
Association of Urinary Iodine Concentration with Depressive Symptoms among Adults: NHANES 2007–2018

Abstract
:1. Introduction
2. Materials and Methods
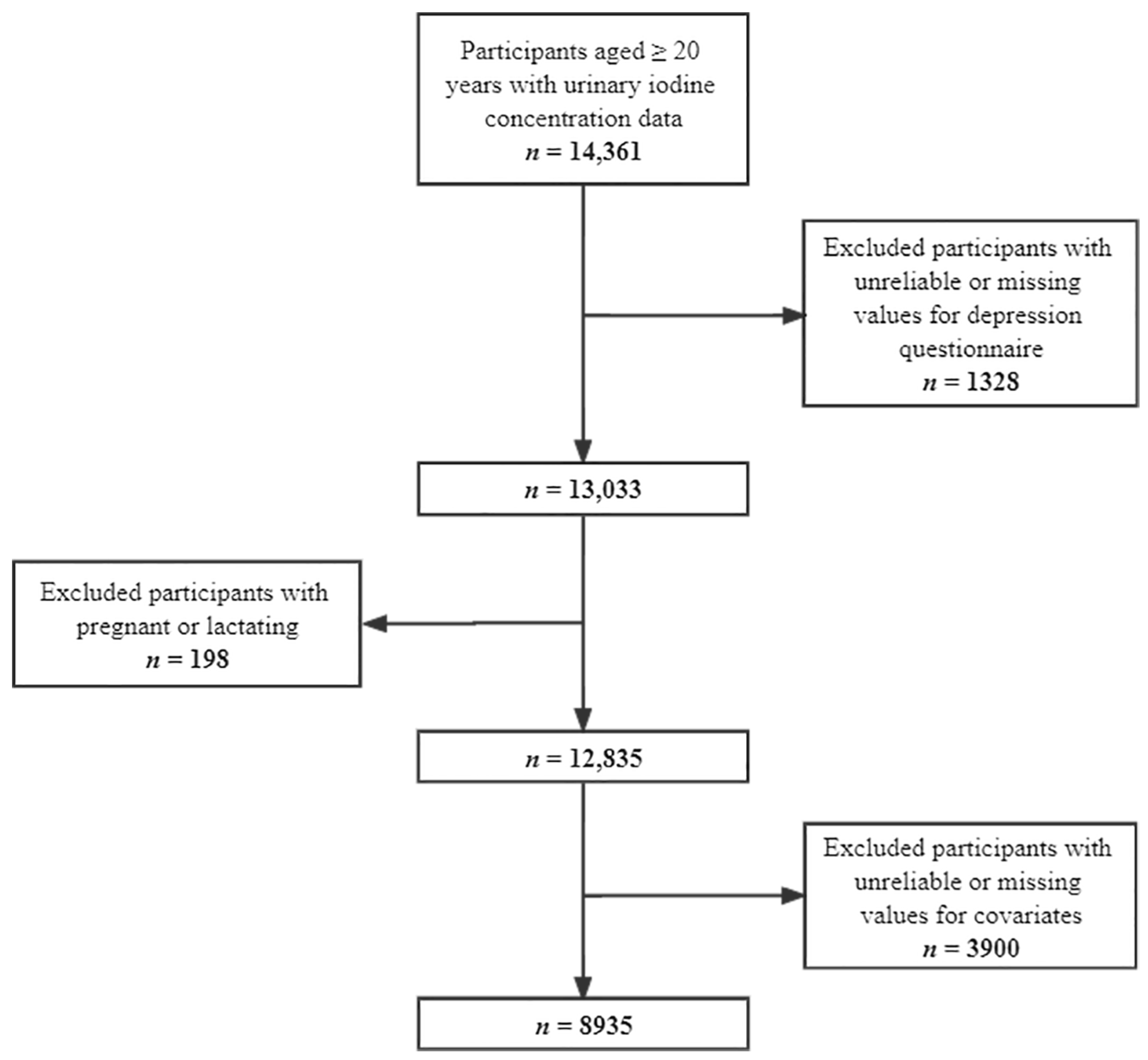
2.1. Study Population
2.2. Urinary Iodine Concentration Measurement
2.3. Depressive Symptoms Assessment
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Depression Fact Sheet. 2020. Available online: https://www.who.int/en/news-room/fact-sheets/detail/depression (accessed on 26 May 2022).
- Cuijpers, P.; Vogelzangs, N.; Twisk, J.; Kleiboer, A.; Li, J.; Penninx, B.W. Comprehensive meta-analysis of excess mortality in depression in the general community versus patients with specific illnesses. Am. J. Psychiatry 2014, 171, 453–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCarron, R.M.; Shapiro, B.; Rawles, J.; Luo, J. Depression. Ann. Intern. Med. 2021, 174, Itc65–itc80. [Google Scholar] [CrossRef]
- WHO. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008.
- Cano-López, I.; Aliño, M.; Duque, A.; Martínez, P.; Almela, M.; García-Rubio, M.J.; Puig-Perez, S. Educational level as a protective factor against the influence of depressive symptoms on cognition in older adults: Implications for functional independence during a 10-year follow-up. Int. Psychogeriatr. 2021, 33, 813–825. [Google Scholar] [CrossRef]
- Wang, W.; Li, W.; Wu, Y.; Tian, X.; Duan, H.; Li, S.; Tan, Q.; Zhang, D. Genome-wide DNA methylation and gene expression analyses in monozygotic twins identify potential biomarkers of depression. Transl. Psychiatry 2021, 11, 416. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Sun, J.; Zhang, D. The relationship between urine polycyclic aromatic hydrocarbons and depressive symptoms in American adults. J. Affect. Disord. 2021, 292, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, Z.; Li, Y.; Zhang, D. Intakes of Specific Categories of Vegetables and Fruits Are Inversely Associated with Depressive Symptoms Among Adults. J. Epidemiol. 2021, 31, 210–219. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.; Luo, J.; Zhang, T.; Zhang, D. Dietary Vitamin C and Vitamin C Derived from Vegetables Are Inversely Associated with the Risk of Depressive Symptoms among the General Population. Antioxidants 2021, 10, 984. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Um, P.; Dickerman, B.A.; Liu, J. Zinc, Magnesium, Selenium and Depression: A Review of the Evidence, Potential Mechanisms and Implications. Nutrients 2018, 10, 584. [Google Scholar] [CrossRef] [Green Version]
- Sun, C.; Wang, R.; Li, Z.; Zhang, D. Dietary magnesium intake and risk of depression. J. Affect. Disord. 2019, 246, 627–632. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Jooste, P.L.; Pandav, C.S. Iodine-deficiency disorders. Lancet 2008, 372, 1251–1262. [Google Scholar] [CrossRef]
- Sorrenti, S.; Baldini, E.; Pironi, D.; Lauro, A.; D’Orazi, V.; Tartaglia, F.; Tripodi, D.; Lori, E.; Gagliardi, F.; Praticò, M.; et al. Iodine: Its Role in Thyroid Hormone Biosynthesis and Beyond. Nutrients 2021, 13, 469. [Google Scholar] [CrossRef] [PubMed]
- Shibuki, K.; Okada, D. Endogenous nitric oxide release required for long-term synaptic depression in the cerebellum. Nature 1991, 349, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Matés, J.M.; Pérez-Gómez, C.; Núñez de Castro, I. Antioxidant enzymes and human diseases. Clin. Biochem. 1999, 32, 595–603. [Google Scholar] [CrossRef]
- Noda, M. Thyroid Hormone in the CNS: Contribution of Neuron-Glia Interaction. Vitam. Horm. 2018, 106, 313–331. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Goetz, T.; Glenn, T.; Whybrow, P.C. The thyroid-brain interaction in thyroid disorders and mood disorders. J. Neuroendocrinol. 2008, 20, 1101–1114. [Google Scholar] [CrossRef]
- Huang, W.; Gong, D.H.; Bao, Y.B. Urinary iodine and serum 25-hydroxyvitamin D are associated with depression in adolescents. Trop. J. Pharm. Res. 2018, 17, 2471–2476. [Google Scholar] [CrossRef]
- Wang, Z.; Li, C.; Teng, Y.; Guan, Y.; Zhang, L.; Jia, X.; Cui, D.; Li, J.; Guan, H. The Effect of Iodine-Containing Vitamin Supplementation During Pregnancy on Thyroid Function in Late Pregnancy and Postpartum Depression in an Iodine-Sufficient Area. Biol. Trace Elem. Res. 2020, 198, 1–7. [Google Scholar] [CrossRef]
- Turan, E.; Karaaslan, O. The Relationship between Iodine and Selenium Levels with Anxiety and Depression in Patients with Euthyroid Nodular Goiter. Oman Med. J. 2020, 35, e161. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations: Past, present, and future. Nutr. Rev. 2012, 70, 553–570. [Google Scholar] [CrossRef]
- World Health Organization; The United Nations Children’s Fund; The International Council for Control of Iodine Deficiency Disorders. Assessment of Iodine Deficiency Disorders and Monitoring their Elimination: A guide for Program Managers. Available online: https://apps.who.int/iris/bitstream/handle/10665/43781/9789241595827_eng.pdf (accessed on 30 May 2022).
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 4 June 2022).
- Approval. NRERBE. Centers for Disease Control and Prevention (CDC) Website. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 4 June 2022).
- NHANES Laboratory/Medical Technologists Procedures Manual (LPM). Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2009-2010/manuals/lab.pdf (accessed on 4 June 2022).
- Levis, B.; Benedetti, A.; Thombs, B.D. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ 2019, 365, l1476. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Sun, J.; Zhang, D. Association between Acrylamide Hemoglobin Adduct Levels and Depressive Symptoms in US Adults: NHANES 2013–2016. J. Agric. Food Chem. 2021, 69, 13762–13771. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Jiang, H.; Wu, Y.; Wang, W.; Zhang, D. The association between Dietary Inflammatory Index and disability in older adults. Clin. Nutr. 2021, 40, 2285–2292. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Sun, J.; Li, Y.; Zhang, D. Associations of n-3, n-6 Fatty Acids Intakes and n-6:n-3 Ratio with the Risk of Depressive Symptoms: NHANES 2009–2016. Nutrients 2020, 12, 240. [Google Scholar] [CrossRef] [Green Version]
- Inoue, K.; Leung, A.M.; Sugiyama, T.; Tsujimoto, T.; Makita, N.; Nangaku, M.; Ritz, B.R. Urinary Iodine Concentration and Mortality Among U.S. Adults. Thyroid Off. J. Am. Thyroid Assoc. 2018, 28, 913–920. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey. Tutorials. Module 3: Weighting. Available online: https://wwwn.cdc.gov/nchs/nhanes/tutorials/module3.aspx (accessed on 4 June 2022).
- Pratt, L.A.; Brody, D.J. Depression in the U.S. household population, 2009–2012. NCHS Data Brief 2014, 172, 1–8. [Google Scholar]
- Vander Weele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Zou, X.; Lin, X.; Bian, J.; Meng, H.; Liu, D. Effect of Excessive Potassium Iodide on Rat Aorta Endothelial Cells. Biol. Trace Elem. Res. 2015, 166, 201–209. [Google Scholar] [CrossRef]
- O’Dell, T.J.; Hawkins, R.D.; Kandel, E.R.; Arancio, O. Tests of the roles of two diffusible substances in long-term potentiation: Evidence for nitric oxide as a possible early retrograde messenger. Proc. Natl. Acad. Sci. USA 1991, 88, 11285–11289. [Google Scholar] [CrossRef] [Green Version]
- Morand, S.; Chaaraoui, M.; Kaniewski, J.; Dème, D.; Ohayon, R.; Noel-Hudson, M.S.; Virion, A.; Dupuy, C. Effect of iodide on nicotinamide adenine dinucleotide phosphate oxidase activity and Duox2 protein expression in isolated porcine thyroid follicles. Endocrinology 2003, 144, 1241–1248. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, L.C.; Martins, D.C.; Figueiredo, M.D.; Rosenthal, D.; Vaisman, M.; Violante, A.H.; Carvalho, D.P. Ca(2+)/nicotinamide adenine dinucleotide phosphate-dependent H(2)O(2) generation is inhibited by iodide in human thyroids. J. Clin. Endocrinol. Metab. 2001, 86, 4339–4343. [Google Scholar] [CrossRef]
- Inada, M.; Nishikawa, M. Thyroid hormone metabolism. Nihon Naibunpi Gakkai Zasshi 1993, 69, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M.B.; Boelaert, K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef]
- Montero-Pedrazuela, A.; Venero, C.; Lavado-Autric, R.; Fernández-Lamo, I.; García-Verdugo, J.M.; Bernal, J.; Guadaño-Ferraz, A. Modulation of adult hippocampal neurogenesis by thyroid hormones: Implications in depressive-like behavior. Mol. Psychiatry 2006, 11, 361–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baba, T.; Ito, S.; Yuasa, M.; Yoshioka, E.; Miyashita, C.; Araki, A.; Sasaki, S.; Kobayashi, S.; Kajiwara, J.; Hori, T.; et al. Association of prenatal exposure to PCDD/Fs and PCBs with maternal and infant thyroid hormones: The Hokkaido Study on Environment and Children’s Health. Sci. Total Environ. 2018, 615, 1239–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yim, G.; Minatoya, M.; Kioumourtzoglou, M.A.; Bellavia, A.; Weisskopf, M.; Ikeda-Araki, A.; Miyashita, C.; Kishi, R. The associations of prenatal exposure to dioxins and polychlorinated biphenyls with neurodevelopment at 6 Months of age: Multi-pollutant approaches. Environ. Res. 2022, 209, 112757. [Google Scholar] [CrossRef]
- Vaiserman, A. Early-life Exposure to Endocrine Disrupting Chemicals and Later-life Health Outcomes: An Epigenetic Bridge? Aging Dis. 2014, 5, 419–429. [Google Scholar] [CrossRef]
- Rasmussen, L.B.; Ovesen, L.; Christiansen, E. Day-to-day and within-day variation in urinary iodine excretion. Eur. J. Clin. Nutr. 1999, 53, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Haddow, J.E.; McClain, M.R.; Palomaki, G.E.; Hollowell, J.G. Urine iodine measurements, creatinine adjustment, and thyroid deficiency in an adult United States population. J. Clin. Endocrinol. Metabol. 2007, 92, 1019–1022. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Non-Depressive Symptoms (PHQ < 10) | Depressive Symptoms (PHQ ≥ 10) | p Value | |
|---|---|---|---|
| Number of participants (%) a | 8108 (90.74) | 827 (9.26) | |
| Age (years), n (%) a | <0.01 | ||
| 20–39 years | 2554 (33.95) | 267 (32.74) | |
| 40–59 years | 2695 (38.70) | 342 (46.21) | |
| ≥60 years | 2859 (27.35) | 218 (21.05) | |
| Sex, n (%) a | <0.001 | ||
| Male | 4391 (51.78) | 326 (37.08) | |
| Female | 3717 (48.22) | 501 (62.92) | |
| Race, n (%) a | <0.001 | ||
| Mexican American | 1140 (7.25) | 115 (7.73) | |
| Other Hispanic | 777 (4.85) | 93 (5.85) | |
| Non-Hispanic White | 3858 (71.78) | 392 (64.11) | |
| Non-Hispanic Black | 1672 (9.88) | 169 (12.64) | |
| Other races | 661 (6.24) | 58 (9.66) | |
| Educational level, n (%) a | <0.001 | ||
| <High school | 1688 (12.20) | 283 (22.83) | |
| High school | 1933 (23.39) | 208 (29.73) | |
| >High school | 4487 (64.41) | 336 (47.43) | |
| Annual household income, n (%) a | <0.001 | ||
| <$20,000 | 1473 (11.23) | 319 (27.68) | |
| ≥$20,000 | 6635 (88.77) | 508 (72.32) | |
| Body mass index, n (%) a | <0.01 | ||
| <25 kg/m2 | 2231 (28.07) | 194 (23.00) | |
| 25 to <30 kg/m2 | 2727 (33.00) | 235 (28.29) | |
| ≥30 kg/m2 | 3150 (38.93) | 398 (48.71) | |
| Marital status, n (%) a | <0.001 | ||
| Not living alone | 5030 (65.30) | 380 (49.00) | |
| Living alone | 3078 (34.70) | 447 (51.00) | |
| Physical activity, n (%) a | <0.001 | ||
| Less | 3060 (33.02) | 420 (48.33) | |
| Normal | 5048 (66.98) | 407 (51.67) | |
| Smoke at least 100 cigarettes in life, n (%) a | 4025 (47.03) | 535 (66.57) | <0.001 |
| Had at least 12 alcohols drink a year, n (%) a | 1270 (14.28) | 239 (31.57) | <0.001 |
| Hypertension, n (%) a | 4427 (50.40) | 494 (58.01) | <0.05 |
| Diabetes, n (%) a | 1450 (13.67) | 199 (19.77) | <0.01 |
| Ever told you had a stroke, n (%) a | 278 (2.21) | 65 (6.10) | <0.001 |
| Caffeine intake (mg/d), median (IQR) b | 109.50 (180.25) | 116.00 (208.00) | 0.210 |
| Total energy intake (kcal/d), median (IQR) b | 1940.50 (1005.50) | 1836.50 (1077.50) | <0.001 |
| Sodium intake (mg/d), median (IQR) b | 3159.75 (1778.75) | 2905.00 (1804.5) | <0.001 |
| Urinary creatinine level (mg/dL), median (IQR) b | 107.00 (102.00) | 111.00 (105.00) | <0.01 |
| Urinary iodine concentration (μg/L), median (IQR) b | 136.15 (162.35) | 152.10 (192.60) | <0.01 |
| Urinary Iodine Concentration (μg/L) | Cases/Participants | Model 1 a | Model 2 b | Model 3 c |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Low UIC (<100) | 274/3170 (8.64%) | 1.12 (0.84–1.52) | 1.06 (0.80–1.43) | 1.22 (0.91–1.65) |
| Normal UIC (100–199) | 254/2867 (8.86%) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Slightly high UIC (200–299) | 116/1314 (8.83%) | 1.03 (0.70–1.52) | 1.10 (0.75–1.61) | 1.02 (0.72–1.46) |
| High UIC (≥300) | 183/1588 (11.55%) | 1.55 (1.11–2.17) * | 1.66 (1.18–2.33) ** | 1.50 (1.04–2.16) * |
| Urinary Iodine Concentration (μg/L) | Cases/Participants | Model 1 a | Model 2 b | Model 3 c |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Females | ||||
| Low UIC (<100) | 171/1662 (10.29%) | 1.17 (0.81–1.69) | 1.13 (0.79–1.64) | 1.50 (1.02–2.18) * |
| Normal UIC (100–199) | 158/1334 (11.84%) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Slightly high UIC (200–299) | 64/549 (11.66%) | 1.32 (0.74–2.35) | 1.35 (0.77–2.37) | 1.15 (0.66–1.99) |
| High UIC (≥300) | 108/669 (16.14%) | 2.08 (1.38–3.15) ** | 2.16 (1.43–3.28) ** | 1.90 (1.19–3.01) ** |
| Males | ||||
| Low UIC (<100) | 103/1508 (6.83%) | 1.00 (0.65–1.56) | 0.99 (0.64–1.54) | 0.94 (0.59–1.49) |
| Normal UIC (100–199) | 96/1530 (6.27%) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Slightly high UIC (200–299) | 51/763 (6.68%) | 0.81 (0.49–1.34) | 0.81 (0.48–1.36) | 0.81 (0.51–1.31) |
| High UIC (≥300) | 75/914 (8.21%) | 1.11 (0.69–1.77) | 1.11 (0.69–1.78) | 1.06 (0.64–1.75) |
| Urinary Iodine Concentration (μg/L) | Cases/Participants | Model 1 a | Model 2 b | Model 3 c |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| 20–39 years | ||||
| Low UIC (<100) | 88/1098 (8.01%) | 0.88 (0.59–1.32) | 0.86 (0.57–1.29) | 0.97 (0.67–1.41) |
| Normal UIC (100–199) | 95/939 (10.12%) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Slightly high UIC (200–299) | 36/359 (10.03%) | 0.96 (0.57–1.60) | 1.00 (0.60–1.67) | 0.87 (0.50–1.51) |
| High UIC (≥300) | 47/423 (11.11%) | 1.33 (0.84–2.12) | 1.33 (0.83–2.12) | 1.21 (0.71–2.07) |
| 40–59 years | ||||
| Low UIC (<100) | 128/1166 (10.98%) | 1.32 (0.86–2.04) | 1.27 (0.83–1.95) | 1.40 (0.85–2.29) |
| Normal UIC (100–199) | 95/948 (10.02%) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Slightly high UIC (200–299) | 37/423 (8.75%) | 0.90 (0.42–1.91) | 0.94 (0.44–1.99) | 0.93 (0.44–1.94) |
| High UIC (≥ 300) | 82/499 (16.43%) | 1.85 (1.15–2.99) * | 1.98 (1.19–3.29) * | 1.90 (1.11–3.25) * |
| ≥60 years | ||||
| Low UIC (< 100) | 58/906 (6.40%) | 1.04 (0.56–1.93) | 1.01 (0.55–1.89) | 1.19 (0.67–2.11) |
| Normal UIC (100–199) | 64/977 (6.55%) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Slightly high UIC (200–299) | 42/530 (7.92%) | 1.47 (0.84–2.55) | 1.53 (0.86–2.71) | 1.34 (0.75–2.40) |
| High UIC (≥ 300) | 54/661 (8.17%) | 1.57 (0.79–3.12) | 1.63 (0.81–3.31) | 1.49 (0.67–3.34) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Cui, K.; Luo, J.; Zhang, D. Association of Urinary Iodine Concentration with Depressive Symptoms among Adults: NHANES 2007–2018. Nutrients 2022, 14, 4165. https://doi.org/10.3390/nu14194165
Chen S, Cui K, Luo J, Zhang D. Association of Urinary Iodine Concentration with Depressive Symptoms among Adults: NHANES 2007–2018. Nutrients. 2022; 14(19):4165. https://doi.org/10.3390/nu14194165
Chicago/Turabian StyleChen, Shumin, Kaiwen Cui, Jia Luo, and Dongfeng Zhang. 2022. "Association of Urinary Iodine Concentration with Depressive Symptoms among Adults: NHANES 2007–2018" Nutrients 14, no. 19: 4165. https://doi.org/10.3390/nu14194165