
Comparison of Adherence to Mediterranean Diet between Spanish and German School-Children and Influence of Gender, Overweight, and Physical Activity
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Anthropometrics
2.2. Questionnaires
2.3. Accelerometers
2.4. Statistics
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Study Registration
References
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: Web Annex: Evidence Profiles; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Lehmann, F.; Varnaccia, G.; Zeiher, J.; Lange, C.; Jordan, S. Influencing factors of obesity in school-age children and adolescents—A systematic review of the literature in the context of obesity monitoring. J. Health Monit. 2020, 5, 2–23. [Google Scholar] [PubMed]
- Moradell, A.; Santaliestra-Pasías, A.M.; Aparicio-Ugarriza, R.; Huybrechts, I.; Bertalanné Szommer, A.; Forsner, M.; González-Gross, M.; Kafatos, A.; Androutsos, O.; Michels, N.; et al. Are Physical Activity and Sedentary Screen Time Levels Associated with Food Consumption in European Adolescents? HELENA Study 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Brettschneider, A.; Barbosa, C.L.; Haftenberger, M.; Lehmann, F.; Mensink, G.B. Adherence to food-based dietary guidelines among adolescents in Germany according to socio-economic status and region: Results from Eating Study as a KiGGS Module (EsKiMo) II. Public Health Nutr. 2021, 24, 1216–1228. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (accessed on 27 July 2022).
- Neufeld, L.M.; Hendriks, S.; Hugas, M. Healthy Diet: A Definition for the United Nations Food Systems Summit 2021; Real Academia de Ingeniería: Madrid, Spain, 2021; ISBN 978-84-95662-77-4. [Google Scholar]
- Cena, H.; Calder, P.C. Defining a healthy diet: Evidence for the role of contemporary dietary patterns in health and disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Donini, L.M.; Serra-Majem, L.; Bulló, M.; Gil, Á.; Salas-Salvadó, J. The Mediterranean diet: Culture, health and science. Br. J. Nutr. 2015, 113, S1–S3. [Google Scholar] [CrossRef] [Green Version]
- Aguilera, E.; Piñero, P.; Infante Amate, J.; González de Molina, M.; Lassaletta, L.; Sanz Cobeña, A. Emisiones de Gases de Efecto Invernadero en el Sistema Agroalimentario y Huella de Carbono de la Alimentación en España; Real Academia de Ingeniería: Madrid, Spain, 2020. [Google Scholar]
- Obeid, C.A.; Gubbels, J.S.; Jaalouk, D.; Kremers, S.P.; Oenema, A. Adherence to the Mediterranean diet among adults in Mediterranean countries: A systematic literature review. Eur. J. Nutr. 2022, 61, 3327–3344. [Google Scholar] [CrossRef]
- Cabrera, S.G.; Fernández, N.H.; Hernández, C.R.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. KIDMED test; prevalence of low adherence to the Mediterranean Diet in children and young; a systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Rakhra, V.; Galappaththy, S.L.; Bulchandani, S.; Cabandugama, P.K. Obesity and the Western Diet: How We Got Here. Mo. Med. 2020, 117, 536–538. [Google Scholar]
- Cristi-Montero, C.; Chillón, P.; Labayen, I.; Casajus, J.A.; Gonzalez-Gross, M.; Vanhelst, J.; Manios, Y.; Moreno, L.A.; Ortega, F.B.; Ruiz, J.R. Cardiometabolic risk through an integrative classification combining physical activity and sedentary behavior in European adolescents: HELENA study. J. Sport Health Sci. 2019, 8, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Cruz, J.; Jiménez-Moleón, J.J.; Fernández-Quesada, F.; Sánchez, M.J. Prevalence of child and youth obesity in Spain in 2012. Rev. Española Cardiol. (Engl. Ed.) 2013, 66, 371–376. [Google Scholar] [CrossRef]
- Schienkiewitz, A.; Brettschneider, A.; Damerow, S.; Rosario, A.S. Übergewicht und Adipositas im Kindes-und Jugendalter in Deutschland–Querschnittergebnisse aus KiGGS Welle 2 und Trends. J. Health Monit. 2018, 3. [Google Scholar]
- Börnhorst, C.; Consortia, O.B.O.T.I.A.T.I.; Huybrechts, I.; Hebestreit, A.; Krogh, V.; De Decker, A.; Barba, G.; Moreno, L.A.; Lissner, L.; Tornaritis, M.; Molnár, D.; et al. Usual energy and macronutrient intakes in 2–9-year-old European children. Int. J. Obes. 2014, 38, S115–S123. [Google Scholar] [CrossRef] [Green Version]
- Svensson, A.; Larsson, C.; Eiben, G.; Lanfer, A.; Pala, V.; Hebestreit, A.; Huybrechts, I.; Fernández-Alvira, J.M.; Russo, P.; Koni, A.C.; et al. European children’s sugar intake on weekdays versus weekends: The IDEFICS study. Eur. J. Clin. Nutr. 2014, 68, 822–828. [Google Scholar] [CrossRef]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adoles-cents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef]
- Mendez, M.A.; Popkin, B.M.; Jakszyn, P.; Berenguer, A.; Tormo, M.J.; Sanchéz, M.J.; Quirós, J.R.; Pera, G.; Navarro, C.; Martinez, C.; et al. Adherence to a Mediterranean diet is associ-ated with reduced 3-year incidence of obesity. J. Nutr. 2006, 136, 2934–2938. [Google Scholar] [CrossRef] [Green Version]
- Finicelli, M.; Di Salle, A.; Galderisi, U.; Peluso, G. The Mediterranean Diet: An Update of the Clinical Trials. Nutrients 2022, 14, 2956. [Google Scholar] [CrossRef]
- Memaran, N.; Schwalba, M.; Borchert-Mörlins, B.; von der Born, J.; Markefke, S.; Bauer, E.; von Wick, A.; Epping, J.; von Maltzahn, N.; Heyn-Schmidt, I.; et al. Gesundheit und Fitness von deutschen Schulkindern. Ergeb. Physiol. 2020, 168, 597–607. [Google Scholar] [CrossRef] [Green Version]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; De Ridder, H. International society for the advancement of kinanthropometry: International standards for anthropometric assessment. Int. Soc. Adv. Kinanthropometry 2011, 115. [Google Scholar]
- Neuhauser, H.; Schienkiewitz, A.; Rosario, A.S.; Dortschy, R.; Kurth, B. Referenzperzentile für Anthropometrische Maßzahlen und Blutdruck aus der Studie zur Gesundheit von Kindern und Jugendlichen in Deutschland (KiGGS); Robert Koch-Institut: Berlin, Germany, 2013. [Google Scholar]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; Von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den Body-mass-Index für das Kindes-und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Mon. Kinderheilkd. 2001, 149, 807–818. [Google Scholar] [CrossRef] [Green Version]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar]
- Rei, M.; Severo, M.; Rodrigues, S. Reproducibility and validity of the Mediterranean Diet Quality Index (KIDMED Index) in a sample of Portuguese adolescents. Br. J. Nutr. 2021, 126, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Norte Navarro, A.I.; Ortiz Moncada, R. Calidad de la dieta española según el índice de alimentación saludable. Nutr. Hosp. 2011, 26, 330–336. [Google Scholar] [PubMed]
- Aranceta-Bartrina, J.; Partearroyo, T.; López-Sobaler, A.M.; Ortega, R.M.; Varela-Moreiras, G.; Serra-Majem, L.; Pérez-Rodrigo, C. Updating the food-based dietary guidelines for the Spanish population: The Spanish society of community nutrition (senc) proposal. Nutrients 2019, 11, 2675. [Google Scholar] [CrossRef]
- Robusto, K.M.; Trost, S.G. Comparison of three generations of ActiGraph™ activity monitors in children and adolescents. J. Sports Sci. 2012, 30, 1429–1435. [Google Scholar] [CrossRef]
- Vanhelst, J.; Béghin, L.; Salleron, J.; Ruiz, J.R.; Ortega, F.B.; Ottevaere, C.; Molnar, D.; Kafatos, A.; Manios, Y.; Widhalm, K.; et al. Impact of the choice of threshold on physical activity patterns in free living conditions among adolescents measured using a uniaxial accelerometer: The HELENA study. J. Sports Sci. 2014, 32, 110–115. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Ortega, F.B.; Martinez-Gomez, D.; Labayen, I.; Moreno, L.A.; De Bourdeaudhuij, I.; Manios, Y.; Gonzalez-Gross, M.; Mauro, B.; Molnar, D.; et al. Objectively measured physical activity and sedentary time in European adolescents: The HELENA study. Am. J. Epidemiol. 2011, 174, 173–184. [Google Scholar] [CrossRef] [Green Version]
- Chandler, J.; Brazendale, K.; Beets, M.; Mealing, B. Classification of physical activity intensities using a wrist-worn accelerome-ter in 8–12-year-old children. Pediatr. Obes. 2016, 11, 120–127. [Google Scholar] [CrossRef]
- Farajian, P.; Risvas, G.; Karasouli, K.; Pounis, G.D.; Kastorini, C.M.; Panagiotakos, D.B.; Zampelas, A. Very high childhood obesity preva-lence and low adherence rates to the Mediterranean diet in Greek children: The GRECO study. Atherosclerosis 2011, 217, 525–530. [Google Scholar] [CrossRef]
- López-Gil, J.F.; Brazo-Sayavera, J.; García-Hermoso, A.; Yuste Lucas, J.L. Adherence to Mediterranean Diet related with physical fitness and physical activity in schoolchildren aged 6–13. Nutrients 2020, 12, 567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattavelli, E.; Olmastroni, E.; Bonofiglio, D.; Catapano, A.L.; Baragetti, A.; Magni, P. Adherence to the Mediterranean Diet: Impact of Geographical Location of the Observations. Nutrients 2022, 14, 2040. [Google Scholar] [CrossRef] [PubMed]
- Mariscal-Arcas, M.; Rivas, A.; Velasco, J.; Ortega, M.; Caballero, A.M.; Olea-Serrano, F. Evaluation of the Mediterranean Diet Qual-ity Index (KIDMED) in children and adolescents in Southern Spain. Public Health Nutr. 2009, 12, 1408–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- del Mar Bibiloni, M.; Martínez, E.; Llull, R.; Pons, A.; Tur, J.A. Western and Mediterranean dietary patterns among Balearic Is-lands’ adolescents: Socio-economic and lifestyle determinants. Public Health Nutr. 2012, 15, 683–692. [Google Scholar] [CrossRef] [Green Version]
- Sjöberg, A.; Hallberg, L.; Höglund, D.; Hulthen, L. Meal pattern, food choice, nutrient intake and lifestyle factors in The Göte-borg Adolescence Study. Eur. J. Clin. Nutr. 2003, 57, 1569–1578. [Google Scholar] [CrossRef]
- del Mar Bibiloni, M.; Martinez, E.; Llull, R.; Juarez, M.D.; Pons, A.; Tur, J.A. Prevalence and risk factors for obesity in Balearic Is-lands adolescents. Br. J. Nutr. 2010, 103, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Hoyland, A.; Dye, L.; Lawton, C.L. A systematic review of the effect of breakfast on the cognitive performance of children and adolescents. Nutr. Res. Rev. 2009, 22, 220–243. [Google Scholar] [CrossRef] [Green Version]
- Forkert, E.C.O.; De Moraes, A.C.F.; Carvalho, H.B.; Manios, Y.; Widhalm, K.; González-Gross, M.; Gutierrez, A.; Kafatos, A.; Censi, L.; De Henauw, S.; et al. Skipping breakfast is associated with adiposity markers especially when sleep time is adequate in adolescents. Sci. Rep. 2019, 9, 6380. [Google Scholar] [CrossRef] [Green Version]
- George, E.S.; Gavrili, S.; Itsiopoulos, C.; Manios, Y.; Moschonis, G. Poor adherence to the Mediterranean diet is associated with increased likelihood of metabolic syndrome components in children: The Healthy Growth Study. Public Health Nutr. 2021, 24, 2823–2833. [Google Scholar] [CrossRef]
- Flieh, S.M.; Moreno, L.A.; Miguel-Berges, M.L.; Stehle, P.; Marcos, A.; Molnár, D.; Widhalm, K.; Béghin, L.; De Henauw, S.; Kafatos, A.; et al. Free sugar consumption and obesity in Eu-ropean adolescents: The HELENA study. Nutrients 2020, 12, 3747. [Google Scholar] [CrossRef]
- Latasa, P.; Louzada, M.; Martinez Steele, E.; Monteiro, C. Added sugars and ultra-processed foods in Spanish households (1990–2010). Eur. J. Clin. Nutr. 2018, 72, 1404–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeedi, P.; Haszard, J.; Stoner, L.; Skeaff, S.; Black, K.E.; Davison, B.; Harrex, H.; Meredith-Jones, K.; Quigg, R.; Wong, J.E.; et al. Relationships between Dietary Patterns and Indices of Arterial Stiffness and Central Arterial Wave Reflection in 9–11-Year-Old Children. Children 2020, 7, 66. [Google Scholar] [CrossRef] [PubMed]
- Hebestreit, A.; Börnhorst, C.; Barba, G.; Siani, A.; Huybrechts, I.; Tognon, G.; Eiben, G.; Moreno, L.A.; Fernández Alvira, J.M.; Loit, H.M.; et al. Associations between energy intake, daily food intake and energy density of foods and BMI z-score in 2–9-year-old European children. Eur. J. Nutr. 2014, 53, 673–681. [Google Scholar] [CrossRef] [Green Version]
- Spengler, S.; Woll, A. The more physically active, the healthier? The relationship between physical activity and health-related quality of life in adolescents: The MoMo study. J. Phys. Act. Health 2013, 10, 708–715. [Google Scholar] [CrossRef]
- Bellisle, F. Food choice, appetite and physical activity. Public Health Nutr. 1999, 2, 357–361. [Google Scholar] [CrossRef]
- Lazarou, C.; Panagiotakos, D.B.; Matalas, A. Physical activity mediates the protective effect of the Mediterranean diet on chil-dren’s obesity status: The CYKIDS study. Nutrition 2010, 26, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Manz, K.; Mensink, G.B.M.; Finger, J.D.; Haftenberger, M.; Brettschneider, A.-K.; Barbosa, C.L.; Krug, S.; Schienkiewitz, A. Associations between physical activity and food intake among children and adolescents: Results of KiGGS Wave 2. Nutrients 2019, 11, 1060. [Google Scholar] [CrossRef] [Green Version]
- Ottevaere, C.; Huybrechts, I.; Cuenca-Garcia, M.; De Bourdeaudhuij, I.; Gottrand, F.; Kafatos, A.; Le Donne, C.; Moreno, L.A.; Widhalm, K.; De Henauw, S.; et al. Relationship between self-reported dietary intake and physical activity levels among adolescents: The HELENA study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Kriemler, S.; Meyer, U.; Martin, E.; van Sluijs, E.M.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: A review of reviews and systematic update. Br. J. Sports Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [Green Version]
- Vanhelst, J.; Beghin, L.; Duhamel, A.; De Henauw, S.; Molnar, D.; Vicente-Rodriguez, G.; Manios, Y.; Widhalm, K.; Kersting, M.; Polito, A.; et al. Relationship between school rhythm and physical activity in adolescents: The HELENA study. J. Sports Sci. 2017, 35, 1666–1673. [Google Scholar]
- Bachner, J.; Sturm, D.J.; Demetriou, Y. Accelerometer-measured physical activity and sedentary behavior levels and patterns in female sixth graders: The CReActivity Project. Int. J. Environ. Res. Public Health 2021, 18, 32. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
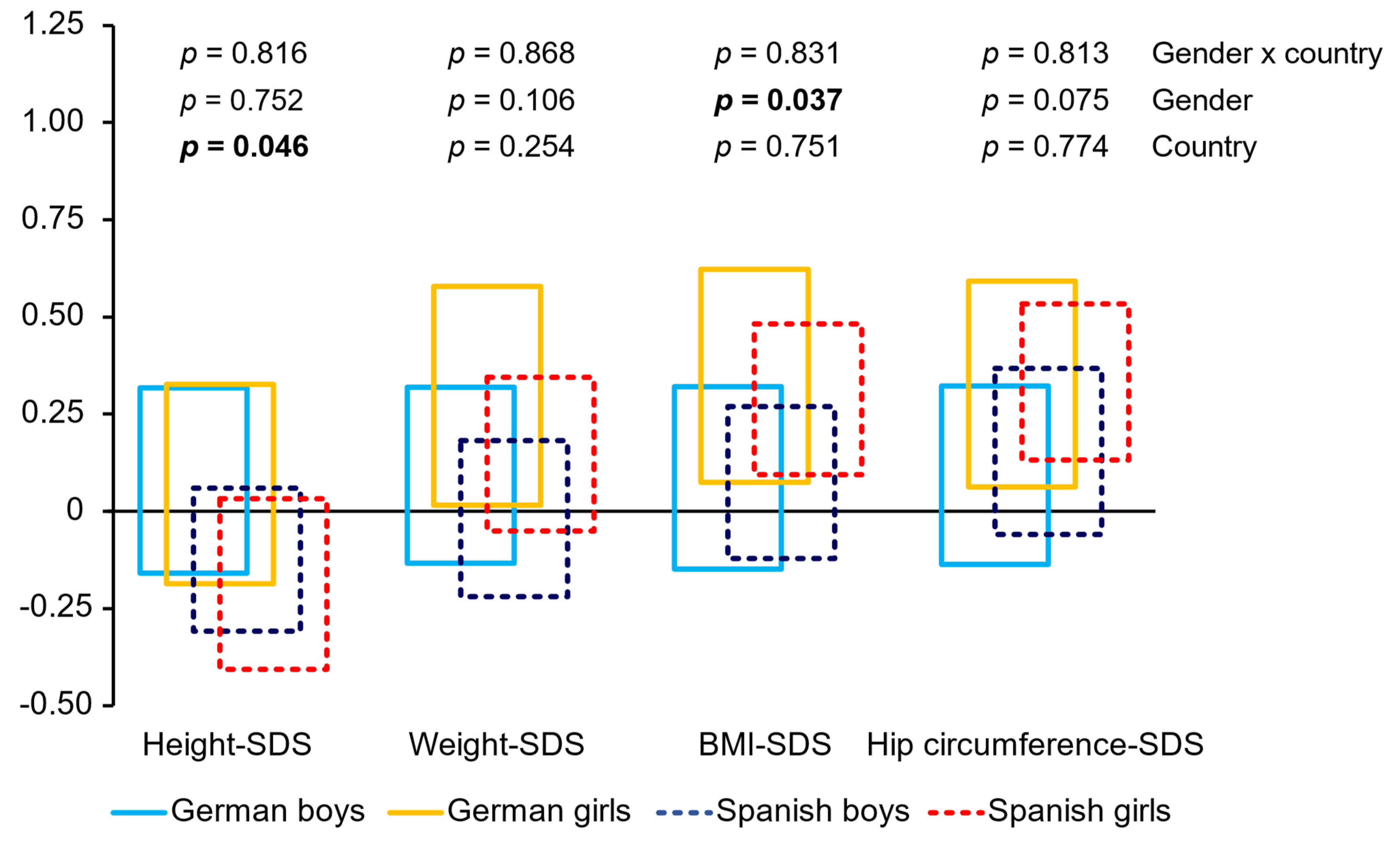
| Germany | Spain | Gender | Country | Gender × Country | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Boys | Girls | Total | Boys | Girls | p | η2 | p | η2 | p | η2 | |
| N | 152 | 82 | 70 | 182 | 86 | 96 | ||||||
| Age (years) | 11.4 ± 0.6 | 11.5 ± 0.6 | 11.3 ± 0.6 | 11.4 ± 0.6 | 11.4 ± 0.7 | 11.5 ± 0.6 | 0.583 | <0.01 | 0.908 | <0.01 | 0.025 | 0.02 |
| Height (m) | 1.50 ± 0.08 | 1.50 ± 0.08 | 1.50 ± 0.08 | 1.49 ± 0.08 | 1.48 ± 0.08 | 1.50 ± 0.08 | 0.319 | <0.01 | 0.076 | 0.01 | 0.335 | <0.01 |
| Weight (kg) | 45.6 ± 12.5 | 44.3 ± 11.6 | 47.0 ± 13.4 | 43.9 ± 11.7 | 42.2 ± 11.4 | 45.4 ± 11.7 | 0.027 | 0.01 | 0.157 | 0.01 | 0.855 | <0.01 |
| BMI (kg/m2) | 20.0 ± 4.3 | 19.5 ± 4.0 | 20.5 ± 4.5 | 19.6 ± 3.9 | 19.1 ± 3.8 | 20.1 ± 3.9 | 0.022 | 0.02 | 0.363 | <0.01 | 0.941 | <0.01 |
| Hip circumference (cm) | 82.1 ± 10.2 | 80.3 ± 9.5 | 84.2 ± 10.7 | 82.1 ± 9.2 | 79.8 ± 8.9 | 84.2 ± 9.0 | <0.001 | 0.05 | 0.778 | <0.01 | 0.844 | <0.01 |
| Germany | Spain | |||||||
|---|---|---|---|---|---|---|---|---|
| PA Level | PA Level | |||||||
| Low | Medium | High | p | Low | Medium | High | p | |
| Boys (n) | 25 | 18 | 16 | 0.091 | 18 | 28 | 40 | <0.001 |
| 42.4% | 30.5% | 27.1% | 20.9% | 32.6% | 46.5% | |||
| Girls (n) | 15 | 22 | 25 | 43 | 32 | 21 | ||
| 24.2% | 35.5% | 40.3% | 44.8% | 33.3% | 21.9% | |||
| Normal weight (n) | 32 | 33 | 31 | 0.740 | 49 | 54 | 59 | 0.014 |
| 33.3% | 34.4% | 32.3% | 30.2% | 33.3% | 36.4% | |||
| Overweight (n) | 8 | 7 | 10 | 12 | 6 | 2 | ||
| 32.0% | 28.0% | 40.0% | 60.0% | 30.0% | 10.0% | |||
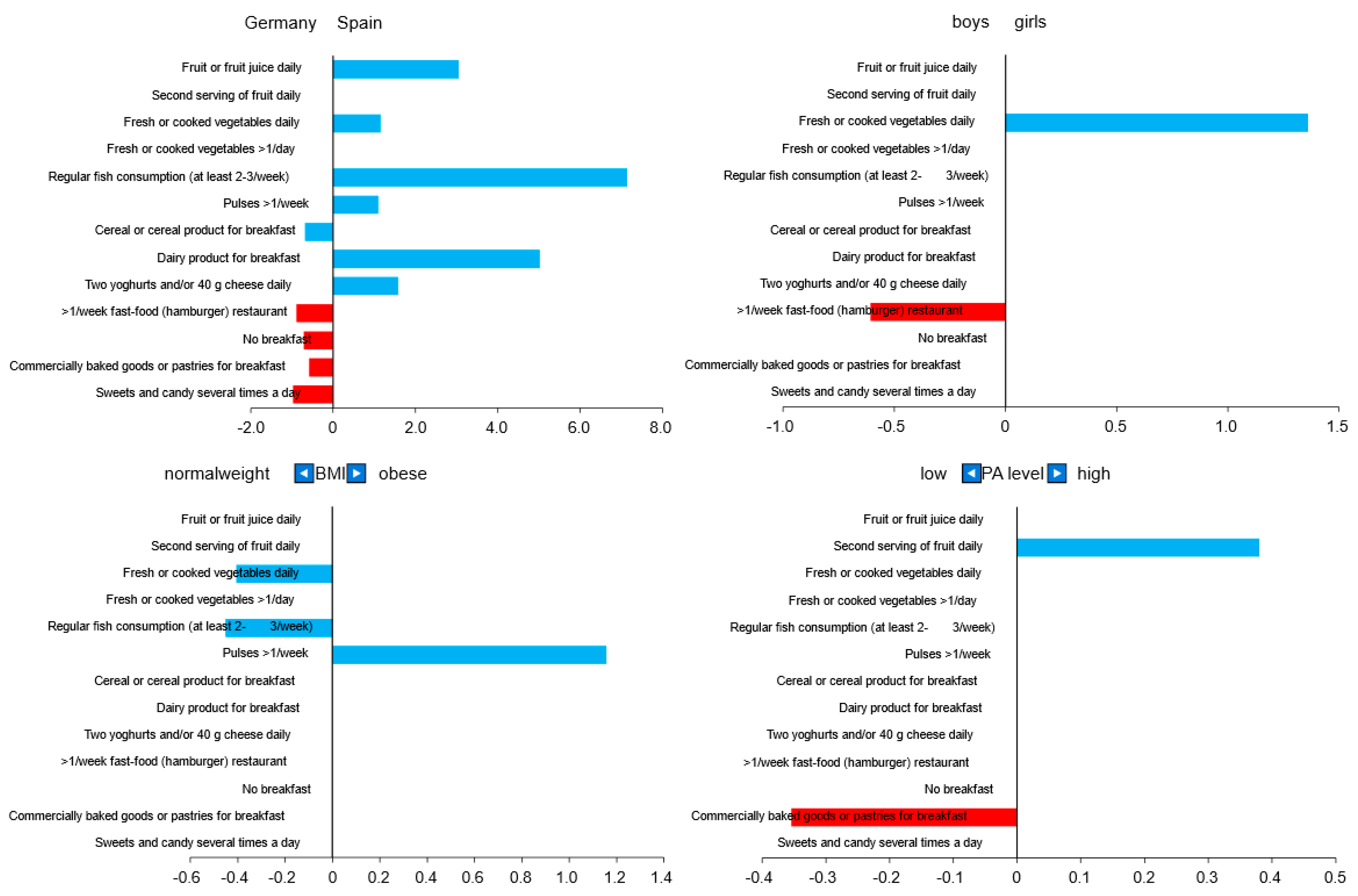
| Germany (%) | Spain (%) | p | |
|---|---|---|---|
| Fruit or fruit juice daily | 70.2 | 91.2 | <0.001 |
| Second serving of fruit daily | 57.0 | 67.0 | 0.062 |
| Fresh or cooked vegetables daily | 56.7 | 75.3 | <0.001 |
| Fresh or cooked vegetables > 1/day | 31.3 | 33.0 | 0.751 |
| Regular fish consumption (at least 2–3/week) | 34.9 | 81.3 | <0.001 |
| >1/week fast-food (hamburger) restaurant | 53.0 | 12.1 | <0.001 |
| Pulses > 1/week | 71.5 | 81.3 | 0.035 |
| Cereal or cereal product for breakfast | 92.0 | 81.9 | 0.007 |
| No breakfast | 45.7 | 18.1 | <0.001 |
| Dairy product for breakfast | 80.7 | 95.6 | <0.001 |
| Commercially baked goods or pastries for breakfast | 44.7 | 27.5 | 0.001 |
| Two yoghurts and/or 40 g cheese daily | 49.3 | 69.2 | <0.001 |
| Sweets and candy several times a day | 52.7 | 3.3 | <0.001 |
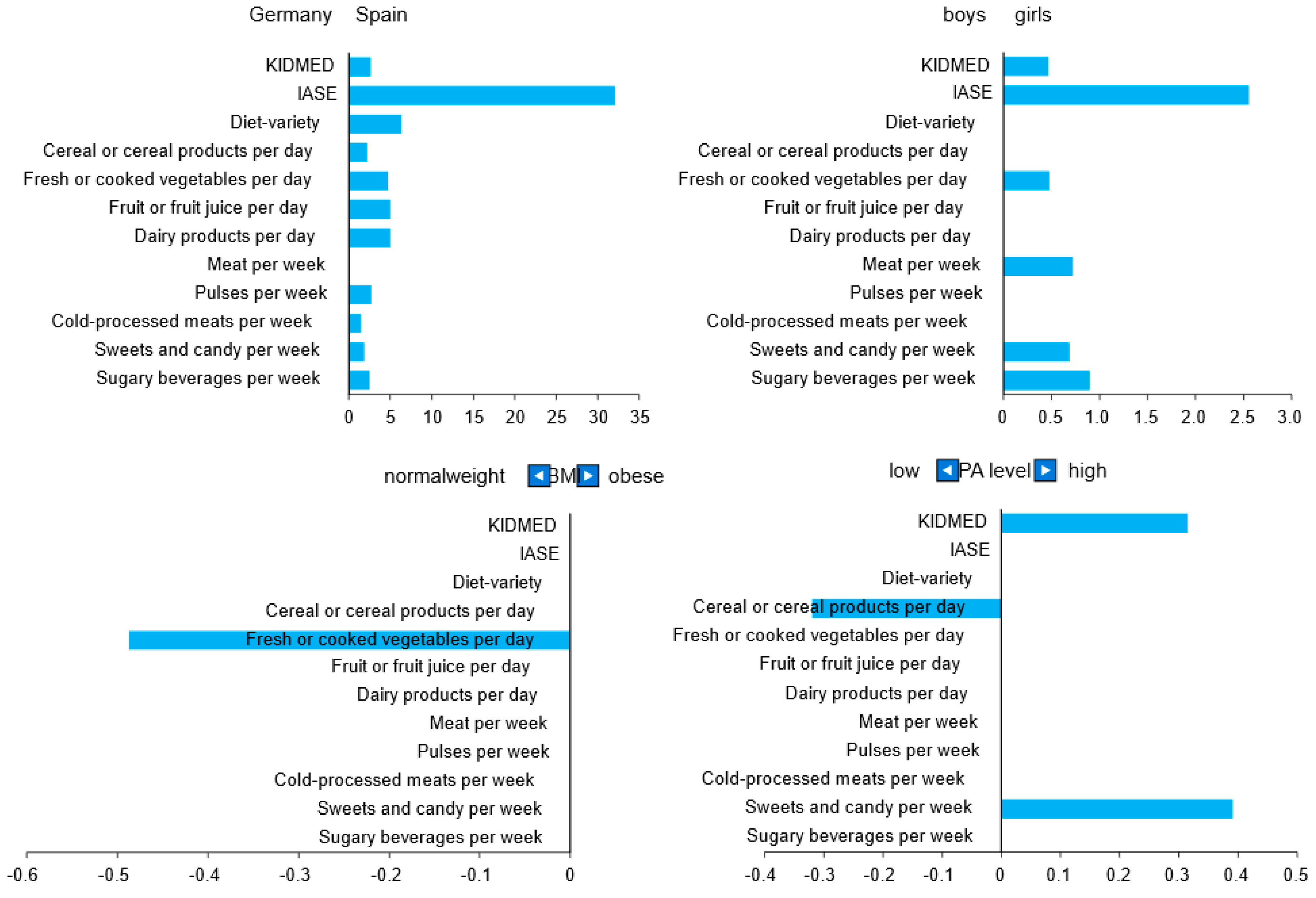
| Germany | Spain | |||||
|---|---|---|---|---|---|---|
| Mean ± SD | n | Mean ± SD | n | p | Hedges’ g | |
| IASE | 4 6.0 ± 10.0 | 144 | 78.3 ± 7.9 | 180 | <0.001 | −3.62 |
| Cereal or cereal products per day | 7.33 ± 2.43 | 149 | 9.55 ± 1.79 | 182 | <0.001 | −1.05 |
| Fresh or cooked vegetables per day | 4.17 ± 1.82 | 150 | 9.00 ± 1.87 | 182 | <0.001 | −2.60 |
| Fruit or fruit juice per day | 4.65 ± 1.81 | 150 | 9.67 ± 1.13 | 182 | <0.001 | −3.40 |
| Dairy products per day | 5.03 ± 2.51 | 150 | 9.92 ± 0.52 | 182 | <0.001 | −2.82 |
| Meat per week | 7.26 ± 2.74 | 146 | 7.73 ± 2.39 | 182 | 0.185 | −0.18 |
| Pulses per week | 5.61 ± 3.97 | 148 | 8.41 ± 2.24 | 181 | <0.001 | −0.89 |
| Cold-processed meats per week | 3.30 ± 3.08 | 147 | 4.86 ± 2.56 | 181 | <0.001 | −0.56 |
| Sweets and candy per week | 3.12 ± 2.65 | 149 | 5.07 ± 2.19 | 182 | <0.001 | −0.81 |
| Sugary beverages per week | 3.74 ± 3.15 | 149 | 6.16 ± 2.73 | 181 | <0.001 | −0.82 |
| Diet-variety | 1.55 ± 1.44 | 152 | 7.96 ± 1.60 | 182 | <0.001 | −4.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grams, L.; Nelius, A.-K.; Pastor, G.G.; Sillero-Quintana, M.; Veiga, Ó.L.; Homeyer, D.; Kück, M. Comparison of Adherence to Mediterranean Diet between Spanish and German School-Children and Influence of Gender, Overweight, and Physical Activity. Nutrients 2022, 14, 4697. https://doi.org/10.3390/nu14214697
Grams L, Nelius A-K, Pastor GG, Sillero-Quintana M, Veiga ÓL, Homeyer D, Kück M. Comparison of Adherence to Mediterranean Diet between Spanish and German School-Children and Influence of Gender, Overweight, and Physical Activity. Nutrients. 2022; 14(21):4697. https://doi.org/10.3390/nu14214697
Chicago/Turabian StyleGrams, Lena, Anne-Katrin Nelius, Guadalupe Garrido Pastor, Manuel Sillero-Quintana, Óscar L. Veiga, Denise Homeyer, and Momme Kück. 2022. "Comparison of Adherence to Mediterranean Diet between Spanish and German School-Children and Influence of Gender, Overweight, and Physical Activity" Nutrients 14, no. 21: 4697. https://doi.org/10.3390/nu14214697