
A Town-Level Comprehensive Intervention Study to Reduce Salt Intake in China: Cluster Randomized Controlled Trial
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
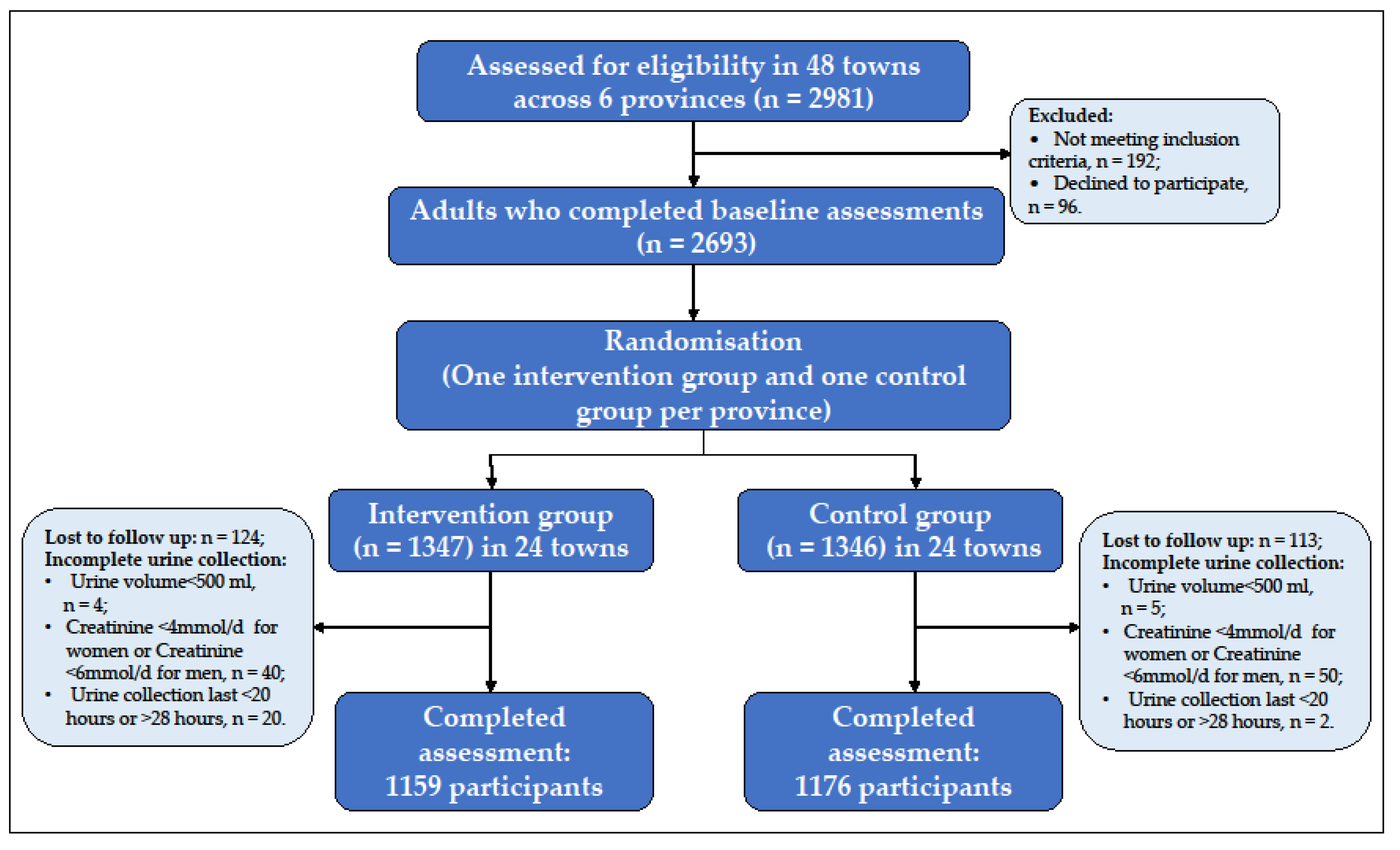
2.2. Study Participants
2.3. Randomization and Masking
2.4. Data Collection
2.5. Intervention
2.5.1. Salt Reduction Campaign
2.5.2. Salt Reduction Interventions in Primary Health Centers
2.5.3. Salt Reduction Interventions in Schools
2.5.4. Salt Reduction Interventions in Restaurants
2.6. Outcomes
2.7. Data Analysis
3. Results
3.1. Baseline Characteristics of Participants
3.2. Primary Outcome
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- He, F.J.; Macgregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Wang, C.; Liu, M.; Chen, Z.; Liu, S. Temporal and spatial trends of ischemic heart disease burden in Chinese and subgroup populations from 1990 to 2016: Data from the 2016 global burden of disease study. BMC Cardiovasc. Disord. 2020, 20, 243. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Tan, M.; Ma, Y.; MacGregor, G.A. Salt Reduction to Prevent Hypertension and Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 632–647. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Zhang, M.; Wu, J.; Zhang, X.; Hu, C.; Zhao, Z.; Li, C.; Huang, Z.; Zhou, M.; Wang, L. Prevalence and control of hypertension in adults in China, 2018. Chin. J. Epidemiol. 2021, 42, 1780–1789. [Google Scholar]
- He, F.J.; Gu, D.; Chen, J.; Wu, X.; Kelly, T.; Huang, J.-F.; Chen, J.-C.; Chen, C.-S.; Bazzano, L.A.; Reynolds, K.; et al. Premature deaths attributable to blood pressure in China: A prospective cohort study. Lancet 2009, 374, 1765–1772. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Noncommunicable Diseases 2014; World Health Organization: Geneva, Switzerland, 2015.
- Li, Y.; Zhang, P.; Wu, J.; Ma, J.; Xu, J.; Zhang, X.; Luo, R.; Liu, M.; Sun, Y.; Li, X.; et al. Twenty-Four-Hour Urinary Sodium and Potassium Excretion and Their Associations with Blood Pressure Among Adults in China: Baseline Survey of Action on Salt China. Hypertension 2020, 76, 1580–1588. [Google Scholar] [CrossRef]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S.; et al. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- Cobb, L.; Appel, L.; Anderson, C. Strategies to reduce dietary sodium intake. Curr. Treat. Options Cardiovasc. Med. 2012, 14, 425–434. [Google Scholar] [CrossRef] [Green Version]
- Trieu, K.; Neal, B.; Hawkes, C.; Dunford, E.; Campbell, N.R.C.; Rodriguez-Fernandez, R.; Legetic, B.; McLaren, L.; Barberio, A.; Webster, J. Salt reduction initiatives around the world-a systematic review of progress towards the global target. PLoS ONE 2015, 10, e0130247. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Wang, Y. Tracking of blood pressure from childhood to adulthood: A systematic review and meta-regression analysis. Circulation 2008, 117, 3171–3780. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Zhang, P.; Li, Y.; MacGregor, G.A. Action on salt China. Lancet 2018, 392, 7–9. [Google Scholar] [CrossRef]
- Zhang, P.; He, F.J.; Li, Y.; Li, C.; Wu, J.; Ma, J.; Zhang, B.; Wang, H.; Li, Y.; Hanbury, M.; et al. Reducing Salt Intake in China with “Action on Salt China” (ASC): Protocol for Campaigns and Randomized Controlled Trials. JMIR Res. Protoc. 2020, 9, e15933. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Zhang, P.; Luo, R.; Li, Y.; Sun, Y.; Chen, F.; Zhao, Y.; Zhao, W.; Li, D.; Chen, H.; et al. App based education programme to reduce salt intake (AppSalt) in schoolchildren and their families in China: Parallel, cluster randomized controlled trial. BMJ 2022, 376, e066982. [Google Scholar] [CrossRef]
- Xu, J.; Tang, B.; Liu, M.; Bai, Y.; Yan, W.; Zhou, X.; Xu, Z.; He, F.J.; Jin, D.; Sun, J.; et al. A town level comprehensive intervention study to reduce salt intake in China: Protocol for a cluster randomised controlled trial. BMJ Open 2020, 10, e032976. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Luo, R.; Li, Y.; He, F.J.; Tan, M.; MacGregor, G.A.; Lui, H.; Zhang, P. App-Based Salt Reduction Intervention in School Children and Their Families (AppSalt) in China: Protocol for a Mixed Method Process Evaluation. JMIR Res. Protoc. 2021, 10, e19430. [Google Scholar] [CrossRef]
- Zhang, X.; Hu, X.; Ma, J.; Zhang, P.; Li, Y.; Luo, R.; He, F.J.; MacGregor, G.A.; Wang, J.; Yin, Z. Cluster randomised controlled trial of home cook intervention to reduce salt intake in China: A protocol study. BMJ Open 2020, 10, e033842. [Google Scholar] [CrossRef]
- Du, W.; Zhang, J.; Li, Y.; He, F.J.; Zhou, X.; Xu, Z.; Gao, Y.; Yin, L.; Chang, X.; Yan, W.; et al. Restaurant interventions for salt reduction in China: Protocol for a randomised controlled trial. BMJ Open 2020, 10, e038744. [Google Scholar] [CrossRef]
- Zhang, J.; Sun, L.; Liu, Y.; Wang, H.; Sun, N.; Zhang, P. Mobile Device-Based electronic data capture system used in a clinical randomized controlled trial: Advantages and challenges. J. Med. Internet Res. 2017, 19, e6978. [Google Scholar] [CrossRef]
- He, F.J.; Wu, Y.; Feng, X.X.; Ma, J.; Ma, Y.; Wang, H.; Zhang, J.; Yuan, J.; Lin, C.-P.; Nowson, C.; et al. School based education programme to reduce salt intake in children and their families (School-EduSalt): Cluster randomised controlled trial. BMJ 2015, 350, h770. [Google Scholar] [CrossRef] [Green Version]
- McLean, R.M. Measuring population sodium intake: A review of methods. Nutrients 2014, 6, 4651–4662. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; He, F.J.; Wang, C.; MacGregor, G.A. Twenty-Four-Hour Urinary Sodium and Potassium Excretion in China: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2019, 8, e012923. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Li, F.; Harmer, P. Healthy China 2030: Moving from blueprint to action with a new focus on public health. Lancet Public Health 2019, 4, e447. [Google Scholar] [CrossRef] [Green Version]
- Xu, A.; Ma, J.; Guo, X.; Wang, L.; Wu, J.; Zhang, J.; Bai, Y.; Xu, J.; Lu, Z.; Xu, Z.; et al. Association of a Province-Wide Intervention With Salt Intake and Hypertension in Shandong Province, China, 2011–2016. JAMA Intern. Med. 2020, 180, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.G.; Guo, Z.Y.; Hu, G.; Yu, S.J.; Sun, W.; Pietinen, P.; Nissinen, A. Changes in sodium intake and blood pressure in a community-based intervention project in China. J. Hum. Hypertens. 1995, 9, 959–968. [Google Scholar] [PubMed]
- Lin, P.H.; Yancy, W.S., Jr.; Pollak, K.I.; Dolor, R.J.; Marcello, J.; Samsa, G.P.; Batch, B.C.; Svetkey, L.P. The influence of a physician and patient intervention program on dietary intake. J. Acad. Nutr. Diet. 2013, 113, 1465–1475. [Google Scholar] [CrossRef] [Green Version]
- Svetkey, L.P.; Pollak, K.I.; Yancy, W.S., Jr.; Dolor, R.J.; Batch, B.C.; Samsa, G.; Matchar, D.B.; Lin, P.H. Hypertension improvement project: Randomized trial of quality improvement for physicians and lifestyle modification for patients. Hypertension 2009, 54, 1226–1233. [Google Scholar] [CrossRef] [Green Version]
- Cappuccio, F.P.; Kerry, S.M.; Micah, F.B.; Plange-Rhule, J.; Eastwood, J.B. A community programme to reduce salt intake and blood pressure in Ghana (ISRCTN88789643]. BMC Public Health 2006, 6, 13. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Yan, L.L.; Niu, W.; Labarthe, D.; Feng, X.; Shi, J.; Zhang, J.; Zhang, R.; Zhang, Y.; Chu, H.; et al. A large-scale cluster randomized trial to determine the effects of community-based dietary sodium reduction—The China Rural Health Initiative Sodium Reduction Study. Am. Heart J. 2013, 166, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Bhana, N.; Utter, J.; Eyles, H. Knowledge, Attitudes and Behaviors Related to Dietary Salt Intake in High-Income Countries: A Systematic Review. Curr. Nutr. Rep. 2018, 7, 183–197. [Google Scholar] [CrossRef]
- Bi, Z.; Liang, X.; Xu, A.; Wang, L.; Shi, X.; Zhao, W.; Ma, J.; Guo, X.; Zhang, X.; Zhang, J.; et al. Hypertension Prevalence, Awareness, Treatment, and Control and Sodium Intake in Shandong Province, China: Baseline Results from Shandong–Ministry of Health Action on Salt Reduction and Hypertension (SMASH), 2011. Prev. Chronic Dis. 2014, 11, E88. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, J.; Shi, X.-M.; Liang, X.-F. A cross-sectional survey on the efficacy of ‘China Healthy Lifestyle for All’ in 2012. Chin. J. Epidemiol. 2013, 34, 869–873. (In Chinese) [Google Scholar]
- He, F.J.; MacGregor, G.A. Fortnightly review: Beneficial effects of potassium. BMJ 2001, 323, 497–501. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Nowson, C.A.; MacGregor, G.A. Fruit and vegetable consumption and stroke: Meta-analysis of cohort studies. Lancet 2006, 367, 320–326. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Control (n = 1347) | Intervention (n = 1346) | p-Value |
|---|---|---|---|
| Age (year), Mean (SD) | 47.2 (13.0) | 48.8 (12.6) | <0.001 |
| Men, n (%) | 667 (49.5) | 667 (49.6) | 0.98 |
| Weight (kg), Mean (SD) | 63.3 (12.1) | 63.1 (11.4) | 0.72 |
| BMI (kg/m2), Mean (SD) | 24.7 (3.7) | 24.8 (3.5) | 0.39 |
| Physical activity: active n (%) | 567 (42.1) | 519 (38.6) | 0.06 |
| Education status (n, %) | |||
| Primary education or less | 540 (40.1) | 596 (44.3) | 0.02 |
| Secondary school | 536 (39.8) | 503 (37.4) | |
| High school | 159 (11.8) | 161 (12.0) | |
| University or college | 112 (8.3) | 86 (6.4) | |
| Alcohol drinkers a (n, %) | 0.82 | ||
| Non-drinkers | 792 (58.8) | 800 (59.4) | |
| Occasional drinkers | 426 (31.7) | 415 (30.8) | |
| Regular drinkers | 128 (9.5) | 131 (9.7) | |
| Urine creatinine (mmol/24 h) | 10.7 (3.3) | 10.5 (3.5) | 0.13 |
| Self-reported hypertension b (n, %) | 233 (17.4) | 300 (22.3) | <0.001 |
| BP treatment in self-reported hypertensives, (n, %) c | 157 (66.8) | 247 (82.3) | <0.001 |
| Control | Intervention | Adjust Difference * (Intervention vs. Control) (95% CI) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline N, Mean (SD) | 12-Month N, Mean (SD) | Model-Based Change from Baseline * (95% CI) | Baseline N, Mean (SD) | 12-Month N, Mean (SD) | Model-Based Change from Baseline * (95% CI) | |||
| Salt intake (g/d) | 1327 | 1159 | −0.23 | 1315 | 1176 | −0.02 | 0.22 | 0.31 |
| 11.5 (4.8) | 11.3 (4.7) | (−0.53 to 0.06) | 11.1 (4.5) | 11.1 (4.8) | (−0.31 to 0.27) | (−0.20 to 0.64) | ||
| Urinary sodium (mmol/24 h) | 1327 | 1159 | −4.00 | 1315 | 1176 | −0.27 | 3.72 | 0.31 |
| 196.1 (81.3) | 192.6 (80.9) | (−9.06 to 1.07) | 189.7 (77.0) | 189.1 (82.4) | (−5.33 to 4.78) | (−3.43 to 10.87) | ||
| Urinary sodium (mg/24 h) | 1327 | 1159 | −91.99 | 1315 | 1176 4349.8 | −6.40 | 85.58 | 0.31 |
| 4510.6 (187.0) | 4430.9 (1860.8) | (−208.47 to 24.50) | 4363.0 (1770.9) | (1894.2) | (−122.63 to 109.83) | (−78.82 to 249.99) | ||
| Urinary potassium (mmol/24 h) | 1327 | 1159 | −1.65 | 1315 | 1176 | 0.53 | 2.18 | 0.004 |
| 40.6 (16.8) | 39.0 (15.1) | (−2.70 to −0.61) | 39.6 (16.3) | 40.3 (16.3) | (−0.52 to 1.57) | (0.70 to 3.66) | ||
| Urinary potassium (mg/24 h) | 1327 | 1159 1519.9 | −64.45 | 1315 | 1176 | 20.58 | 85.03 | 0.004 |
| 1584.6 (654.0) | (589.4) | (−105.30 to −23.60) | 1546.2 (637.0) | 1573.4 (634.6) | (−20.18 to 61.34) | (27.38 to 142.68) | ||
| sodium-to-potassium ratio | 1327 | 1159 | 0.09 | 1315 | 1176 | −0.07 | −0.17 | 0.11 |
| 5.2 (2.3) | 5.3 (2.3) | (−0.05 to 0.24) | 5.1 (2.1) | 5.0 (2.2) | (−0.22 to 0.07) | (−0.37 to−0.04) | ||
| Systolic blood pressure (mm Hg) | 1347 | 1242 | 0.71 | 1346 | 1231 | −2.24 | −2.95 | <0.001 |
| 125.6 (19.3) | 128.0 (20.0) | (−0.21 to 1.64) | 127.2 (19.3) | 126.8 (18.8) | (−3.21 to −1.27) | (−4.08 to −1.83) | ||
| Diastolic blood pressure (mm Hg) | 1347 | 1242 | −0.89 | 1346 | 1231 | −1.34 | −0.45 | 0.22 |
| 79.0 (11.8) | 79.1 (12.3) | (−1.49 to −0.29) | 80.1 (11.4) | 80.0 (11.5) | (−1.97 to −0.71) | (−1.17 to 0.27) | ||
| Urinary creatinine (mmol/24 h) | 1327 | 1159 | −0.57 | 1315 | 1176 | −0.27 | 0.30 | 0.01 |
| 10.8 (3.2) | 10.1 (3.2) | (−0.74 to −0.41) | 10.6 (3.4) | 10.3 (3.4) | (−0.44 to −0.11) | (0.06 to 0.53) | ||
| Urine volume (mL/24 h) | 1327 | 1159 | −43.01 | 1315 | 1176 | 78.55 | 121.57 | <0.001 |
| 1608.3 (643.0) | 1565.7 (631.1) | (−79.71 to −6.32) | 1623.2 (652.4) | 1711.9 (699.2) | (41.95 to 115.16) | (66.79 to 173.34) | ||
| Control | Intervention | Intervention Effect * (Intervention Group vs. Control Group, OR, 95% CI) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline n (%) | 12-Month n (%) | Model-Based Change (OR, 95% CI) | Baseline n (%) | 12-Month n (%) | Model-Based Change (OR, 95% CI) | |||
| Knowledge | ||||||||
| Knowledge of the salt intake recommended by the Chinese nutrition guidelines (6 g/d) | 330 | 375 | 1.38 | 233 | 889 | 12.99 | 9.43 (7.28,12.21) | <0.001 |
| (24.5) | (30.4) | (1.16, 1.64) | (17.3) | (71.6) | (10.73, 15.72) | |||
| Having heard about a low-sodium salt substitute | 342 | 458 | 1.81 | 371 | 725 | 3.99 | 2.20 (1.73, 2.80) | <0.001 |
| (25.4) | (37.1) | (1.52, 2.15) | (27.6) | (58.4) | (3.37, 4.72) | |||
| Having the ability to identify salt content on a food label | 577 | 505 | 0.97 | 504 | 784 | 3.40 | 3.50 (2.76, 4.43) | <0.001 |
| (42.8) | (40.9) | (0.83, 1.15) | (37.4) | (63.2) | (2.87, 4.03) | |||
| Attitude | ||||||||
| Willingness to choose a low-sodium diet | 1075 | 991 | 1.02 | 1067 | 1099 | 2.03 | 1.99 (1.48, 2.66) | <0.001 |
| (79.8) | (80.3) | (0.84, 1.24) | (79.3) | (88.6) | (1.63, 2.53) | |||
| Preferring a less salty taste | 380 | 372 | 1.08 | 366 | 369 | 1.12 | 1.04 (0.81, 1.32) | 0.77 |
| (28.2) | (30.2) | (0.91, 1.28) | (27.2) | (29.7) | (0.94, 1.33) | |||
| Behaviors | ||||||||
| Using a low-sodium salt substitute a | 109 | 133 | 0.91 | 130 | 239 | 1.01 | 1.11 (0.74, 1.67) | 0.62 |
| (31.9) | (29.0) | (0.67, 1.24) | (35.0) | (33.0) | (0.77, 1.32) | |||
| Eating processed food once per week or less | 746 | 714 | 1.10 | 788 | 814 | 1.34 | 1.22 (0.97, 1.52) | 0.09 |
| (55.4) | (57.9) | (0.94, 1.29) | (58.5) | (65.6) | (1.14, 1.58) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, M.; Xu, J.; Li, Y.; He, F.J.; Zhang, P.; Song, J.; Gao, Y.; Yan, S.; Yan, W.; Jin, D.; et al. A Town-Level Comprehensive Intervention Study to Reduce Salt Intake in China: Cluster Randomized Controlled Trial. Nutrients 2022, 14, 4698. https://doi.org/10.3390/nu14214698
Liu M, Xu J, Li Y, He FJ, Zhang P, Song J, Gao Y, Yan S, Yan W, Jin D, et al. A Town-Level Comprehensive Intervention Study to Reduce Salt Intake in China: Cluster Randomized Controlled Trial. Nutrients. 2022; 14(21):4698. https://doi.org/10.3390/nu14214698
Chicago/Turabian StyleLiu, Min, Jianwei Xu, Yuan Li, Feng J He, Puhong Zhang, Jing Song, Yifu Gao, Shichun Yan, Wei Yan, Donghui Jin, and et al. 2022. "A Town-Level Comprehensive Intervention Study to Reduce Salt Intake in China: Cluster Randomized Controlled Trial" Nutrients 14, no. 21: 4698. https://doi.org/10.3390/nu14214698