (44%) | 396 (14%) | 141 (5%) | 324 (12%) | 444 (16%) | 310 (11%) |
| Gender | |||||||
| Female | 1009 (37%) | 463 (39%) | 126 (32%) | 49 (35%) | 131 (40%) | 139 (31%) | 127 (41%) |
| Male | 1745 (63%) | 739 (62%) | 270 (68%) | 92 (65%) | 193 (60%) | 305 (69%) | 183 (59%) |
| Age | |||||||
| 20–30 | 45 (2%) | 6 (0.5%) | 28 (7.1%) | 0 (0%) | 0 (0%) | 6 (1.4%) | 7 (2.3%) |
| 31–40 | 46 (2%) | 11 (0.9%) | 16 (4.0%) | 1 (0.7%) | 0 (0%) | 12 (2.7%) | 8 (2.6%) |
| 41–50 | 127 (5%) | 48 (4.0%) | 20 (5.1%) | 2 (1.4%) | 1 (0.3%) | 44 (9.9%) | 13 (4.2%) |
| 51–65 | 380 (14%) | 198 (17%) | 58 (15%) | 7 (5.0%) | 3 (0.9%) | 77 (17%) | 41 (13%) |
| >65 | 2156 (78%) | 939 (78%) | 274 (69%) | 131 (93%) | 320 (99%) | 305 (69%) | 241 (78%) |
| Mean, (SD) | 73.4 (14.2) | 73.5 (12.5) | 68.6 (18.4) | 77.8 (9.35) | 81.8 (7.41) | 70.3 (15.5) | 73.2(15.2) |
| Area | |||||||
| Northern | 1042 (38%) | 478 (40%) | 124 (31%) | 46 (33%) | 133 (41%) | 174 (39%) | 104 (34%) |
| Central | 832 (30%) | 384 (32%) | 146 (37%) | 33 (23%) | 76 (24%) | 123 (28%) | 91 (29%) |
| Southern | 367 (13%) | 146 (12%) | 43 (11%) | 33 (23%) | 50 (15%) | 61 (14%) | 48 (15%) |
| Eastern and island | 513 (19%) | 194 (16%) | 83 (21%) | 29 (21%) | 65 (20%) | 86 (19%) | 67 (22%) |
| Comorbidities | |||||||
| Hypertension | 2135 (78%) | 1023 (85%) | 266 (67%) | 122 (87%) | 278 (86%) | 299 (67%) | 198 (64%) |
| Diabetes | 1113 (40%) | 532 (44%) | 141 (36%) | 62 (44%) | 131 (40%) | 165 (37%) | 107 (35%) |
| Hyperlipidemia | 983 (36%) | 474 (39%) | 136 (34%) | 67 (47%) | 123 (38%) | 136 (31%) | 73 (24%) |
| CAD | 325 (12%) | 151 (13%) | 40 (10%) | 20 (14%) | 46 (14%) | 43 (9.7%) | 32 (10%) |
| CHF | 448 (16%) | 178 (15%) | 39 (9.8%) | 33 (23%) | 78 (24%) | 69 (16%) | 64 (21%) |
| CKD | 333 (12%) | 142 (12%) | 33 (8.3%) | 22 (17%) | 43 (13%) | 58 (13%) | 39 (13%) |
| COPD | 1387 (50%) | 549 (46%) | 175 (44%) | 91 (65%) | 218 (67%) | 225 (51%) | 155 (50%) |
| AF | 244 (9.0%) | 121 (10%) | 15 (3.8%) | 16 (11%) | 43 (13%) | 26 (5.9%) | 25 (8.1%) |
| Hospital level | |||||||
| Medical center | 952 (35%) | 455 (38%) | 136 (34%) | 37 (26%) | 74 (23%) | 184 (41%) | 93 (30%) |
| District hospital | 1209 (44%) | 513 (43%) | 202 (51%) | 60 (43%) | 133 (41%) | 161 (36%) | 142 (46%) |
| Local hospital | 593 (22%) | 234 (19%) | 58 (15%) | 44 (31%) | 117 (36%) | 99 (22%) | 75 (24%) |
| Non-NGT | NGT | Rehabilitation | PEG | ||||||
|---|---|---|---|---|---|---|---|---|---|
| N = 11,016 | N = 2754 | N = 364 (13%) | N = 7 (0.62%) | ||||||
| n | % | n | % | p-Value | n | % | n | % | |
| Gender | 0.74 | ||||||||
| Female | 3996 | 36% | 1009 | 37% | 118 | (32%) | 5 | (29%) | |
| Male | 7020 | 64% | 1745 | 63% | 246 | (68%) | 12 | (71%) | |
| Age, year | 1.00 | ||||||||
| 20–30 | 180 | 2% | 45 | 2% | 17 | (5%) | 0 | (0%) | |
| 31–40 | 185 | 2% | 46 | 2% | 14 | (4%) | 1 | (6%) | |
| 41–50 | 494 | 4% | 127 | 5% | 33 | (9%) | 1 | (6%) | |
| 51–65 | 1520 | 14% | 380 | 14% | 97 | (27%) | 4 | (24%) | |
| >65 | 8637 | 78% | 2156 | 78% | 203 | (56%) | 11 | (65%) | |
| Area | 0.61 | ||||||||
| Northern | 4239 | 38% | 1042 | 38% | 155 | (43%) | 9 | (53%) | |
| Central | 3314 | 30% | 832 | 30% | 162 | (45%) | 5 | (29%) | |
| Southern | 1454 | 13% | 367 | 13% | 27 | (7%) | 3 | (18%) | |
| Eastern and island | 2009 | 18% | 513 | 19% | 20 | (5%) | 0 | (0%) | |
| Comorbidities | |||||||||
| Hypertension | 8637 | 78% | 2135 | 78% | 0.33 | 265 | (73%) | 11 | (65%) |
| Diabetes | 4552 | 41% | 1113 | 40% | 0.98 | 138 | (38%) | 7 | (41%) |
| Hyperlipidemia | 3855 | 35% | 983 | 36% | 0.51 | 152 | (42%) | 4 | (24%) |
| CAD | 1100 | 10% | 325 | 12% | 0.01 | 36 | (10%) | 0 | (0%) |
| CKD | 1732 | 16% | 448 | 16% | 0.50 | 38 | (10%) | 0 | (0%) |
| CHF | 1180 | 11% | 333 | 12% | 0.04 | 17 | (5%) | 0 | (0%) |
| COPD | 5704 | 52% | 1387 | 50% | 0.19 | 123 | (34%) | 5 | (29%) |
| AF | 782 | 7% | 244 | 9% | 0.002 | 30 | (8%) | 3 | (18%) |
| Main cause | |||||||||
| Stroke | 1202 | 44% | 237 | (65%) | 6 | (35%) | |||
| Head injury | 396 | 14% | 86 | (24%) | 1 | (6%) | |||
| PD and parkinsonism | 141 | 5% | 9 | (2%) | 1 | (6%) | |||
| Dementia | 324 | 12% | 6 | (2%) | 3 | (18%) | |||
| Cancer | 444 | 16% | 20 | (5%) | 6 | (35%) | |||
| Something else | 310 | 11% | 12 | (3%) | 0 | (0%) | |||
| Hospital level | |||||||||
| Medical center | 952 | 35% | 199 | (55%) | 9 | (53%) | |||
| District hospital | 1209 | 44% | 149 | (41%) | 5 | (29%) | |||
| Local hospital | 593 | 22% | 16 | (4%) | 3 | (18%) | |||
| Re-intubation of NGT | 291 | (80%) | |||||||
| Non-NGT | NGT | HR | ||||||
|---|---|---|---|---|---|---|---|---|
| n | PY | IR | n | PY | IR | cHR (95% CI) | aHR † (95% CI) | |
| Morbidities | ||||||||
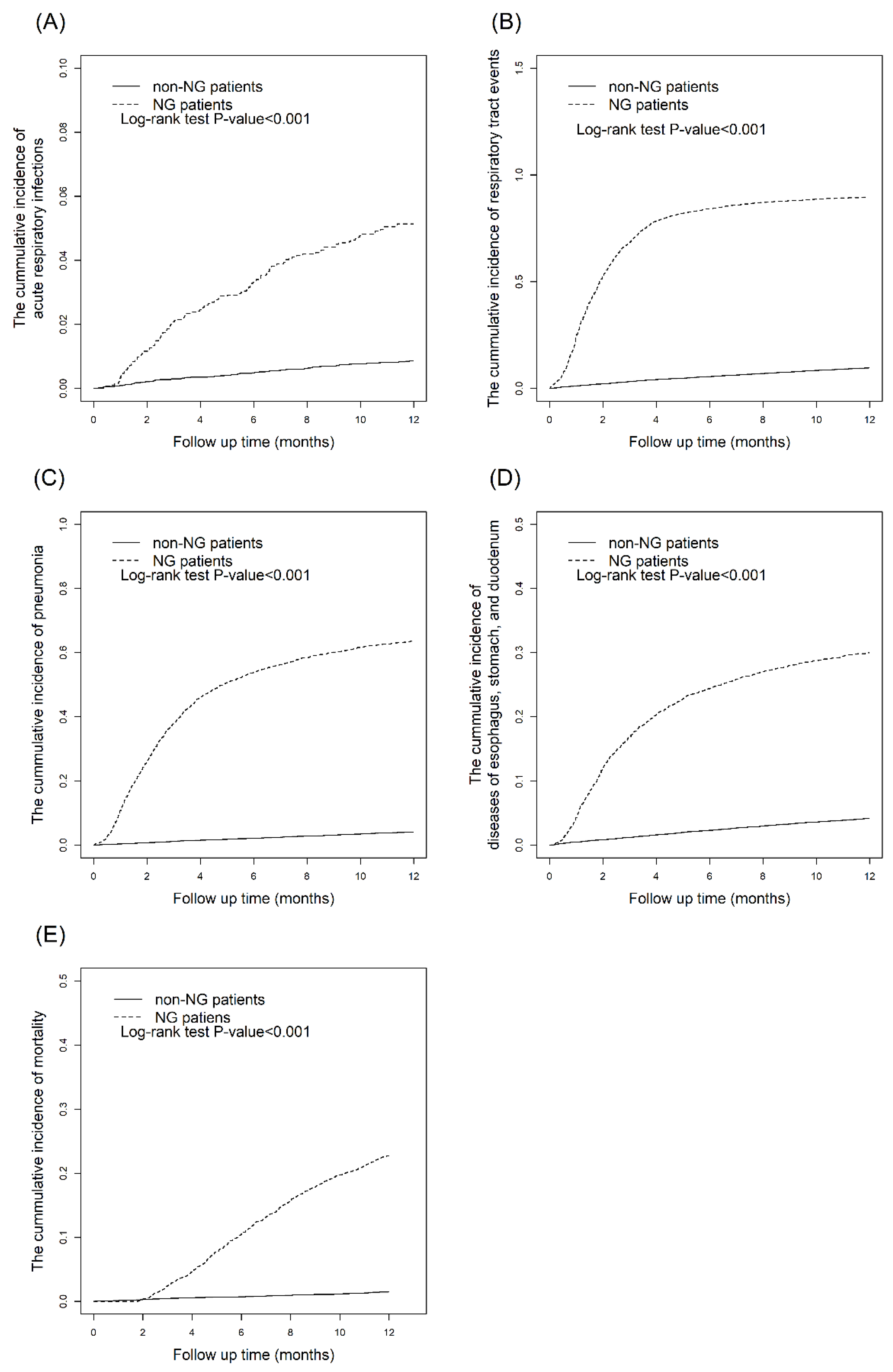
| Acute and chronic respiratory infections | 1061 | 10,375 | 1.02 | 2444 | 734 | 33.3 | 25.4 (23.5,27.4) *** | 28.1 (26.0,30.3) *** |
| Acute respiratory infections | 94 | 10,860 | 0.09 | 131 | 2389 | 0.55 | 6.20 (4.72,8.03) *** | 6.16 (4.73,8.04) *** |
| Pneumonia | 444 | 10,706 | 0.41 | 1701 | 1392 | 12.2 | 25.6 (23.0,28.5) *** | 26.8 (24.1,29.8) *** |
| Diseases of esophagus, stomach, and duodenum | 456 | 10,680 | 0.43 | 788 | 1962 | 4.02 | 8.70 (7.78,9.81) *** | 8.84 (7.87,9.93) *** |
| Mortality | 162 | 10,912 | 0.15 | 625 | 2464 | 2.54 | 17.3 (14.6,20.6) *** | 17.5 (14.7,20.8) *** |
| Time Span of NGT | N | Pneumonia | COR (95% CI) | AOR † (95% CI) |
|---|---|---|---|---|
| 3 months–6 months | 2573 | 1572 | 1.00 (reference) | 1.00 (reference) |
| >6 months | 181 | 129 | 1.57 (1.13,2.20) ** | 1.58 (1.13,2.20) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.Y.; Lai, J.-N.; Kung, W.-M.; Hung, C.-H.; Yip, H.-T.; Chang, Y.-C.; Wei, C.-Y. Nationwide Prevalence and Outcomes of Long-Term Nasogastric Tube Placement in Adults. Nutrients 2022, 14, 1748. https://doi.org/10.3390/nu14091748
Hsu CY, Lai J-N, Kung W-M, Hung C-H, Yip H-T, Chang Y-C, Wei C-Y. Nationwide Prevalence and Outcomes of Long-Term Nasogastric Tube Placement in Adults. Nutrients. 2022; 14(9):1748. https://doi.org/10.3390/nu14091748
Chicago/Turabian StyleHsu, Chung Y., Jung-Nien Lai, Woon-Man Kung, Chao-Hsien Hung, Hei-Tung Yip, Yu-Chen Chang, and Cheng-Yu Wei. 2022. "Nationwide Prevalence and Outcomes of Long-Term Nasogastric Tube Placement in Adults" Nutrients 14, no. 9: 1748. https://doi.org/10.3390/nu14091748