
The Effect of Different Nutritional Education Models on Reducing Cardiovascular Disease Risk Factors by Improving Dietary Fat Quality in Hemodialysis Patients


 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
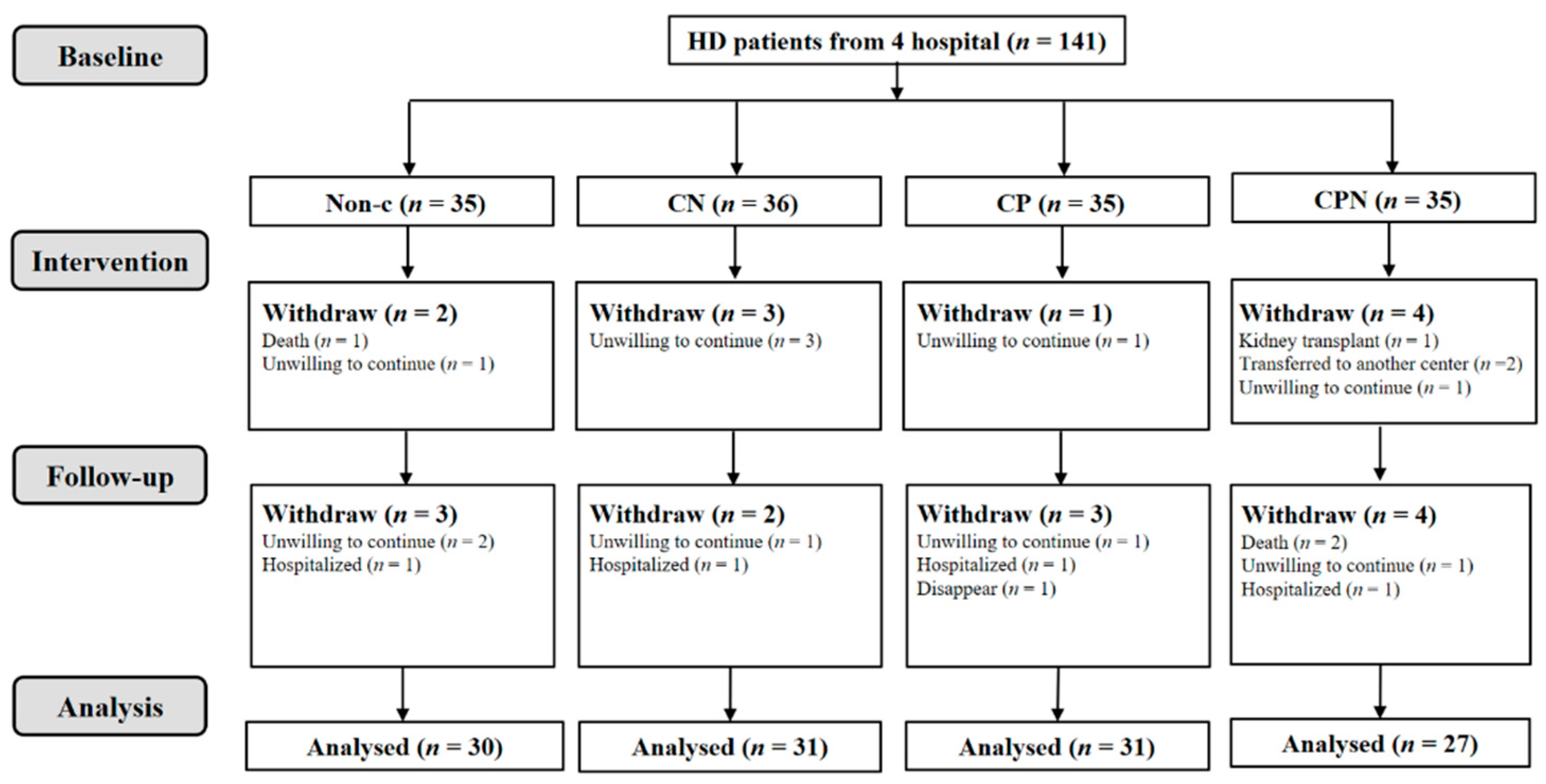
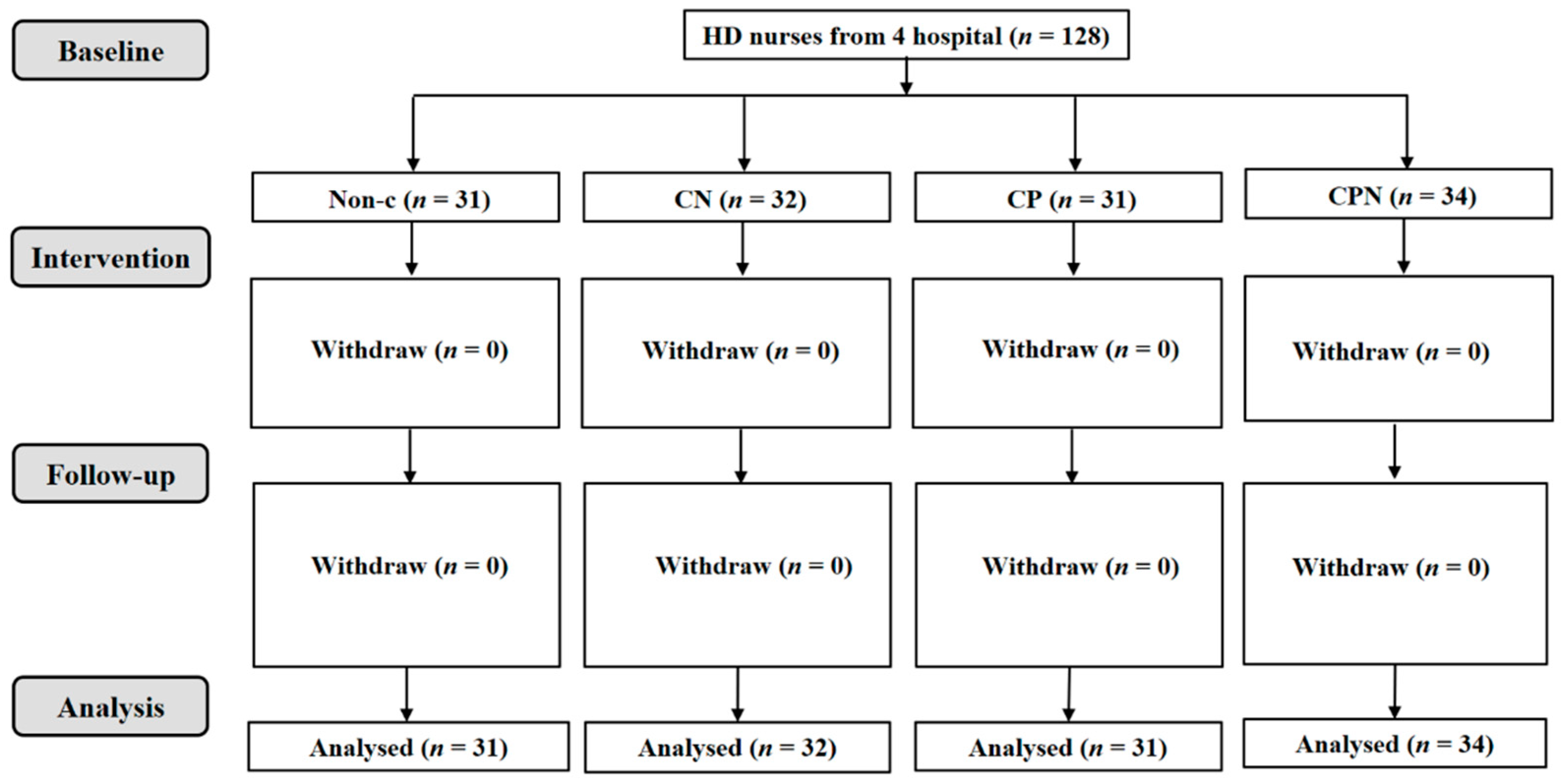
2.1. Study Design and Participants
2.2. Study Groups and Intervention Content
2.3. Patients’ Characteristics
2.4. Cardiovascular Risk Factors
2.5. Dietary Intake and Dietary Fat Quality
2.6. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. The Relationship between the h/H and CVD Risk Factors
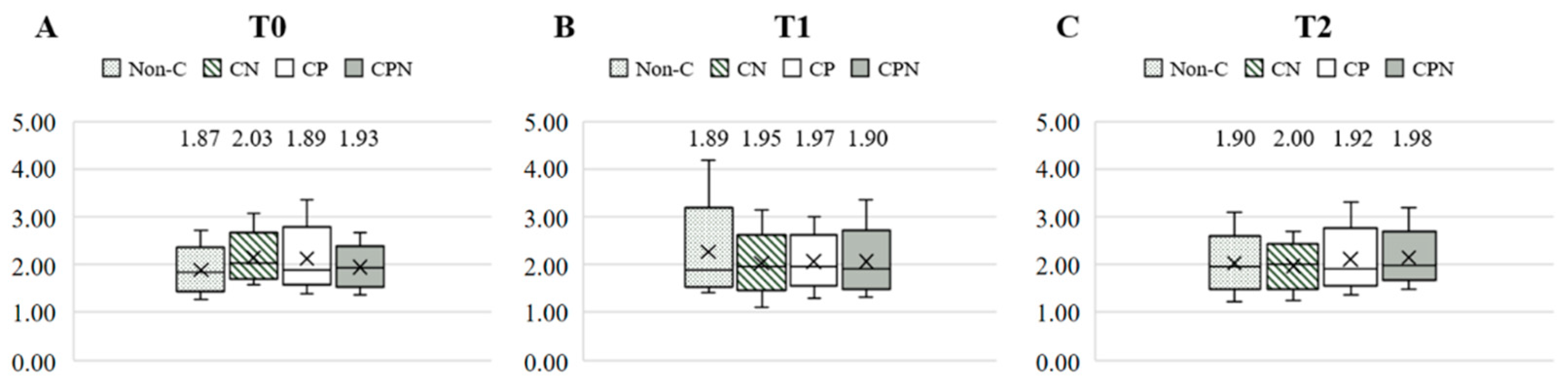
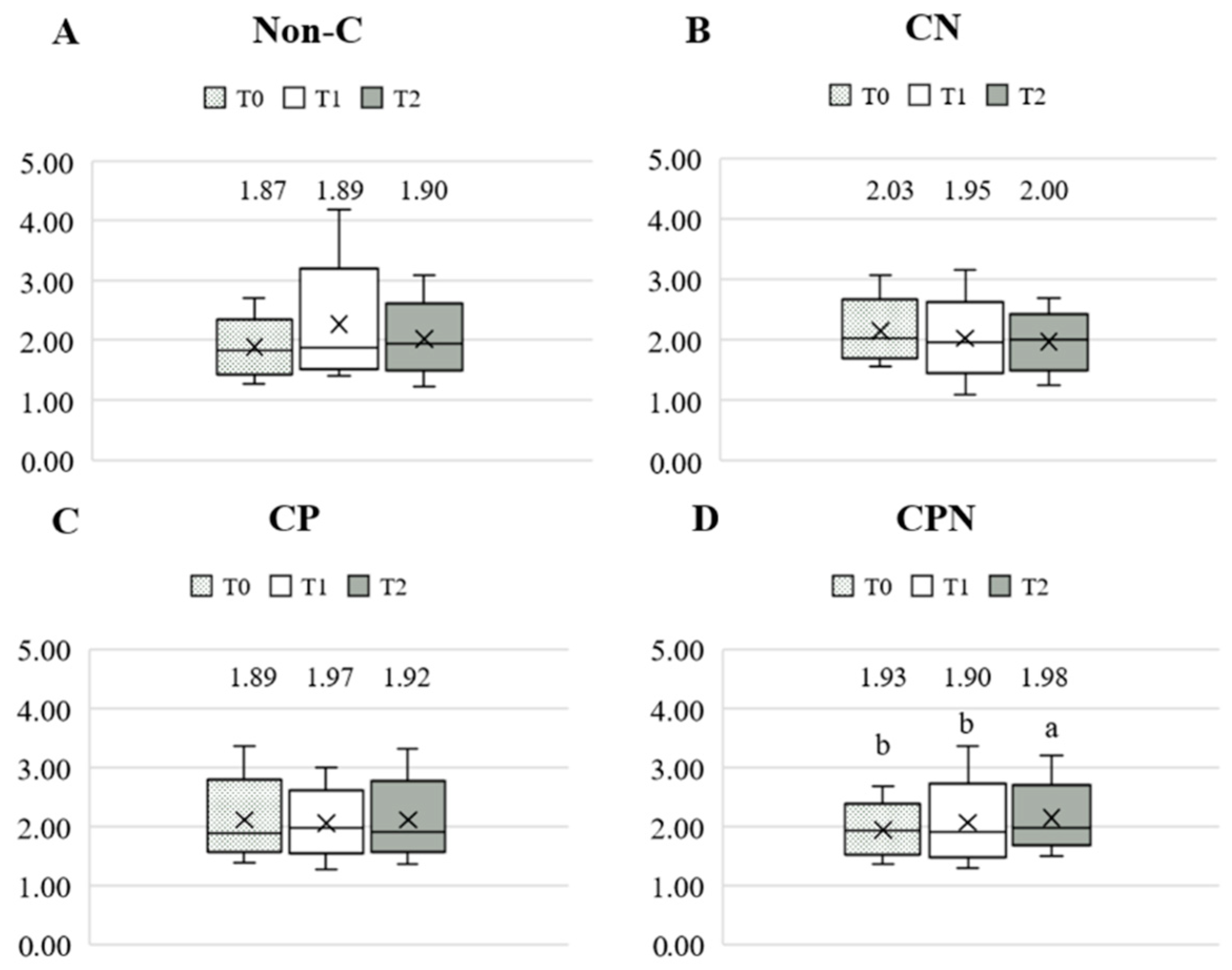
3.3. Dietary Fat Quality in Different Nutritional Education Models
3.4. CVD Risk Factors in Different Nutritional Education Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bello, A.K.; Okpechi, I.G.; Osman, M.A.; Cho, Y.; Htay, H.; Jha, V.; Wainstein, M.; Johnson, D.W. Epidemiology of haemodialysis outcomes. Nat. Rev. Nephrol. 2022, 18, 378–395. [Google Scholar] [CrossRef] [PubMed]
- CADTH Optimal Use Reports. In Dialysis Modalities for the Treatment of End-Stage Kidney Disease: A Health Technology Assessment—Project Protocol; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2016.
- Albakr, R.B.; Bargman, J.M. A Comparison of Hemodialysis and Peritoneal Dialysis in Patients with Cardiovascular Disease. Cardiol. Clin. 2021, 39, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Cozzolino, M.; Mangano, M.; Stucchi, A.; Ciceri, P.; Conte, F.; Galassi, A. Cardiovascular disease in dialysis patients. Nephrol. Dial. Transplant. 2018, 33, iii28–iii34. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, F.M.; Yilmaz, G.; Duranay, M.; Parpucu, H.; Senes, M.; Tekeli, N.; Yücel, D. Cardiovascular risk factors in hemodialysis and peritoneal dialysis patients. Scand. J. Clin. Lab. Investig. 2005, 65, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.; Liu, M.; Li, H.; Luo, Z.; Zhong, X.; Huang, J.; Liu, R.; He, F.; Fu, J. Mortality and Associated Risk Factors in Dialysis Patients with Cardiovascular Disease. Kidney Blood Press. Res. 2016, 41, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Steffen, L.M.; Selvin, E.; Rebholz, C.M. Diet quality, change in diet quality and risk of incident CVD and diabetes. Public Health Nutr. 2020, 23, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Torres, N.; Guevara-Cruz, M.; Velázquez-Villegas, L.A.; Tovar, A.R. Nutrition and Atherosclerosis. Arch. Med. Res. 2015, 46, 408–426. [Google Scholar] [CrossRef] [PubMed]
- Ravera, A.; Carubelli, V.; Sciatti, E.; Bonadei, I.; Gorga, E.; Cani, D.; Vizzardi, E.; Metra, M.; Lombardi, C. Nutrition and Cardiovascular Disease: Finding the Perfect Recipe for Cardiovascular Health. Nutrients 2016, 8, 363. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Lichtenstein, A.H.; Wu, J.H.Y.; Appel, L.J.; Creager, M.A.; Kris-Etherton, P.M.; Miller, M.; Rimm, E.B.; Rudel, L.L.; Robinson, J.G.; et al. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation 2017, 136, e1–e23. [Google Scholar] [CrossRef] [PubMed]
- Santos-Silva, J.; Bessa, R.J.B.; Santos-Silva, F. Effect of genotype, feeding system and slaughter weight on the quality of light lambs: II. Fatty acid composition of meat. Livest. Prod. Sci. 2002, 77, 187–194. [Google Scholar] [CrossRef]
- Moussavi Javardi, M.S.; Madani, Z.; Movahedi, A.; Karandish, M.; Abbasi, B. The correlation between dietary fat quality indices and lipid profile with Atherogenic index of plasma in obese and non-obese volunteers: A cross-sectional descriptive-analytic case-control study. Lipids Health Dis. 2020, 19, 213. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, H.; Sadeghi, M.; Amanpour, F.; Dadgari, A. Influence of nutritional education on hemodialysis patients’ knowledge and quality of life. Saudi J. Kidney Dis. Transpl. 2016, 27, 250–255. [Google Scholar] [PubMed]
- Nooriani, N.; Mohammadi, V.; Feizi, A.; Shahnazi, H.; Askari, G.; Ramezanzade, E. The Effect of Nutritional Education Based on Health Belief Model on Nutritional Knowledge, Health Belief Model Constructs, and Dietary Intake in Hemodialysis Patients. Iran. J. Nurs. Midwifery Res. 2019, 24, 372–378. [Google Scholar] [PubMed]
- Duong, T.V.; Tseng, I.-H.; Wong, T.-C.; Chen, H.-H.; Chen, T.-H.; Hsu, Y.-H.; Peng, S.-J.; Kuo, K.-L.; Liu, H.-C.; Lin, E.-T.; et al. Adaptation and Validation of Alternative Healthy Eating Index in Hemodialysis Patients (AHEI-HD) and Its Association with all-Cause Mortality: A Multi-Center Follow-Up Study. Nutrients 2019, 11, 1407. [Google Scholar] [CrossRef] [PubMed]
- Hager, M.R.; Narla, A.D.; Tannock, L.R. Dyslipidemia in patients with chronic kidney disease. Rev. Endocr. Metab. Disord. 2017, 18, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Tsimihodimos, V.; Dounousi, E.; Siamopoulos, K.C. Dyslipidemia in chronic kidney disease: An approach to pathogenesis and treatment. Am. J. Nephrol. 2008, 28, 958–973. [Google Scholar] [CrossRef]
- Chen, J.; Liu, H. Nutritional Indices for Assessing Fatty Acids: A Mini-Review. Int. J. Mol. Sci. 2020, 21, 5695. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Peterson, K.; Bourne, D.; Boundy, E. VA Evidence Synthesis Program Reports. In Evidence Brief: Use of Intradialytic Parenteral Nutrition (IDPN) to Treat Malnutrition in Hemodialysis Patients; Department of Veterans Affairs (US): Washington, DC, USA, 2018. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Non-C | CN | CP | CPN | p-Value | |
|---|---|---|---|---|---|---|
| n | 119 | 30 | 31 | 31 | 27 | |
| Age, y | 57.9 ± 10.0 | 60.10 ± 10.7 | 54.8 ± 10.9 | 59.6 ± 7.8 | 56.9 ± 10.5 | 0.13 |
| Male, n (%) | 83 (69.7) | 20 (66.7) | 21 (67.7) | 25 (80.6) | 17 (62.9) | 0.47 |
| Post-HD weight, kg | 64.1 ± 13.8 | 63.8 ± 17.0 | 63.0 ± 9.2 | 67.1 ± 13.9 | 62.4 ± 14.2 | 0.56 |
| Height, cm | 165.3 ± 8.1 | 164.8 ± 9.9 | 164.1 ± 6.3 | 168.0 ± 7.6 | 164.3 ± 8.0 | 0.20 |
| BMI, kg/m2 | 23.3 ± 3.9 | 23.2 ± 4.3 | 23.4 ± 3.3 | 23.7 ± 4.6 | 22.9 ± 3.5 | 0.88 |
| Body shape, n (%) | 0.46 | |||||
| Underweight | 6 (5.0) | 1 (3.3) | 0 (0.0) | 3 (9.7) | 2 (7.4) | |
| Normal | 73 (61.3) | 19 (63.3) | 22 (71.0) | 16 (51.6) | 16 (59.3) | |
| Overweight | 21 (17.7) | 6 (20.0) | 2 (6.5) | 7 (22.6) | 6 (22.2) | |
| Obesity | 19 (16.0) | 4 (13.3) | 7 (22.6) | 5 (16.1) | 3 (11.1) | |
| HD vintage, y | 6.0 ± 5.8 | 7.5 ± 7.1 | 5.3 ± 3.7 | 5.4 ± 5.9 | 5.5 ± 6.2 | 0.10 |
| CCI | 2.8 ± 0.8 | 3.0 ± 1.0 | 2.8 ± 0.8 | 2.7 ± 0.7 | 2.5 ± 0.8 | 0.21 |
| DM, n (%) | 47 (39.5) | 10 (30.0) | 12 (38.7) | 15 (48.4) | 10 (37.0) | 0.66 |
| HTN, n (%) | 65 (54.6) | 14 (46.7) | 18 (58.1) | 20 (64.5) | 13 (48.1) | 0.40 |
| CVD, n (%) | 45 (37.8) | 14 (46.7) | 13 (41.9) | 9 (29.0) | 9 (33.3) | 0.54 |
| Education status, n (%) | 0.76 | |||||
| Junior | 25 (21.0) | 4 (13.3) | 6 (19.4) | 9 (29.0) | 6 (22.2) | |
| Senior | 43 (36.1) | 13 (43.3) | 12 (38.7) | 11 (35.5) | 7 (25.9) | |
| Colleges | 44 (37.0) | 12 (40.0) | 12 (38.7) | 9 (29.0) | 11 (40.7) | |
| ≥Master | 7 (5.9) | 1 (3.3) | 1 (3.2) | 2 (6.5) | 3 (11.1) | |
| Incomes (NTD), n (%) | 0.23 | |||||
| No income | 48 (40.3) | 13 (43.3) | 10 (32.3) | 16 (53.3) | 9 (33.3) | |
| Below 20,000 | 13 (10.9) | 1 (3.3) | 6 (19.4) | 3 (9.7) | 3 (11.1) | |
| 20,000–30,000 | 11 (9.2) | 3 (10.0) | 2 (6.7) | 3 (9.7) | 3 (11.1) | |
| 30,000–50,000 | 22 (18.5) | 4 (13.3) | 9 (30.0) | 3 (9.7) | 6 (22.2) | |
| 50,000–70,000 | 7 (5.9) | 1 (3.3) | 2 (6.7) | 3 (9.7) | 1 (3.7) | |
| 70,000 or more | 11 (9.2) | 6 (20.0) | 2 (6.7) | 2 (6.7) | 1 (3.7) | |
| Alcohol use, n (%) | 0.60 | |||||
| Never dink | 92 (77.3) | 22 (73.3) | 25 (21.0) | 23 (74.2) | 22 (71.0) | |
| Once a month | 11 (9.2) | 4 (13.3) | 2 (6.5) | 3 (9.7) | 2 (6.5) | |
| 2~3 times/month | 5 (4.2) | 1 (3.3) | 1 (3.2) | 3 (9.7) | 0 (0.0) | |
| Once a week | 5 (4.2) | 1 (3.3) | 2 (6.5) | 2 (6.5) | 0 (0.0) | |
| 2~3 times/week | 4 (3.4) | 2 (6.7) | 0 (0.0) | 0 (0.0) | 2 (6.5) | |
| 4~5 times/week | 2 (1.7) | 0 (0.0) | 1 (3.2) | 0 (0.0) | 1 (3.2) | |
| Drink everyday | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Smoking status, n (%) | 0.83 | |||||
| Never smoke | 63 (52.9) | 16 (53.3) | 15 (48.4) | 15 (48.4) | 17 (63.0) | |
| Used to smoke | 40 (33.6) | 9 (30.0) | 11 (36.7) | 13 (41.9) | 7 (25.9) | |
| Smoker | 16 (13.5) | 5 (16.7) | 5 (16.1) | 3 (9.7) | 3 (11.1) |
| Variable | Model 1 | Model 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | p | B | 95% CI | p | |||||
| BMI, kg/m2 | −0.13 | −0.22 | - | −0.25 | 0.01 | −0.12 | −0.21 | - | −0.01 | 0.02 |
| pre-SBP, mmHg | 0.07 | −0.57 | - | 0.70 | 0.84 | 0.14 | −0.49 | - | 0.78 | 0.66 |
| pre-DBP, mmHg | −0.48 | −0.85 | - | −0.09 | 0.01 | −0.15 | −0.49 | - | 0.19 | 0.37 |
| Alb, g/dL | −0.003 | −0.01 | - | 0.01 | 0.54 | 0.002 | −0.00 | - | 0.08 | 0.95 |
| HbA1C, % | 0.34 | −0.04 | - | 0.73 | 0.08 | 0.24 | −0.13 | - | 0.60 | 0.20 |
| TG, mg/dL | −1.43 | −5.22 | - | 2.35 | 0.45 | −2.11 | −6.00 | - | 1.77 | 0.28 |
| TC, mg/dL | 0.24 | −0.73 | - | 1.21 | 0.62 | −0.03 | −0.99 | - | 0.92 | 0.95 |
| LDL-C, mg/dL | −0.33 | −1.18 | - | 0.53 | 0.45 | −0.48 | −1.36 | - | 0.40 | 0.28 |
| HDL-C, mg/dL | 0.77 | 0.28 | - | 1.25 | <0.01 | 0.66 | 0.16 | - | 1.15 | <0.01 |
| Hgb, mg/dL | −0.01 | −0.04 | - | 0.01 | 0.47 | 0.005 | −0.02 | - | 0.03 | 0.73 |
| Ferritin, ng/mL | −0.25 | −11.1 | - | 10.6 | 0.96 | −10.61 | −21.12 | - | −0.11 | 0.05 |
| TSAT, % | 0.07 | −0.24 | - | 0.39 | 0.64 | 0.04 | −0.27 | - | 0.36 | 0.79 |
| hsCRP, mg/dL | −0.005 | −0.02 | - | 0.01 | 0.66 | −0.007 | −0.02 | - | 0.01 | 0.52 |
| Hcy, umol/L | −0.12 | −0.36 | - | 0.12 | 0.33 | −0.03 | −0.23 | - | 0.22 | 0.97 |
| Serum K, mEq/L | 0.008 | −0.01 | - | 0.23 | 0.47 | 0.01 | −0.01 | - | 0.02 | 0.34 |
| Serum Ca, mg/dL | −0.003 | −0.02 | - | 0.01 | 0.73 | 0.002 | −0.01 | - | 0.02 | 0.83 |
| Serum P, mg/dL | −0.02 | −0.06 | - | 0.00 | 0.08 | −0.006 | −0.03 | - | 0.02 | 0.72 |
| Ca-P product | −0.28 | −0.62 | - | 0.06 | 0.11 | −0.04 | −0.38 | - | 0.31 | 0.82 |
| Model 1 | Model 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | p-Value | B | 95% CI | p-Value | |||||
| h/H | ||||||||||
| Non-C | Reference | Reference | ||||||||
| CN | −0.05 | −0.10 | - | 0.01 | 0.08 | −0.06 | −0.11 | - | −0.01 | 0.02 |
| CP | −0.03 | −0.11 | - | 0.05 | 0.49 | −0.02 | −0.12 | - | 0.09 | 0.76 |
| CPN | 0.10 | 0.02 | - | 0.18 | <0.01 | 0.11 | 0.11 | - | 0.02 | <0.01 |
| CVD Risk Factors | Model 1 | CVD Risk Factors | Model 1 | CVD Risk Factors | Model 1 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | p-Value | B | 95% CI | p-Value | B | 95% CI | p-Value | |||||||||
| BMI, kg/m2 | TC, mg/dL | hsCRP, mg/dL | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −0.04 | −0.25 | - | 0.17 | 0.72 | CN | −5.19 | −11.65 | - | 1.26 | 0.11 | CN | 0.07 | −0.11 | - | 0.25 | 0.45 |
| CP | 0.01 | −0.20 | - | 0.22 | 0.94 | CP | −11.36 | −17.63 | - | −5.09 | <0.01 | CP | 0.04 | −0.13 | - | 0.22 | 0.62 |
| CPN | −0.08 | −0.31 | - | 0.16 | 0.51 | CPN | −7.97 | −14.25 | - | −1.69 | 0.01 | CPN | −0.03 | −0.31 | - | 0.26 | 0.85 |
| Pre-SBP, mmHg | LDL-C, mg/dL | Hcy, umol/L | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −4.18 | −8.43 | - | 0.07 | 0.05 | CN | −0.40 | −6.02 | - | 5.22 | 0.88 | CN | −0.51 | −2.32 | - | 1.29 | 0.57 |
| CP | −3.40 | −8.04 | - | 1.25 | 0.15 | CP | 0.44 | −5.54 | - | 6.43 | 0.88 | CP | −2.13 | −3.81 | - | −0.43 | 0.01 |
| CPN | −2.57 | −7.51 | - | 2.37 | 0.30 | CPN | −2.27 | −8.49 | - | 3.95 | 0.47 | CPN | −0.53 | −2.28 | - | 1.22 | 0.55 |
| Pre-DBP, mmHg | HDL-C, mg/dL | Serum K, mEq/L | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −0.42 | −2.25 | - | 1.42 | 0.65 | CN | 3.16 | 1.13 | - | 5.19 | <0.01 | CN | 0.12 | 0.12 | - | 0.14 | 0.86 |
| CP | −0.04 | −1.91 | - | 1.84 | 0.97 | CP | 0.61 | −1.46 | - | 2.68 | 0.56 | CP | 0.01 | 0.12 | - | 0.13 | 0.99 |
| CPN | 0.22 | −2.37 | - | 2.81 | 0.86 | CPN | 3.68 | 1.43 | - | 5.92 | <0.01 | CPN | −0.09 | −0.22 | - | 0.04 | 0.18 |
| Alb, g/dL | Hgb, mg/dL | Serum Ca, mg/dL | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | 0.0 | 0.0 | - | 0.0 | - | CN | −0.14 | −0.42 | - | −0.42 | 0.32 | CN | −0.10 | −0.22 | - | 0.02 | 0.11 |
| CP | 0.0 | 0.0 | - | 0.0 | - | CP | −0.01 | −0.21 | - | 0.20 | 0.96 | CP | −0.03 | −0.18 | - | 0.11 | 0.65 |
| CPN | 0.0 | 0.0 | - | 0.0 | - | CPN | −0.21 | −0.55 | - | 0.13 | 0.22 | CPN | −0.01 | −0.15 | - | 0.14 | 0.94 |
| HbA1c, % | Ferritin, ng/mL | Serum P, mg/dL | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | 0.03 | −0.28 | - | 0.35 | 0.84 | CN | 31.23 | −71.11 | - | 133.57 | 0.55 | CN | −0.16 | −0.43 | - | 0.12 | 0.26 |
| CP | −0.03 | −0.03 | - | 0.34 | 0.86 | CP | 46.54 | −28.16 | - | 121.24 | 0.22 | CP | 0.12 | −0.13 | - | 0.84 | 0.35 |
| CPN | −0.04 | −0.04 | - | 0.18 | 0.44 | CPN | 52.28 | −42.38 | - | 146.93 | 0.27 | CPN | 0.07 | −0.19 | - | 1.22 | 0.59 |
| TG, mg/dL | TSAT, % | Ca-P product | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −33.04 | −81.23 | - | 15.14 | 0.17 | CN | −2.03 | −5.75 | - | 1.70 | 0.28 | CN | −1.77 | −4.41 | - | 0.88 | 0.19 |
| CP | −33.11 | −67.58 | - | 1.36 | 0.06 | CP | 2.40 | −0.78 | - | 5.57 | 0.13 | CP | 1.11 | −1.48 | - | 3.69 | 0.40 |
| CPN | 2.20 | −29.58 | - | 33.68 | 0.89 | CPN | −0.67 | −4.29 | - | 2.95 | 0.71 | CPN | 0.62 | −2.29 | - | 3.53 | 0.67 |
| CVD Risk Factors | Model 2 | CVD Risk Factors | Model 2 | CVD Risk Factors | Model 2 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | 95% CI | p-Value | B | 95% CI | p-Value | B | 95% CI | p-Value | |||||||||
| BMI, kg/m2 | TC, mg/dL | hsCRP, mg/dL | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −0.06 | −0.27 | - | 0.15 | 0.56 | CN | −5.64 | −12.40 | - | 1.12 | 0.10 | CN | 0.07 | −0.11 | - | 0.25 | 0.44 |
| CP | −0.05 | −0.24 | - | 0.14 | 0.32 | CP | −14.11 | −21.01 | - | −7.20 | <0.01 | CP | 0.04 | −0.16 | - | 0.25 | 0.68 |
| CPN | −0.08 | −0.31 | - | 0.16 | 0.51 | CPN | −6.99 | −13.06 | - | −0.92 | 0.02 | CPN | −0.03 | −0.31 | - | 0.26 | 0.86 |
| Pre-SBP, mmHg | LDL-C, mg/dL | Hcy, umol/L | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −6.05 | −10.67 | - | −1.42 | 0.01 | CN | −0.22 | −6.23 | - | 5.80 | 0.94 | CN | −0.51 | −2.34 | - | 1.31 | 0.58 |
| CP | −3.19 | −8.89 | - | 2.51 | 0.27 | CP | 1.29 | −5.37 | - | 7.95 | 0.70 | CP | −2.07 | −3.91 | - | −0.23 | 0.02 |
| CPN | −3.13 | −8.48 | - | 2.22 | 0.25 | CPN | −0.85 | −7.41 | - | 5.80 | 0.80 | CPN | −0.59 | −2.29 | - | 1.18 | 0.52 |
| Pre-DBP, mmHg | HDL-C, mg/dL | Serum K, mEq/L | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −0.79 | −2.67 | - | 1.09 | 0.41 | CN | 2.76 | 0.22 | - | 5.30 | 0.03 | CN | 0.03 | −0.10 | - | 0.16 | 0.64 |
| CP | 0.10 | −1.90 | - | 2.09 | 0.92 | CP | −0.79 | −3.51 | - | 1.93 | 0.57 | CP | 0.02 | −0.12 | - | 0.15 | 0.82 |
| CPN | 0.14 | −2.54 | - | 2.81 | 0.92 | CPN | 3.10 | 0.16 | - | 6.03 | 0.03 | CPN | −0.09 | −0.22 | - | 0.04 | 0.17 |
| Alb, g/dL | Hgb, mg/dL | Serum Ca, mg/dL | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | 0.0 | 0.0 | - | 0.0 | - | CN | −0.14 | −0.42 | - | 0.14 | 0.34 | CN | −0.07 | −0.18 | - | 0.04 | 0.21 |
| CP | 0.0 | 0.0 | - | 0.0 | - | CP | 0.02 | −0.18 | - | 0.22 | 0.84 | CP | 0.01 | −0.17 | - | 0.18 | 0.94 |
| CPN | 0.0 | 0.0 | - | 0.0 | - | CPN | −0.21 | −0.53 | - | 0.12 | 0.22 | CPN | −0.01 | −0.15 | - | 0.14 | 0.94 |
| HbA1C, % | Ferritin, ng/mL | Serum P, mg/dL | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | 0.02 | −0.25 | - | 0.31 | 0.84 | CN | 22.17 | −74.95 | - | 119.28 | 0.65 | CN | −0.13 | −0.41 | - | 0.15 | 0.38 |
| CP | 0.03 | −0.31 | - | 0.37 | 0.85 | CP | 51.30 | −16.37 | - | 121.97 | 0.15 | CP | 0.12 | −0.18 | - | 0.43 | 0.43 |
| CPN | −0.03 | −0.36 | - | 0.30 | 0.86 | CPN | 48.17 | −37.63 | - | 133.97 | 0.27 | CPN | 0.05 | −0.22 | - | 0.32 | 0.73 |
| TG, mg/dL | TSAT, % | Ca-P product | |||||||||||||||
| Non-C | Reference | Non-C | Reference | Non-C | Reference | ||||||||||||
| CN | −25.53 | −82.11 | - | 31.04 | 0.37 | CN | −2.244 | −6.01 | - | 1.54 | 0.24 | CN | −1.40 | −4.14 | - | 1.34 | 0.31 |
| CP | −37.54 | −86.74 | - | 11.84 | 0.13 | CP | 1.87 | −1.38 | - | 5.12 | 0.26 | CP | 1.43 | −1.71 | - | 4.57 | 0.37 |
| CPN | 7.13 | −30.06 | - | 44.33 | 0.70 | CPN | −0.72 | −4.37 | - | 2.93 | 0.70 | CPN | 0.41 | −2.51 | - | 3.34 | 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.-L.; Chen, Y.-H.; Duong, T.V.; Wong, T.-C.; Chen, H.-H.; Chen, T.-H.; Hsu, Y.-H.; Peng, S.-J.; Yang, S.-H. The Effect of Different Nutritional Education Models on Reducing Cardiovascular Disease Risk Factors by Improving Dietary Fat Quality in Hemodialysis Patients. Nutrients 2022, 14, 3840. https://doi.org/10.3390/nu14183840
Liu W-L, Chen Y-H, Duong TV, Wong T-C, Chen H-H, Chen T-H, Hsu Y-H, Peng S-J, Yang S-H. The Effect of Different Nutritional Education Models on Reducing Cardiovascular Disease Risk Factors by Improving Dietary Fat Quality in Hemodialysis Patients. Nutrients. 2022; 14(18):3840. https://doi.org/10.3390/nu14183840
Chicago/Turabian StyleLiu, Wan-Lin, Yun-Han Chen, Tuyen Van Duong, Te-Chih Wong, Hsi-Hsien Chen, Tso-Hsiao Chen, Yung-Ho Hsu, Sheng-Jeng Peng, and Shwu-Huey Yang. 2022. "The Effect of Different Nutritional Education Models on Reducing Cardiovascular Disease Risk Factors by Improving Dietary Fat Quality in Hemodialysis Patients" Nutrients 14, no. 18: 3840. https://doi.org/10.3390/nu14183840