

Adequacy of Nutritional Intakes during the Year after Critical Illness: An Observational Study in a Post-ICU Follow-Up Clinic
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
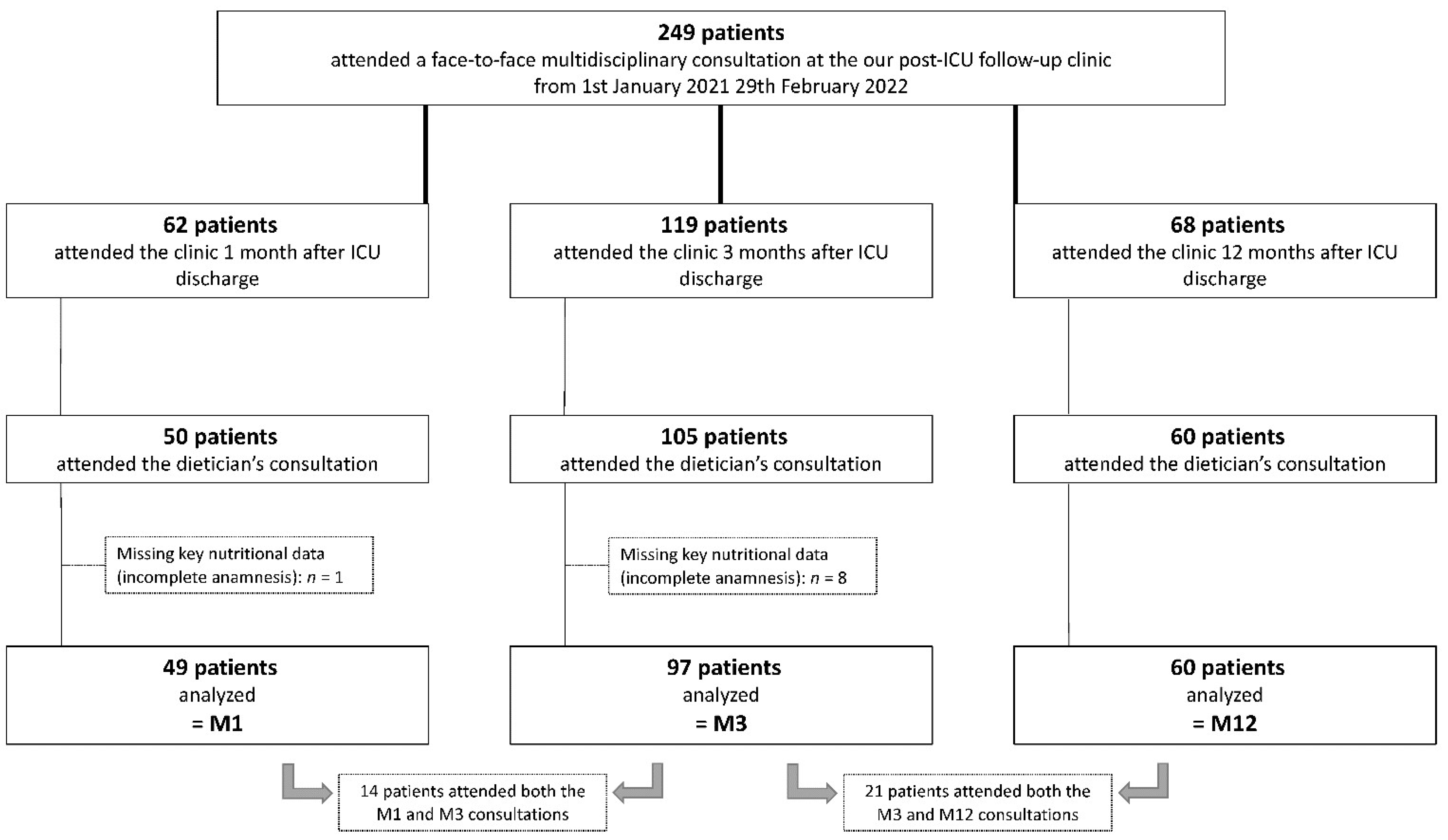
2.1. Population
2.2. Assessment of Nutritional Intakes
2.3. Calculation of Nutritional Targets
2.4. Other Clinical Data
2.5. Biological Data
2.6. Study Outcomes and Analysis
2.7. Statistical Analysis
3. Results
3.1. Patients
3.2. Nutritional Data
3.3. Outcome Analysis According to Nutritional Adequacy
3.4. Nutritional Data in Patients Who Attended More Than One Consultation
3.5. Nutritional Intakes in Older Adults Compared to Younger Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgment
Conflicts of Interest
References
- Puthucheary, Z.A.; Rawal, J.; McPhail, M.; Connolly, B.; Ratnayake, G.; Chan, P.; Hopkinson, N.S.; Phadke, R.; Dew, T.; Sidhu, P.S.; et al. Acute skeletal muscle wasting in critical illness. JAMA 2013, 310, 1591–1600. [Google Scholar] [CrossRef]
- van Zanten, A.R.H.; De Waele, E.; Wischmeyer, P.E. Nutrition therapy and critical illness: Practical guidance for the ICU, post-ICU, and long-term convalescence phases. Crit. Care 2019, 23, 368. [Google Scholar] [CrossRef] [PubMed]
- Ridley, E.J.; Chapple, L.S.; Chapman, M.J. Nutrition intake in the post-ICU hospitalization period. Curr. Opin. Clin. Nutr. Metab. Care 2020, 23, 111–115. [Google Scholar] [CrossRef]
- Moisey, L.L.; Pikul, J.; Keller, H.; Yeung, C.Y.E.; Rahman, A.; Heyland, D.K.; Mourtzakis, M. Adequacy of Protein and Energy Intake in Critically Ill Adults Following Liberation From Mechanical Ventilation is Dependent on Route of Nutrition Delivery. Nutr. Clin. Pract. 2021, 36, 201–212. [Google Scholar] [CrossRef]
- Peterson, S.J.; Tsai, A.A.; Scala, C.M.; Sowa, D.C.; Sheean, P.M.; Braunschweig, C.L. Adequacy of oral intake in critically ill patients 1 week after extubation. J. Am. Diet Assoc. 2010, 110, 427–433. [Google Scholar] [CrossRef]
- Jarden, R.J.; Sutton-Smith, L.; Boulton, C. Oral intake evaluation in patients following critical illness: An ICU cohort study. Nurs. Crit. Care 2018, 23, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Ridley, E.J.; Parke, R.L.; Davies, A.R.; Bailey, M.; Hodgson, C.; Deane, A.M.; McGuinness, S.; Cooper, D.J. What Happens to Nutrition Intake in the Post-Intensive Care Unit Hospitalization Period? An Observational Cohort Study in Critically Ill Adults. J. Parenter. Enter. Nutr. 2019, 43, 88–95. [Google Scholar] [CrossRef]
- Haines, K.J.; Hibbert, E.; Leggett, N.; Boehm, L.M.; Hall, T.; Bakhru, R.N.; Bastin, A.J.; Butcher, B.W.; Eaton, T.L.; Harris, W.; et al. Transitions of Care After Critical Illness-Challenges to Recovery and Adaptive Problem Solving. Crit. Care Med. 2021, 49, 1923. [Google Scholar] [CrossRef]
- Meyer, J.; Brett, S.J.; Waldmann, C. Should ICU clinicians follow patients after ICU discharge? Yes. Intensive Care Med. 2018, 44, 1539–1541. [Google Scholar] [CrossRef]
- Sidiras, G.; Patsaki, I.; Karatzanos, E.; Dakoutrou, M.; Kouvarakos, A.; Mitsiou, G.; Routsi, C.; Stranjalis, G.; Nanas, S.; Gerovasili, V. Long term follow-up of quality of life and functional ability in patients with ICU acquired Weakness—A post hoc analysis. J. Crit. Care 2019, 53, 223–230. [Google Scholar] [CrossRef]
- van Beusekom, I.; Bakhshi-Raiez, F.; de Keizer, N.F.; van der Schaaf, M.; Busschers, W.B.; Dongelmans, D.A. Healthcare costs of ICU survivors are higher before and after ICU admission compared to a population based control group: A descriptive study combining healthcare insurance data and data from a Dutch national quality registry. J. Crit. Care 2018, 44, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Bear, D.E.; Wandrag, L.; Merriweather, J.L.; Connolly, B.; Hart, N.; Grocott, M.P.W. The role of nutritional support in the physical and functional recovery of critically ill patients: A narrative review. Crit. Care 2017, 21, 226. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Singer, P.; Blaser, A.R.; Berger, M.M.; Alhazzani, W.; Calder, P.C.; Casaer, M.P.; Hiesmayr, M.; Mayer, K.; Montejo, J.C.; Pichard, C.; et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin. Nutr. 2019, 38, 48–79. [Google Scholar] [CrossRef] [PubMed]
- Fadeur, M.; Preiser, J.C.; Verbrugge, A.M.; Misset, B.; Rousseau, A.F. Oral Nutrition during and after Critical Illness: SPICES for Quality of Care! Nutrients 2020, 12, 3509. [Google Scholar] [CrossRef]
- Kistler, B.M.; Moore, L.W.; Benner, D.; Biruete, A.; Boaz, M.; Brunori, G.; Chen, J.; Drechsler, C.; Guebre-Egziabher, F.; Hensley, M.K.; et al. The International Society of Renal Nutrition and Metabolism Commentary on the National Kidney Foundation and Academy of Nutrition and Dietetics KDOQI Clinical Practice Guideline for Nutrition in Chronic Kidney Disease. J. Ren. Nutr. 2021, 31, 116–120.e1. [Google Scholar] [CrossRef]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Kyle, U.G.; Schutz, Y.; Dupertuis, Y.M.; Pichard, C. Body composition interpretation. Contributions of the fat-free mass index and the body fat mass index. Nutrition 2003, 19, 597–604. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Salisbury, L.G.; Merriweather, J.L.; Walsh, T.S. The development and feasibility of a ward-based physiotherapy and nutritional rehabilitation package for people experiencing critical illness. Clin. Rehabil. 2010, 24, 489–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapple, L.S.; Weinel, L.M.; Abdelhamid, Y.A.; Summers, M.J.; Nguyen, T.; Kar, P.; Lange, K.; Chapman, M.J.; Deane, A.M. Observed appetite and nutrient intake three months after ICU discharge. Clin. Nutr. 2019, 38, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Merriweather, J.; Smith, P.; Walsh, T. Nutritional rehabilitation after ICU—does it happen: A qualitative interview and observational study. J. Clin. Nurs. 2014, 23, 654–662. [Google Scholar] [CrossRef]
- Merriweather, J.L.; Griffith, D.M.; Walsh, T.S. Appetite during the recovery phase of critical illness: A cohort study. Eur. J. Clin. Nutr. 2018, 72, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Jeschke, M.G.; Gauglitz, G.G.; Kulp, G.A.; Finnerty, C.C.; Williams, F.N.; Kraft, R.; Suman, O.E.; Mlcak, R.P.; Herndon, D.N. Long-term persistance of the pathophysiologic response to severe burn injury. PLoS ONE 2011, 6, e21245. [Google Scholar] [CrossRef] [PubMed]
- Delsoglio, M.; Dupertuis, Y.M.; Oshima, T.; van der Plas, M.; Pichard, C. Evaluation of the accuracy and precision of a new generation indirect calorimeter in canopy dilution mode. Clin. Nutr. 2019, 39, 1927–1934. [Google Scholar] [CrossRef] [PubMed]
- Oshima, T.; Delsoglio, M.; Dupertuis, Y.M.; Singer, P.; De Waele, E.; Veraar, C.; Heidegger, C.-H.; Wernermann, J.; Wischmeyer, P.E.; Berger, M.M.; et al. The clinical evaluation of the new indirect calorimeter developed by the ICALIC project. Clin. Nutr. 2020, 39, 3105–3111. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Joris, M.; Pincemail, J.; Colson, C.; Joris, J.; Calmes, D.; Cavalier, E.; Misset, B.; Guiot, J.; Minguet, G.; Rousseau, A.-F. Exercise Limitation after Critical Versus Mild COVID-19 Infection: A Metabolic Perspective. J. Clin. Med. 2022, 11, 4322. [Google Scholar] [CrossRef]
- Ripani, U.; Bisaccia, M.; Meccariello, L. Dexamethasone and Nutraceutical Therapy Can Reduce the Myalgia Due to COVID-19—A Systemic Review of the Active Substances that Can Reduce the Expression of Interlukin-6. Med. Arch. 2022, 76, 66–71. [Google Scholar] [CrossRef]
- Romani, M.; Berger, M.M.; D’Amelio, P. From the Bench to the Bedside: Branched Amino Acid and Micronutrient Strategies to Improve Mitochondrial Dysfunction Leading to Sarcopenia. Nutrients 2022, 14, 483. [Google Scholar] [CrossRef] [PubMed]
- Viana, M.V.; Becce, F.; Pantet, O.; Schmidt, S.; Bagnoud, G.; Thaden, J.J.; Ten Have, G.A.M.; Engelen, M.P.K.J.; Voidey, A.; Deutz, N.E.P.; et al. Impact of beta-hydroxy-beta-methylbutyrate (HMB) on muscle loss and protein metabolism in critically ill patients: A RCT. Clin. Nutr. 2021, 40, 4878–4887. [Google Scholar] [CrossRef] [PubMed]
- Davies, T.W.; van Gassel, R.J.J.; van de Poll, M.; Gunst, J.; Casaer, M.P.; Christopher, K.B.; Preiser, J.C.; Hill, A.; Gundogan, K.; Reintam-Blaser, A.; et al. Core outcome measures for clinical effectiveness trials of nutritional and metabolic interventions in critical illness: An international modified Delphi consensus study evaluation (CONCISE). Crit. Care 2022, 26, 240. [Google Scholar] [CrossRef]
- Vlake, J.H.; Wils, E.J.; van Bommel, J.; Gommers, D.; van Genderen, M.E. Familiarity with the post-intensive care syndrome among general practitioners and opportunities to improve their involvement in ICU follow-up care. Intensive Care Med. 2022, 48, 1090–1092. [Google Scholar] [CrossRef]
- Rousseau, A.F.; Prescott, H.C.; Brett, S.J.; Weiss, B.; Azoulay, E.; Creteur, J.; Latronico, N.; Hough, C.L.; Weber-Carstens, S.; Vincent, J.-L.; et al. Long-term outcomes after critical illness: Recent insights. Crit. Care 2021, 25, 108. [Google Scholar] [CrossRef]
- Cawood, A.L.; Elia, M.; Stratton, R.J. Systematic review and meta-analysis of the effects of high protein oral nutritional supplements. Ageing Res. Rev. 2012, 11, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Stratton, R.J.; Hebuterne, X.; Elia, M. A systematic review and meta-analysis of the impact of oral nutritional supplements on hospital readmissions. Ageing Res. Rev. 2013, 12, 884–897. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, C.; Smith, R.; Gibbs, M.; Weekes, C.E.; Emery, P.W. Quality of the Evidence Supporting the Role of Oral Nutritional Supplements in the Management of Malnutrition: An Overview of Systematic Reviews and Meta-Analyses. Adv. Nutr. 2021, 12, 503–522. [Google Scholar] [CrossRef]


{kind=link}
| Data | M1 n = 49 | M3 n = 97 | M12 n = 60 | |
|---|---|---|---|---|
| Age, year | 60 [51–67] | 62 [54–70] | 61.5 [52–68] | |
| Male, n (%) | 32 (65.3) | 59 (60.8) | 41 (68.3) | |
| SAPS II | 28.5 [24–39.5] | 31 [25–49] | 34 [25.5–49] | |
| Admission failure, n (%) | Cardiovascular | 22 (44.9) | 28 (28.9) | 6 (10) |
| Pulmonary | 21 (42.9) | 49 (50.5) | 51 (85) | |
| Neurologic | 3 (6.1) | 9 (9.3) | 2 (3.3) | |
| Digestive | 1 (2) | 2 (2.1) | 0 | |
| Trauma | 0 | 1 (1) | 0 | |
| Other | 2 (4.1) | 8 (8.2) | 1 (1.7) | |
| Mechanical ventilation, n (%) | 24 (49) | 57 (58.8) | 47 (78.3) | |
| Duration of mechanical ventilation, day | 2 [1–7] | 8 [2.5–19.5] | 13 [8–24] | |
| ICU LOS, day | 7.5 [7–10] | 11 [8–20] | 16 [11–27] | |
| Hospital LOS, day | 21.5 [13.5–38.8] | 30 [19–51] | 34.5 [22–50.2] | |
| Socioeconomic problems, n (%) | 2/31 (6.5) | 3/63 (4.8) | 2/42 (4.8) | |
| Data | M1 n = 49 | M3 n = 97 | M12 n = 60 | |
|---|---|---|---|---|
| Initial weight, kg | 88 [69–102] | 84 [70–95] | 92 [74.5–105] | |
| Weight during the week after ICU discharge, kg | 79.5 [67.3–92.8] | 71.9 [62–86] | 81.8 [64.5–90.4] | |
| Actual weight, kg | 81.5 [66.2–93.5] | 77 [67.5–90] | 90 [76.2–101] | |
| Actual weight considered for nutritional calculation, kg | 77.1 [66.2–84.5] | 73 [65.2–82] | 79.1 [68.7–84.3] | |
| BMI, kg/m2 | 26.6 [22.7–30.9] | 26.7 [23.7–31.1] | 31.6 [26.8–34.2] | |
| Fat mass, % of total body weight | Males | 27.5 [24.3–32.8] | 28.6 [24.7–32.4] | 28.7 [23.5–32.4] |
| Females | 41.4 [29.1–48.4] | 41.6 [34.4–45.6] | 38.8 [33.5–43.6] | |
| MUST score ≥ 2, n (%) | 5 (10.2) | 4 (4.1) | 0 | |
| GLIM, n (%) | Moderate malnutrition | 16 (32.7) | 5 (5.2) | 1 (1.7) |
| Severe malnutrition | 11 (22.4) | 5 (5.2) | 0 | |
| Swallowing problems, n (%) | 3 (6.1) | 14 (14.4) | 5 (8.3) | |
| Loss of appetite, n (%) | 18 (36.7) | 29 (30) | 7 (11.6) | |
| Energy intakes, kcal/day | 1800 [1530–2250] | 2000 [1619–2200] | 2100 (1778–2400] | |
| Energy intakes, kcal/kg/day | 24.5 [21.2–29.3] | 26.1 [23–29.7] | 27 [23.1–29.1] | |
| Energy healthy target (FAO/WHO/UNU), kcal/day | 2518 [2238–2810] | 2392 [2169–2756] | 2425 [2239–2763] | |
| Energy intakes, % of healthy target | 73.2 [63.3–86.3] | 79.3 [69.3–89.3] | 82.7 [70.6–93.7] | |
| Energy ICU target (25 kcal/kg/day), kcal/day | 1928 [1656–2113] | 1825 [1631–2050] | 1980 [1735–2139] | |
| Energy post-ICU target (35 kcal/kg/day), kcal/day | 2699 [2319–2958] | 2555 [2284–2870] | 2772 [2428–2995] | |
| Protein intakes, g/day | 70 [50–87.4] | 80 [60–90] | 86.2 [68.9–110] | |
| Protein intakes, g/kg/day | 0.94 [0.7–1.22] | 1.07 [0.8–1.2] | 1.11 [0.9–1.33] | |
| Protein healthy target (0.8 g/kg/day), g/day | 61.7 [53–67.6] | 58.4 [52.2–65.6] | 63.4 [55.4–68.8] | |
| Protein intakes, % of healthy target | 117.6 [87.2–152.3] | 134.1 [99.7–155.7] | 134.6 [109.9–158.2] | |
| Protein ICU target (1.3 g/kg/day or 2 g/kg/day if obese, or 0.8 g/kg/day if CKD), g/day | 91.2 [70.2–122.2] | 92.6 [74.1–132.5] | 123.3 [83.4–164.1] | |
| Protein post-ICU target (1.5 g/kg/day or 2 g/kg/day if obese or 0.8 g/kg/day if CKD), g/day | 99.7 [74.4–137.2] | 106.8 [85.5–139.5] | 136.8 [94.7–164.1] | |
| Protein intakes, % of post-ICU target | 67.9 [46.5–95.8] | 68.5 [48.8–99.3] | 71.7 [44.9–95.1] | |
| Barthel index | 100 [100–100] | 100 [100–100] | 100 [100–100] | |
| Handgrip strength, kg | Males | 33.5 [29.7–41] | 35 [29–42] | 36 [25–43.5] |
| Females | 22 [18.5–25.8] | 19 [14–24] | 33.5 [21.5–43] | |
| Blood Analysis | Reference Ranges | M1 n = 49 | M3 n = 97 | M12 n = 60 |
|---|---|---|---|---|
| C-reactive protein (CRP), mg/L | 0–5 | 3.1 [1.6–19.6] | 2.5 [1–5.1] | 2.4 [1.2–4.6] |
| Albumin, g/L | ≤ 60 years: 35–52 >60 years: 32–46 | 41 [39–43] | 43 [41–44] | 44 [43–46] |
| Prealbumin, g/L | 0.2–0.4 | 0.29 [0.24–0.34] | 0.28 [0.25–0.32] | 0.3 [0.25–0.34] |
| Triglycerides, mg/dL | <175 | 163 [124–202.5] | 163 [113.8–221.8] | 172.5 [108–244.8] |
| 25OH-D, ng/mL | 20–50 | 25.7 [16.4–37.7] | 30 [20.7–37.6] | 26.8 [17.5–33.9] |
| Creatinine, mg/dL | Males: 0.55–1.18 Females: 0.55–1.02 | 0.93 [0.71–1.32] | 0.91 [0.71–1.11] | 0.99 [0.82–1.14] |
| Prealbumin, g/L | ||||
|---|---|---|---|---|
| Timepoints | Energy intakes < healthy targets (FAO/WHO/UNU) | Energy intakes ≥ healthy targets (FAO/WHO/UNU) | p value | |
| M1 | 0.29 [0.24–0.34] | 0.31 [0.19–0.4] | 0.815 | |
| M3 | 0.28 [0.25–0.32] | 0.26 [0.18–0.36] | 0.554 | |
| M12 | 0.3 [0.25–0.34] | 0.33 [0.24–0.36] | 0.776 | |
| Handgrip Strength, kg | ||||
| Timepoints | Protein intakes < healthy targets (0.8 g/kg/day) | Protein intakes ≥ healthy targets (0.8 g/kg/day) | p value | |
| M1 | Males | 30 [21.7–33] | 39 [33–43.3] | 0.003 |
| Females | 23.5 [18.7–27.5] | 22 [20–24] | 0.553 | |
| M3 | Males | 32 [24–42] | 36 [29.5–42] | 0.585 |
| Females | 18 [14–20] | 20.5 [16.2–25.5] | 0.091 | |
| M12 | Males | 35.5 [25.2–37.5] | 38 [25–48] | 0.441 |
| Females | 26 [18–43] | 34 [22–42] | 0.657 | |
| Data | Patients Who Attended Both M1 and M3 Consultations (n = 14) | p Value | |
|---|---|---|---|
| M1 | M3 | ||
| Actual weight, kg | 82.7 [60.2–88.5] | 86.5 [66.2–91.4] | 0.004 |
| Energy intakes, kcal/day | 1710 [1325–1975] | 2000 [1570–2165] | 0.064 |
| Protein intakes, g/day | 65 [42.5–82.2] | 73.9 [54.9–83.7] | 0.445 |
| Patients Who Attended Both M3 and M12 Consultations (n = 21) | |||
| M3 | M12 | ||
| Actual weight, kg | 79 [69–90.8] | 79.8 [68–97.5] | 0.004 |
| Energy intakes, kcal/day | 2000 [1800–2275] | 2045 [1787–2436] | 0.12 |
| Protein intakes, g/day | 80 [52.5–90] | 80.1 [60.4–107.5] | 0.056 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rousseau, A.-F.; Lucania, S.; Fadeur, M.; Verbrugge, A.-M.; Cavalier, E.; Colson, C.; Misset, B. Adequacy of Nutritional Intakes during the Year after Critical Illness: An Observational Study in a Post-ICU Follow-Up Clinic. Nutrients 2022, 14, 3797. https://doi.org/10.3390/nu14183797
Rousseau A-F, Lucania S, Fadeur M, Verbrugge A-M, Cavalier E, Colson C, Misset B. Adequacy of Nutritional Intakes during the Year after Critical Illness: An Observational Study in a Post-ICU Follow-Up Clinic. Nutrients. 2022; 14(18):3797. https://doi.org/10.3390/nu14183797
Chicago/Turabian StyleRousseau, Anne-Françoise, Sara Lucania, Marjorie Fadeur, Anne-Marie Verbrugge, Etienne Cavalier, Camille Colson, and Benoit Misset. 2022. "Adequacy of Nutritional Intakes during the Year after Critical Illness: An Observational Study in a Post-ICU Follow-Up Clinic" Nutrients 14, no. 18: 3797. https://doi.org/10.3390/nu14183797