
Multidisciplinary Prehabilitation and Postoperative Rehabilitation for Avoiding Complications in Patients Undergoing Resection of Colon Cancer: Rationale, Design, and Methodology of the ONCOFIT Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
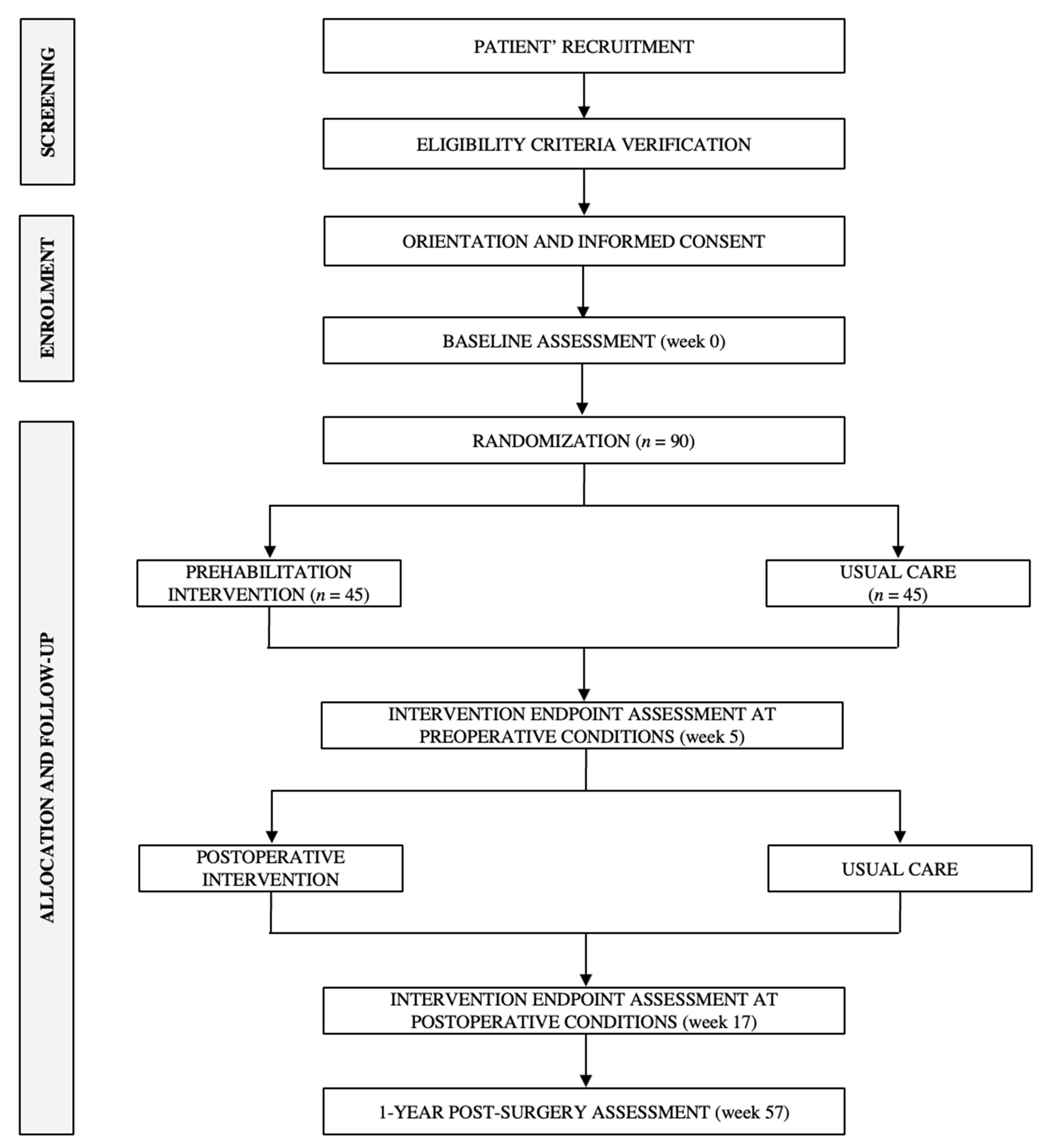
2.1. Study Design
2.2. Participants and Selection Criteria
2.3. Recruitment and Randomization
Evaluation of Integrity, Compliance of the Intervention and Patients’ Retention/Adherence
2.4. Intervention Description
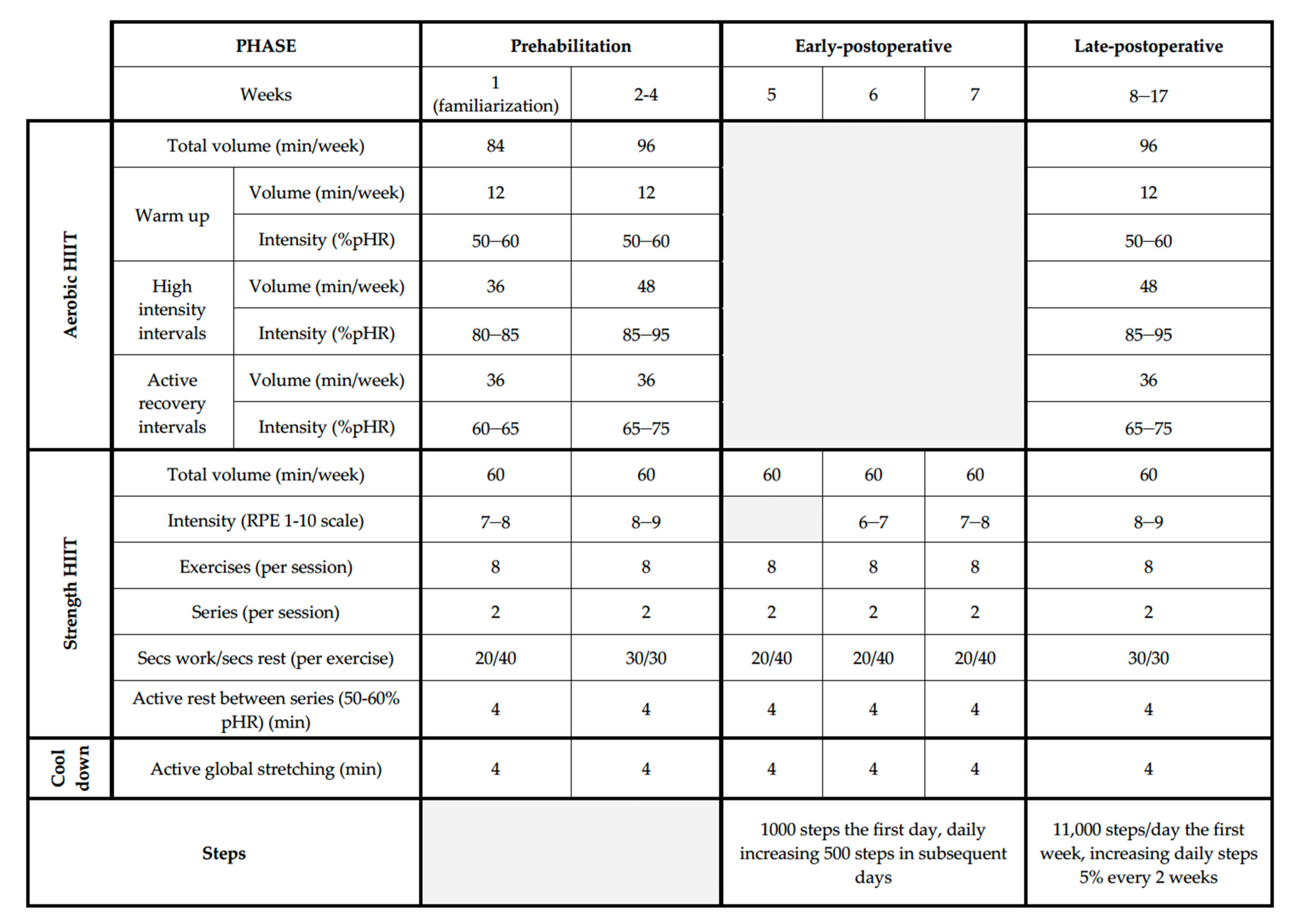
2.4.1. Physical Exercise Intervention
Volume
Intensity
Frequency
Type of Exercise
Training Load Variation
Training Periodization
Prehabilitation Phase
Early-Postoperative Phase
Late-Postoperative Phase
2.4.2. Dietary Behavior Change
Prehabilitation Phase
Postoperative Phase
2.4.3. Psychological Support
Prehabilitation Phase
Postoperative Phase
2.5. Usual Care/Control Group
2.6. Study Endpoints
2.6.1. Primary Endpoint
2.6.2. Secondary Endpoints
Additional Surgery-Derived Events
Functional Capacity
Patients-Reported Outcome Measures
Anthropometry and Body Composition
Clinical/Tumor Parameters
Physical Activity and Sedentariness
Dietary Habits
Others Unhealthy Habits
Sleep Quality
Fecal Microbiota Analysis
2.7. Cost-Effectiveness Analysis Outcome
2.8. Sample Size
2.9. Analytical Approach and Statistical Power/Data Management
3. Potential Impact of the ONCOFIT Study
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Boeding, J.R.E.; Ramphal, W.; Rijken, A.M.; Crolla, R.M.P.H.; Verhoef, C.; Gobardhan, P.D.; Schreinemakers, J.M.J. A Systematic Review Comparing Emergency Resection and Staged Treatment for Curable Obstructing Right-Sided Colon Cancer. Ann. Surg. Oncol. 2021, 28, 3545–3555. [Google Scholar] [CrossRef] [PubMed]
- Desborough, J.P. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Fagard, K.; Leonard, S.; Deschodt, M.; Devriendt, E.; Wolthuis, A.; Prenen, H.; Flamaing, J.; Milisen, K.; Wildiers, H.; Kenis, C. The impact of frailty on postoperative outcomes in individuals aged 65 and over undergoing elective surgery for colorectal cancer: A systematic review. J. Geriatr. Oncol. 2016, 7, 479–491. [Google Scholar] [CrossRef] [PubMed]
- McDermott, F.D.; Heeney, A.; Kelly, M.E.; Steele, R.J.; Carlson, G.L.; Winter, D.C. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br. J. Surg. 2015, 102, 462–479. [Google Scholar] [CrossRef]
- Cheng, E.; Ou, F.-S.; Ma, C.; Spiegelman, D.; Zhang, S.; Zhou, X.; Bainter, T.M.; Saltz, L.B.; Niedzwiecki, D.; Mayer, R.J.; et al. Diet- and Lifestyle-Based Prediction Models to Estimate Cancer Recurrence and Death in Patients With Stage III Colon Cancer (CALGB 89803/Alliance). J. Clin. Oncol. 2022, 40, 740–751. [Google Scholar] [CrossRef]
- Gomez, D.; Jimenez-Fonseca, P.; Fernández, A.M.; Castellanos, P.C.; Arbizu, M.V.; Cabañes, R.M.; Estellés, D.L.; Ferreira, E.; del Rio, J.; García, T.G.; et al. Impact of Obesity on Quality of Life, Psychological Distress, and Coping on Patients with Colon Cancer. Oncologist 2021, 26, e874–e882. [Google Scholar] [CrossRef]
- Jeong, S.; Lee, G.; Choi, S.; Kim, K.H.; Chang, J.; Kim, S.M.; Kim, K.; Son, J.S.; Cho, Y.; Park, S.M. Estimating Risk of Cardiovascular Disease Among Long-Term Colorectal Cancer Survivors: A Nationwide Cohort Study. Front. Cardiovasc. Med. 2022, 8, 721107. [Google Scholar] [CrossRef]
- Fulop, A.; Lakatos, L.; Susztak, N.; Szijarto, A.; Banky, B. The effect of trimodal prehabilitation on the physical and psychological health of patients undergoing colorectal surgery: A randomised clinical trial. Anaesthesia 2021, 76, 82–90. [Google Scholar] [CrossRef]
- Suen, M.; Liew, A.; Turner, J.D.; Khatri, S.; Lin, Y.; Raso, K.L.; Vardy, J.L. Short-term multimodal prehabilitation improves functional capacity for colorectal cancer patients prior to surgery. Asia. Pac. J. Clin. Oncol. 2021, 18, e103–e110. [Google Scholar] [CrossRef]
- Shelton, E.; Barreto, N.B.; Bidwell, S.; Folk-Tolbert, M.; Shelton, A.; Trickey, A.W.; Kin, C.J. Engagement and Adherence with a Web-Based Prehabilitation Program for Patients Awaiting Abdominal Colorectal Surgery. J. Gastrointest. Surg. 2021, 25, 3198–3207. [Google Scholar] [CrossRef] [PubMed]
- Minnella, E.M.; Bousquet-Dion, G.; Awasthi, R.; Scheede-Bergdahl, C.; Carli, F. Multimodal prehabilitation improves functional capacity before and after colorectal surgery for cancer: A five-year research experience. Acta Oncol. 2017, 56, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA. Cancer J. Clin. 2012, 62, 242–274. [Google Scholar] [CrossRef] [Green Version]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [Green Version]
- Cheville, A.L.; Mustian, K.; Winters-Stone, K.; Zucker, D.S.; Gamble, G.L.; Alfano, C.M. Cancer Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 1–17. [Google Scholar] [CrossRef]
- Frawley, H.C.; Lin, K.-Y.; Granger, C.L.; Higgins, R.; Butler, M.; Denehy, L. An allied health rehabilitation program for patients following surgery for abdomino-pelvic cancer: A feasibility and pilot clinical study. Support. Care Cancer 2020, 28, 1335–1350. [Google Scholar] [CrossRef]
- Mohammed, T.; Parekh, T.; Desai, A. Cardiovascular risk management in cancer survivors: Are we doing it right? World J. Clin. Oncol. 2021, 12, 144–149. [Google Scholar] [CrossRef]
- Carli, F.; Bousquet-Dion, G.; Awasthi, R.; Elsherbini, N.; Liberman, S.; Boutros, M.; Stein, B.; Charlebois, P.; Ghitulescu, G.; Morin, N.; et al. Effect of Multimodal Prehabilitation vs Postoperative Rehabilitation on 30-Day Postoperative Complications for Frail Patients Undergoing Resection of Colorectal Cancer. JAMA Surg. 2020, 155, 233. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Grimes, D.; Schulz, K.F.; Grimes, D.A. Generation of allocation sequences in randomised trials: Chance, not choice. Lancet 2002, 359, 515–519. [Google Scholar] [CrossRef]
- Friedberg, J.P.; Lipsitz, S.R.; Natarajan, S. Challenges and recommendations for blinding in behavioral interventions illustrated using a case study of a behavioral intervention to lower blood pressure. Patient Educ. Couns. 2010, 78, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, B. The assessment, monitoring, and enhancement of treatment fidelity in public health clinical trials. J. Public Health Dent. 2011, 71, S52–S63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carneiro-Barrera, A.; Amaro-Gahete, F.J.; Díaz-Román, A.; Guillén-Riquelme, A.; Jurado-Fasoli, L.; Sáez-Roca, G.; Martín-Carrasco, C.; Ruiz, J.R.; Buela-Casal, G. Interdisciplinary weight loss and lifestyle intervention for obstructive sleep apnoea in adults: Rationale, design and methodology of the INTERAPNEA study. Nutrients 2019, 11, 2227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochaska, J.O.; Velicer, W.F. The Transtheoretical Model of Health Behavior Change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle. Part II: Anaerobic energy, neuromuscular load and practical applications. Sports Med. 2013, 43, 927–954. [Google Scholar] [CrossRef]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle: Part I: Cardiopulmonary emphasis. Sport. Med. 2013, 43, 313–338. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Hwang, C.L.; Yoo, J.K.; Kim, H.K.; Hwang, M.H.; Handberg, E.M.; Petersen, J.W.; Christou, D. Novel all-extremity high-intensity interval training improves aerobic fitness, cardiac function and insulin resistance in healthy older adults. Exp. Gerontol. 2016, 82, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Amaro-Gahete, F.J.; De-la-O, A.; Jurado-Fasoli, L.; Espuch-Oliver, A.; Robles-Gonzalez, L.; Navarro-Lomas, G.; de Haro, T.; Femia, P.; Castillo, M.J.; Gutierrez, A. Exercise training as S-Klotho protein stimulator in sedentary healthy adults: Rationale, design, and methodology. Contemp. Clin. Trials Commun. 2018, 11, 10–19. [Google Scholar] [CrossRef]
- Haidari, F.; Abiri, B.; Iravani, M.; Razavi, S.-M.; Sarbakhsh, P.; Ahmadi-Angali, K.; Vafa, M. Effects of vitamin D and omega-3 fatty acids co-supplementation on inflammatory biomarkers, tumor marker CEA, and nutritional status in patients with colorectal cancer: A study protocol for a double blind randomized controlled trial. Trials 2019, 20, 682. [Google Scholar] [CrossRef]
- Morishima, T.; Sato, A.; Nakata, K.; Miyashiro, I. Geriatric assessment domains to predict overall survival in older cancer patients: An analysis of functional status, comorbidities, and nutritional status as prognostic factors. Cancer Med. 2020, 9, 5839–5850. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Liu, L.; Wang, W.; Fung, T.T.; Wu, K.; Smith-Warner, S.A.; Cao, Y.; Hu, F.B.; Ogino, S.; Fuchs, C.S.; et al. Association of Dietary Inflammatory Potential With Colorectal Cancer Risk in Men and Women. JAMA Oncol. 2018, 4, 366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, V.; Atkinson, C.; Ness, A.R.; Thomas, S.; Burden, S.; Sutton, E. Patient experiences of perioperative nutrition within an Enhanced Recovery After Surgery programme for colorectal surgery: A qualitative study. Color. Dis. 2016, 18, O74–O80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. Benefits of the Mediterranean Diet: Insights From the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, M.A.; Sato, K.; Niedzwiecki, D.; Ye, X.; Saltz, L.B.; Mayer, R.J.; Mowat, R.B.; Whittom, R.; Hantel, A.; Benson, A.; et al. Sugar-Sweetened Beverage Intake and Cancer Recurrence and Survival in CALGB 89803 (Alliance). PLoS ONE 2014, 9, e99816. [Google Scholar] [CrossRef] [Green Version]
- Winkels, R.M.; Heine-Bröring, R.C.; van Zutphen, M.; van Harten-Gerritsen, S.; Kok, D.E.; van Duijnhoven, F.J.; Kampman, E. The COLON study: Colorectal cancer: Longitudinal, Observational study on Nutritional and lifestyle factors that may influence colorectal tumour recurrence, survival and quality of life. BMC Cancer 2014, 14, 374. [Google Scholar] [CrossRef] [Green Version]
- Harvard, T.-H. Healthy Eating Plate; University of Hardvard: Cambridge, MA, USA, 2011. [Google Scholar]
- Carbajal, A. Manual de nutrición y dietética: Dieta en españa. In Consumo de Alimentos; Universidad Complutense de Madrid: Madrid, Spain, 2019. [Google Scholar]
- Metcalfe, J.J.; Leonard, D. The relationship between culinary skills and eating behaviors: Challenges and opportunities for parents and families. Physiol. Behav. 2018, 191, 95–99. [Google Scholar] [CrossRef]
- Gonzalez-Ayora, S.; Pastor, C.; Guadalajara, H.; Ramirez, J.M.; Royo, P.; Redondo, E.; Arroyo, A.; Moya, P.; Garcia-Olmo, D. Enhanced recovery care after colorectal surgery in elderly patients. Compliance and outcomes of a multicenter study from the Spanish working group on ERAS. Int. J. Colorectal Dis. 2016, 31, 1625–1631. [Google Scholar] [CrossRef] [Green Version]
- Miller, T.E.; Roche, A.M.; Mythen, M. Fluid management and goal-directed therapy as an adjunct to Enhanced Recovery After Surgery (ERAS). Can. J. Anesth. Can. D’anesthésie 2015, 62, 158–168. [Google Scholar] [CrossRef] [Green Version]
- Moya, P.; Soriano-Irigaray, L.; Ramirez, J.M.; Garcea, A.; Blasco, O.; Blanco, F.J.; Brugiotti, C.; Miranda, E.; Arroyo, A. Perioperative Standard Oral Nutrition Supplements Versus Immunonutrition in Patients Undergoing Colorectal Resection in an Enhanced Recovery (ERAS) Protocol. Medicine (Baltimore) 2016, 95, e3704. [Google Scholar] [CrossRef]
- Van Rooijen, S.; Carli, F.; Dalton, S.; Thomas, G.; Bojesen, R.; Le Guen, M.; Barizien, N.; Awasthi, R.; Minnella, E.; Beijer, S.; et al. Multimodal prehabilitation in colorectal cancer patients to improve functional capacity and reduce postoperative complications: The first international randomized controlled trial for multimodal prehabilitation. BMC Cancer 2019, 19, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.F.; Ho, J.W.C.; Fong, D.Y.T.; Macfarlane, D.J.; Cerin, E.; Lee, A.M.; Leung, S.; Chan, W.Y.Y.; Leung, I.P.F.; Lam, S.H.S.; et al. Dietary and Physical Activity Interventions for Colorectal Cancer Survivors: A Randomized Controlled Trial. Sci. Rep. 2018, 8, 5731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.G.A.; Molinger, J.; Wischmeyer, P.E. The malnourished surgery patient. Curr. Opin. Anaesthesiol. 2019, 32, 405–411. [Google Scholar] [CrossRef]
- Gómez Sánchez, M.B.; García-Talavera Espín, N.V.; Sánchez Álvarez, C.; Zomeño Ros, A.I.; Hernández, M.N.; Gómez Ramos, M.J.; Parra Baños, P.; González Valverde, F.M. Perioperative nutritional support in patients with colorectal neoplasms. Nutr. Hosp. 2010, 25, 797–805. [Google Scholar] [PubMed]
- Garth, A.K.; Newsome, C.M.; Simmance, N.; Crowe, T.C. Nutritional status, nutrition practices and post—operative complications in patients with gastrointestinal cancer. J. Hum. Nutr. Diet. 2010, 23, 393–401. [Google Scholar] [CrossRef]
- Uçar, A.; Yilmaz, M.V.; Çakiroglu, F.P. Food Safety—Problems and Solutions. In Significance, Prevention and Control of Food Related Diseases; InTech: Istanbul, Turkey, 2016. [Google Scholar]
- Garrett, W.S. The gut microbiota and colon cancer. Science 2019, 364, 1133–1135. [Google Scholar] [CrossRef]
- Helmink, B.A.; Khan, M.A.W.; Hermann, A.; Gopalakrishnan, V.; Wargo, J.A. The microbiome, cancer, and cancer therapy. Nat. Med. 2019, 25, 377–388. [Google Scholar] [CrossRef]
- Veintimilla, D.R.; Frías Toral, E. Microbiota intestinal y cáncer. Rev. Nutr. Clínica y Metab. 2021, 4, 94–102. [Google Scholar] [CrossRef]
- Ames, B.N.; Wakimoto, P. Are vitamin and mineral deficiencies a major cancer risk? Nat. Rev. Cancer 2002, 2, 694–704. [Google Scholar] [CrossRef]
- Nissensohn, M.; Sánchez-Villegas, A.; Ortega, R.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Varela-Moreiras, G.; Serra-Majem, L. Beverage Consumption Habits and Association with Total Water and Energy Intakes in the Spanish Population: Findings of the ANIBES Study. Nutrients 2016, 8, 232. [Google Scholar] [CrossRef]
- Shaukat, A.; Dostal, A.; Menk, J.; Church, T.R. BMI Is a Risk Factor for Colorectal Cancer Mortality. Dig. Dis. Sci. 2017, 62, 2511–2517. [Google Scholar] [CrossRef] [PubMed]
- Nestares, T.; Martín-Masot, R.; Flor-Alemany, M.; Bonavita, A.; Maldonado, J.; Aparicio, V.A. Influence of Ultra-Processed Foods Consumption on Redox Status and Inflammatory Signaling in Young Celiac Patients. Nutrients 2021, 13, 156. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, C.; Cornelius, V.; Love, S.; Graham, J.; Richards, M.; Ramirez, A. Depression and anxiety in women with early breast cancer: Five year observational cohort study. BMJ 2005, 330, 702. [Google Scholar] [CrossRef] [Green Version]
- Sheard, T.; Maguire, P. The effect of psychological interventions on anxiety and depression in cancer patients: Results of two meta-analyses. Br. J. Cancer 1999, 80, 1770–1780. [Google Scholar] [CrossRef] [Green Version]
- Dunn, J.; Ng, S.K.; Holland, J.; Aitken, J.; Youl, P.; Baade, P.D.; Chambers, S.K. Trajectories of psychological distress after colorectal cancer. Psychooncology 2013, 22, 1759–1765. [Google Scholar] [CrossRef]
- Wells, K.B.; Stewart, A.; Hays, R.D.; Burnam, M.A.; Rogers, W.; Daniels, M.; Berry, S.; Greenfield, S.; Ware, J. The functioning and well-being of depressed patients. Results from the Medical Outcomes Study. JAMA 1989, 262, 914–919. [Google Scholar] [CrossRef]
- Lynch, B.M.; Steginga, S.K.; Hawkes, A.L.; Pakenham, K.I.; Dunn, J. Describing and predicting psychological distress after colorectal cancer. Cancer 2008, 112, 1363–1370. [Google Scholar] [CrossRef]
- Faller, H.; Schuler, M.; Richard, M.; Heckl, U.; Weis, J.; Küffner, R. Effects of Psycho-Oncologic Interventions on Emotional Distress and Quality of Life in Adult Patients With Cancer: Systematic Review and Meta-Analysis. J. Clin. Oncol. 2013, 31, 782–793. [Google Scholar] [CrossRef] [Green Version]
- Mosher, C.E.; Winger, J.G.; Given, B.A.; Shahda, S.; Helft, P.R. A systematic review of psychosocial interventions for colorectal cancer patients. Support. Care Cancer 2017, 25, 2349–2362. [Google Scholar] [CrossRef]
- Pugliese, P.; Perrone, M.; Nisi, E.; Garufi, C.; Giannarelli, D.; Bottomley, A.; Terzoli, E. An integrated psychological strategy for advanced colorectal cancer patients. Health Qual. Life Outcomes 2006, 4, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery After Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slankamenac, K.; Nederlof, N.; Pessaux, P.; de Jonge, J.; Wijnhoven, B.P.L.; Breitenstein, S.; Oberkofler, C.E.; Graf, R.; Puhan, M.A.; Clavien, P.-A. The Comprehensive Complication Index. Ann. Surg. 2014, 260, 757–763. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la-O, A.; Jurado-Fasoli, L.; Martinez-Tellez, B.; Ruiz, J.R.; Castillo, M.J. Exercise Training as a Treatment for Cardiometabolic Risk in Sedentary Adults: Are Physical Activity Guidelines the Best Way to Improve Cardiometabolic Health? The FIT-AGEING Randomized Controlled Trial. J. Clin. Med. 2019, 8, 2097. [Google Scholar] [CrossRef] [Green Version]
- Kervio, G.; Carre, F.; Ville, N.S. Reliability and Intensity of the Six-Minute Walk Test in Healthy Elderly Subjects. Med. Sci. Sport. Exerc. 2003, 35, 169–174. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Pecorelli, N.; Fiore, J.F.; Gillis, C.; Awasthi, R.; Mappin-Kasirer, B.; Niculiseanu, P.; Fried, G.M.; Carli, F.; Feldman, L.S. The six-minute walk test as a measure of postoperative recovery after colorectal resection: Further examination of its measurement properties. Surg. Endosc. 2016, 30, 2199–2206. [Google Scholar] [CrossRef]
- Antonescu, I.; Scott, S.; Tran, T.T.; Mayo, N.E.; Feldman, L.S. Measuring postoperative recovery: What are clinically meaningful differences? Surgery 2014, 156, 319–327. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. A. Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyère, O.; Beaudart, C.; Reginster, J.Y.; Buckinx, F.; Schoene, D.; Hirani, V.; Cooper, C.; Kanis, J.A.; Rizzoli, R.; McCloskey, E.; et al. Assessment of muscle mass, muscle strength and physical performance in clinical practice: An international survey. Eur. Geriatr. Med. 2016, 7, 243–246. [Google Scholar] [CrossRef]
- Cesari, M.; Kritchevsky, S.B.; Newman, A.B.; Simonsick, E.M.; Harris, T.B.; Penninx, B.W.; Brach, J.S.; Tylavsky, F.A.; Satterfield, S.; Bauer, D.C.; et al. Added Value of Physical Performance Measures in Predicting Adverse Health-Related Events: Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2009, 57, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Ruiz, J.; Mesa, J.L.M.; Gutiérrez, A.; Castillo, M.J. Hand size influences optimal grip span in women but not in men. J. Hand Surg. Am. 2002, 27, 897–901. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; McCloskey, E.; Bruyère, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Bautmans, I.; Bertière, M.-C.; et al. Sarcopenia in daily practice: Assessment and management. BMC Geriatr. 2016, 16, 170. [Google Scholar] [CrossRef]
- Alcazar, J.; Kamper, R.S.; Aagaard, P.; Haddock, B.; Prescott, E.; Ara, I.; Suetta, C. Relation between leg extension power and 30-s sit-to-stand muscle power in older adults: Validation and translation to functional performance. Sci. Rep. 2020, 10, 16337. [Google Scholar] [CrossRef]
- Arraras, J.I.; Suárez, J.; Arias de la Vega, F.; Vera, R.; Asín, G.; Arrazubi, V.; Rico, M.; Teijeira, L.; Azparren, J. The EORTC quality of life questionnaire for patients with colorectal cancer: EORTC QLQ-CR29 validation study for Spanish patients. Clin. Transl. Oncol. 2011, 13, 50–56. [Google Scholar] [CrossRef]
- Wang, Y.; Gorenstein, C. Assessment of depression in medical patients: A systematic review of the utility of the Beck Depression Inventory-II. Clinics 2013, 68, 1274–1287. [Google Scholar] [CrossRef]
- Buela-Casal, G.; Guillén-Riquelme, A.; Seisdedos Cubero, N. Cuestionario de Ansiedad Estado-Rasgo: Adaptación Española; TEA Edicio: Madrid, Spain, 2011. [Google Scholar]
- López-Roig, S.; Terol, M.C.; Pastor, M.A.; Neipp, M.C.; Massutí, B. Ansiedad y depresión. Validación de la escala HAD en pacientes oncológicos. Rev. Psicol. Salud 2000, 12, 127–155. [Google Scholar] [CrossRef]
- Berlanga, J.F.; Aliaga, M.T.; Martín, M.P.B. Evaluación cognitiva y afrontamiento como predictores del bienestar futuro de las pacientes con cáncer de mama. Rev. Latinoam. Psicol. 1995, 27, 87–102. [Google Scholar]
- Marfell-Jones, M.J.; Stewart, A.D.; de Ridder, J.H. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Wellington, New Zealand, 2012. [Google Scholar]
- Whelton, P.K.; Williams, B. The 2018 European Society of Cardiology/European Society of Hypertension and 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines. JAMA 2018, 320, 1749. [Google Scholar] [CrossRef] [PubMed]
- Schootman, M.; Jeffe, D.B.; Ratnapradipa, K.L.; Eberth, J.M.; Davidson, N.O. Increased 30-Day Mortality Risk in Patients With Diabetes Mellitus After Colon Cancer Surgery: A Mediation Analysis. Dis. Colon Rectum 2020, 63, 290–299. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Pereira, S.S.; Monteiro, M.P.; Araújo, A.; Faria, G. Effect of Metabolic Syndrome and Individual Components on Colon Cancer Characteristics and Prognosis. Front. Oncol. 2021, 11, 631257. [Google Scholar] [CrossRef]
- Chen, W.; Wang, M.; Jing, X.; Wu, C.; Zeng, Y.; Peng, J.; Cai, X. High risk of colorectal polyps in men with non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 2051–2065. [Google Scholar] [CrossRef]
- Wang, S.C.; Schulman-Marcus, J.; Fantauzzi, J.; Bevington, T.; Sayegh, A.; Lee, E.; Ata, A.; Kambam, M.; Sidhu, M.; Lyubarova, R. Colon cancer laterality is associated with atherosclerosis and coronary artery disease. J. Gastrointest. Oncol. 2018, 10, 30–36. [Google Scholar] [CrossRef]
- Ascaso, J.F.; Romero, P.; Real, J.T.; Priego, A.; Valdecabres, C.; Carmena, R. Insulin resistance quantification by fasting insulin plasma values and HOMA index in a non-diabetic population. Med. Clin. 2001, 117, 530–533. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- del Río-Moreno, M.; Luque, R.M.; Rangel-Zúñiga, O.A.; Alors-Pérez, E.; Alcalá-Diaz, J.F.; Roncero-Ramos, I.; Camargo, A.; Gahete, M.D.; López-Miranda, J.; Castaño, J.P. Dietary Intervention Modulates the Expression of Splicing Machinery in Cardiovascular Patients at High Risk of Type 2 Diabetes Development: From the CORDIOPREV Study. Nutrients 2020, 12, 3528. [Google Scholar] [CrossRef]
- Gahete, M.D.; del Rio-Moreno, M.; Camargo, A.; Alcala-Diaz, J.F.; Alors-Perez, E.; Delgado-Lista, J.; Reyes, O.; Ventura, S.; Perez-Martínez, P.; Castaño, J.P.; et al. Changes in Splicing Machinery Components Influence, Precede, and Early Predict the Development of Type 2 Diabetes: From the CORDIOPREV Study. EBioMedicine 2018, 37, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Gahete, M.D.; Luque, R.M.; Yubero-Serrano, E.M.; Cruz-Teno, C.; Ibañez-Costa, A.; Delgado-Lista, J.; Gracia-Navarro, F.; Perez-Jimenez, F.; Castaño, J.P.; Lopez-Miranda, J. Dietary fat alters the expression of cortistatin and ghrelin systems in the PBMCs of elderly subjects: Putative implications in the postprandial inflammatory response. Mol. Nutr. Food Res. 2014, 58, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- López-Cánovas, J.L.; del Rio-Moreno, M.; García-Fernandez, H.; Jiménez-Vacas, J.M.; Moreno-Montilla, M.T.; Sánchez-Frias, M.E.; Amado, V.; López, L.F.; Fondevila, M.F.; Ciria, R.; et al. Splicing factor SF3B1 is overexpressed and implicated in the aggressiveness and survival of hepatocellular carcinoma. Cancer Lett. 2021, 496, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Vacas, J.M.; Herrero-Aguayo, V.; Montero-Hidalgo, A.J.; Gómez-Gómez, E.; Fuentes-Fayos, A.C.; León-González, A.J.; Sáez-Martínez, P.; Alors-Pérez, E.; Pedraza-Arévalo, S.; González-Serrano, T.; et al. Dysregulation of the splicing machinery is directly associated to aggressiveness of prostate cancer. EBioMedicine 2020, 51, 102547. [Google Scholar] [CrossRef] [Green Version]
- Fuentes-Fayos, A.C.; Vázquez-Borrego, M.C.; Jiménez-Vacas, J.M.; Bejarano, L.; Pedraza-Arévalo, S.; López, L.F.; Blanco-Acevedo, C.; Sánchez-Sánchez, R.; Reyes, O.; Ventura, S.; et al. Splicing machinery dysregulation drives glioblastoma development/aggressiveness: Oncogenic role of SRSF3. Brain 2020, 143, 3273–3293. [Google Scholar] [CrossRef]
- del Río-Moreno, M.; Alors-Pérez, E.; González-Rubio, S.; Ferrín, G.; Reyes, O.; Rodríguez-Perálvarez, M.; Sánchez-Frías, M.E.; Sánchez-Sánchez, R.; Ventura, S.; López-Miranda, J.; et al. Dysregulation of the Splicing Machinery Is Associated to the Development of Nonalcoholic Fatty Liver Disease. J. Clin. Endocrinol. Metab. 2019, 104, 3389–3402. [Google Scholar] [CrossRef] [PubMed]
- Roman-Viñas, B.; Serra-Majem, L.; Hagströmer, M.; Ribas-Barba, L.; Sjöström, M.; Segura-Cardona, R. International Physical Activity Questionnaire: Reliability and validity in a Spanish population. Eur. J. Sport Sci. 2010, 10, 297–304. [Google Scholar] [CrossRef]
- Kim, Y.; Park, I.; Kang, M. Convergent validity of the International Physical Activity Questionnaire (IPAQ): Meta-analysis. Public Health Nutr. 2013, 16, 440–452. [Google Scholar] [CrossRef] [Green Version]
- Mataix, J.L.; Martinez de Victoria, E.; Montellano, M.; Lopez, M.; Aranda, P.L. Valoración del estado nutricional de la comunidad autónoma de Andalucía. Cons Salud. 2000. Available online: https://www.repositoriosalud.es/bitstream/10668/1215/5/ValoracionNutricional_2000.pdf (accessed on 2 October 2022).
- López, M.D.R.; Martín-Lagos, R.A.; Martin-Lagos, R.A. Guía Para Estudios Dietéticos: Álbum Fotográfico de Alimentos; Editorial Universidad de Granada: Granada, Spain, 2010; ISBN 8433851675. [Google Scholar]
- Zaragoza-Martí, A.; Cabañero-Martínez, M.; Hurtado-Sánchez, J.; Laguna-Pérez, A.; Ferrer-Cascales, R. Evaluation of Mediterranean diet adherence scores: A systematic review. BMJ Open 2018, 8, e019033. [Google Scholar] [CrossRef] [Green Version]
- Becoña, E.; Alvarez-Soto, E.; Gómez-Durán, B.; García, M.P. Scores of Spanish Smokers on Fagerström’s Tolerance Questionnaire. Psychol. Rep. 1992, 71, 1227–1233. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Ternes, D.; Karta, J.; Tsenkova, M.; Wilmes, P.; Haan, S.; Letellier, E. Microbiome in Colorectal Cancer: How to Get from Meta-omics to Mechanism? Trends Microbiol. 2020, 28, 401–423. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.H.; Yu, J. Gut microbiota in colorectal cancer: Mechanisms of action and clinical applications. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 690–704. [Google Scholar] [CrossRef]
- Sánchez-Alcoholado, L.; Ramos-Molina, B.; Otero, A.; Laborda-Illanes, A.; Ordóñez, R.; Medina, J.A.; Gómez-Millán, J.; Queipo-Ortuño, M.I. The Role of the Gut Microbiome in Colorectal Cancer Development and Therapy Response. Cancers 2020, 12, 1406. [Google Scholar] [CrossRef] [PubMed]
- Herlemann, D.; Labrenz, M.; Jü Rgens, K.; Bertilsson, S.; Waniek, J.J.; Andersson, A.F. Transitions in bacterial communities along the 2000 km salinity gradient of the Baltic Sea. ISME J. 2011, 5, 1571–1579. [Google Scholar] [CrossRef] [Green Version]
- Lozupone, C.A.; Knight, R. Species divergence and the measurement of microbial diversity. FEMS Microbiol. Rev. 2008, 32, 557–578. [Google Scholar] [CrossRef]
- Kim, B.-R.; Shin, J.; Guevarra, R.B.; Lee, J.H.; Kim, D.W.; Seol, K.-H.; Lee, J.-H.; Kim, H.B.; Isaacson, R.E. Deciphering Diversity Indices for a Better Understanding of Microbial Communities. J. Microbiol. Biotechnol 2017, 27, 2089–2093. [Google Scholar] [CrossRef] [Green Version]
- Simpson, E.H. Measurement of diversity. Nature 1949, 163, 688. [Google Scholar] [CrossRef]
- Aßhauer, K.P.; Wemheuer, B.; Daniel, R.; Meinicke, P. Tax4Fun: Predicting functional profiles from metagenomic 16S rRNA data. Bioinformatics 2015, 31, 2882–2884. [Google Scholar] [CrossRef] [Green Version]
- Hlatky, M.A.; Owens, D.K.; Sanders, G.D. Cost-effectiveness as an outcome in randomized clinical trials. Clin. Trials 2006, 3, 543–551. [Google Scholar] [CrossRef]
- Ramos-Goñi, J.M.; Craig, B.M.; Oppe, M.; Ramallo-Fariña, Y.; Pinto-Prades, J.L.; Luo, N.; Rivero-Arias, O. Handling Data Quality Issues to Estimate the Spanish EQ-5D-5L Value Set Using a Hybrid Interval Regression Approach. Value Health 2018, 21, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edejer, T.T.T.; Baltussen, R.; Adam, T.; Hutubessy, R.; Acharya, A.; Evans, D.B.; Murray, C.J.L. Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Onerup, A.; Angenete, E.; Bonfre, P.; Börjesson, M.; Haglind, E.; Wessman, C.; Nilsson, H. Self-assessed preoperative level of habitual physical activity predicted postoperative complications after colorectal cancer surgery: A prospective observational cohort study. Eur. J. Surg. Oncol. 2019, 45, 2045–2051. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 406–5823. [Google Scholar] [CrossRef]
- Orangio, G.R. The Economics of Colon Cancer. Surg. Oncol. Clin. N. Am. 2018, 27, 327–347. [Google Scholar] [CrossRef]
- Zadlo, J. Cost-effectiveness of new and emerging treatment options for the treatment of metastatic colorectal cancer. Am. J. Manag. Care 2018, 24, S118–S124. [Google Scholar]
- Rezende, L.F.M.; Ferrari, G.; Bahia, L.R.; Rosa, R.D.S.; da Rosa, M.Q.M.; de Souza, R.C.; Lee, D.H.; Giovannucci, E.; Eluf-Neto, J. Economic burden of colorectal and breast cancers attributable to lack of physical activity in Brazil. BMC Public Health 2021, 21, 1190. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
| Outcome | Measurement | Assessment |
|---|---|---|
| Sociodemographic data and medical history | ||
| Anamnesis | Week 0 | |
| Physical exploration | Week 0 | |
| Sociodemographic interview | Week 0 | |
| Surgery-derived events | ||
| Post-surgery complications | Week 17 and 57 | |
| Hospital length of stay | Week 17 and 57 | |
| Readmissions | Week 17 and 57 | |
| Emergency department appointments | Week 17 and 57 | |
| Functional capacity | ||
| Cardiorespiratory fitness | 6 min walking test | Week 0, 5, 17 and 57 |
| Gait speed | 4 min usual walking speed test | Week 0, 5, 17 and 57 |
| Muscular strength | Handgrip strength | Week 0, 5, 17 and 57 |
| 5-times sit-to-stand test | Week 0, 5, 17 and 57 | |
| 30 s sit-to-stand muscle power | Week 0, 5, 17 and 57 | |
| Subjective physical fitness | International fitness scale | Week 0, 5, 17 and 57 |
| Patients-reported outcome measures | ||
| Health-related quality of life | EORTC QLQ-C30 | Week 0, 5, 17 and 57 |
| Depression symptoms | Beck Depression Inventory-II | Week 0, 5, 17 and 57 |
| Anxiety symptoms | State-Trait Anxiety Inventory | Week 0, 5, 17 and 57 |
| Hospital Anxiety and Depression Scale | Week 0, 5, 17 and 57 | |
| Mental adjustment to cancer | Mini--Mental Adjustment to Cancer | Week 0, 5, 17 and 57 |
| Anthropometry and body composition | ||
| Anthropometry | Weight and height measurement, and neck, waist, and hip circumferences | Week 0, 5, 17 and 57 |
| Body composition | Dual Energy X-ray Absorptiometry | Week 0, 5, 17 and 57 |
| Clinical/tumor parameters | ||
| Blood parameters | Glycemic profile, lipid profile, hepatic transaminases, blood cell profile, and renal function profile | Week 0, 5, 17 and 57 |
| Clinical characterization | Blood pressure, homeostatic model assessment of insulin resistance index (HOMA), fatty liver index (FLI) and the cardiometabolic risk score | Week 0, 5, 17 and 57 |
| Tumor biomarkers | Genetic and molecular biomarkers | Week 0, 5, 17 and 57 |
| Circulatory biomarkers | Inflammatory factors, immunological blood profiles, and hormones | Week 0, 5, 17 and 57 |
| Physical activity and sedentariness | ||
| Physical activity habits | International Physical Activity Questionnaire | Week 0, 5, 17 and 57 |
| Dietary habits | ||
| Food frequency questionnaire | Week 0, 5, 17 and 57 | |
| Mediterranean Diet Adherence | Mediterranean Diet Score | Week 0, 5, 17 and 57 |
| Others unhealthy habits | ||
| Tobacco dependence | The Fagerstrom Test for Nicotine Dependence | Week 0, 5, 17 and 57 |
| Tobacco consumption | Self-reported tobacco consumption logs | Week 0, 5, 17 and 57 |
| Alcohol consumption | Self-reported alcohol consumption logs | Week 0, 5, 17 and 57 |
| Sleep quality | ||
| Pittsburgh Sleep Quality Index | Week 0, 5, 17 and 57 | |
| Fecal microbiota | Week 0, 5, 17 and 57 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amaro-Gahete, F.J.; Jurado, J.; Cisneros, A.; Corres, P.; Marmol-Perez, A.; Osuna-Prieto, F.J.; Fernández-Escabias, M.; Salcedo, E.; Hermán-Sánchez, N.; Gahete, M.D.; et al. Multidisciplinary Prehabilitation and Postoperative Rehabilitation for Avoiding Complications in Patients Undergoing Resection of Colon Cancer: Rationale, Design, and Methodology of the ONCOFIT Study. Nutrients 2022, 14, 4647. https://doi.org/10.3390/nu14214647
Amaro-Gahete FJ, Jurado J, Cisneros A, Corres P, Marmol-Perez A, Osuna-Prieto FJ, Fernández-Escabias M, Salcedo E, Hermán-Sánchez N, Gahete MD, et al. Multidisciplinary Prehabilitation and Postoperative Rehabilitation for Avoiding Complications in Patients Undergoing Resection of Colon Cancer: Rationale, Design, and Methodology of the ONCOFIT Study. Nutrients. 2022; 14(21):4647. https://doi.org/10.3390/nu14214647
Chicago/Turabian StyleAmaro-Gahete, Francisco J., Javier Jurado, Andrea Cisneros, Pablo Corres, Andres Marmol-Perez, Francisco J. Osuna-Prieto, Manuel Fernández-Escabias, Estela Salcedo, Natalia Hermán-Sánchez, Manuel D. Gahete, and et al. 2022. "Multidisciplinary Prehabilitation and Postoperative Rehabilitation for Avoiding Complications in Patients Undergoing Resection of Colon Cancer: Rationale, Design, and Methodology of the ONCOFIT Study" Nutrients 14, no. 21: 4647. https://doi.org/10.3390/nu14214647