

Adipose and Plasma microRNAs miR-221 and 222 Associate with Obesity, Insulin Resistance, and New Onset Diabetes after Peritoneal Dialysis
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
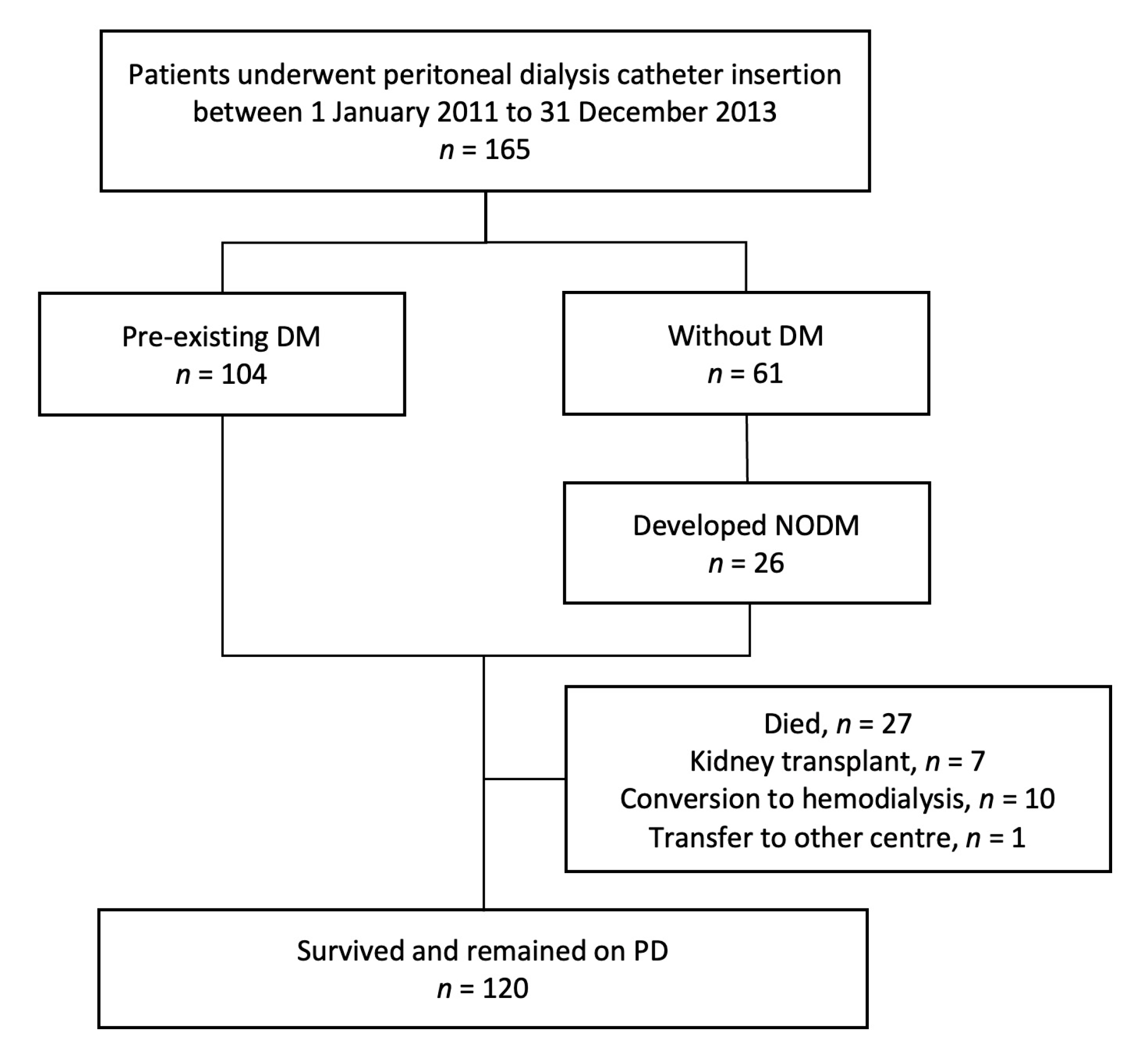
2.1. Study Design
2.2. Extraction of RNA and miRNA
2.3. Anthropometric Measurements
2.4. Glycemic Profile
2.5. Other Clinical and Biochemical Parameters
2.6. Follow-Up and Outcome Measurements
2.7. Statistical Analysis
3. Results
3.1. Clinical Characteristics
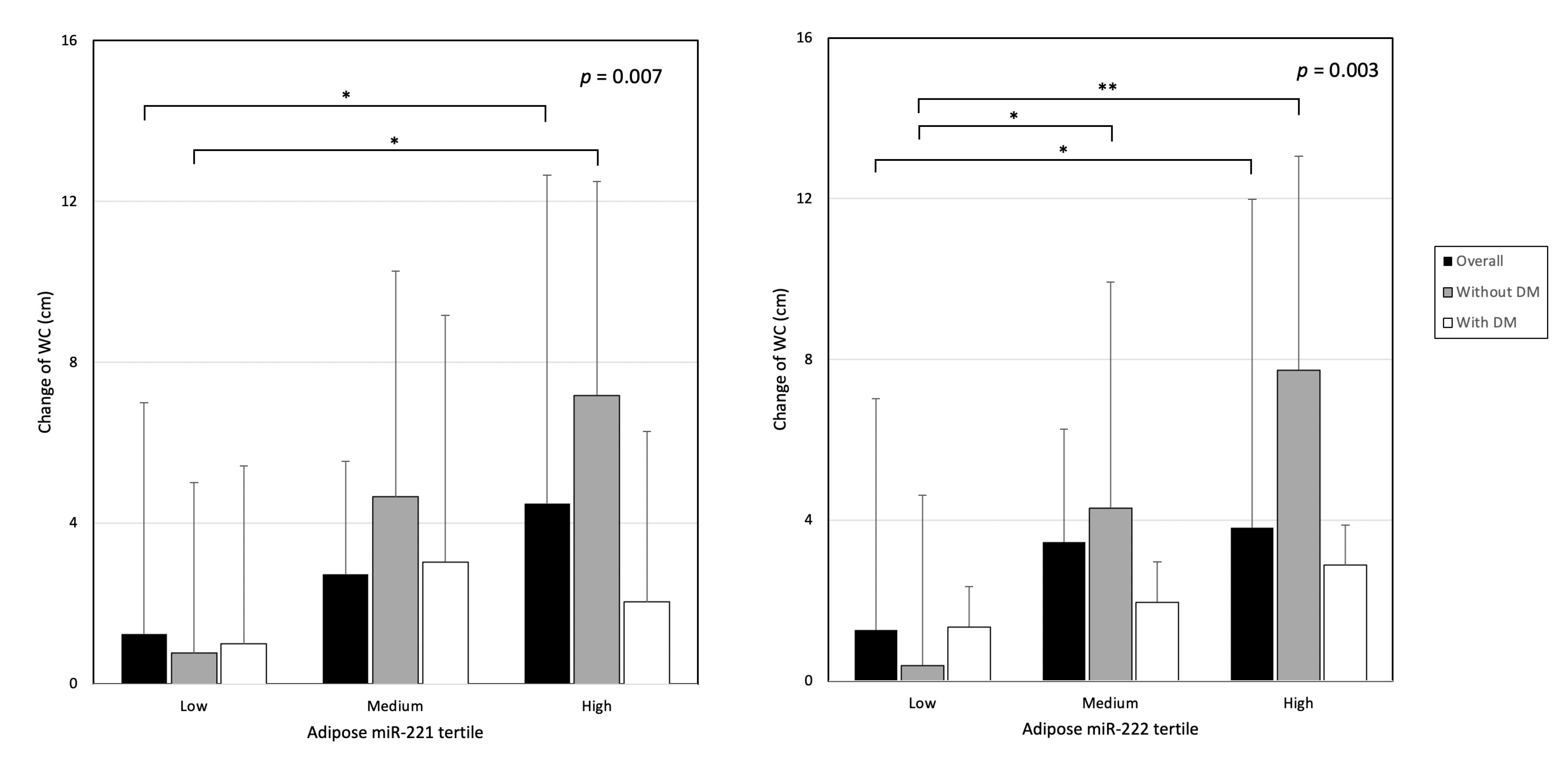
3.2. Changes in Adiposity
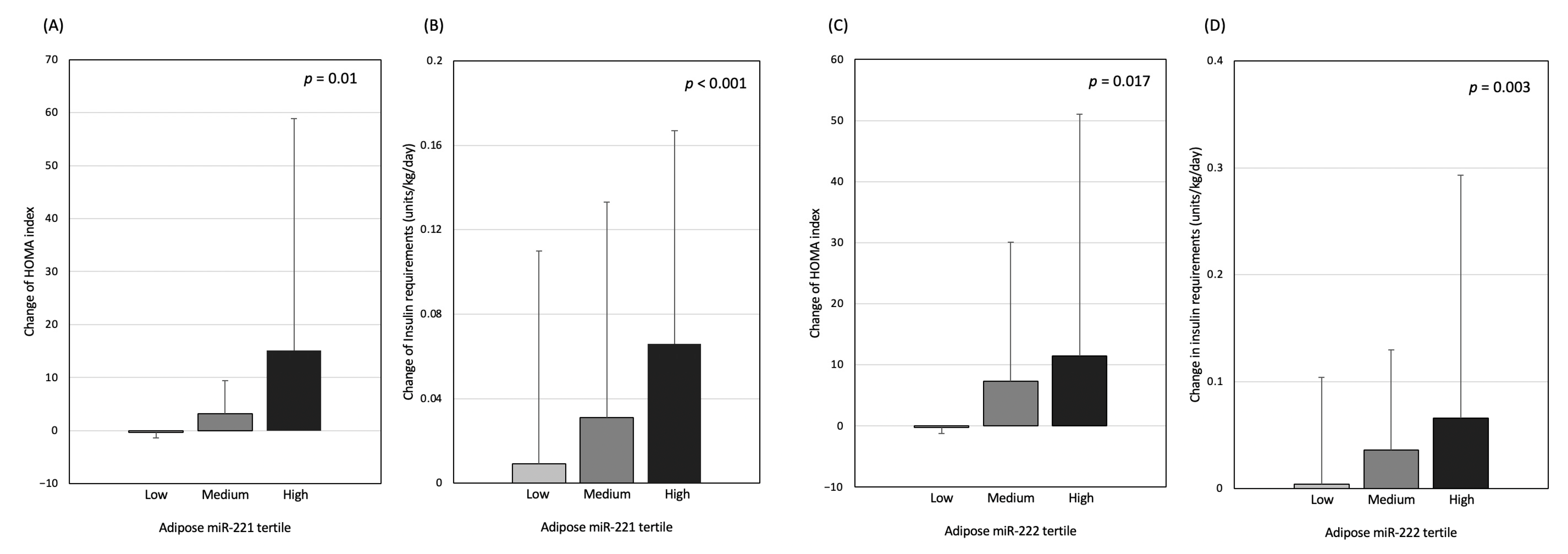
3.3. Changes in Glycaemic Parameters
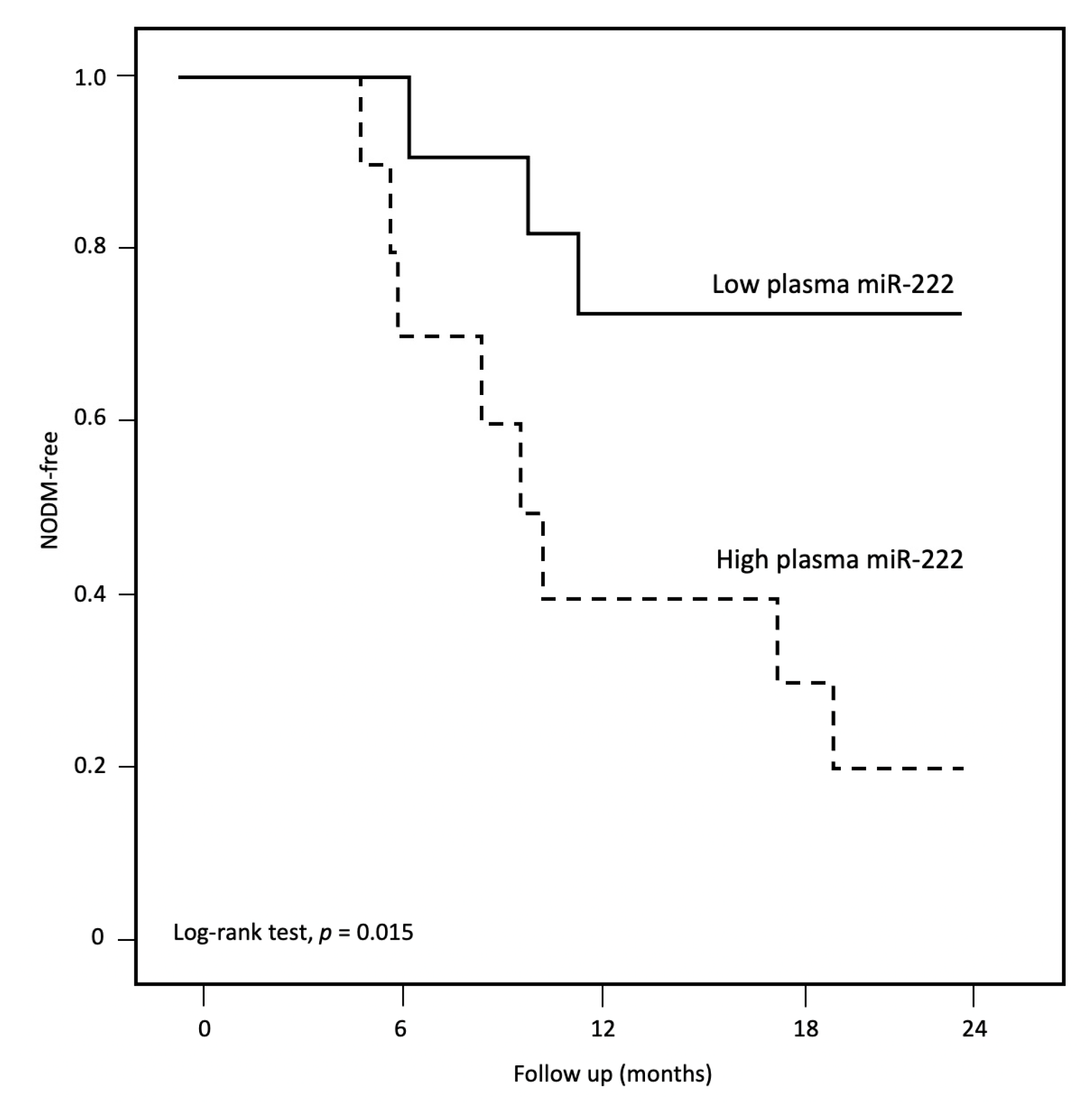
3.4. New Onset Diabetes Mellitus after Peritoneal Dialysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gokal, R.; Moberly, J.; Lindholm, B.; Mujais, S. Metabolic and laboratory effects of icodextrin. Kidney Int. 2002, 62, S62–S71. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.K.; Kim, Y.S.; Song, Y.R.; Kim, H.J.; Kim, S.G.; Moon, S.J. Excessive Weight Gain during the First Year of Peritoneal Dialysis Is Associated with Inflammation, Diabetes Mellitus, and a Rapid Decrease in Residual Renal Function. PLoS ONE 2015, 10, e0139033. [Google Scholar] [CrossRef] [PubMed]
- Choy, A.S.-M.; Chow, K.-M.; Kwan, B.C.-H.; Cheng, P.M.-S.; Kwong, V.W.-K.; Pang, W.-F.; Leung, C.-B.; Law, M.-C.; Li, P.K.-T.; Szeto, C.-C. Weight change during the first year of peritoneal dialysis: Risk factors and prognostic implications. Hong Kong J. Nephrol. 2015, 17, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.K.; Park, H.C.; Song, Y.R.; Kim, H.J.; Moon, S.J.; Kim, S.G. Effects of Excessive Body Fat Accumulation on Long-Term Outcomes during Peritoneal Dialysis. Perit. Dial. Int. 2019, 39, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Than, W.H.; Ng, J.K.; Chan, G.C.; Fung, W.W.; Chow, K.M.; Szeto, C.C. The change in the prevalence of obesity and new-onset diabetes in Chinese peritoneal dialysis patients over 25 years. Clin. Kidney J. 2022, 15, 70–78. [Google Scholar] [CrossRef]
- Szeto, C.C.; Chow, K.M.; Leung, C.B.; Kwan, B.C.; Chung, K.Y.; Law, M.C.; Li, P.K. Increased subcutaneous insulin requirements in diabetic patients recently commenced on peritoneal dialysis. Nephrol. Dial. Transplant. 2007, 22, 1697–1702. [Google Scholar] [CrossRef] [Green Version]
- Obi, Y.; Streja, E.; Mehrotra, R.; Rivara, M.B.; Rhee, C.M.; Soohoo, M.; Gillen, D.L.; Lau, W.L.; Kovesdy, C.P.; Kalantar-Zadeh, K. Impact of Obesity on Modality Longevity, Residual Kidney Function, Peritonitis, and Survival among Incident Peritoneal Dialysis Patients. Am. J. Kidney Dis. 2018, 71, 802–813. [Google Scholar] [CrossRef]
- Chan, G.C.-K.; Jack Kit-Chung, N.G.; Chow, K.M.; Kwong, V.W.; Pang, W.F.; Cheng, P.M.; Law, M.C.; Leung, C.B.; Philip Kam-Tao, L.I.; Szeto, C.C. Interaction between central obesity and frailty on the clinical outcome of peritoneal dialysis patients. PLoS ONE 2020, 15, e0241242. [Google Scholar] [CrossRef]
- Yarragudi, R.; Gessl, A.; Vychytil, A. New-Onset Diabetes Mellitus in Peritoneal Dialysis and Hemodialysis Patients: Frequency, Risk Factors, and Prognosis—A Review. Ther. Apher. Dial. 2019, 23, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chan, G.C.; Than, W.H.; Kwan, B.C.; Lai, K.B.; Chan, R.C.; Ng, J.K.; Chow, K.M.; Cheng, P.M.; Law, M.C.; Leung, C.B.; et al. Adipose expression of miR-130b and miR-17-5p with wasting, cardiovascular event and mortality in advanced chronic kidney disease patients. Nephrol. Dial. Transplant. 2021, 37, 1935–1943. [Google Scholar] [CrossRef]
- Chan, G.C.; Than, W.H.; Kwan, B.C.; Lai, K.B.; Chan, R.C.; Teoh, J.Y.; Ng, J.K.; Chow, K.M.; Fung, W.W.; Cheng, P.M.; et al. Adipose and serum zinc alpha-2-glycoprotein (ZAG) expressions predict longitudinal change of adiposity, wasting and predict survival in dialysis patients. Sci. Rep. 2022, 12, 9087. [Google Scholar] [CrossRef]
- Chan, G.C.; Than, W.H.; Kwan, B.C.; Lai, K.B.; Chan, R.C.; Teoh, J.Y.; Ng, J.K.; Chow, K.M.; Fung, W.W.; Cheng, P.M.; et al. Zinc alpha-2-glycoprotein (ZAG) in Peritoneal Dialysis Effluent Correlates with Peritoneal Transport Characteristics, Peritonitis Rate and Outcome. Kidney Res. Clin. Pract. 2022, in press. [Google Scholar]
- Shi, Z.; Zhao, C.; Guo, X.; Ding, H.; Cui, Y.; Shen, R.; Liu, J. Differential expression of microRNAs in omental adipose tissue from gestational diabetes mellitus subjects reveals miR-222 as a regulator of ERalpha expression in estrogen-induced insulin resistance. Endocrinology 2014, 155, 1982–1990. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.J.; Mercader, J.M.; Catalan, V.; Moreno-Navarrete, J.M.; Pueyo, N.; Sabater, M.; Gomez-Ambrosi, J.; Anglada, R.; Fernandez-Formoso, J.A.; Ricart, W.; et al. Targeting the circulating microRNA signature of obesity. Clin. Chem. 2013, 59, 781–792. [Google Scholar] [CrossRef] [Green Version]
- Li, M.Y.; Pan, S.R.; Qiu, A.Y. Roles of microRNA-221/222 in type 2 diabetic patients with post-menopausal breast cancer. Genet. Mol. Res. 2016, 15, 10–4238. [Google Scholar] [CrossRef]
- De Candia, P.; Spinetti, G.; Specchia, C.; Sangalli, E.; La Sala, L.; Uccellatore, A.; Lupini, S.; Genovese, S.; Matarese, G.; Ceriello, A. A unique plasma microRNA profile defines type 2 diabetes progression. PLoS ONE 2017, 12, e0188980. [Google Scholar] [CrossRef] [Green Version]
- Fodor, A.; Lazar, A.L.; Buchman, C.; Tiperciuc, B.; Orasan, O.H.; Cozma, A. MicroRNAs: The Link between the Metabolic Syndrome and Oncogenesis. Int. J. Mol. Sci. 2021, 22, 6337. [Google Scholar] [CrossRef]
- Villard, A.; Marchand, L.; Thivolet, C.; Rome, S. Diagnostic Value of Cell-free Circulating MicroRNAs for Obesity and Type 2 Diabetes: A Meta-analysis. J. Mol. Biomark. Diagn. 2015, 6, 251. [Google Scholar] [CrossRef] [Green Version]
- Matias-Garcia, P.R.; Wilson, R.; Mussack, V.; Reischl, E.; Waldenberger, M.; Gieger, C.; Anton, G.; Peters, A.; Kuehn-Steven, A. Impact of long-term storage and freeze-thawing on eight circulating microRNAs in plasma samples. PLoS ONE 2020, 15, e0227648. [Google Scholar] [CrossRef] [Green Version]
- Neville, M.J.; Collins, J.M.; Gloyn, A.L.; McCarthy, M.I.; Karpe, F. Comprehensive human adipose tissue mRNA and microRNA endogenous control selection for quantitative real-time-PCR normalization. Obesity 2011, 19, 888–892. [Google Scholar] [CrossRef]
- Rao, X.; Huang, X.; Zhou, Z.; Lin, X. An improvement of the 2^(-delta delta CT) method for quantitative real-time polymerase chain reaction data analysis. Biostat. Bioinform. Biomath. 2013, 3, 71–85. [Google Scholar]
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. 1), S17–S38. [Google Scholar] [CrossRef] [PubMed]
- Li, P.K.; Chan, G.C.; Chen, J.; Chen, H.C.; Cheng, Y.L.; Fan, S.L.; He, J.C.; Hu, W.; Lim, W.H.; Pei, Y.; et al. Tackling Dialysis Burden around the World: A Global Challenge. Kidney Dis. 2021, 7, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Li, P.K.; Chow, K.M.; Van de Luijtgaarden, M.W.; Johnson, D.W.; Jager, K.J.; Mehrotra, R.; Naicker, S.; Pecoits-Filho, R.; Yu, X.Q.; Lameire, N. Changes in the worldwide epidemiology of peritoneal dialysis. Nat. Rev. Nephrol. 2017, 13, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, J.M.; Niu, J.; Ho, V.; Winkelmayer, W.C.; Erickson, K.F. A Comparison of US Medicare Expenditures for Hemodialysis and Peritoneal Dialysis. J. Am. Soc. Nephrol. 2022, 33, 2059–2070. [Google Scholar] [CrossRef]
- Caron-Lienert, R.S.; Poli-de-Figueiredo, C.E.; Figueiredo, A.; da Costa, B.E.P.; Crepaldi, C.; Pizzato, A.C.; Ferrari, F.; Giuliani, A.; Ronco, C. The Influence of Glucose Exposure Load and Peritoneal Membrane Transport on Body Composition and Nutritional Status Changes after 1 Year on Peritoneal Dialysis. Perit. Dial. Int. 2017, 37, 458–463. [Google Scholar] [CrossRef]
- Law, S.; Davenport, A. Glucose absorption from peritoneal dialysate is associated with a gain in fat mass and a reduction in lean body mass in prevalent peritoneal dialysis patients. Br. J. Nutr. 2020, 123, 1269–1276. [Google Scholar] [CrossRef]
- Xie, H.; Lim, B.; Lodish, H.F. MicroRNAs induced during adipogenesis that accelerate fat cell development are downregulated in obesity. Diabetes 2009, 58, 1050–1057. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.J.; Moreno-Navarrete, J.M.; Pardo, G.; Sabater, M.; Hummel, M.; Ferrer, A.; Rodriguez-Hermosa, J.I.; Ruiz, B.; Ricart, W.; Peral, B.; et al. MiRNA expression profile of human subcutaneous adipose and during adipocyte differentiation. PLoS ONE 2010, 5, e9022. [Google Scholar] [CrossRef] [Green Version]
- Meerson, A.; Traurig, M.; Ossowski, V.; Fleming, J.M.; Mullins, M.; Baier, L.J. Human adipose microRNA-221 is upregulated in obesity and affects fat metabolism downstream of leptin and TNF-alpha. Diabetologia 2013, 56, 1971–1979. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Jiang, L.; Shan, A.; Su, Y.; Cheng, Y.; Song, D.; Ji, H.; Ning, G.; Wang, W.; Cao, Y. Targeting hepatic miR-221/222 for therapeutic intervention of nonalcoholic steatohepatitis in mice. EBioMedicine 2018, 37, 307–321. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.; Shan, A.; Su, Y.; Cheng, Y.; Ji, H.; Yang, Q.; Lei, Y.; Liu, B.; Wang, W.; Ning, G.; et al. MiR-221/222 Inhibit Insulin Production of Pancreatic beta-Cells in Mice. Endocrinology 2020, 161, bqz027. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Zhang, D.; Katayama, A.; Kurooka, N.; Sugawara, R.; Albuayjan, H.H.H.; Nakatsuka, A.; Eguchi, J.; Wada, J. Adipocyte-Specific Inhibition of Mir221/222 Ameliorates Diet-Induced Obesity Through Targeting Ddit4. Front. Endocrinol. 2021, 12, 750261. [Google Scholar] [CrossRef]
- Song, J.; Ouyang, Y.; Che, J.; Li, X.; Zhao, Y.; Yang, K.; Zhao, X.; Chen, Y.; Fan, C.; Yuan, W. Potential Value of miR-221/222 as Diagnostic, Prognostic, and Therapeutic Biomarkers for Diseases. Front. Immunol. 2017, 8, 56. [Google Scholar] [CrossRef] [Green Version]
- Fernstrom, A.; Hylander, B.; Moritz, A.; Jacobsson, H.; Rossner, S. Increase of intra-abdominal fat in patients treated with continuous ambulatory peritoneal dialysis. Perit. Dial. Int. 1998, 18, 166–171. [Google Scholar] [CrossRef]
- Szeto, C.C.; Chow, K.M.; Kwan, B.C.; Chung, K.Y.; Leung, C.B.; Li, P.K. New-onset hyperglycemia in nondiabetic chinese patients started on peritoneal dialysis. Am. J. Kidney Dis. 2007, 49, 524–532. [Google Scholar] [CrossRef]
- Tien, K.J.; Lin, Z.Z.; Chio, C.C.; Wang, J.J.; Chu, C.C.; Sun, Y.M.; Kan, W.C.; Chien, C.C. Epidemiology and mortality of new-onset diabetes after dialysis: Taiwan national cohort study. Diabetes Care 2013, 36, 3027–3032. [Google Scholar] [CrossRef] [Green Version]
- Chou, C.Y.; Liang, C.C.; Kuo, H.L.; Chang, C.T.; Liu, J.H.; Lin, H.H.; Wang, I.K.; Yang, Y.F.; Huang, C.C. Comparing risk of new onset diabetes mellitus in chronic kidney disease patients receiving peritoneal dialysis and hemodialysis using propensity score matching. PLoS ONE 2014, 9, e87891. [Google Scholar] [CrossRef] [Green Version]
- Wang, I.K.; Lin, C.L.; Chen, H.C.; Lin, S.Y.; Chang, C.T.; Yen, T.H.; Sung, F.C. Risk of new-onset diabetes in end-stage renal disease patients undergoing dialysis: Analysis from registry data of Taiwan. Nephrol. Dial. Transplant. 2018, 33, 670–675. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.; Zhou, Y.; Deng, Z.; Zhang, H.; Wu, Y.; Song, T.; Yang, Y.; Wei, H.; Peng, J. miR-221 negatively regulates inflammation and insulin sensitivity in white adipose tissue by repression of sirtuin-1 (SIRT1). J. Cell. Biochem. 2018, 119, 6418–6428. [Google Scholar] [CrossRef]
- Le Sage, C.; Nagel, R.; Egan, D.A.; Schrier, M.; Mesman, E.; Mangiola, A.; Anile, C.; Maira, G.; Mercatelli, N.; Ciafre, S.A.; et al. Regulation of the p27(Kip1) tumor suppressor by miR-221 and miR-222 promotes cancer cell proliferation. EMBO J. 2007, 26, 3699–3708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, K.; Igata, M.; Kondo, T.; Kitano, S.; Takaki, Y.; Hanatani, S.; Sakaguchi, M.; Goto, R.; Senokuchi, T.; Kawashima, J.; et al. Identification of microRNA that represses IRS-1 expression in liver. PLoS ONE 2018, 13, e0191553. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Song, H.; Shuo, L.; Wang, L.; Xie, P.; Li, W.; Liu, J.; Tong, Y.; Zhang, C.Y.; Jiang, X.; et al. Gonadal white adipose tissue-derived exosomal MiR-222 promotes obesity-associated insulin resistance. Aging 2020, 12, 22719–22743. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.W.; Wang, Y.T.; Liao, Y.C.; Chuang, S.C.; Wang, S.N.; Juo, S.H. Decreased microRNA-221 is associated with high levels of TNF-alpha in human adipose tissue-derived mesenchymal stem cells from obese woman. Cell. Physiol. Biochem. 2013, 32, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Tsukita, S.; Yamada, T.; Takahashi, K.; Munakata, Y.; Hosaka, S.; Takahashi, H.; Gao, J.; Shirai, Y.; Kodama, S.; Asai, Y.; et al. MicroRNAs 106b and 222 Improve Hyperglycemia in a Mouse Model of Insulin-Deficient Diabetes via Pancreatic beta-Cell Proliferation. EBioMedicine 2017, 15, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.; Yang, Z.K.; Chen, Y. Older Age, Higher Body Mass Index and Inflammation Increase the Risk for New-Onset Diabetes and Impaired Glucose Tolerance in Patients on Peritoneal Dialysis. Perit. Dial. Int. 2016, 36, 277–283. [Google Scholar] [CrossRef]
- Rivara, M.B.; Mehrotra, R. New-Onset Diabetes in Peritoneal Dialysis Patients—Which Predictors Really Matter? Perit. Dial. Int. 2016, 36, 243–246. [Google Scholar] [CrossRef] [Green Version]
- Ho, L.C.; Yen, C.J.; Chao, C.T.; Chiang, C.K.; Huang, J.W.; Hung, K.Y. Visceral fat area is associated with HbA1c but not dialysate-related glucose load in nondiabetic PD patients. Sci. Rep. 2015, 5, 12811. [Google Scholar] [CrossRef] [Green Version]
- Nejad, C.; Stunden, H.J.; Gantier, M.P. A guide to miRNAs in inflammation and innate immune responses. FEBS J. 2018, 285, 3695–3716. [Google Scholar] [CrossRef] [Green Version]
- Sadeghzadeh, S.; Dehghani Ashkezari, M.; Seifati, S.M.; Vahidi Mehrjardi, M.Y.; Dehghan Tezerjani, M.; Sadeghzadeh, S.; Ladan, S.A.B. Circulating miR-15a and miR-222 as Potential Biomarkers of Type 2 Diabetes. Diabetes Metab. Syndr. Obes. 2020, 13, 3461–3469. [Google Scholar] [CrossRef]
- Filardi, T.; Catanzaro, G.; Grieco, G.E.; Splendiani, E.; Trocchianesi, S.; Santangelo, C.; Brunelli, R.; Guarino, E.; Sebastiani, G.; Dotta, F.; et al. Identification and Validation of miR-222-3p and miR-409-3p as Plasma Biomarkers in Gestational Diabetes Mellitus Sharing Validated Target Genes Involved in Metabolic Homeostasis. Int. J. Mol. Sci. 2022, 23, 4276. [Google Scholar] [CrossRef]
- Icli, B.; Feinberg, M.W. MicroRNAs in dysfunctional adipose tissue: Cardiovascular implications. Cardiovasc. Res. 2017, 113, 1024–1034. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Derose, S.F.; Nicholas, S.; Benner, D.; Sharma, K.; Kovesdy, C.P. Burnt-out diabetes: Impact of chronic kidney disease progression on the natural course of diabetes mellitus. J. Ren. Nutr. 2009, 19, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Abe, M.; Hamano, T.; Hoshino, J.; Wada, A.; Nakai, S.; Masakane, I. Rate of the “burnt-out diabetes” phenomenon in patients on peritoneal dialysis. Diabetes Res. Clin. Pract. 2018, 143, 254–262. [Google Scholar] [CrossRef]
- Muralidharan, J.; Ramezani, A.; Hubal, M.; Knoblach, S.; Shrivastav, S.; Karandish, S.; Scott, R.; Maxwell, N.; Ozturk, S.; Beddhu, S.; et al. Extracellular microRNA signature in chronic kidney disease. Am. J. Physiol. Ren. Physiol. 2017, 312, F982–F991. [Google Scholar] [CrossRef] [Green Version]
- Neal, C.S.; Michael, M.Z.; Pimlott, L.K.; Yong, T.Y.; Li, J.Y.; Gleadle, J.M. Circulating microRNA expression is reduced in chronic kidney disease. Nephrol. Dial. Transplant. 2011, 26, 3794–3802. [Google Scholar] [CrossRef] [Green Version]
- Peiro-Chova, L.; Pena-Chilet, M.; Lopez-Guerrero, J.A.; Garcia-Gimenez, J.L.; Alonso-Yuste, E.; Burgues, O.; Lluch, A.; Ferrer-Lozano, J.; Ribas, G. High stability of microRNAs in tissue samples of compromised quality. Virchows Arch. 2013, 463, 765–774. [Google Scholar] [CrossRef]
- Ge, Q.; Zhou, Y.; Lu, J.; Bai, Y.; Xie, X.; Lu, Z. miRNA in plasma exosome is stable under different storage conditions. Molecules 2014, 19, 1568–1575. [Google Scholar] [CrossRef] [Green Version]
- Balzano, F.; Deiana, M.; Dei Giudici, S.; Oggiano, A.; Baralla, A.; Pasella, S.; Mannu, A.; Pescatori, M.; Porcu, B.; Fanciulli, G.; et al. miRNA Stability in Frozen Plasma Samples. Molecules 2015, 20, 19030–19040. [Google Scholar] [CrossRef] [Green Version]
- Glinge, C.; Clauss, S.; Boddum, K.; Jabbari, R.; Jabbari, J.; Risgaard, B.; Tomsits, P.; Hildebrand, B.; Kaab, S.; Wakili, R.; et al. Stability of Circulating Blood-Based MicroRNAs—Pre-Analytic Methodological Considerations. PLoS ONE 2017, 12, e0167969. [Google Scholar] [CrossRef]
- Spoto, B.; Pisano, A.; Zoccali, C. Insulin resistance in chronic kidney disease: A systematic review. Am. J. Physiol. Ren. Physiol. 2016, 311, F1087–F1108. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| With DM (n = 104) | Without DM (n = 61) | p-Value | |
|---|---|---|---|
| Age | 60.9 ± 9.0 | 54.1 ± 12.9 | p < 0.001 a |
| Male sex, No. (%) | 86 (82.7%) | 40 (65.6%) | p = 0.01 b |
| Primary renal disease, No. (%) | p < 0.001 b | ||
| Diabetes mellitus | 85 (81.7%) | 0 (0%) | |
| Hypertension | 3 (2.9%) | 12 (19.7%) | |
| Glomerulonephritis | 10 (9.6%) | 27 (44.3%) | |
| Polycystic kidney disease | 2 (1.9%) | 1 (1.6%) | |
| Urological | 0 (0%) | 6 (9.8%) | |
| Others | 1 (1.0%) | 2 (3.3%) | |
| Unknown | 3 (2.9%) | 13 (21.3%) | |
| Comorbidities | |||
| Ischemic heart disease | 39 (37.5%) | 7 (11.5%) | p < 0.001 b |
| Cerebrovascular accident | 23 (22.1%) | 9 (14.8%) | p = 0.2 b |
| Peripheral vascular disease | 12 (11.5%) | 0 (0%) | p = 0.006 b |
| Charlson comorbidities index | 7.3 ± 1.9 | 4.3 ± 2.0 | p < 0.001 a |
| Residual GFR (ml/min/1.73 m2) | 4.4 ± 2.8 | 3.1 ± 2.3 | p = 0.01 a |
| nPCR (g/kg/day) | 1.1 ± 0.3 | 1.1 ± 0.2 | p = 0.2 a |
| Laboratory parameters | |||
| Urea (mmol/L) | 30.4 ± 7.4 | 31.0 ± 8.0 | p = 0.7 a |
| Creatinine (umol/L) | 811 ± 236 | 921 ± 303 | p = 0.02 a |
| Albumin (g/L) | 34.9 ± 4.2 | 35.9 ± 4.7 | p = 0.2 a |
| High-sensitive C-reactive protein (mg/L) | 10.7 ± 26.3 | 15.6 ± 33.5 | p = 0.3 a |
| Cholesterol, total (mmol/L) | 4.5 ± 1.2 | 4.6 ± 1.2 | p = 0.7 a |
| High-density lipoprotein (mmol/L) | 1.2 ± 0.4 | 1.3 ± 0.3 | p = 0.1 a |
| Low-density lipoprotein (mmol/L) | 2.5 ± 1.0 | 2.7 ± 1.1 | p = 0.5 a |
| Triglycerides (mmol/L) | 1.6 ± 0.9 | 1.3 ± 0.7 | p = 0.03 a |
| Peritoneal characteristics | |||
| D/P4 | 0.69 ± 0.13 | 0.69 ± 0.12 | p = 0.8 a |
| MTAC | 10.6 ± 4.9 | 11.3 ± 5.2 | p = 0.4 a |
| Pulse wave velocity | |||
| Carotid-femoral (m/s) | 12.0 ± 2.4 | 10.5 ± 1.9 | p < 0.001 a |
| Carotid-radial (m/s) | 10.5 ± 1.3 | 10.6 ± 1.4 | p = 0.6 a |
| Medication use | |||
| Statins | 15 (24.6%) | 63 (60.6%) | p < 0.001 b |
| Beta blockers | 44 (72.1%) | 83 (79.8%) | p = 0.3 b |
| Thiazide diuretics | 19 (31.1%) | 49 (47.1%) | p = 0.04 b |
| Antidepressants | 3 (4.9%) | 6 (5.8%) | p = 0.8 b |
| Antipsychotics | 1 (1.6%) | 4 (3.8%) | p = 0.4 b |
| Antiepileptics | 5 (8.2%) | 1 (1.0%) | p = 0.02 b |
| With DM (n = 104) | Without DM (n = 61) | p-Value | |
|---|---|---|---|
| Anthropometry | |||
| Body weight (kg) | 68.3 ± 13.6 | 62.0 ± 14.9 | p = 0.011 |
| Body height (m) | 164 ± 8 | 163 ± 9 | p = 0.4 |
| BMI (kg/m2) | 25.3 ± 3.9 | 23.3 ± 4.4 | p = 0.006 |
| WC (cm) | 91.8 ± 9.9 | 84.0 ± 12.5 | p < 0.001 |
| Glycemic profile | |||
| HbA1c (%) | 6.9 ± 1.1 | 5.5 ± 0.4 | p < 0.001 |
| Fasting glucose (mmol/L) | 6.4 ± 2.2 | 4.9 ± 0.6 | p < 0.001 |
| Fasting insulin (mIU/L) | 33.1 ± 44.3 | 13.5 ± 10.7 | p = 0.002 |
| C-peptide (ng/mL) | 8.4 ± 5.7 | 10.3 ± 8.8 | p = 0.1 |
| HOMA | 9.2 ± 12.4 | 2.9 ± 2.2 | p < 0.001 |
| microRNA level (fold) | |||
| miR-221 | |||
| Adipose | 1.13 ± 1.19 | 0.70 ± 0.85 | p = 0.02 |
| Plasma | 2.52 ± 1.20 | 3.25 ± 1.42 | p = 0.04 |
| miR-222 | |||
| Adipose | 1.90 ± 1.97 | 1.16 ± 1.29 | p = 0.01 |
| Plasma | 0.13 ± 0.06 | 0.18 ± 0.16 | p = 0.08 |
| (A) Anthropometry | |||||
|---|---|---|---|---|---|
| Baseline | At 12th Month (Change) | p-Value | At 24th Month (Change) | p-Value | |
| Body weight (kg) | 65.9 ± 14.4 | 66.9 ± 13.4(1.8 ± 5.1) | p < 0.001 | 66.8 ± 13.7(0.5 ± 4.7) | p = 0.3 |
| BMI (kg/m2) | 24.5 ± 4.2 | 24.9 ± 3.9(0.7 ± 1.9) | p < 0.001 | 25.1 ± 4.0(0.2 ± 1.9) | p = 0.3 |
| WC (cm) | 88.8 ± 11.6 | 91.4 ± 11.6(2.9 ± 5.8) | p < 0.001 | 92.7 ± 12.5(1.3 ± 4.0) | p = 0.002 |
| (B) Glycaemic Profile | |||||
| Baseline | At 12th Month (Change) | p-Value | At 24th Month (Change) | p-Value | |
| HbA1c (%) | 6.3 ± 1.1 | 6.2 ± 1.1 (−0.2 ± 0.9) | p = 0.04 | 6.2 ± 1.2(+0.1 ± 0.8) | p = 0.4 |
| Fasting glucose (mmol/L) | 5.8 ± 1.9 | 6.5 ± 1.9 (+0.7 ± 2.0) | p < 0.001 | 6.0 ± 1.6(−0.3 ± 2.1) | p = 0.1 |
| Fasting insulin (mIU/L) | 25.6 ± 36.6 | 43.1 ± 114.9 (+19.1 ± 89.4) | p = 0.02 | 32.8 ± 73.8(−16.4 ± 83.0) | p = 0.07 |
| C-peptide (ng/mL) | 9.1 ± 7.1 | 9.3 ± 5.1 (+0.3 ± 8.2) | p = 0.02 | 8.0 ± 4.0(−1.2 ± 4.6) | p = 0.7 |
| HOMA | 6.8 ± 10.2 | 12.1 ± 32.5 (+ 6.3 ± 27.2) | p = 0.02 | 9.2 ± 22.4(−4.4 ± 20.2) | p = 0.04 |
| (C) Insulin Requirements | |||||
| Total Daily Insulin Prescription (Units/Day) | Body Weight-Adjusted Daily Insulin Prescription (Units/kg/Day) | ||||
| Dosage | Change | Dosage | Change | p-Value | |
| Baseline | 7.78 ± 14.10 | 0.11 ± 0.20 | |||
| At 6th month | 11.05 ± 15.97 | +2.72 ± 10.85 | 0.15 ± 0.23 | +0.03 ± 0.15 | p = 0.006 |
| At 12th month | 11.76 ± 18.07 | +0.57 ± 7.75 | 0.15 ± 0.23 | −0.005 ± 0.09 | p = 0.5 |
| At 18th month | 11.61 ± 18.25 | −0.22 ± 8.56 | 0.15 ± 0.24 | +0.001 ± 0.12 | p = 0.9 |
| At 24th month | 11.00 ± 18.33 | −0.79 ± 10.27 | 0.13 ± 0.23 | −0.017 ± 0.12 | p = 0.1 |
| (A) Change in Anthropometry | ||||||
|---|---|---|---|---|---|---|
| BW Change at 12th Month | BMI Change at 12th Month | WC Change at 12th Month | ||||
| Beta (95% CI) | p-value | Beta (95% CI) | p-value | Beta (95% CI) | p-value | |
| Adipose miR-221 | 1.44 (0.31–2.57) | p = 0.01 | 0.56 (0.15–0.98) | p = 0.009 | 1.82 (0.57–3.07) | p = 0.005 |
| Adipose miR-222 | 1.35 (0.08–2.63) | p = 0.038 | ||||
| hsCRP | 0.15 (0.00–0.03) | p = 0.048 | ||||
| Baseline BMI | −0.12 (−0.22–−0.03) | p = 0.01 | ||||
| Albumin | 0.25 (0.02–0.47) | p = 0.03 | ||||
| Pre-existing DM | −2.35 (−4.69–−0.01) | p = 0.049 | ||||
| Dialysate dextrose load | 0.04 (0.01–0.07) | p = 0.003 | ||||
| Antidepressant use | −4.77 (−8.61–−0.94) | p = 0.015 | −1.89 (−3.29–−0.46) | p = 0.01 | ||
| (B) Change in Glycemic Profile | ||||||
| Plasma Insulin Change at 12th Month | HOMA Change at 12th Month | Insulin Requirement Change at 6th Month | ||||
| Beta (95% CI) | p-value | Beta (95% CI) | p-value | Beta (95% CI) | p-value | |
| Adipose miR-221 | 28.61 (10.73–46.50) | p = 0.002 | 8.16 (2.80–13.53) | p = 0.003 | 0.05 (0.006–0.09) | p = 0.02 |
| Adipose miR-222 | 21.61 (3.22–40.01) | p = 0.02 | 6.59 (1.13–12.05) | p = 0.018 | 0.06 (0.02–0.11) | p = 0.002 |
| Baseline HOMA | 5.91 (4.19–7.63) | p < 0.001 | 1.77 (1.26–2.28) | p < 0.001 | 0.008 (0.004–0.011) | p < 0.001 |
| Pre-existing DM | 0.19 (0.12–0.27) | p < 0.001 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, G.C.K.; Than, W.H.; Kwan, B.C.H.; Lai, K.B.; Chan, R.C.K.; Teoh, J.Y.C.; Ng, J.K.C.; Chow, K.M.; Cheng, P.M.S.; Law, M.C.; et al. Adipose and Plasma microRNAs miR-221 and 222 Associate with Obesity, Insulin Resistance, and New Onset Diabetes after Peritoneal Dialysis. Nutrients 2022, 14, 4889. https://doi.org/10.3390/nu14224889
Chan GCK, Than WH, Kwan BCH, Lai KB, Chan RCK, Teoh JYC, Ng JKC, Chow KM, Cheng PMS, Law MC, et al. Adipose and Plasma microRNAs miR-221 and 222 Associate with Obesity, Insulin Resistance, and New Onset Diabetes after Peritoneal Dialysis. Nutrients. 2022; 14(22):4889. https://doi.org/10.3390/nu14224889
Chicago/Turabian StyleChan, Gordon Chun Kau, Win Hlaing Than, Bonnie Ching Ha Kwan, Ka Bik Lai, Ronald Cheong Kin Chan, Jeremy Yuen Chun Teoh, Jack Kit Chung Ng, Kai Ming Chow, Phyllis Mei Shan Cheng, Man Ching Law, and et al. 2022. "Adipose and Plasma microRNAs miR-221 and 222 Associate with Obesity, Insulin Resistance, and New Onset Diabetes after Peritoneal Dialysis" Nutrients 14, no. 22: 4889. https://doi.org/10.3390/nu14224889