
Malnutrition in Older Adults—Effect on Falls and Fractures: A Narrative Review


Abstract
:1. Introduction
1.1. Aim
1.2. Malnutrition in Older Adults
1.3. Diagnosis, Epidemiology, Estimation
2. Falls and Fractures—Consequences of Malnutrition
2.1. Falls
2.2. Fracture Risk
2.3. Negative Outcomes after Hip Fracture
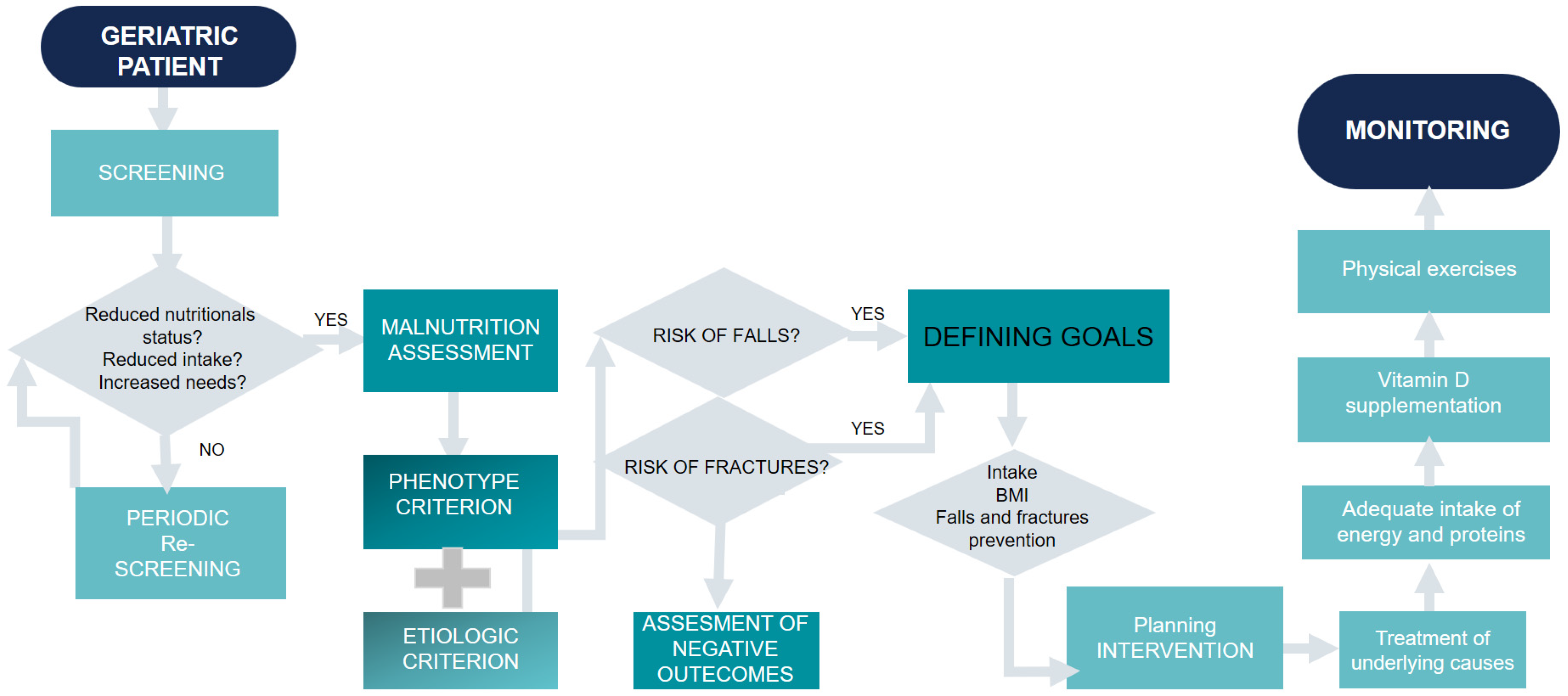
3. Directions for Clinical Practice
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Union of Medical Specialists (EUMS), Geriatric Medicine Section. Definition of Geriatrics. Available online: http://uemsgeriatricmedicine.org/www/land/definition/english.asp-1089 (accessed on 5 April 2022).
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, M.J.; Bauer, J.M.; Rämsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.S.; Charlton, K.E.; Maggio, M.; et al. Mini Nutritional Assessment International Group. Frequency of malnutrition in older adults: A multinational perspective using the mini nutritional assessment. J. Am. Geriatr. Soc. 2010, 58, 1734–1738. [Google Scholar] [CrossRef]
- Cereda, E.; Pedrolli, C.; Klersy, C.; Bonardi, C.; Quarleri, L.; Cappello, S.; Turri, A.; Rondanelli, M.; Caccialanza, R. Nutritional status in older persons according to healthcare setting: A systematic review and meta-analysis of prevalence data using MNA®. Clin. Nutr. 2016, 35, 1282–1290. [Google Scholar] [CrossRef]
- Reid, I.R.; Bolland, M.J.; Sellier, C. Malnutrition chez la personne âgée, dépister et prendre en charge. Soins Gerontol. 2018, 23, 12–17. [Google Scholar]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM Working Group. GLIM criteria for the diagnosis of malnutrition-A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Besora-Moreno, M.; Llauradó, E.; Tarro, L. Social and Economic Factors and Malnutrition or the Risk of Malnutrition in the Elderly: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2020, 12, 737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javed, A.A.; Aljied, R.; Allison, D.J.; Anderson, L.N.; Ma, J.; Raina, P. Body mass index and all-cause mortality in older adults: A scoping review of observational studies. Obes. Rev. 2020, 21, e13035. [Google Scholar] [CrossRef]
- Mioche, L.; Brigand, A.; Bidot, C.; Denis, J.B. Fat-free mass predictions through a bayesian network enable body composition comparisons in various populations. J. Nutr. 2011, 141, 1573–1580. [Google Scholar]
- Lee, D.H.; Keum, N.; Hu, F.B.; Orav, E.J.; Rimm, E.B.; Sun, Q.; Willett, W.C.; Giovannucci, E.L. Development and validation of anthropometric prediction equations for lean body mass, fat mass and percent fat in adults using the National Health and Nutrition Examination Survey (NHANES) 1999–2006. Br. J. Nutr. 2017, 118, 858–866. [Google Scholar]
- Inoue, T.; Misu, S.; Tanaka, T.; Sakamoto, H.; Iwata, K.; Chuman, Y.; Ono, R. Pre-fracture nutritional status is predictive of functional status at discharge during the acute phase with hip fracture patients: A multicenter prospective cohort study. Clin. Nutr. 2017, 36, 1320–1325. [Google Scholar] [CrossRef]
- Norman, K.; Haß, U.; Pirlich, M. Malnutrition in Older Adults-Recent Advances and Remaining Challenges. Nutrients 2021, 12, 2764. [Google Scholar] [CrossRef] [PubMed]
- Corish, C.A.; Bardon, L.A. Malnutrition in older adults: Screening and determinants. Proc. Nutr. Soc. 2019, 78, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Morrison, A.; Fan, T.; Sen, S.S.; Weisenfluh, L. Epidemiology of falls and osteoporotic fractures: A systematic review. Clinicoecon. Outcomes Res. 2013, 5, 9–18. [Google Scholar] [PubMed]
- Gusdal, A.K.; Johansson-Pajala, R.M.; Arkkukangas, M.; Ekholm, A.; Zander, V. Preventing Falls and Malnutrition among Older Adults in Municipal Residential Care in Sweden: A Registry Study. SAGE Open Nurs. 2021, 7, 2377–2386. [Google Scholar] [CrossRef]
- Choi, K.A.; Heu, E.; Nam, H.C.; Park, Y.; Kim, D.; Ha, Y.C. Relationship between Low Muscle Strength, and Protein Intake: A Preliminary Study of Elderly Patients with Hip Fracture. J. Bone Metab. 2022, 29, 17–21. [Google Scholar] [CrossRef]
- Inoue, T.; Maeda, K.; Nagano, A.; Shimizu, A.; Ueshima, J.; Murotani, K.; Sato, K.; Tsubaki, A. Undernutrition, Sarcopenia, and Frailty in Fragility Hip Fracture: Advanced Strategies for Improving Clinical Outcomes. Nutrients 2020, 12, 3743. [Google Scholar] [CrossRef] [PubMed]
- Lackoff, A.S.; Hickling, D.; Collins, P.F.; Stevenson, K.J.; Nowicki, T.A.; Bell, J.J. The association of malnutrition with falls and harm from falls in hospital inpatients: Findings from a 5-year observational study. J. Clin. Nurs. 2020, 29, 429–436. [Google Scholar] [CrossRef]
- Ishida, Y.; Maeda, K.; Nonogaki, T.; Shimizu, A.; Yamanaka, Y.; Matsuyama, R.; Kato, R.; Mori, N. Malnutrition at Admission Predicts In-Hospital Falls in Hospitalized Older Adults. Nutrients 2020, 12, 541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witt, S.; Englander, E.; Kumlien, C.; Axelsson, M. Mismatch between risk factors and preventive interventions? A register study of fall prevention among older people in one Swedish county. Int. J. Older People Nurs. 2018, 13, e12209. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Oden, A.; Johnell, O.; Johansson, H.; De Laet, C.; Brown, J.; Burckhardt, P.; Cooper, C.; Christiansen, C.; Cummings, S.; et al. The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. Osteoporos. Int. 2007, 18, 1033–1046. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.M.; Rosen, H.N.; Katz, J.N.; Rosner, B.A.; Rimm, E.B.; Gordon, C.M.; Curhan, G.C. BMI, Waist Circumference, and Risk of Incident Vertebral Fracture in Women. Obesity 2019, 27, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.D.; Orwoll, E.S.; Nielson, C.M.; Morin, S.N.; Majumdar, S.R.; Johansson, H.; Odén, A.; McCloskey, E.V.; Kanis, J.A. Estimated lean mass and fat mass differentially affect femoral bone density and strength index but are not FRAX independent risk factors for fracture. J. Bone Miner. Res. 2014, 29, 2511–2519. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.D.; Schousboe, J.T.; Morin, S.N.; Martineau, P.; Lix, L.M.; Johansson, H.; McCloskey, E.V.; Harvey, N.C.; Kanis, J.A. Loss in DXA-estimated total body lean mass but not fat mass predicts incident major osteoporotic fracture and hip fracture independently from FRAX: A registry-based cohort study. Arch. Osteoporos. 2020, 15, 96. [Google Scholar] [CrossRef] [PubMed]
- Johansson, H.; Kanis, J.A.; Odén, A. A meta-analysis of the association of fracture risk and body mass index in women. J. Bone Miner. Res. 2014, 29, 223–233. [Google Scholar] [CrossRef]
- Kim, J.H.; Hong, A.R.; Choi, H.J.; Ku, E.J.; Cho, N.H.; Shin, C.S. Sex-based Differences in the Association between Body Composition and Incident Fracture Risk in Koreans. Sci. Rep. 2017, 20, 5975. [Google Scholar] [CrossRef] [Green Version]
- Maezawa, K.; Nozawa, M.; Maruyama, Y.; Sakuragi, E.; Sugimoto, M.; Ishijima, M.L. Comparison of anemia, renal function, and nutritional status in older women with femoral neck fracture and older women with osteoarthritis of the hip joint. J. Orthop. Sci. 2022; in press. [Google Scholar] [CrossRef]
- Becker, N.; Hafner, T.; Pishnamaz, M.; Hildebrand, F.; Kobbe, P. Patient-specific risk factors for adverse outcomes following geriatric proximal femur fractures. Eur. J. Trauma Emerg. Surg. 2022, 48, 753–761. [Google Scholar] [CrossRef]
- Mariconda, M.; Costa, G.G.; Cerbasi, S.; Recano, P.; Aitanti, E.; Gambacorta, M.; Misasi, M. The determinants of mortality and morbidity during the year following fracture of the hip: A prospective study. Bone Jt. J. 2015, 97, 383–390. [Google Scholar] [CrossRef]
- Sim, Y.E.; Sim, S.D.; Seng, C.; Howe, T.S.; Koh, S.B.; Abdullah, H.R. Preoperative Anemia, Functional Outcomes, and Quality of Life after Hip Fracture Surgery. J. Am. Geriatr. Soc. 2018, 66, 1524–1531. [Google Scholar] [CrossRef]
- Han, T.S.; Yeong, K.; Lisk, R.; Fluck, D.; Fry, C.H. Prevalence and consequences of malnutrition and malnourishment in older individuals admitted to hospital with a hip fracture. Eur. J. Clin. Nutr. 2021, 75, 645–652. [Google Scholar] [CrossRef]
- Han, T.S.; Lisk, R.; Osmani, A.; Sharmin, R.; Sharmin, R.; El Gammel, S.; Yeong, K.; Fluck, D.; Fry, C.H. Increased Association with Malnutrition and Malnourishment in Older Adults Admitted with Hip Fractures Who Have Cognitive Impairment and Delirium, as Assessed by 4AT. Nutr. Clin. Pract. 2021, 36, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Espaulella, J.; Guyer, H.; Diaz-Escriu, F.; Stewart, A.; Garratt, E.; Wong, S.; Wiessing, K.R.; Bolland, M.J.; Bastin, S.; Gamble, G.D. Nutritional supplementation of elderly hip fracture patients. A randomized, double-blind, placebo-controlled trial. Age Ageing 2000, 29, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Bruce, D.; Laurance, I.; McGuiness, M.; Ridley, M.; Goldswain, P. Nutritional supplements after hip fracture: Poor compliance limits effectiveness. Clin. Nutr. 2003, 22, 497–500. [Google Scholar] [CrossRef]
- Wyers, C.E.; Reijven, P.L.; Breedveld-Peters, J.L.; Denissen, K.; Schotanus, M.; van Dongen, M.; Eussen, S.; Heyligers, I.C.; van den Brandt, P.A.; Willems, P.C.; et al. Efficacy of Nutritional Intervention in Elderly After Hip Fracture: A Multicenter Randomized Controlled Trial. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1429–1437. [Google Scholar] [CrossRef] [Green Version]
- Grant, W.B.; Al Anouti, F.; Boucher, B.J.; Dursun, E.; Gezen-Ak, D.; Jude, E.B.; Karonova, T.; Pludowski, P. A Narrative Review of the Evidence for Variations in Serum 25-Hydroxyvitamin D Concentration Thresholds for Optimal Health. Nutrients 2022, 14, 639. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Takacs, I.; Boyanov, M.; Belaya, Z.; Diaconu, C.C.; Mokhort, T.; Zherdova, N.; Rasa, I.; Payer, J.; Pilz, S. Clinical Practice in the Prevention, Diagnosis and Treatment of Vitamin D Deficiency: A Central and Eastern European Expert Consensus Statement. Nutrients 2022, 14, 1483. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.M.; Kamkar, N.; Pieruccini-Faria, F.; Osman, A.; Sarquis-Adamson, Y.; Close, J.; Hogan, D.B.; Hunter, S.W.; Kenny, R.A.; Lipsitz, L.A.; et al. Evaluation of Clinical Practice Guidelines on Fall Prevention and Management for Older Adults: A Systematic Review. JAMA Netw. Open 2021, 4, e2138911. [Google Scholar] [CrossRef]
- Murad, M.H.; Elamin, K.B.; Abu Elnour, N.O.; Elamin, M.B.; Alkatib, A.A.; Fatourechi, M.M.; Almandoz, J.P.; Mullan, R.J.; Lane, M.A.; Liu, H.; et al. Clinical review: The effect of vitamin D on falls: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2011, 96, 2997–3006. [Google Scholar] [CrossRef] [Green Version]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Willett, W.C.; Staehelin, H.B.; Bazemore, M.G.; Zee, R.Y.; Wong, J.B. Effect of vitamin D on falls: A meta-analysis. JAMA 2004, 291, 1999–2006. [Google Scholar] [CrossRef]
- Smith, L.M.; Gallagher, J.C.; Suiter, C. Medium doses of daily vitamin D decrease falls and higher doses of daily vitamin D3 increase falls: A randomized clinical trial. J. Steroid Biochem. Mol. Biol. 2017, 173, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Yu, S. Effectiveness of multifactorial interventions in preventing falls among older adults in the community: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2020, 106, 103564. [Google Scholar] [CrossRef]
- Nakahara, S.; Takasaki, M.; Abe, S.; Kakitani, C.; Nishioka, S.; Wakabayashi, H.; Maeda, K. Aggressive nutrition therapy in malnutrition and sarcopenia. Nutrition 2021, 84, 111109. [Google Scholar] [CrossRef]
- Gielen, E.; Beckwe´e, D.; Delaere, A.; De Breucker, S.; Vandewoude, M.; Bautmans, I.; Sarcopenia Guidelines Development Group of the Belgian Society of Gerontology and Geriatrics (BSGG). Nutritional interventions to improve muscle mass, muscle strength, and physical performance in older people: An umbrella review of systematic reviews and meta-analyses. Nutr. Rev. 2021, 79, 121–147. [Google Scholar] [CrossRef]
- Lin, Z.; Zhao, Y.; Chen, Q. Effects of oral administration of beta-hydroxy betamethylbutyrate on lean body mass in older adults: A systematic review and meta-analysis. Eur. Geriatr. Med. 2021, 12, 239–251. [Google Scholar] [CrossRef]
- Backlund, A.; Holmbeck, O.; Kumlien, C.; Axelsson, M. A registry study of nursing assessments, interventions and evaluations according to nutrition for persons living in municipal residential care homes. Nurs. Open 2018, 16, 341–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, S.H.; Jang, H.N.; Kim, J.H.; Kim, S.W.; Shin, C.S. Effect of Vitamin D Supplementation on Risk of Fractures and Falls According to Dosage and Interval: A Meta-Analysis. Endocrinol. Metab. 2022, 37, 344–358. [Google Scholar] [CrossRef]
- Iuliano, S.; Poon, S.; Robbins, J.; Bui, M.; Wang, X.; De Groot, L.; Van Loan, M.; Zadeh, A.G.; Nguyen, T.; Seeman, E. Effect of dietary sources of calcium and protein on hip fractures and falls in older adults in residential care: Cluster randomised controlled trial. BMJ 2021, 375, n2364. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| GLIM Scheme | GLIM Recommendation | Geriatric Consideration |
|---|---|---|
| Risk screening | At risk of malnutrition Use validated screening tool | Chose the screening tool that includes other geriatric syndromes. Early detection of malnutrition predictors in males and females. |
| ↓ | ||
| Diagnostic assessment | Assessment criteria
| Necessity of continuing education in the field of anthropometric cutoff points for older adults (for professional and nonprofessional caregivers), verification of weight loss in patients with dementia or depression (collecting data from home caregiversas well), muscle strength, and function assessment. Necessity of pharmacological treatment assessment for reduced food intake. |
| ↓ | ||
| Diagnosis | Meets criteria for malnutrition
| Need of continuing education for professional caregivers, as well as home caregivers, to diagnose malnutrition, one of the geriatric syndromes. |
| ↓ | ||
| Severity grading | Determine severity of malnutrition
| Contribution of other geriatric syndromes, assessment of its clinical outcomes, high risk of negative outcomes when coexisting. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kupisz-Urbanska, M.; Marcinowska-Suchowierska, E. Malnutrition in Older Adults—Effect on Falls and Fractures: A Narrative Review. Nutrients 2022, 14, 3123. https://doi.org/10.3390/nu14153123
Kupisz-Urbanska M, Marcinowska-Suchowierska E. Malnutrition in Older Adults—Effect on Falls and Fractures: A Narrative Review. Nutrients. 2022; 14(15):3123. https://doi.org/10.3390/nu14153123
Chicago/Turabian StyleKupisz-Urbanska, Malgorzata, and Ewa Marcinowska-Suchowierska. 2022. "Malnutrition in Older Adults—Effect on Falls and Fractures: A Narrative Review" Nutrients 14, no. 15: 3123. https://doi.org/10.3390/nu14153123