
Differential Effects of Three Nutritional Supplements on the Nutrient Intake of Pregnant Women Enrolled in a Conditional Cash Transfer Program in Mexico: A Cluster Randomized Trial

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
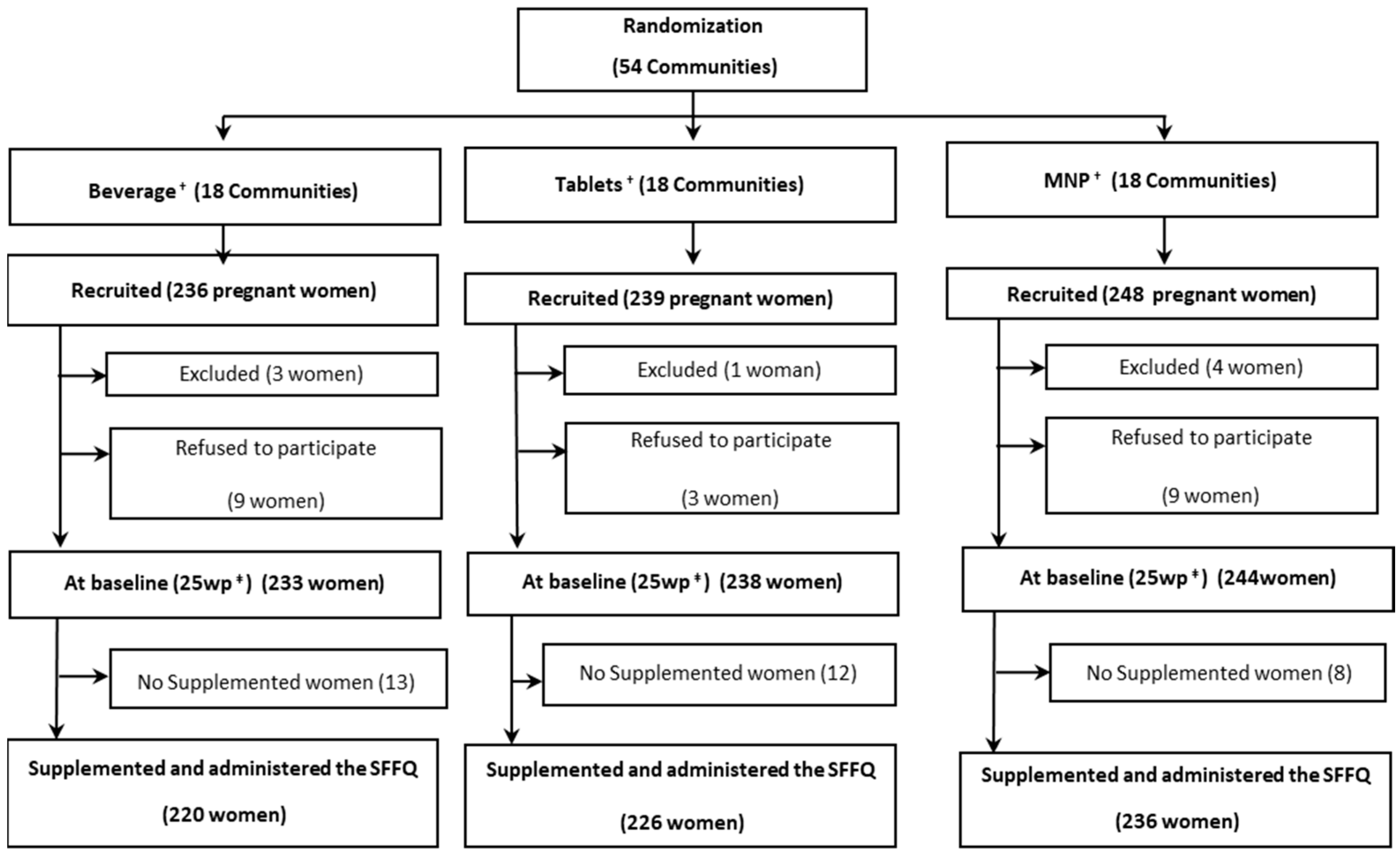
2.1. Study Design
2.2. Recruitment and Supplement Delivery
2.2.1. Inclusion and Exclusion Criteria
2.2.2. Supplement Delivery
2.2.3. Data Collection
2.2.4. Dietary Intake
2.2.5. Energy, Nutrient Intake, and Food Group Estimation
2.2.6. Body Mass Index and Socioeconomic Status Index
2.3. Ethics
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
3.2. Covariate-Adjusted Median Changes of Nutrient Consumption from Diet Alone
3.3. Covariate-Adjusted Median Changes of Nutrient Consumption from the Diet Plus Supplements
3.4. Adherence to Supplementation
3.5. Food Groups
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Osendarp, S.; Akuoku, J.; Black, R.; Headey, D.; Heidkamp, R. The COVID-19 crisis will exacerbate maternal and child undernutrition and child mortality in low- and middle-income countries. Nat. Food 2021, 2, 476–484. [Google Scholar] [CrossRef]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; De Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Keats, E.C.; Haider, B.A.; Tam, E.; Bhutta, Z.A. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Carroll, G.; Vilar-Compte, M.; Teruel, G.; Moncada, M.; Aban-Tamayo, D.; Werneck, H.; de Moraes, R.M.; Pérez-Escamilla, R. Estimating the costs for implementing a maternity leave cash transfer program for women employed in the informal sector in Brazil and Ghana. Int. J. Equity Health 2022, 21, 20. [Google Scholar] [CrossRef]
- Neufeld, L.M.; García-Guerra, A.; Quezada, A.D.; Théodore, F.; Arenas, A.B.; Islas, C.D.; Garcia-Feregrino, R.; Hernandez, A.; Colchero, A.; Habicht, J.P. Fortified Food Can Be Replaced by Micronutrient Supplements for Distribution in a Mexican Social Protection Program Based on Results of a Cluster-Randomized Trial and Costing Analysis. J. Nutr. 2019, 149 (Suppl. 1), 2302S–2309S. [Google Scholar] [CrossRef]
- Neufeld, L.M.; Steta, C.; Rivera, J.; Valle, A.M.; Grados, R.; Uriega, S.; López, V.H. Evaluation for program decision making: A case study of the Oportunidades program in Mexico. J. Nutr. 2011, 141, 2076–2083. [Google Scholar] [CrossRef] [Green Version]
- Neufeld, L.M.; Grados, R.; De La Vega, A.V.; Steta, C.; Regalia, F.; A Rivera-Dommarco, J. A Brief History of Evidence-Informed Decision Making for Nutrition in Mexico. J. Nutr. 2019, 149 (Suppl. 1), 2277S–2280S. [Google Scholar] [CrossRef]
- García-Guerra, A.; Neufeld, L.M.; Bonvecchio Arenas, A.; Fernández-Gaxiola, A.C.; Mejía-Rodríguez, F.; García-Feregrino, R.; Rivera-Dommarco, J.A. Closing the Nutrition Impact Gap Using Program Impact Pathway Analyses to Inform the Need for Program Modifications in Mexico’s Conditional Cash Transfer Program. J. Nutr. 2019, 149 (Suppl. 1), 2281S–2289S. [Google Scholar] [CrossRef] [Green Version]
- Ríos, E. Suplementos de Micronutrientes Múltiples “SMM”: Una Solución Costo-Efectiva Para Las Deficiencias Maternas de Micronutrientes. Available online: https://www.amemexico.org/memoria/ (accessed on 5 April 2022).
- Organización Mundial de la Salud. Obesidad y sobrepeso; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/es/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 21 November 2019).
- Organización Mundial de la Salud. Directriz: Actualizaciones Sobre la Atención de la Desnutrición Aguda Severa en Lactantes y Niños; Organización Mundial de la Salud: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/bitstream/handle/10665/249206/9789243506326-spa.pdf (accessed on 8 July 2021).
- Barquera, S.; Hernández-Barrera, L.; Trejo-Valdivia, B.; Shamah, T.; Campos-Nonato, I.; Rivera-Dommarco, J. Obesidad en México, prevalencia y tendencias en adultos. Salud Publica Mex. 2020, 62, 682–692. [Google Scholar] [CrossRef]
- Mejía-Rodríguez, F.; Shamah-Levy, T.; Villalpando, S.; García-Guerra, A.; Méndez-Gómez Humarán, I. Iron, zinc, copper and magnesium deficiencies in Mexican adults from the National Health and Nutrition Survey 2006. Salud Publica Mex. 2013, 55, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Mejía-Rodríguez, F.; Villalpando, S.; Shamah-Levy, T.; García-Guerra, A.; Méndez-Gómez Humarán, I.; De la Cruz-Góngora, V. Prevalence of iron deficiency was stable and anemia increased during 12 years (2006–2018) in Mexican women 20–49 years of age. Salud Publica Mex. 2021, 63, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Shamah-Levy, T.; Villalpando, S.; Mejía-Rodríguez, F.; Cuevas-Nasu, L.; Gaona-Pineda, E.B.; Rangel-Baltazar, E.; Zambrano-Mujica, N. Prevalence of iron, folate, and vitamin B12 deficiencies in 20 to 49 years old women: Ensanut 2012. Salud Publica Mex. 2015, 57, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Mejía-Rodríguez, F.; Mundo-Rosas, V.; Rodríguez-Ramírez, S.; Hernández-F, M.; García-Guerra, A.; Rangel-Baltazar, E.; Gómez-Acosta, L.M.; Shamah-Levy, T. High prevalence of anemia in Mexican women in poverty, Ensanut 100k. Salud Publica Mex. 2019, 61, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Habicht, J. Standardization of anthropometric methods in the field. PAHO Bull. 1974, 76, 375–384. [Google Scholar]
- Lohman, T.; Roche, A.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champlaign, IL, USA, 1988. [Google Scholar]
- Neufeld, L.M.; Haas, J.; Grajéda, R.; Martorell, R. Last menstrual period provides the best estimate of gestation length for women in rural Guatemala. Paediat. Perinat. Epidemiol. 2006, 20, 290–298. [Google Scholar] [CrossRef]
- Hernández, A.M.; Romieu, I.; Parra, S.; Hernández, J.A.; Madrigal, H.; Willet, W. Validity and reproducibility of a food frequency questionnaire to assess dietary intake of women living in Mexico City. Salud Publica Mex. 1998, 40, 133–140. Available online: https://www.saludpublica.mx/index.php/spm/article/view/6068 (accessed on 8 July 2021). [CrossRef]
- Ramírez-Silva, I.; Jiménez-Aguilar, A.; Valenzuela-Bravo, D.; Martinez-Tapia, B.; Rodríguez-Ramírez, S.; Gaona-Pineda, E.B.; Angulo-Estrada, S.; Shamah-Levy, T. Methodology for estimating dietary data from the semi-quantitative food frequency questionnaire of the Mexican National Health and Nutrition Survey 2012. Salud Publica Mex. 2016, 58, 629–638. [Google Scholar] [CrossRef] [Green Version]
- Safdie, M. Bases de Datos de Valor Nutritivo de los Alimentos; Complied by Instituto Nacional de Salud Pública; Instituto Nacional de Salud Pública: Cuernavaca, Morelos, 2004. [Google Scholar]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and its Panel on Folate, Other B Vitamins, and Choline. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academies Press (US): Washington, DC, USA, 1998. Available online: https://www.ncbi.nlm.nih.gov/books/NBK114310/ (accessed on 21 November 2019). [CrossRef]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry; WHO Technical Report Series 845; WHO: Geneva, Switzerland, 1995; Available online: https://apps.who.int/iris/bitstream/handle/10665/37003/WHO_TRS_854.pdf;jsessionid=58250311BFE72F32D31A9E04E57AA9A6?sequence=1 (accessed on 9 October 2019).
- Vyas, S.; Kumaranayake, L. Constructing socio-economic status indices: How to use principal component analysis. Health Policy Plan. 2006, 21, 459–468. [Google Scholar] [CrossRef] [Green Version]
- Parente, P.M.D.C.; Santos Silva, J.M.C. Quantile regression with clustered data. J. Econom. Meth. 2016, 5, 1–15. [Google Scholar] [CrossRef]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M.; Food and Nutrition Board of the Institute of Medicine; The National Academies. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Neufeld, L.M.; Sotres Alvarez, D.; Flores López, M.; Tolentino Mayo, L.; Jiménez Ruiz, J.; Rivera Dommarco, J. Estudio sobre el consumo de los suplementos alimenticios Nutrisano y Nutrivida en niños y mujeres de zonas urbanas beneficiarios de Oportunidades [Study on the consumption of food supplements Nutrisano and Nutrivida among children and women beneficiaries of Oportunidades in urban areas]. In Evaluación externa de impacto del Programa Oportunidades 2004; Hernández-Prado, B., Meditors, H.-Á., Eds.; Tomo III. Alimentación; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2004; pp. 119–147. Available online: https://evaluacion.prospera.gob.mx/es/wersd53465sdg1/docs/2004/insp_ciesas_2004_tomo_iii.pdf (accessed on 23 May 2019).
- World Health Organization. Guideline: Use of Multiple Micronutrient Powders for Point-of-Use Fortification of Foods Consumed by Pregnant Women; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/elena/titles/micronutrientpowder_pregnancy/en/ (accessed on 5 March 2020).
- Suchdev, P.S.; Peña-Rosas, J.P.; De-Regil, L.M. Multiple micronutrient powders for home (point-of-use) fortification of foods in pregnant women. Cochrane Database Syst. Rev. 2015, 6, CD011158. [Google Scholar] [CrossRef] [PubMed]
- Secretaria de Desarrollo Social (SEDESOL). Reglas de Operación del Programa de Desarrollo Humano Oportunidades, Para el Ejercicio Fiscal 2012. Diario Oficial, Tercera Sección. Available online: https://www.dof.gob.mx/nota_detalle.php?codigo=5257845&fecha=05/07/2012. (accessed on 9 October 2019).
- Martin, S.L.; Wawire, V.; Ombunda, H.; Li, T.; Sklar, K.; Tzehaie, H.; Wong, A.; Pelto, G.H.; Omotayo, M.O.; Chapleau, G.M.; et al. Integrating Calcium Supplementation into Facility-Based Antenatal Care Services in Western Kenya: A Qualitative Process Evaluation to Identify Implementation Barriers and Facilitators. Curr. Dev. Nutr. 2018, 2, nzy068. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, A.D.; Tiruneh, S.A.; Abate, B.A.; Engidaw, M.T.; Asnakew, D.T. Adherence to iron with folic acid supplementation and its associated factors among pregnant women attending antenatal care follow up at Debre Tabor General Hospital, Ethiopia. PLoS ONE 2017, 14, e0210086. [Google Scholar] [CrossRef]
- Klemm, G.C.; Birhanu, Z.; Ortolano, S.E.; Kebede, Y.; Martin, S.L.; Mamo, G.; Dickin, K.L. Integrating Calcium Into Antenatal Iron-Folic Acid Supplementation in Ethiopia: Women’s Experiences, Perceptions of Acceptability, and Strategies to Support Calcium Supplement Adherence. Glob. Health Sci. Pract. 2020, 8, 413–430. [Google Scholar] [CrossRef] [PubMed]
- Getachew, M.; Abay, M.; Zelalem, H.; Gebremedhin, T.; Grum, T.; Bayray, A. Magnitude and factors associated with adherence to Iron-folic acid supplementation among pregnant women in Eritrean refugee camps, northern Ethiopia. BMC Pregnancy Childbirth 2018, 18, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demis, A.; Geda, B.; Alemayehu, T.; Abebe, H. Iron and folic acid supplementation adherence among pregnant women attending antenatal care in North Wollo Zone northern Ethiopia: Institution based cross-sectional study. BMC Res. Notes 2019, 12, 107. [Google Scholar] [CrossRef] [Green Version]
- Molla, T.; Guadu, T.; Muhammad, E.A.; Hunegnaw, M.T. Factors associated with adherence to iron folate supplementation among pregnant women in West Dembia district, northwest Ethiopia: A cross sectional study. BMC Res. Notes 2019, 12, 6. [Google Scholar] [CrossRef]
- Rivera, J.A.; Martorell, R.; González, W.; Lutter, C.; González de Cossío, T.; Flores-Ayala, R.; Uauy, R.; Delgado, H.; Grupo Técnico de Nutrición del SMS. Preventing maternal and child malnutrition: The nutrition component of the Mesoamerican Health Initiative 2015. Salud Publica Mex 2011, 53 (Suppl. 3), S303–S311. Available online: http://www.scielo.org.mx/scielo.php?script=sci_abstract&pid=S0036-36342011000900004&lng=es&nrm=iso&tlng=en (accessed on 8 July 2021).
- López-Olmedo, N.; Hernández-Cordero, S.; Neufeld, L.M.; García-Guerra, A.; Mejía-Rodríguez, F.; Méndez Gómez-Humarán, I. The associations of maternal weight change with breastfeeding, diet and physical activity during the postpartum period. Matern Child. Health J. 2016, 20, 270–280. [Google Scholar] [CrossRef]
- Carriquiry, A.L. Estimation of usual intake distributions of nutrients and foods. J. Nutr. 2003, 133, 601S–608S. [Google Scholar] [CrossRef] [Green Version]
- Dewey, K.G. Reducing stunting by improving maternal, infant and young child nutrition in regions such as South Asia: Evidence, challenges and opportunities. Matern Child. Nutr. 2016, 12 (Suppl. 1), 27–38. [Google Scholar] [CrossRef]
- Moreno-Villares, J.M.; Collado MCn Larqué, E.; Leis-Trabazo, M.R.; Sáenz-de-Pipaon, M.; Moreno-Aznar, L.A. Los primeros 1000 días: Una oportunidad para reducir la carga de las enfermedades no transmisibles. Nutr. Hosp. 2019, 36, 218–232. [Google Scholar] [CrossRef] [PubMed]
- Sahebnasagh, A.; Saghafi, F.; Avan, R.; Khoshi, A.; Khataminia, M.; Safdari, M.; Habtemariam, S.; Ghaleno, H.R.; Nabavi, S.M. The prophylaxis and treatment potential of supplements for COVID-19. Eur. J. Pharmacol. 2020, 887, 173530. [Google Scholar] [CrossRef] [PubMed]
- Jovic, T.H.; Ali, S.R.; Ibrahim, N.; Jessop, Z.M.; Tarassoli, S.P.; Dobbs, T.D.; Holford, P.; A Thornton, C.; Whitaker, I.S. Could Vitamins Help in the Fight Against COVID-19? Nutrients 2020, 12, 2550. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Supplements (Dose) | |||
|---|---|---|---|
| Beverage †, ‡ | Tablets † | MNP † | |
| Energy (kcal) | 250 | - | - |
| Protein (g) | 12 | - | - |
| Carbohydrates (g) | 25.3 | - | - |
| Lipid (g) | 11.2 | - | - |
| Sodium (mg) | 81.2 | - | - |
| Iron (mg) Φ | 15 | 15 | 15 |
| Zinc gluconate (mg) | 15 | 15 | 15 |
| Iodine (µg) | 100 | 100 | 100 |
| Folic acid (µg) | 400 | 400 | 400 |
| Ascorbic acid (mg) § | 100 | 100 | 100 |
| Potassium Iodine (µg) | 100 | 100 | 100 |
| Vitamin E (Acetate; mg ET) | 10 | 10 | 10 |
| Vitamin B12 (Cyanocobalamin; µg) | 2.6 | 2.6 | 2.6 |
| Beverage ‡ | Tablets ‡ | MNP ‡ | Excluded | |
|---|---|---|---|---|
| n = 200 | n = 206 | n = 192 | n = 117 £ | |
| Age | 27.7 [22.2, 32.9] | 26.6 [23.4, 31.2] | 26.9 [22.8, 31.4] | 26.0 [21.4, 30.8] |
| Weight, kg | 59.0 [52.7, 68.9] | 58.4 [52.7, 65.4] | 60.5 [53.1, 66.7] | 60.0 [53.0, 67.3] |
| Height, cm | 149.4 [146.0, 152.9] | 150.0 [145.7, 154.6] | 150.0 [147.4, 153.9] | - |
| BMI, kg/m2 | 26.6 [23.4, 30.9] | 26.3 [23.4, 28.9] | 26.4 [23.2, 29.7] | - |
| Overweight, % | 34.0 | 42.3 | 39.3 | 39.5 |
| Obesity, % | 28.9 | 19.4 | 23.0 | 19.8 |
| SES Index, SD ¥ | 0.1 [−0.5, 0.7] | 0.0 [−0.6, 0.6] | −0.1 [−0.8, 0.5] | 0.2 [−0.4, 0.8] |
| Primiparous, % | 18.5 | 14.1 | 12.5 | 19.7 |
| Indigenous, % ψ | 7.0 | 8.8 | 6.8 | 7.7 |
| Educational level Φ | ||||
| None, % | 35.0 | 25.4 | 35.9 | 25.6 |
| Elementary, % | 27.0 | 31.7 | 32.3 | 34.2 |
| Middle or higher, % | 38.0 | 42.9 | 31.8 | 40.2 |
| Diet intake alone | ||||
| Energy, kcal | 1890 [1426, 2569] | 1743 [1141, 2445] | 1826 [1338, 2606] | 1836 [1340, 2847] |
| Carbohydrates, g | 258.0 [195.5, 351.3] | 234.6 [156.3, 336.8] | 241.5 [183.7, 351.5] | 249.7 [183.3, 342.1] |
| Protein, g | 61.9 [42.4, 83.3] | 55.8 [35.7, 78.9] | 61.5 [44.7, 83.8] | 62.0 [42.1, 88.1] |
| Lipids, g | 74.2 [46.1, 104.0] | 65.7 [39.0, 94.0] | 71.0 [44.7, 127.0] | 70.9 [46.0, 114.9] |
| Iron, mg | 12.4 [8.6, 16.9] | 10.9 [7.7, 15.8] | 11.7 [8.6, 17.4] | 11.8 [8.0, 17.1] |
| Zinc, mg | 8.9 [6.0, 12.0] | 8.2 [5.3, 11.3] | 8.6 [6.1, 11.8] | 8.5 [5.9, 12.4] |
| Vitamin C, mg | 168.6 [108.1, 318.3] | 161.6 [94.1, 289.5] | 196.7 [111.7, 295.7] | 181.5 [95.7, 293.4] |
| Vitamin E, mg | 10.3 [5.1, 16.1] | 9.1 [4.4, 14.7] | 9.7 [4.7, 19.6] | 8.6 [4.7, 15.5] |
| Vitamin B12, mcg | 3.6 [2.4, 5.5] | 3.2 [1.7, 4.9] | 3.8 [2.3, 5.3] | 3.5 [2.3, 6.0] |
| DFE, mcg § | 416.3 [302.2, 648.9] | 403.4 [241.8, 573.7] | 458.3 [293.5, 715.4] | 428.2 [265.7, 651.2] |
| Beverage | Tablets | MNP | Tablets vs. Beverage | MNP vs. Beverage | MNP vs. Tablets | |
|---|---|---|---|---|---|---|
| Changes from baseline to 37 wk | ||||||
| n = 152 | n = 168 | n = 157 | ||||
| Energy, kcal | −239.9 *** ± 65.6 | −260.9 ** ± 89.8 | −77.7 ± 67.2 | −20.9 ± 118.4 | 162.2 ± 97.7 | 183.2 ± 115.8 |
| Carbohydrates, g | −41.5 *** ± 8.5 | −43.7 *** ± 8.6 | −25.8 *** ± 7.8 | −2.2 ± 12.2 | 15.7 ± 11.3 | 17.9 ± 12.0 |
| Protein, g | −7.71 *** ± 1.85 | −9.16 *** ± 2.44 | −4.91 * ± 2.08 | −1.45 ± 3.11 | 2.80 ± 2.74 | 4.25 ± 3.43 |
| Lipids, g | −14.53 *** ± 3.09 | −12.43 ** ± 4.25 | −7.05 ± 4.02 | 2.10 ± 6.10 | 7.48 ± 5.14 | 5.38 ± 5.82 |
| Iron, mg | −1.65 *** ± 0.43 | −1.88 ** ± 0.66 | −0.64 ± 0.43 | −0.23 ± 0.84 | 1.00 ± 0.56 | 1.24 ± 0.89 |
| Zinc, mg | −1.31 *** ± 0.30 | −1.41 *** ± 0.39 | −0.30 ± 0.27 | −0.10 ± 0.52 | 1.01 ** ± 0.39 | 1.10 * ± 0.52 |
| Vitamin C, mg | −62.5 *** ± 8.8 | −47.2 *** ± 8.1 | −33.9 *** ± 7.3 | 15.3 ± 12.8 | 28.5 ** ± 10.3 | 13.3 ± 12.0 |
| Vitamin E, mg | −3.48 *** ± 0.57 | −3.30 *** ± 0.63 | −2.29 *** ± 0.55 | 0.18 ± 0.89 | 1.19 ± 0.74 | 1.01 ± 0.88 |
| Vitamin B12, mcg | −0.88 *** ± 0.19 | −0.56 ** ± 0.20 | −0.10 ± 0.18 | 0.32 ± 0.28 | 0.78 ** ± 0.28 | 0.46 ± 0.30 |
| DFE, mcg § | −80.0 ** ± 24.7 | −98.0 ** ± 31.1 | −61.9 ** ± 21.6 | −18.0 ± 45.0 | 18.0 ± 28.5 | 36.1 ± 41.7 |
| Changes from baseline to 1 mpp | ||||||
| n = 188 | n = 197 | n = 178 | ||||
| Energy, kcal | −319.5 *** ± 67.5 | −176.8 * ± 81.0 | −189.0 * ± 75.4 | 142.7 ± 102.7 | 130.5 ± 87.0 | −12.2 ± 110.2 |
| Carbohydrates, g | −40.6 *** ± 8.3 | −34.1 ** ± 12.2 | −37.1 *** ± 7.2 | 6.4 ± 14.3 | 3.5 ± 10.0 | −2.9 ± 12.5 |
| Protein, g | −5.33 ** ± 1.76 | −1.25 ± 2.60 | −1.80 ± 2.26 | 4.08 ± 3.22 | 3.53 ± 2.68 | −0.55 ± 3.64 |
| Lipids, g | −20.49 *** ± 2.73 | −14.37 ** ± 4.61 | −18.37 *** ± 3.86 | 6.12 ± 5.50 | 2.12 ± 4.60 | −4.00 ± 6.03 |
| Iron, mg | −2.56 *** ± 0.56 | −1.69 *** ± 0.48 | −1.46 ** ± 0.48 | 0.87 ± 0.76 | 1.10 ± 0.65 | 0.23 ± 0.74 |
| Zinc, mg | −1.29 *** ± 0.29 | −0.71 ± 0.38 | −0.65 ± 0.40 | 0.58 ± 0.48 | 0.64 ± 0.50 | 0.06 ± 0.63 |
| Vitamin C, mg | −113.9 *** ± 7.7 | −118.2 *** ± 6.8 | −114.7 *** ± 6.1 | −4.3 ± 11.2 | −0.8 ± 9.2 | 3.5 ± 9.5 |
| Vitamin E, mg | −6.35 *** ± 0.50 | −5.60 *** ± 0.56 | −5.55 *** ± 0.54 | 0.75 ± 0.75 | 0.80 ± 0.62 | 0.04 ± 0.69 |
| Vitamin B12, mcg | −0.65 *** ± 0.17 | −0.46 ± 0.25 | −0.22 ± 0.19 | 0.19 ± 0.26 | 0.43 ± 0.24 | 0.24 ± 0.32 |
| DFE, mcg § | −181.5 *** ± 18.1 | −156.6 *** ± 16.9 | −131.3 *** ± 17.2 | 24.9 ± 22.7 | 50.2 * ± 23.9 | 25.3 ± 25.5 |
| Changes from baseline to 3 mpp | ||||||
| n = 187 | n = 198 | n = 169 | ||||
| Energy, kcal | −334.2 *** ± 70.7 | −223.0 * ± 89.5 | −212.1 * ± 90.9 | 111.2 ± 116.3 | 122.1 ± 125.7 | 10.9 ± 139.1 |
| Carbohydrates, g | −56.2 *** ± 10.0 | −49.4 *** ± 10.5 | −38.5 ** ± 14.9 | 6.9 ± 12.7 | 17.8 ± 19.0 | 10.9 ± 19.9 |
| Protein, g | −9.10 *** ± 2.28 | −6.51 ** ± 2.40 | −4.25 ± 3.44 | 2.59 ± 3.49 | 4.85 ± 4.22 | 2.26 ± 4.29 |
| Lipids, g | −14.92 ** ± 4.54 | −5.42 ± 5.11 | −9.38 * ± 3.86 | 9.50 ± 6.67 | 5.54 ± 5.45 | −3.96 ± 6.05 |
| Iron, mg | −2.45 *** ± 0.48 | −1.74 *** ± 0.48 | −0.72 ± 0.62 | 0.71 ± 0.63 | 1.73 * ± 0.82 | 1.02 ± 0.80 |
| Zinc, mg | −1.22 ** ± 0.39 | −1.16 ** ± 0.36 | −0.36 ± 0.49 | 0.06 ± 0.52 | 0.86 ± 0.66 | 0.80 ± 0.63 |
| Vitamin C, mg | −108.7 *** ± 7.6 | −94.1 *** ± 5.5 | −96.1 *** ± 8.8 | 14.6 ± 10.2 | 12.6 ± 11.8 | −2.1 ± 10.5 |
| Vitamin E, mg | −4.53 *** ± 0.68 | −3.90 *** ± 1.05 | −4.25 *** ± 0.69 | 0.63 ± 1.21 | 0.28 ± 0.97 | −0.35 ± 1.28 |
| Vitamin B12, mcg | −0.59 * ± 0.23 | −0.49 * ± 0.24 | −0.32 ± 0.23 | 0.10 ± 0.36 | 0.27 ± 0.30 | 0.17 ± 0.33 |
| DFE, mcg § | −163.6 *** ± 20.1 | −108.0 *** ± 16.3 | −83.3 *** ± 24.7 | 55.5 * ± 27.1 | 80.3 ** ± 30.1 | 24.8 ± 30.8 |
| Beverage | Tablets | MNP | Tablets vs. Beverage | MNP vs. Beverage | MNP vs. Tablets | |
|---|---|---|---|---|---|---|
| Changes from baseline to 37 wk | ||||||
| n = 152 | n = 168 | n = 157 | ||||
| Energy, kcal | −25.0 ± 83.2 | −264.6 ** ± 94.3 | −89.2 ± 70.0 | −239.6 ± 141.5 | −64.2 ± 109.7 | 175.4 ± 120.3 |
| Carbohydrates, g | −16.1 ± 8.5 | −44.4 *** ± 10.0 | −23.5 ** ± 8.4 | −28.4 * ± 13.2 | −7.4 ± 12.0 | 20.9 ± 14.0 |
| Protein, g | 2.60 ± 1.90 | −8.94 *** ± 2.38 | −5.20 * ± 2.20 | −11.54 *** ± 3.00 | −7.80 ** ± 2.90 | 3.74 ± 3.54 |
| Lipids, g | −4.22 ± 3.39 | −12.83 ** ± 4.15 | −6.96 ± 3.93 | −8.60 ± 6.33 | −2.73 ± 5.18 | 5.87 ± 5.60 |
| Iron, mg | 11.94 *** ± 0.47 | 12.01 *** ± 0.53 | 12.69 *** ± 0.32 | 0.08 ± 0.71 | 0.75 ± 0.54 | 0.68 ± 0.69 |
| Zinc, mg | 13.00 *** ± 0.44 | 12.74 *** ± 0.42 | 13.61 *** ± 0.33 | −0.26 ± 0.64 | 0.61 ± 0.50 | 0.86 ± 0.63 |
| Vitamin C, mg | 25.2 *** ± 7.6 | 40.7 *** ± 9.5 | 56.3 *** ± 8.8 | 15.5 ± 13.5 | 31.2 ** ± 11.7 | 15.6 ± 14.7 |
| Vitamin E, mg | 5.39 *** ± 0.64 | 5.63 *** ± 0.76 | 7.07 *** ± 0.70 | 0.24 ± 1.06 | 1.67 * ± 0.81 | 1.44 ± 1.13 |
| Vitamin B12, mcg | 1.48 *** ± 0.19 | 1.66 *** ± 0.22 | 2.31 *** ± 0.17 | 0.18 ± 0.31 | 0.83 ** ± 0.27 | 0.65 * ± 0.31 |
| DFE, mcg § | 546.8 *** ± 25.7 | 540.5 *** ± 36.2 | 587.6 *** ± 21.2 | −6.3 ± 49.5 | 40.8 ± 30.4 | 47.1 ± 47.3 |
| Changes from baseline to 1 mpp | ||||||
| n = 188 | n = 197 | n = 178 | ||||
| Energy, kcal | −103.3 ± 63.4 | −200.0 * ± 86.9 | −175.4 * ± 75.0 | −96.8 ± 103.2 | −72.2 ± 90.0 | 24.6 ± 116.5 |
| Carbohydrates, g | −22.8 ** ± 8.8 | −31.7 ** ± 11.4 | −35.8 *** ± 7.5 | −8.9 ± 13.9 | −13.0 ± 10.7 | −4.1 ± 13.0 |
| Protein, g | 5.50 ** ± 2.12 | −0.82 ± 2.45 | −1.84 ± 2.23 | −6.32 ± 3.31 | −7.34 * ± 2.90 | −1.02 ± 3.42 |
| Lipids, g | −9.76 *** ± 2.61 | −14.43 ** ± 4.51 | −18.12 *** ± 3.72 | −4.67 ± 5.35 | −8.36 ± 4.38 | −3.69 ± 5.83 |
| Iron, mg | 11.35 *** ± 0.57 | 11.64 *** ± 0.58 | 12.41 *** ± 0.49 | 0.28 ± 0.87 | 1.05 ± 0.73 | 0.77 ± 0.79 |
| Zinc, mg | 12.86 *** ± 0.46 | 13.21 *** ± 0.42 | 13.63 *** ± 0.36 | 0.35 ± 0.59 | 0.77 ± 0.62 | 0.42 ± 0.63 |
| Vitamin C, mg | −19.1 * ± 7.7 | −26.2 *** ± 7.2 | −18.9 ** ± 5.8 | −7.2 ± 9.9 | 0.1 ± 9.0 | 7.3 ± 9.3 |
| Vitamin E, mg | 3.21 *** ± 0.53 | 3.67 *** ± 0.59 | 3.62 *** ± 0.50 | 0.46 ± 0.78 | 0.41 ± 0.59 | −0.05 ± 0.70 |
| Vitamin B12, mcg | 1.72 *** ± 0.19 | 1.77 *** ± 0.21 | 2.27 *** ± 0.18 | 0.04 ± 0.26 | 0.55 * ± 0.25 | 0.50 ± 0.28 |
| DFE, mcg § | 444.1 *** ± 22.5 | 490.7 *** ± 24.8 | 507.5 *** ± 14.1 | 46.7 ± 33.2 | 63.4 ** ± 24.3 | 16.8 ± 28.4 |
| Changes from baseline to 3 mpp | ||||||
| n = 187 | n = 198 | n = 169 | ||||
| Energy, kcal | −142.6 ± 80.0 | −235.0 * ± 103.9 | −207.3 * ± 95.5 | −92.3 ± 136.3 | −64.6 ± 138.2 | 27.7 ± 156.1 |
| Carbohydrates, g | −34.0 *** ± 9.8 | −48.5 *** ± 10.6 | −39.4 * ± 16.2 | −14.5 ± 13.0 | −5.3 ± 20.5 | 9.2 ± 20.7 |
| Protein, g | 0.08 ± 2.43 | −6.46 * ± 2.73 | −3.55 ± 3.43 | −6.54 ± 3.88 | −3.63 ± 4.44 | 2.91 ± 4.55 |
| Lipids, g | −5.72 ± 4.42 | −5.89 ± 4.52 | −9.27 * ± 4.19 | −0.17 ± 6.34 | −3.55 ± 5.76 | −3.37 ± 6.04 |
| Iron, mg | 10.13 *** ± 0.70 | 10.93 *** ± 0.77 | 12.50 *** ± 0.84 | 0.81 ± 1.08 | 2.38 * ± 1.06 | 1.57 ± 1.19 |
| Zinc, mg | 11.69 *** ± 0.45 | 12.26 *** ± 0.62 | 13.11 *** ± 0.56 | 0.57 ± 0.84 | 1.43 ± 0.73 | 0.85 ± 0.91 |
| Vitamin C, mg | −24.3 *** ± 6.4 | −13.4 ** ± 5.1 | −8.3 ± 9.5 | 10.9 ± 8.3 | 16.0 ± 11.5 | 5.1 ± 11.0 |
| Vitamin E, mg | 3.67 *** ± 0.94 | 4.77 *** ± 0.84 | 4.01 *** ± 0.74 | 1.10 ± 1.15 | 0.34 ± 0.91 | −0.76 ± 1.02 |
| Vitamin B12, mcg | 1.48 *** ± 0.22 | 1.67 *** ± 0.23 | 1.79 *** ± 0.27 | 0.19 ± 0.33 | 0.31 ± 0.37 | 0.12 ± 0.38 |
| DFE, mcg § | 418.3 *** ± 28.9 | 481.2 *** ± 35.8 | 512.7 *** ± 28.5 | 62.9 ± 48.2 | 94.4 * ± 38.1 | 31.5 ± 49.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mejía-Rodríguez, F.; Quezada-Sánchez, A.D.; Gómez-Humarán, I.M.; García-Feregrino, R.; García-Guerra, A.; Fernández-Gaxiola, A.C.; Neufeld, L.M. Differential Effects of Three Nutritional Supplements on the Nutrient Intake of Pregnant Women Enrolled in a Conditional Cash Transfer Program in Mexico: A Cluster Randomized Trial. Nutrients 2022, 14, 3003. https://doi.org/10.3390/nu14153003
Mejía-Rodríguez F, Quezada-Sánchez AD, Gómez-Humarán IM, García-Feregrino R, García-Guerra A, Fernández-Gaxiola AC, Neufeld LM. Differential Effects of Three Nutritional Supplements on the Nutrient Intake of Pregnant Women Enrolled in a Conditional Cash Transfer Program in Mexico: A Cluster Randomized Trial. Nutrients. 2022; 14(15):3003. https://doi.org/10.3390/nu14153003
Chicago/Turabian StyleMejía-Rodríguez, Fabiola, Amado D. Quezada-Sánchez, Ignacio Méndez Gómez-Humarán, Raquel García-Feregrino, Armando García-Guerra, Ana Cecilia Fernández-Gaxiola, and Lynnette M. Neufeld. 2022. "Differential Effects of Three Nutritional Supplements on the Nutrient Intake of Pregnant Women Enrolled in a Conditional Cash Transfer Program in Mexico: A Cluster Randomized Trial" Nutrients 14, no. 15: 3003. https://doi.org/10.3390/nu14153003