
Nutritional Status and Selected Adipokines in Children with Irritable Bowel Syndrome

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients with IBS
2.2. Control Group
2.3. Anthropometric Measurements
2.4. Laboratory Measurements
2.5. Statistical Analysis
3. Results
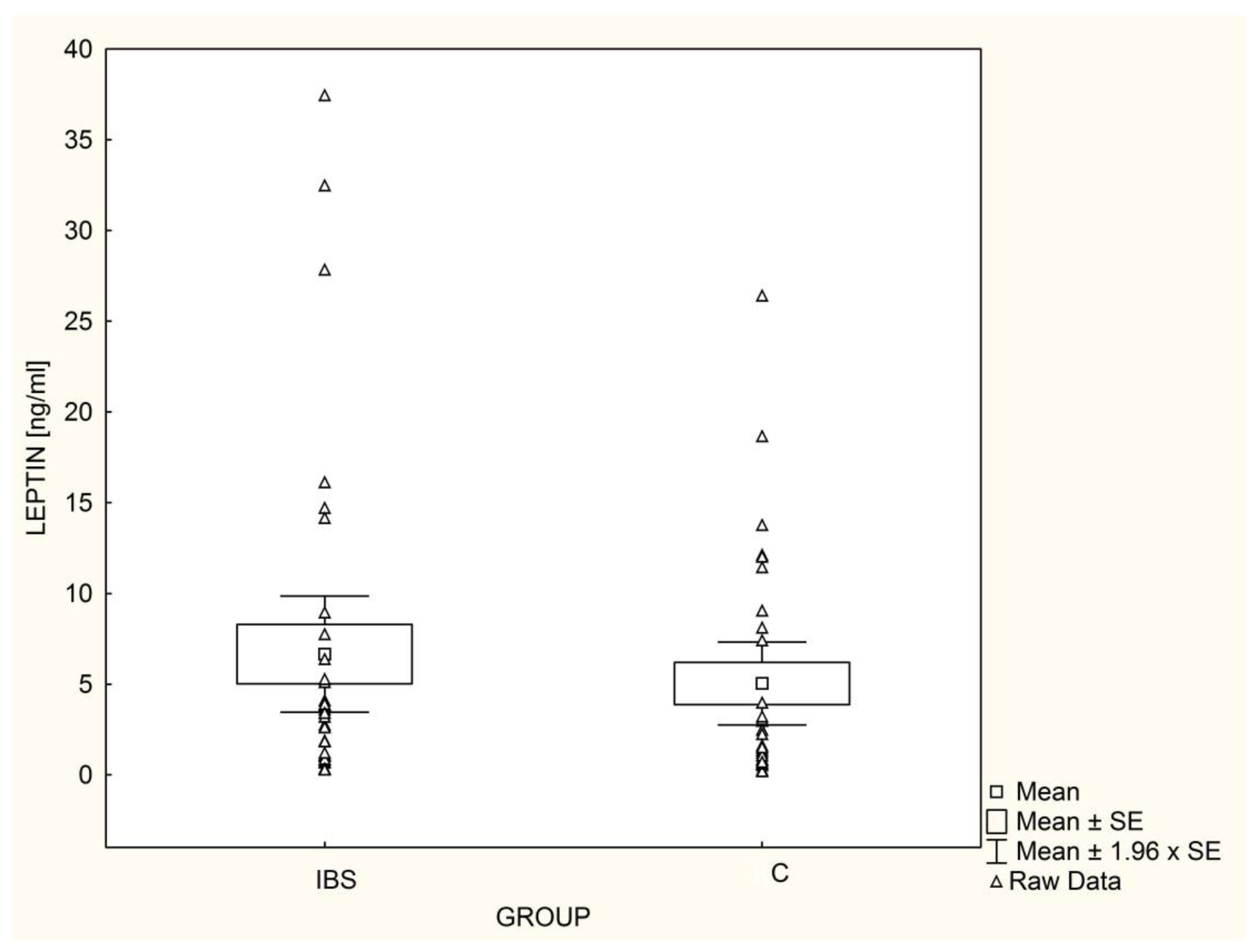
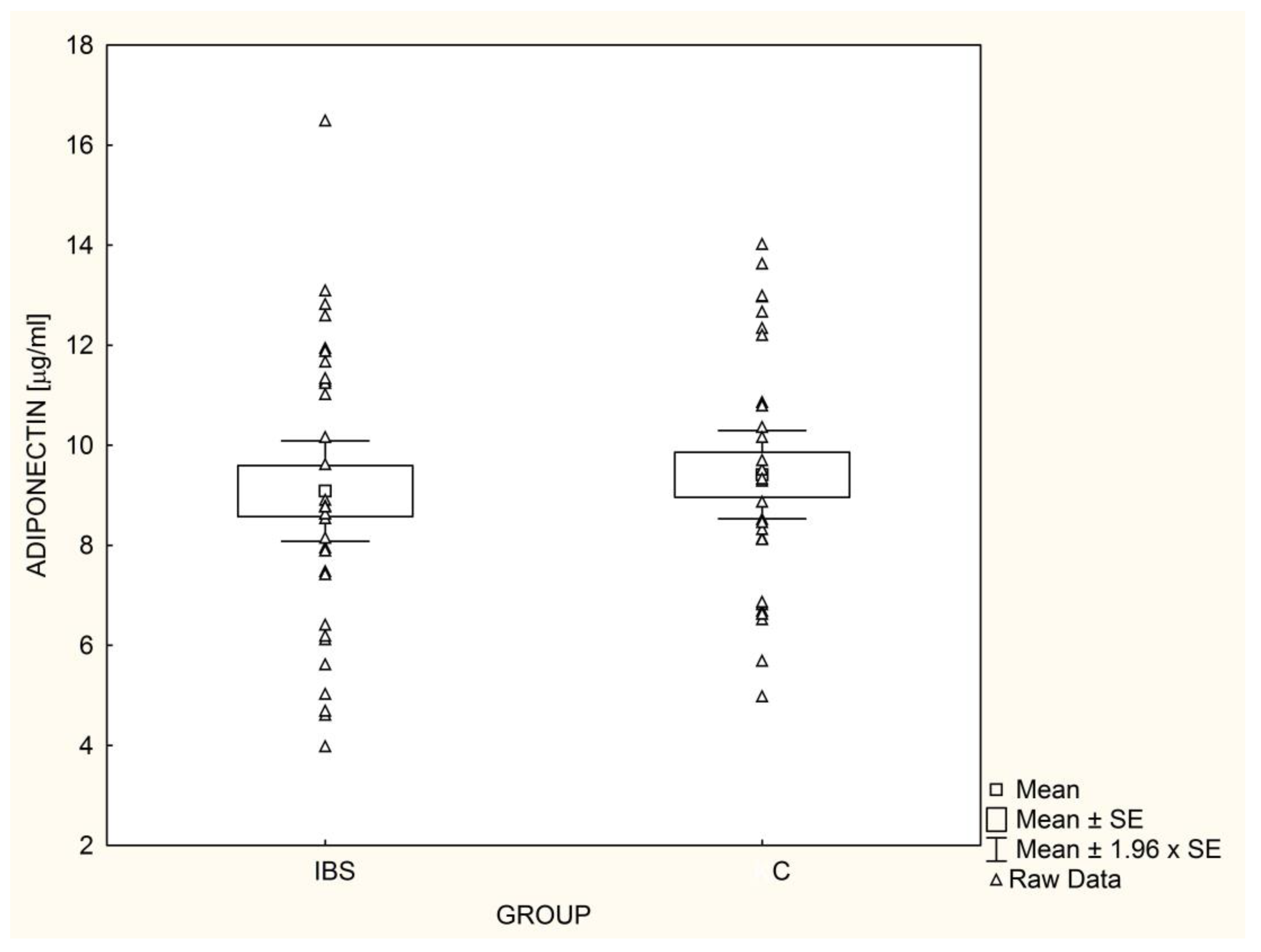
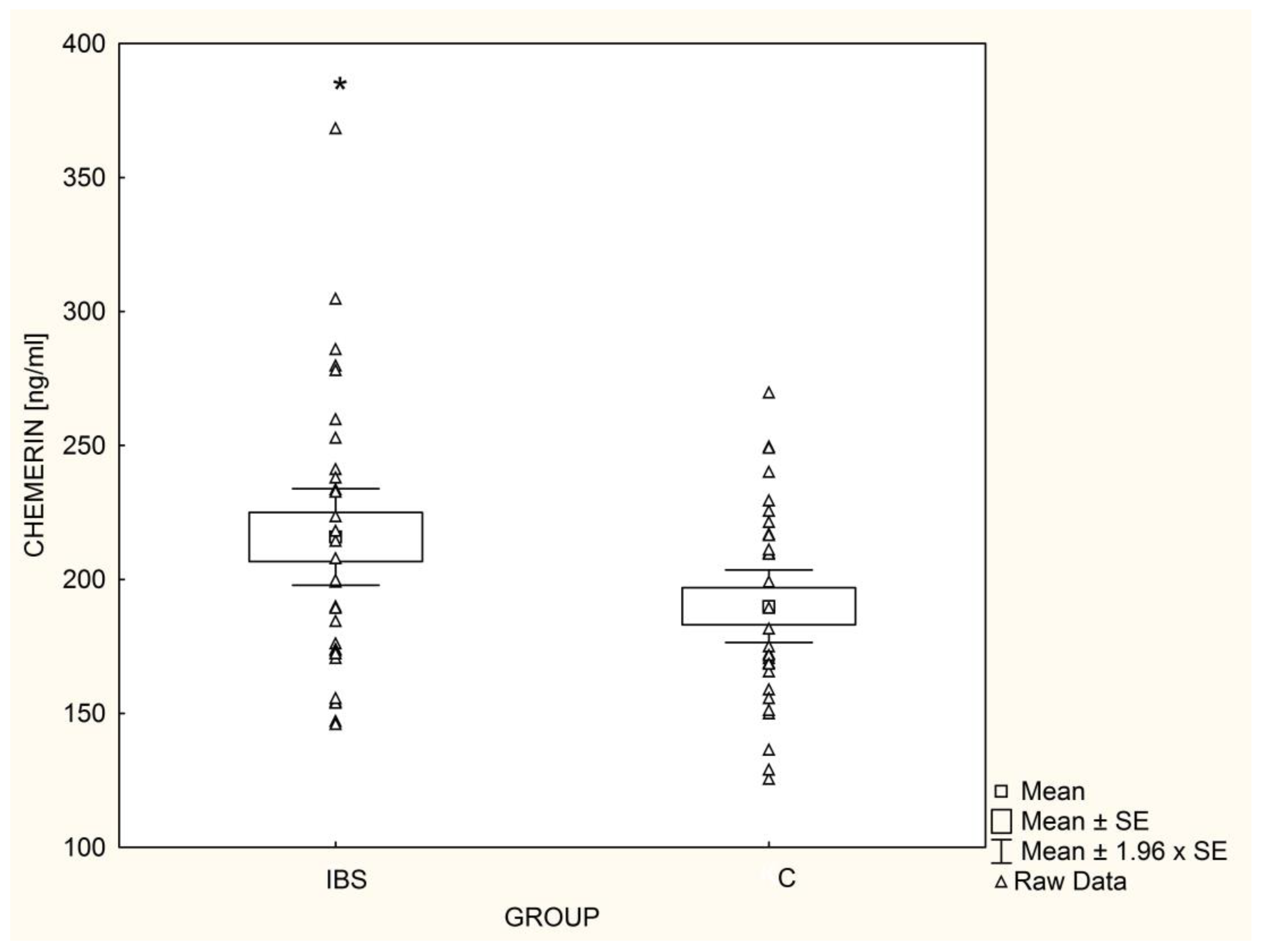
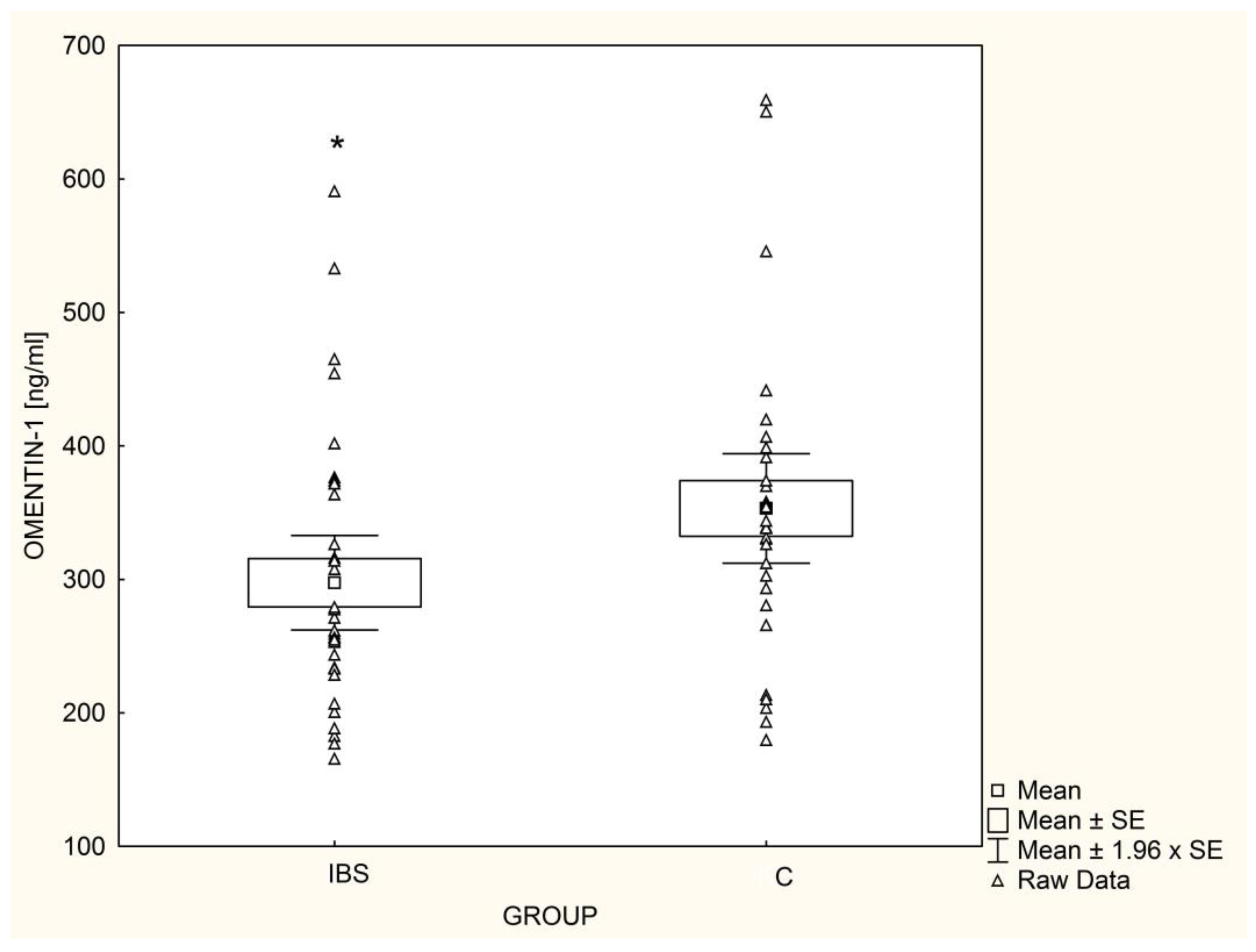
3.1. Adipokine Concentrations
3.2. Adipokine Concentration, Age, and Anthropometric Parameters
3.3. Adipokine Concentration and Laboratory Results
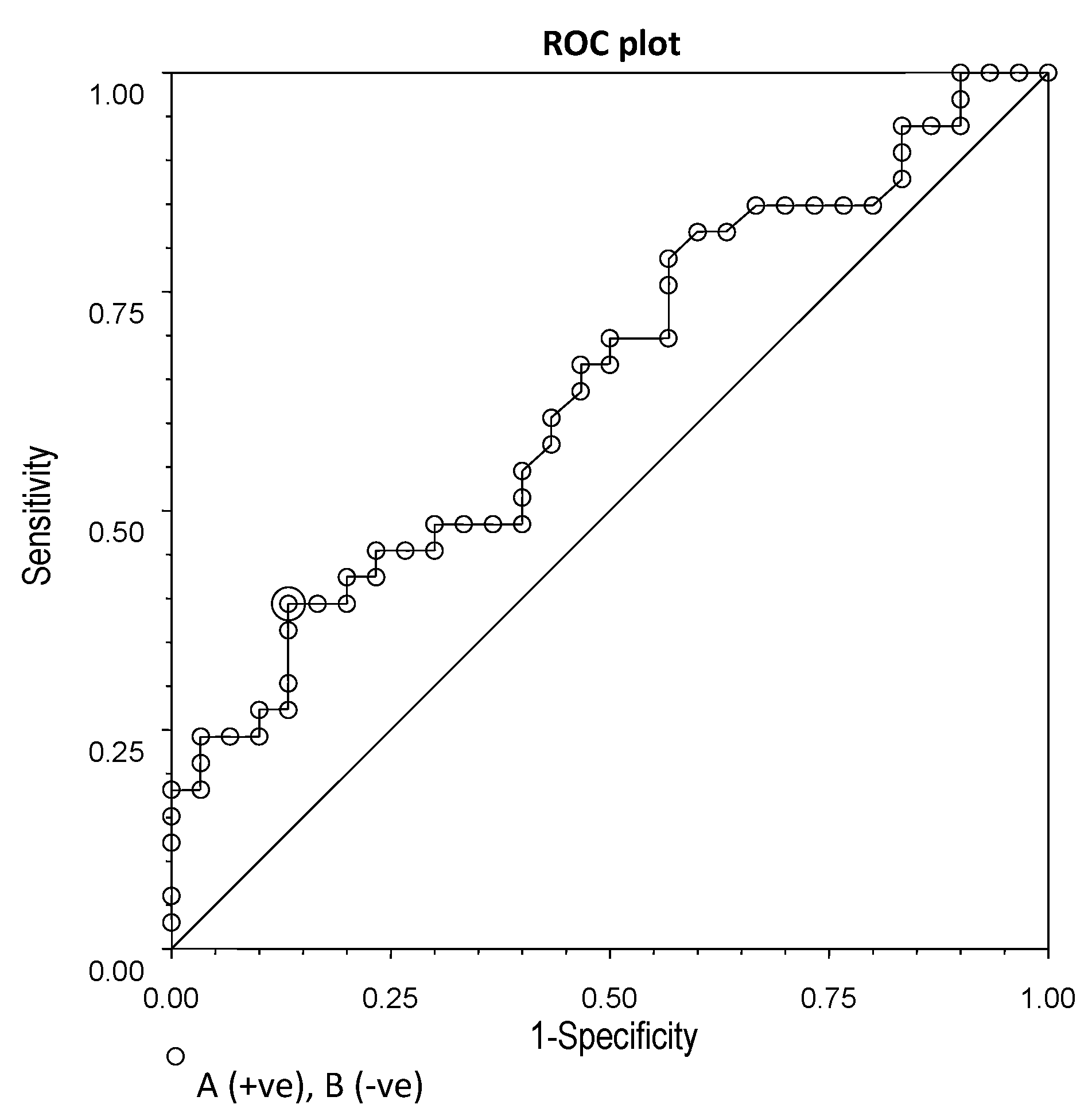
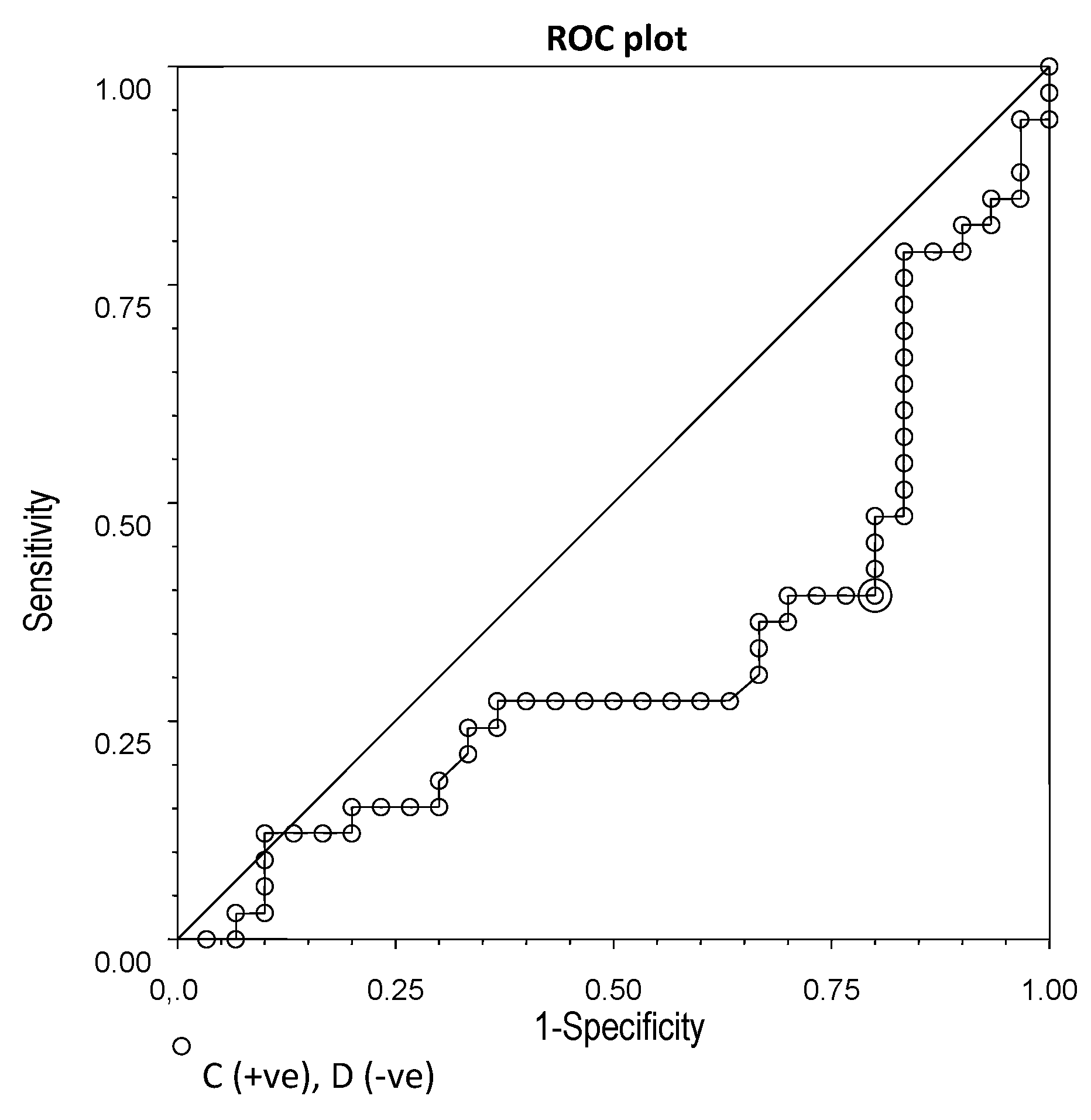
3.4. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Soares, R.L. Irritable bowel syndrome: A clinical review. World J. Gastroenterol. 2014, 20, 12144–12160. [Google Scholar] [CrossRef]
- Lee, Y.J.; Park, K.S. Irritable bowel syndrome: Emerging paradigm in pathophysiology. World J. Gastroenterol. 2014, 20, 2456–2469. [Google Scholar] [CrossRef]
- Saha, L. Irritable bowel syndrome: Pathogenesis, diagnosis, treatment, and evidence-based medicine. World J. Gastroenterol. 2014, 20, 6759–6773. [Google Scholar] [CrossRef]
- Oświęcimska, J.; Szymlak, A.; Roczniak, W.; Girczys-Połedniok, K.; Kwiecień, J. New insights into the pathogenesis and treatment of irritable bowel syndrome. Adv. Med. Sci. 2017, 62, 17–30. [Google Scholar] [CrossRef]
- Chey, W.D. The role of food in the functional gastrointestinal disorders: Introduction to a manuscript series. Am. J. Gastroenterol. 2013, 108, 694–697. [Google Scholar] [CrossRef] [PubMed]
- Pawłowska, K.; Umławska, W.; Iwańczak, B. A Link between Nutritional and Growth States in Pediatric Patients with Functional Gastrointestinal Disorders. J. Pediatr. 2018, 199, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Galai, T.; Moran-Lev, H.; Cohen, S.; Ben-Tov, A.; Levy, D.; Weintraub, Y.; Yerushalmy-Feler, A. Higher prevalence of obesity among children with functional abdominal pain disorders. BMC Pediatr. 2020, 20, 193. [Google Scholar] [CrossRef]
- Phatak, U.P.; Pashankar, D.S. Prevalence of functional gastrointestinal disorders in obese and overweight children. Int. J. Obes. 2014, 38, 1324–1327. [Google Scholar] [CrossRef] [PubMed]
- Bonilla, S.; Wang, D.; Saps, M. Obesity predicts persistence of pain in children with functional gastrointestinal disorders. Int. J. Obes. 2010, 35, 517–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fifi, A.C.; Velasco-Benitez, C.; Saps, M. Functional Abdominal Pain and Nutritional Status of Children. A School-Based Study. Nutrients 2020, 12, 2559. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, G.; Cremon, C.; Staiano, A.; Stanghellini, V.; Borrelli, O.; Strisciuglio, C.; Romano, C.; Mallardo, S.; Scarpato, E.; Marasco, G.; et al. Role of inflammation in pediatric irritable bowel syndrome. Neurogastroenterol. Motil. 2022; online ahead of print. [Google Scholar]
- Olszanecka-Glinianowicz, M.; Handzlik-Orlik, G.; Orlik, B.; Chudek, J. Adipokines in the pathogenesis of idiopathic inflammatory bowel disease. Endokrynol. Pol. 2013, 64, 226–231. [Google Scholar] [PubMed]
- Waluga, M.; Hartleb, M.; Boryczka, G.; Kukla, M.; Żwirska-Korczala, K. Serum adipokines in inflammatory bowel disease. World J. Gastroenterol. 2014, 20, 6912–6917. [Google Scholar] [CrossRef] [PubMed]
- Piche, T.; Huet, P.M.; Gelsi, E.; Barjoan, E.M.; Cherick, F.; Caroli-Bosc, F.X.; Hébuterne, X.; Tran, A. Fatigue in irritable bowel syndrome: Characterization and putative role of leptin. Eur. J. Gastroenterol. Hepatol. 2007, 19, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Semnani, S.; Roshandel, G.; Keshtkar, A.; Najafi, L.; Amiriani, T.; Farajollahi, M.; Moradi, A.; Joshaghani, H. Serum leptin levels and irritable bowel syndrome: A new hypothesis. J. Clin. Gastroenterol. 2009, 43, 826–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, F.; Chimienti, G.; Clemente, C.; D’Attoma, B.; Linsalata, M.; Orlando, A.; De Carne, M.; Cariola, F.; Semeraro, F.P.; Pepe, G.; et al. Adipokine profile in celiac patients: Differences in comparison with patients suffering from diarrhea-predominant IBS and healthy subjects. Scand. J. Gastroenterol. 2013, 48, 1377–1385. [Google Scholar] [CrossRef]
- Russo, F.; Chimienti, G.; Riezzo, G.; Linsalata, M.; D’Attoma, B.; Clemente, C.; Orlando, A. Adipose Tissue-Derived Biomarkers of Intestinal Barrier Functions for the Characterization of Diarrhoea-Predominant IBS. Dis. Markers 2018, 2018, 1827937. [Google Scholar] [CrossRef] [Green Version]
- Weaver, K.R.; Boulineaux, C.M.; Robinson, J.M.; Butler, K.; Heitkemper, M.M.; Henderson, W.A. Sex Hormones, BDNF, Leptin, and TGF-β1 in Females With IBS: A Pilot Investigation. Biol. Res. Nurs. 2021, 23, 231–237. [Google Scholar] [CrossRef]
- Saidi, K.; Nilholm, C.; Roth, B.; Ohlsson, B. A carbohydrate-restricted diet for patients with irritable bowel syndrome lowers serum C-peptide, insulin, and leptin without any correlation with symptom reduction. Nutr. Res. 2021, 86, 23–36. [Google Scholar] [CrossRef]
- Baram, M.A.; Abbasnezhad, A.; Ghanadi, K.; Anbari, K.; Choghakhori, R.; Ahmadvand, H. Serum Levels of Chemerin, Apelin, and Adiponectin in Relation to Clinical Symptoms, Quality of Life, and Psychological Factors in Irritable Bowel Syndrome. J. Clin. Gastroenterol. 2020, 54, e40–e49. [Google Scholar] [CrossRef]
- Lee, C.G.; Lee, J.K.; Kang, Y.S.; Shin, S.; Kim, J.H.; Lim, Y.J.; Koh, M.S.; Lee, J.H.; Kang, H.W. Visceral abdominal obesity is associated with an increased risk of irritable bowel syndrome. Am. J. Gastroenterol. 2015, 110, 310–319. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Chełchowska, M.; Rowicka, G.; Klemarczyk, W.; Strucińska, M.; Gajewska, J. Anti-Inflammatory and Pro-Inflammatory Adipokine Profiles in Children on Vegetarian and Omnivorous Diets. Nutrients 2018, 10, 1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoramipour, K.; Chamari, K.; Hekmatikar, A.A.; Ziyaiyan, A.; Taherkhani, S.; Elguindy, N.M.; Bragazzi, N.L. Adiponectin: Structure, Physiological Functions, Role in Diseases, and Effects of Nutrition. Nutrients 2021, 13, 1180. [Google Scholar] [CrossRef] [PubMed]
- Oświecimska, J.M.; Ziora, K.T.; Suwała, A.; Świętochowska, E.; Gorczyca, P.; Ziora-Jakutowicz, K.; Machura, E.; Szczepańska, M.; Ostrowska, Z.; Ziora, D.; et al. Chemerin serum levels in girls with anorexia nervosa. Neuroendocrinol. Lett. 2014, 35, 490–496. [Google Scholar] [PubMed]
- Oświęcimska, J.; Suwała, A.; Świętochowska, E.; Ostrowska, Z.; Gorczyca, P.; Ziora-Jakutowicz, K.; Machura, E.; Szczepańska, M.; Kukla, M.; Stojewska, M.; et al. Serum omentin levels in adolescent girls with anorexia nervosa and obesity. Physiol. Res. 2015, 64, 701–709. [Google Scholar] [CrossRef]
- de Candia, P.; Prattichizzo, F.; Garavelli, S.; Alviggi, C.; La Cava, A.; Matarese, G. The pleiotropic roles of leptin in metabolism, immunity, and cancer. J. Exp. Med. 2021, 218, e20191593. [Google Scholar] [CrossRef]
- Al-Suhaimi, E.A.; Shehzad, A. Leptin, resistin and visfatin: The missing link between endocrine metabolic disorders and immunity. Eur. J. Med. Res. 2013, 18, 12. [Google Scholar] [CrossRef] [Green Version]
- Park, H.K.; Ahima, R.S. Leptin signaling. F1000Prime Rep. 2014, 6, 73. [Google Scholar] [CrossRef] [Green Version]
- Oświęcimska, J. Ocena Zaburzeń Metabolicznych oraz Czynności Hormonalnej Tkanki Tłuszczowej u Młodzieży i Młodych Dorosłych z Niedoborem Hormonu Wzrostu; Śląski Uniwersytet Medyczny w Katowicach: Katowice, Poland, 2010. [Google Scholar]
- Paz-Filho, G.; Mastronardi, C.; Franco, C.B.; Wang, K.B.; Wong, M.L.; Licinio, J. Leptin: Molecular mechanisms, systemic pro-inflammatory effects, and clinical implications. Arq. Bras. Endocrinol. Metabol. 2012, 56, 597–607. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J. 20 years of leptin: Leptin at 20: An overview. J. Endocrinol. 2014, 223, T1–T8. [Google Scholar] [CrossRef] [Green Version]
- Kiernan, K.; MacIver, N.J. The Role of the Adipokine Leptin in Immune Cell Function in Health and Disease. Front. Immunol. 2021, 11, 622468. [Google Scholar] [CrossRef]
- Choi, H.M.; Doss, H.M.; Kim, K.S. Multifaceted Physiological Roles of Adiponectin in Inflammation and Diseases. Int. J. Mol. Sci. 2020, 21, 1219. [Google Scholar] [CrossRef] [Green Version]
- Robinson, K.; Prins, J.; Venkatesh, B. Clinical review: Adiponectin biology and its role in inflammation and critical illness. Crit. Care 2011, 15, 221. [Google Scholar] [CrossRef] [Green Version]
- Fantuzzi, G. Adiponectin in inflammatory and immune-mediated diseases. Cytokine 2013, 64, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Dąbrowska, M.; Szydlarska, D.; Bar-Andziak, E. Adiponektyna a insulinooporność i miażdżyca. Endokrynol. Otyłość. Zab Przem. Materii 2011, 7, 186–191. [Google Scholar]
- Buechler, C.; Wanninger, J.; Neumeier, M. Adiponectin, a key adipokine in obesity related liver diseases. World J. Gastroenterol. 2011, 17, 2801–2811. [Google Scholar] [PubMed] [Green Version]
- Graňák, K.; Vnučák, M.; Beliančinová, M.; Kleinová, P.; Pytliaková, M.; Miklušica, J.; Dedinská, I. Adiponectin/Leptin Ratio as an Index to Determine Metabolic Risk in Patients after Kidney Transplantation. Medicina 2022, 58, 1656. [Google Scholar] [CrossRef] [PubMed]
- Banas, M.; Zabieglo, K.; Kasetty, G.; Kapinska-Mrowiecka, M.; Borowczyk, J.; Drukala, J.; Murzyn, K.; Zabel, B.A.; Butcher, E.C.; Schroeder, J.M.; et al. Chemerin is an antimicrobial agent in human epidermis. PLoS ONE 2013, 8, e58709. [Google Scholar] [CrossRef]
- Ziora, K.; Suwała, A. Chemeryna—Struktura, funkcje biologiczne oraz związek z otyłościa i zespołem metabolicznym. Endokrynol. Pediatr. 2012, 11, 49–58. [Google Scholar]
- Chamberland, J.P.; Berman, R.L.; Aronis, K.N.; Mantzoros, C.S. Chemerin is expressed mainly in pancreas and liver, is regulated by energy deprivation, and lacks day/night variation in humans. Eur. J. Endocrinol. 2013, 169, 453–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zabel, B.A.; Kwitniewski, M.; Banas, M.; Zabieglo, K.; Murzyn, K.; Cichy, J. Chemerin regulation and role in host defense. Am. J. Clin. Exp. Immunol. 2014, 3, 1–19. [Google Scholar]
- Sell, H.; Laurencikiene, J.; Taube, A.; Eckardt, K.; Cramer, A.; Horrighs, A.; Arner, P.; Eckel, J. Chemerin is a novel adipocyte-derived factor inducing insulin resistance in primary human skeletal muscle cells. Diabetes 2009, 58, 2731–4270. [Google Scholar] [CrossRef] [Green Version]
- de Souza Batista, C.M.; Yang, R.Z.; Lee, M.J.; Glynn, N.M.; Yu, D.Z.; Pray, J.; Ndubuizu, K.; Patil, S.; Schwartz, A.; Kligman, M.; et al. Omentin plasma levels and gene expression are decreased in obesity. Diabetes 2007, 56, 1655–1661. [Google Scholar] [CrossRef] [Green Version]
- Wang, C. Obesity, inflammation, and lung injury (OILI): The good. Mediat. Inflamm. 2014, 2014, 978463. [Google Scholar] [CrossRef]
- Yang, R.Z.; Lee, M.J.; Hu, H.; Pray, J.; Wu, H.B.; Hansen, B.C.; Shuldiner, A.R.; Fried, S.K.; McLenithan, J.C.; Gong, D.W. Identification of omentin as a novel depot-specific adipokine in human adipose tissue: Possible role in modulating insulin action. Am. J. Physiol. Endocrinol. Metab. 2006, 290, E1253–E1261. [Google Scholar] [CrossRef]
- Moreno-Navarrete, J.M.; Ortega, F.; Castro, A.; Sabater, M.; Ricart, W.; Fernández-Real, J.M. Circulating omentin as a novel biomarker of endothelial dysfunction. Obesity 2011, 19, 1552–1559. [Google Scholar] [CrossRef] [PubMed]
- Shibata, R.; Ouchi, N.; Takahashi, R.; Terakura, Y.; Ohashi, K.; Ikeda, N.; Higuchi, A.; Terasaki, H.; Kihara, S.; Murohara, T. Omentin as a novel biomarker of metabolic risk factors. Diabetol. Metab. Syndr. 2012, 4, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auguet, T.; Quintero, Y.; Riesco, D.; Morancho, B.; Terra, X.; Crescenti, A.; Broch, M.; Aguilar, C.; Olona, M.; Porras, J.A.; et al. New adipokines vaspin and omentin. Circulating levels and gene expression in adipose tissue from morbidly obese women. BMC Med. Genet. 2011, 12, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palczewska, I.; Niedźwiedzka, Z. Wskaźnik rozwoju somatycznego u dzieci i młodzieży warszawskiej. Med. Wieku Rozw. 2001, 2 (Suppl. S1), 18–118. [Google Scholar]
- Kułaga, Z.; Litwin, M.; Zajączkowska, M.M.; Wasilewska, A.; Morawiec-Knysak, A.; Różdżyńska, A.; Gajda, A.; Gurzkowska, B.; Napieralska, E.; Barwicka, K.; et al. Porównanie wartości obwodów talii i bioder dzieci i młodzieży polskiej w wieku 7–18 lat z wartościami dla oceny ryzyka sercowo naczyniowego—Wyniki wstępne projektu badawczego OLAF (PL0080). Stand. Med. Pediatr. 2008, 5, 473–483. [Google Scholar]
- Ziora, K.; Oświęcimska, J.; Świętochowska, E.; Stojewska, M.; Ostrowska, Z.; Suwała, A. Ocena stężeń leptyny—Hormonu tkanki tłuszczowej w surowicy krwi u dziewcząt z jadłowstrętem psychicznym. Endokrynol. Pediatr. 2010, 9, 43–53. [Google Scholar]
- Murawska, S.; Kuczyńska, R.; Mierzwa, G.; Kulwas, A.; Rość, D.; Landowski, P.; Kamińska, B.; Czerwionka-Szaflarska, M. Ocena stężenia leptyny oraz rozpuszczalnej frakcji receptora dla niej u dzieci i młodzieży z chorobą Leśniowskiego-Crohna. Prz. Gastroenterol. 2009, 4, 262–272. [Google Scholar]
- Li, Y.; Shi, B.; Li, S. Association between serum chemerin concentrations and clinical indices in obesity or metabolic syndrome: A meta-analysis. PLoS ONE 2014, 9, e113915. [Google Scholar] [CrossRef] [PubMed]
- Landgraf, K.; Friebe, D.; Ullrich, T.; Kratzsch, J.; Dittrich, K.; Herberth, G.; Adams, V.; Kiess, W.; Erbs, S.; Körner, A. Chemerin as a mediator between obesity and vascular inflammation in children. J. Clin. Endocrinol. Metab. 2012, 97, E556–E564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams-Huet, B.; Devaraj, S.; Siegel, D.; Jialal, I. Increased adipose tissue insulin resistance in metabolic syndrome: Relationship to circulating adipokines. Metab. Syndr. Relat. Disord. 2014, 12, 503–507. [Google Scholar] [CrossRef]
- Rhee, E.J. Chemerin: A Novel Link between Inflammation and Atherosclerosis? Diabetes Metab. J. 2011, 35, 216–218. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Yuan, G.Y.; Wang, X.Z.; Jia, J.; Di, L.-L.; Yang, L.; Chen, X.; Qian, F.-F.; Chen, J.-J. Plasma chemerin level in metabolic syndrome. Genet. Mol. Res. 2013, 12, 5986–5991. [Google Scholar] [CrossRef]
- Barraco, G.M.; Luciano, R.; Semeraro, M.; Prieto-Hontoria, P.L.; Manco, M. Recently discovered adipokines and cardio-metabolic comorbidities in childhood obesity. Int. J. Mol. Sci. 2014, 15, 19760–19776. [Google Scholar] [CrossRef]
- Weigert, J.; Obermeier, F.; Neumeier, M.; Wanninger, J.; Filarsky, M.; Bauer, S.; Aslanidis, C.; Rogler, G.; Ott, C.; Schäffler, A.; et al. Circulating levels of chemerin and adiponectin are higher in ulcerative colitis and chemerin is elevated in Crohn’s disease. Inflamm. Bowel. Dis. 2010, 16, 630–637. [Google Scholar] [CrossRef] [Green Version]
- Terzoudis, S.; Malliaraki, N.; Damilakis, J.; Dimitriadou, D.A.; Zavos, C.; Koutroubakis, I.E. Chemerin, visfatin, and vaspin serum levels in relation to bone mineral density in patients with inflammatory bowel disease. Eur. J. Gastroenterol. Hepatol. 2016, 28, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Dranse, H.J.; Rourke, J.L.; Stadnyk, A.W.; Sinal, C.J. Local chemerin levels are positively associated with DSS-induced colitis but constitutive loss of CMKLR1 does not protect against development of colitis. Physiol. Rep. 2015, 3, e12497. [Google Scholar] [CrossRef] [PubMed]
- Catli, G.; Anik, A.; Abaci, A.; Kume, T.; Bober, E. Low omentin-1 levels are related with clinical and metabolic parameters in obese children. Exp. Clin. Endocrinol. Diabetes 2013, 121, 595–600. [Google Scholar] [CrossRef]
- Prats-Puig, A.; Bassols, J.; Bargallo, E.; Mas-Parareda, M.; Ribot, R.; Soriano-Rodríguez, P.; Berengüí, À.; Díaz, M.; de Zegher, F.; Ibánez, L.; et al. Toward an early marker of metabolic dysfunction: Omentin-1 in prepubertal children. Obesity 2011, 19, 1905–1907. [Google Scholar] [CrossRef]
- Lis, I.; Pilarski, L.; Bogdanski, P. Omentyna—Nowo odkryta adipocytokina w patogenezie insulinooporności. Pol. Merkur Lekarski 2015, 39, 56–60. [Google Scholar]
- Shrestha, B.; Patel, D.; Shah, H.; Hanna, K.S.; Kaur, H.; Alazzeh, M.S.; Thandavaram, A.; Channar, A.; Purohit, A.; Venugopal, S. The Role of Gut-Microbiota in the Pathophysiology and Therapy of Irritable Bowel Syndrome: A Systematic Review. Cureus 2022, 14, e28064. [Google Scholar] [CrossRef] [PubMed]
- Sood, R.; Law, G.R.; Ford, A.C. Diagnosis of IBS: Symptoms, symptom-based criteria, biomarkers or ‘psychomarkers’? Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 683–691. [Google Scholar] [CrossRef]
- Plavsic, I.; Hauser, G.; Tkalcic, M.; Pletikosić, S.; Salkić, N. Diagnosis of Irritable Bowel Syndrome: Role of Potential Biomarkers. Gastroenterol. Res. Pr. 2015, 2015, 490183. [Google Scholar] [CrossRef]
- Guo, Y.; Niu, K.; Momma, H.; Kobayashi, Y.; Chujo, M.; Otomo, A.; Fukudo, S.; Nagatomi, R. Irritable bowel syndrome is positively related to metabolic syndrome: A population-based cross-sectional study. PLoS ONE 2014, 9, e112289. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Cuevas, J.; Sandoval-Rodriguez, A.; Meza-Rios, A.; Monroy-Ramírez, H.C.; Galicia-Moreno, M.; García-Bañuelos, J.; Santos, A.; Armendariz-Borunda, J. Molecular Mechanisms of Obesity-Linked Cardiac Dysfunction: An Up-Date on Current Knowledge. Cells 2021, 10, 629. [Google Scholar] [CrossRef] [PubMed]
- Konrad, D.; Wueest, S. The gut-adipose-liver axis in the metabolic syndrome. Physiology 2014, 29, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Clegg, D.J. Metabolic Flexibility and Its Impact on Health Outcomes. Mayo Clin. Proc. 2022, 97, 761–776. [Google Scholar] [CrossRef]
- Rynders, C.A.; Blanc, S.; DeJong, N.; Bessesen, D.H.; Bergouignan, A. Sedentary behaviour is a key determinant of metabolic inflexibility. J. Physiol. 2018, 596, 1319–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llorente-Cantarero, F.J.; Aguilar-Gómez, F.J.; Bueno-Lozano, G.; Anguita-Ruiz, A.; Rupérez, A.I.; Vázquez-Cobela, R.; Flores-Rojas, K.; Aguilera, C.M.; Moreno, L.A.; Gil, A.; et al. Impact of Physical Activity Intensity Levels on the Cardiometabolic Risk Status of Children: The Genobox Study. Int. J. Sport. Nutr. Exerc. Metab. 2022, 32, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, N.; Diez, G.G.; Antúnez-Almagro, C.; Bressa, C.; Bailén, M.; González-Soltero, R.; Pérez, M.; Larrosa, M. Key Bacteria in the Gut Microbiota Network for the Transition between Sedentary and Active Lifestyle. Microorganisms 2020, 8, 785. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group | |
|---|---|---|
| IBS (n = 33) | Controls (n = 30) | |
| Age (years) | 13.6 ± 3.2 (5.7–17.8) | 13.6 ± 3.4 (5.1–17.5) |
| Height (cm) | 163.2 ± 18.5 (119.5–185.0) | 161.6 ± 19.7 (118.9–187.9) |
| Weight (kg) | 56.4 ± 21.4 (23.4–110.0) | 52.6 ± 19.5 (20.2–90.9) |
| Weight SDS | 0.47 ± 1.87 (−2.13–4.67) | 0.05 ± 1.14 (−1.42–2.58) |
| BMI (kg/m2) | 20.00 ± 4.69 (12.64–30.09) | 19.36 ± 4.31 (14.29–30.87) |
| BMI SDS | 0.22 ± 1.71 (−2.2–4.48) | −0.09 ± 1.33 (−1.38–3.66) |
| Waist circumference (cm) | 69.4 ± 12.4 (50.3–92.6) | 67.1 ± 10.4 (51.2–93.2) |
| Waist circumference SDS | 0.58 ± 2.75 (−3.07–6.93) | 0.19 ± 1.77 (−1.88–4.32) |
| WHR | 0.82 ± 0.05 (0.74–0.94) | 0.80 ± 0.05 (0.68–0.91) |
| CRP (mg/L) | 1.19 ± 1.28 (0.0–6.2) | 0.94 ± 0.84 (0.0–3.6) |
| Glucose (mg/dL) | 89.6 ± 6.9 (77.0–104.0) | 85.8 ± 8.0 (65.0–102.0) |
| Insulin (μU/mL) | 9.98 ± 5.99 (1.62–29.52) | 7.92 ± 4.53 (1.13–20.97) |
| ALT (U/L) | 9.8 ± 5.0 (5.8–29.1) | 10.2 ± 4.0 (4.3–22.9) |
| AST (U/L) | 18.2 ± 4.59 (10.7–32.3) | 19.8 ± 5.7 (11.8–36.0) |
| Total cholesterol (mmol/L) | 3.92 ± 0.82 (2.67–6.16) | 3.83 ± 0.58 (2.63–4.97) |
| HDL cholesterol (mmol/L) | 1.26 ± 0.31 a (0.86–2.17) | 1.49 ± 0.36 (0.92–2.29) |
| LDL cholesterol (mmol/L) | 2.18 ± 0.68 (1.11–4.27) | 2.02 ± 0.45 (1.06–2.83) |
| Triglycerides (mmol/L) | 1.05 ± 0.49 b (0.37–2.81) | 0.68 ± 0.32 (0.42–1.94) |
| HOMA-IR | 2.21 ± 1.5 b (0.36–7.14) | 1.57 ± 0.81 (0.23–3.59) |
| Parameter | IBS (n = 33) | Controls (n = 30) | ||||||
|---|---|---|---|---|---|---|---|---|
| Leptin (ng/mL) | Adiponectin (µg/mL) | Chemerin (ng/mL) | Omentin-1 (ng/mL) | Leptin (ng/mL) | Adiponectin (µg/mL) | Chemerin (ng/mL) | Omentin-1 (ng/mL) | |
| Age (years) | r = −0.07 p = 0.70 | r = −0.34 p = 0.06 | r = 0.11 p = 0.58 | r = −0.22 p = 0.24 | r = 0.27 p = 0.15 | r = −0.47 * p = 0.009 | r = −0.31 p = 0.09 | r = 0.14 p = 0.46 |
| Height (cm) | r = −0.01 p = 0.99 | r = −0.49 * p = 0.03 | r = 0.09 p = 0.63 | r = −0.39 * p = 0.03 | r = −0.04 p = 0.84 | r = −0.48 * p = 0.007 | r = −0.52 * p = 0.004 | r = 0.10 p = 0.59 |
| Weight (kg) | r = 0.44 * p = 0.01 | r = −0.51 * p = 0.004 | r = 0.33 p = 0.08 | r = −0.49 * p = 0.006 | r = 0.31 p = 0.09 | r = −0.58 * p = 0.001 | r = −0.34 p = 0.06 | r = −0.14 p = 0.47 |
| Weight SDS | r = 0.56 * p < 0.001 | r = −0.31 p = 0.10 | r = 0.39 p = 0.03 | r = −0.43 * p = 0.02 | r = 0.27 p = 0.15 | r = −0.28 p = 0.13 | r = −0.16 p = 0.40 | r = −0.36 * p = 0.049 |
| BMI (kg/m2) | r = 0.57 * p < 0.001 | r = −0.41 * p = 0.02 | r = 0.47 p = 0.01 | r = −0.52 * p = 0.003 | r = 0.44 p = 0.01 | r = −0.49 * p = 0.006 | r = −0.10 p = 0.59 | r = −0.31 p = 0.10 |
| BMI-SDS | r = 0.63 * p < 0.001 | r = −0.25 p = 0.10 | r = 0.48 p = 0.007 | r = −0.44 * p = 0.02 | r = 0.40 p = 0.03 | r = −0.33 p = 0.08 | r = −0.02 p = 0.90 | r = −0.45 * p = 0.01 |
| Waist circ. (cm) | r = 0.49 * p < 0.001 | r = −0.52 * p = 0.003 | r = 0.36 p = 0.05 | r = −0.54 * p = 0.002 | r = 0.39 p = 0.03 | r = −0.48 * p = 0.007 | r = −0.28 p = 0.13 | r = −0.12 p = 0.50 |
| Waist circ. SDS | r = 0.54 * p = 0.001 | r = −0.26 p = 0.14 | r = 0.45 p = 0.007 | r = −0.44 * p = 0.009 | r = 0.35 p = 0.05 | r = −0.25 p = 0.18 | r = −0.01 p = 0.93 | r = −0.21 p = 0.26 |
| WHR | r = 0.33 * p = 0.004 | r = −0.25 p = 0.17 | r = 0.26 p = 0.16 | r = −0.42 * p = 0.02 | r = −0.06 p = 0.76 | r = 0.80 p = 0.69 | r = 0.04 p = 0.84 | r = −0.17 p = 0.37 |
| Parameter | IBS (n = 33) | Controls (n = 30) | ||||||
|---|---|---|---|---|---|---|---|---|
| Leptin (ng/mL) | Adiponectin (µg/mL) | Chemerin (ng/mL) | Omentin-1 (ng/mL) | Leptin (ng/mL) | Adiponectin (µg/mL) | Chemerin (ng/mL) | Omentin-1 (ng/mL) | |
| CRP (mg/L) | r = 0.44 * p = 0.01 | r = −0.06 p = 0.75 | r = 0.31 p = 0.08 | r = −0.36 * p = 0.04 | r = −0.06 p = 0.77 | r = −0.07 p = 0.71 | r = 0.33 p = 0.08 | r = 0.13 p = 0.50 |
| Glucose (mg/dL) | r = 0.29 p = 0.12 | r = −0.15 p = 0.44 | r = 0.10 p = 0.62 | r = −0.30 p = 0.11 | r = −0.07 p = 0.70 | r = 0.05 p = 0.80 | r = −0.25 p = 0.80 | r = −0.29 p = 0.12 |
| Insulin (μU/mL) | r = 0.53 * p = 0.001 | r = −0.36 p = 0.05 | r = 0.53 * p = 0.003 | r = −0.50 * p = 0.005 | r = 0.48 * p = 0.007 | r = −0.47 * p = 0.009 | r = −0.15 p = 0.42 | r = −0.30 p = 0.11 |
| ALT (U/L) | r = 0.30 p = 0.90 | r = −0.15 p = 0.42 | r = 0.18 p = 0.31 | r = −0.21 p = 0.24 | r = 0.23 p = 0.22 | r = −0.11 p = 0.58 | r = −0.34 p = 0.07 | r = −0.34 p = 0.07 |
| AST (U/L) | r = −0.17 p = 0.35 | r = −0.03 p = 0.90 | r = −0.04 p = 0.82 | r = 0.26 p = 0.16 | r = −0.31 p = 0.09 | r = 0.16 p = 0.39 | r = −0.23 p = 0.22 | r = −0.09 p = 0.65 |
| Total cholesterol (mmol/L) | r = 0.21 p = 0.24 | r = 0.37 * p = 0.05 | r = 0.45 * p = 0.01 | r = 0.06 p = 0.74 | r = −0.03 p = 0.89 | r = 0.29 p = 0.12 | r = −0.06 p = 0.77 | r = −0.16 p = 0.40 |
| HDL cholesterol (mmol/L) | r = −0.19 p = 0.28 | r = 0.19 p = 0.31 | r = −0.17 p = 0.37 | r = 0.38 * p = 0.04 | r = 0.01 p = 0.99 | r = 0.39 * p = 0.03 | r = −0.10 p = 0.60 | r = −0.10 p = 0.60 |
| LDL cholesterol (mmol/L) | r = 0.26 p = 0.14 | r = 0.36 * p = 0.05 | r = 0.49 * p = 0.006 | r = 0.03 p = 0.88 | r = −0.03 p = 0.86 | r = 0.17 p = 0.37 | r = −0.01 p = 0.98 | r = −0.08 p = 0.68 |
| Triglycerides (mmol/L) | r = 0.36 * p = 0.04 | r = 0.03 p = 0.86 | r = 0.41 * p = 0.02 | r = −0.37 * p = 0.04 | r = 0.18 p = 0.34 | r = −0.33 p = 0.08 | r = 0.07 p = 0.70 | r = −0.11 p = 0.57 |
| HOMA-IR | r = 0.61 * p < 0.001 | r = −0.37 * p = 0.04 | r = 0.50 * p = 0.004 | r = −0.49 * p = 0.006 | r = 0.39 * p = 0.04 | r = −0.44 * p = 0.01 | r = −0.23 p = 0.21 | r = −0.26 p = 0.21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roczniak, W.; Szymlak, A.; Mazur, B.; Chobot, A.; Stojewska, M.; Oświęcimska, J. Nutritional Status and Selected Adipokines in Children with Irritable Bowel Syndrome. Nutrients 2022, 14, 5282. https://doi.org/10.3390/nu14245282
Roczniak W, Szymlak A, Mazur B, Chobot A, Stojewska M, Oświęcimska J. Nutritional Status and Selected Adipokines in Children with Irritable Bowel Syndrome. Nutrients. 2022; 14(24):5282. https://doi.org/10.3390/nu14245282
Chicago/Turabian StyleRoczniak, Wojciech, Agnieszka Szymlak, Bogdan Mazur, Agata Chobot, Małgorzata Stojewska, and Joanna Oświęcimska. 2022. "Nutritional Status and Selected Adipokines in Children with Irritable Bowel Syndrome" Nutrients 14, no. 24: 5282. https://doi.org/10.3390/nu14245282