
Body Composition-Specific Asthma Phenotypes: Clinical Implications

 and
and
Abstract
:1. Introduction
2. Materials and Methods
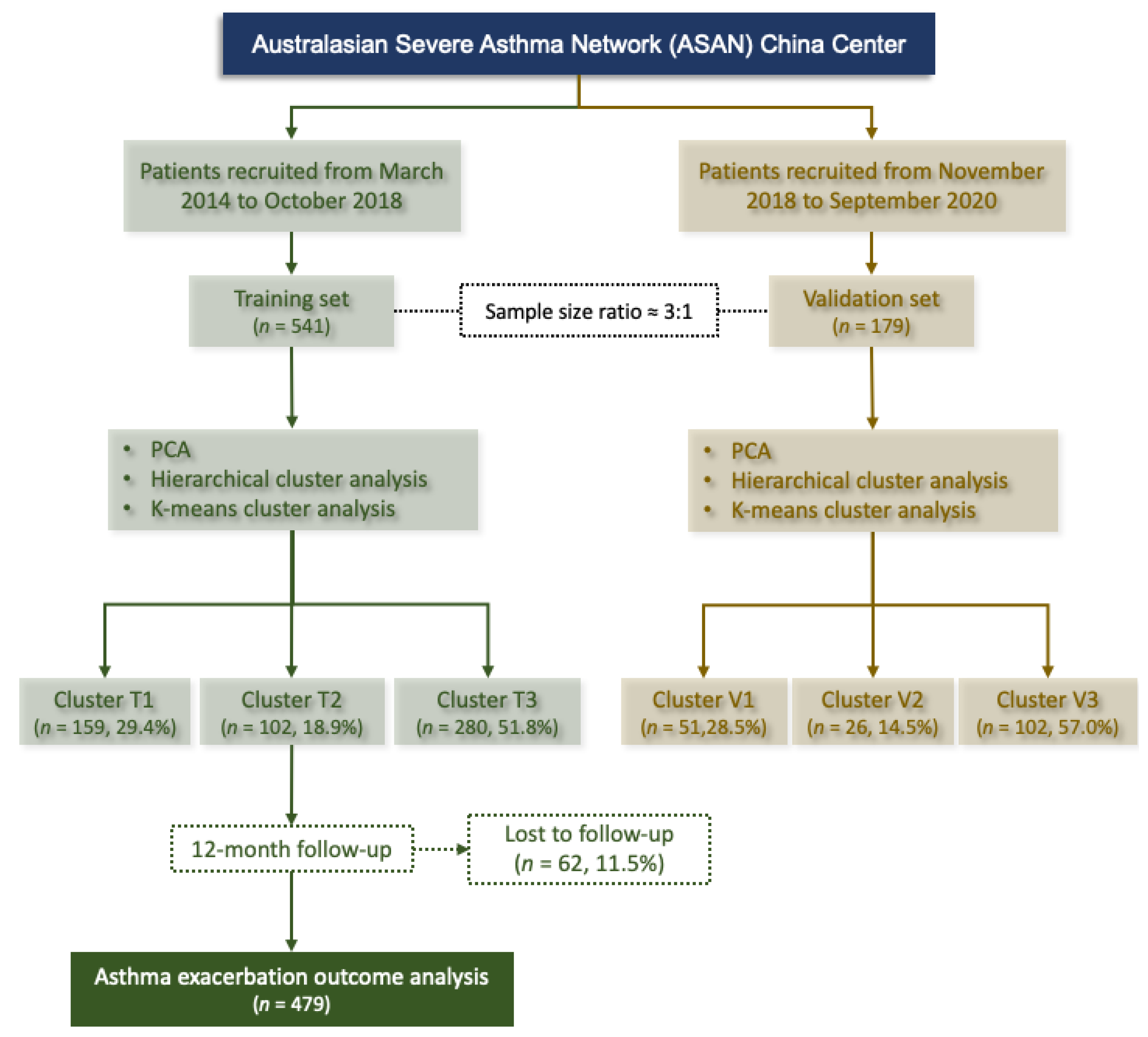
2.1. Study Design and Participants
2.2. Multidimensional Assessment and Data Collection
Measurements of Body Composition
2.3. Statistical Analysis
2.3.1. Principal Component Analysis (PCA)
2.3.2. Cluster Analysis
2.3.3. Other Analyses
3. Results
3.1. Training Cohort and Characteristics
3.2. Cluster Analysis and Description
3.2.1. Cluster T1 (Cluster 1 in the Training Set): Patients with Undernutrition
3.2.2. Cluster T2 (Cluster 2 in the Training Set): Intermediate Level of Nutrition with Psychological Dysfunction
3.2.3. Cluster T3 (Cluster 3 in the Training Set): Patients with Good Nutrition
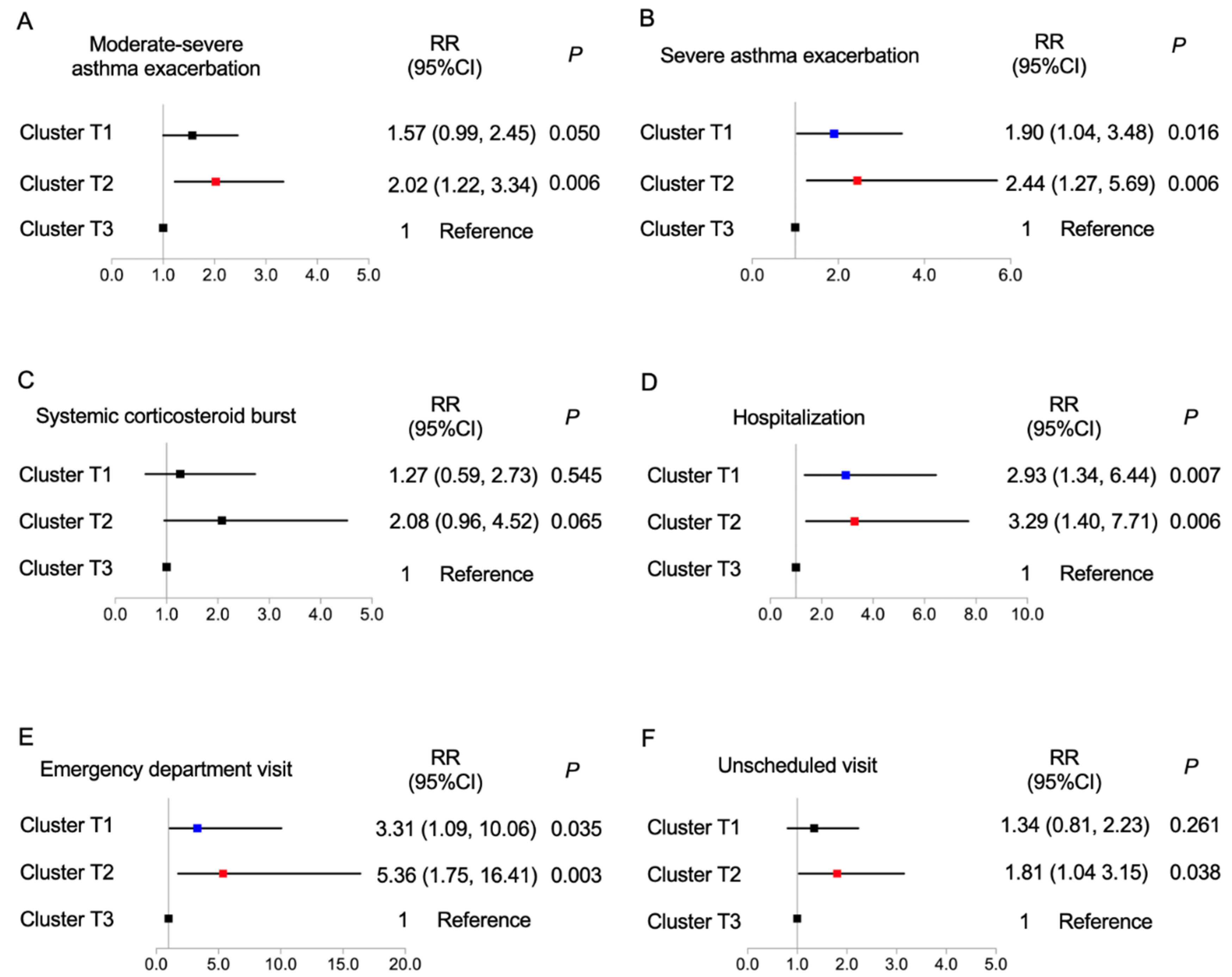
3.3. Asthma Exacerbations in the Following Year
3.4. Factors Associated with Current Asthma Control and Further Exacerbation
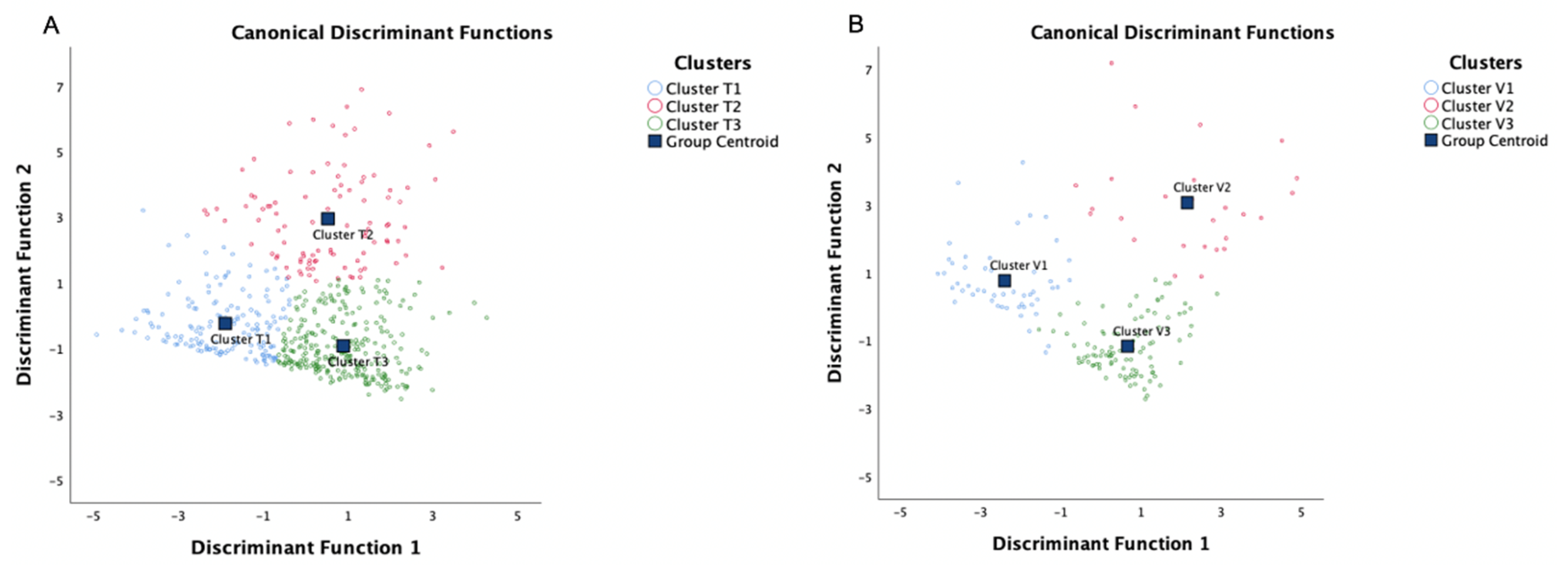
3.5. Internal and External Validation
3.5.1. Discriminant Analysis
3.5.2. Cluster Analysis in Validation Set
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nurmagambetov, T.; Kuwahara, R.; Garbe, P. The Economic Burden of Asthma in the United States, 2008–2013. Ann. Am. Thorac. Soc. 2018, 15, 348–356. [Google Scholar] [CrossRef]
- Zhang, X.; Zheng, J.; Zhang, L.; Liu, Y.; Chen, G.P.; Zhang, H.P.; Wang, L.; Kang, Y.; Wood, L.G.; Wang, G. Systemic inflammation mediates the detrimental effects of obesity on asthma control. Allergy Asthma Proc. 2018, 39, 43–50. [Google Scholar] [CrossRef]
- Deng, K.; Zhang, X.; Liu, Y.; Cheng, G.P.; Zhang, H.P.; Wang, T.; Wang, L.; Li, W.M.; Wang, G.; Wood, L. Visceral obesity is associated with clinical and inflammatory features of asthma: A prospective cohort study. Allergy Asthma Proc. 2020, 41, 348–356. [Google Scholar] [CrossRef]
- Holguin, F.; Bleecker, E.R.; Busse, W.W.; Calhoun, W.J.; Castro, M.; Erzurum, S.C.; Fitzpatrick, A.M.; Gaston, B.; Israel, E.; Jarjour, N.N.; et al. Obesity and asthma: An association modified by age of asthma onset. J. Allergy Clin. Immunol. 2011, 127, 1486–1493.e2. [Google Scholar] [CrossRef]
- Schatz, M.; Hsu, J.W.; Zeiger, R.S.; Chen, W.; Dorenbaum, A.; Chipps, B.E.; Haselkorn, T. Phenotypes determined by cluster analysis in severe or difficult-to-treat asthma. J. Allergy Clin. Immunol. 2014, 133, 1549–1556. [Google Scholar] [CrossRef]
- Muc, M.; Mota-Pinto, A.; Padez, C. Association between obesity and asthma—Epidemiology, pathophysiology and clinical profile. Nutr. Res. Rev. 2016, 29, 194–201. [Google Scholar] [CrossRef]
- Peters, U.; Dixon, A.E.; Forno, E. Obesity and asthma. J. Allergy Clin. Immunol. 2018, 141, 1169–1179. [Google Scholar] [CrossRef] [Green Version]
- Vortmann, M.; Eisner, M.D. BMI and health status among adults with asthma. Obesity 2008, 16, 146–152. [Google Scholar] [CrossRef]
- Boulet, L.P.; Franssen, E. Influence of obesity on response to fluticasone with or without salmeterol in moderate asthma. Respir. Med. 2007, 101, 2240–2247. [Google Scholar] [CrossRef] [Green Version]
- Miethe, S.; Karsonova, A.; Karaulov, A.; Renz, H. Obesity and asthma. J. Allergy Clin. Immunol. 2020, 146, 685–693. [Google Scholar] [CrossRef]
- Müller, M.J.; Bosy-Westphal, A.; Krawczak, M. Genetic studies of common types of obesity: A critique of the current use of phenotypes. Obes. Rev. 2010, 11, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J. From BMI to functional body composition. Eur. J. Clin. Nutr. 2013, 67, 1119–1121. [Google Scholar] [CrossRef] [PubMed]
- Connor Gorber, S.; Tremblay, M.; Moher, D.; Gorber, B. A comparison of direct vs. self-report measures for assessing height, weight and body mass index: A systematic review. Obes. Rev. 2007, 8, 307–326. [Google Scholar] [CrossRef]
- Hattori, A.; Sturm, R. The obesity epidemic and changes in self-report biases in BMI. Obesity 2013, 21, 856–860. [Google Scholar] [CrossRef]
- Thibault, R.; Pichard, C. The evaluation of body composition: A useful tool for clinical practice. Ann. Nutr. Metab. 2012, 60, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Bourdin, A.; Molinari, N.; Vachier, I.; Varrin, M.; Marin, G.; Gamez, A.S.; Paganin, F.; Chanez, P. Prognostic value of cluster analysis of severe asthma phenotypes. J. Allergy Clin. Immunol. 2014, 134, 1043–1050. [Google Scholar] [CrossRef]
- Freitas, P.D.; Xavier, R.F.; McDonald, V.M.; Gibson, P.G.; Cordova-Rivera, L.; Furlanetto, K.C.; de Oliveira, J.M.; Carvalho-Pinto, R.M.; Cukier, A.; Stelmach, R.; et al. Identification of asthma phenotypes based on extrapulmonary treatable traits. Eur. Respir. J. 2021, 57, 2000240. [Google Scholar] [CrossRef] [PubMed]
- Haldar, P.; Pavord, I.D.; Shaw, D.E.; Berry, M.A.; Thomas, M.; Brightling, C.E.; Wardlaw, A.J.; Green, R.H. Cluster analysis and clinical asthma phenotypes. Am. J. Respir. Crit. Care Med. 2008, 178, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Moore, W.C.; Meyers, D.A.; Wenzel, S.E.; Teague, W.G.; Li, H.; Li, X.; D’Agostino, R., Jr.; Castro, M.; Curran-Everett, D.; Fitzpatrick, A.M.; et al. Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program. Am. J. Respir. Crit. Care Med. 2010, 181, 315–323. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhang, L.; Wang, G.; Feng, M.; Liang, R.; McDonald, V.M.; Zhang, H.P.; Yu, H.; Liang, Z.A.; Wang, L.; et al. Clinical Phenotypes of Patients Hospitalized for an Asthma Exacerbation: Prognostic Implications. J. Allergy Clin. Immunol. Pract. 2021, 9, 830–841.e14. [Google Scholar] [CrossRef]
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. 2020. Available online: www.ginasthma.org (accessed on 25 August 2020).
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Reginster, J.Y.; Dardenne, N.; Croisiser, J.L.; Kaux, J.F.; Beaudart, C.; Slomian, J.; Bruyère, O. Concordance between muscle mass assessed by bioelectrical impedance analysis and by dual energy X-ray absorptiometry: A cross-sectional study. BMC Musculoskelet. Disord. 2015, 16, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, K.; Inage, K.; Eguchi, Y.; Orita, S.; Toyoguchi, T.; Yamauchi, K.; Suzuki, M.; Kubota, G.; Sainoh, T.; Sato, J.; et al. Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analysis are Beneficial Tools for Measuring the Trunk Muscle Mass of Patients with Low Back Pain. Spine Surg. Relat. Res. 2019, 3, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between Dual-Energy X-ray Absorptiometry and Bioelectrical Impedance Analyses for Accuracy in Measuring Whole Body Muscle Mass and Appendicular Skeletal Muscle Mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef] [Green Version]
- Deng, K.; Zhang, X.; Liu, Y.; Zhang, L.; Wang, G.; Feng, M.; Oliver, B.G.; Wang, L.; Hansbro, P.M.; Qin, L.; et al. Heterogeneity of Paucigranulocytic Asthma: A Prospective Cohort Study with Hierarchical Cluster Analysis. J. Allergy Clin. Immunol. Pract. 2021, 9, 2344–2355. [Google Scholar] [CrossRef]
- Moore, W.C.; Hastie, A.T.; Li, X.; Li, H.; Busse, W.W.; Jarjour, N.N.; Wenzel, S.E.; Peters, S.P.; Meyers, D.A.; Bleecker, E.R. Sputum neutrophil counts are associated with more severe asthma phenotypes using cluster analysis. J. Allergy Clin. Immunol. 2014, 133, 1557–1563.e5. [Google Scholar] [CrossRef] [Green Version]
- Qiu, R.; Xie, J.; Chung, K.F.; Li, N.; Yang, Z.; He, M.; Li, J.; Chen, R.; Zhong, N.; Zhang, Q. Asthma Phenotypes Defined from Parameters Obtained during Recovery from a Hospital-Treated Exacerbation. J. Allergy Clin. Immunol. Pract. 2018, 6, 1960–1967. [Google Scholar] [CrossRef]
- Turner, J.H.; Chandra, R.K.; Li, P.; Bonnet, K.; Schlundt, D.G. Identification of clinically relevant chronic rhinosinusitis endotypes using cluster analysis of mucus cytokines. J. Allergy Clin. Immunol. 2018, 141, 1895–1897.e7. [Google Scholar] [CrossRef] [Green Version]
- Bacharier, L.B.; Beigelman, A.; Calatroni, A.; Jackson, D.J.; Gergen, P.J.; O’Connor, G.T.; Kattan, M.; Wood, R.A.; Sandel, M.T.; Lynch, S.V.; et al. Longitudinal Phenotypes of Respiratory Health in a High-Risk Urban Birth Cohort. Am. J. Respir. Crit. Care Med. 2019, 199, 71–82. [Google Scholar] [CrossRef]
- Segar, M.W.; Patel, K.V.; Ayers, C.; Basit, M.; Tang, W.H.W.; Willett, D.; Berry, J.; Grodin, J.L.; Pandey, A. Phenomapping of patients with heart failure with preserved ejection fraction using machine learning-based unsupervised cluster analysis. Eur. J. Heart Fail. 2020, 22, 148–158. [Google Scholar] [CrossRef]
- De Vries, R.; Brinkman, P.; van der Schee, M.P.; Fens, N.; Dijkers, E.; Bootsma, S.K.; de Jongh, F.H.; Sterk, P.J. Integration of electronic nose technology with spirometry: Validation of a new approach for exhaled breath analysis. J. Breath Res. 2015, 9, 046001. [Google Scholar] [CrossRef] [PubMed]
- Yeomans, K.A.; Golder, P.A. The Guttman-Kaiser Criterion as a predictor of the number of common factors. J. R Stat. Soc. Ser. D Stat. 1982, 31, 221–229. [Google Scholar] [CrossRef]
- Brinkman, P.; van de Pol, M.A.; Gerritsen, M.G.; Bos, L.D.; Dekker, T.; Smids, B.S.; Sinha, A.; Majoor, C.J.; Sneeboer, M.M.; Knobel, H.H.; et al. Exhaled breath profiles in the monitoring of loss of control and clinical recovery in asthma. Clin. Exp. Allergy 2017, 47, 1159–1169. [Google Scholar] [CrossRef]
- De Vries, R.; Dagelet, Y.W.F.; Spoor, P.; Snoey, E.; Jak, P.M.C.; Brinkman, P.; Dijkers, E.; Bootsma, S.K.; Elskamp, F.; de Jongh, F.H.C.; et al. Clinical and inflammatory phenotyping by breathomics in chronic airway diseases irrespective of the diagnostic label. Eur. Respir. J. 2018, 51, 1701817. [Google Scholar] [CrossRef] [Green Version]
- Xavier, R.F.; Pereira, A.; Lopes, A.C.; Cavalheri, V.; Pinto, R.M.C.; Cukier, A.; Ramos, E.M.C.; Carvalho, C.R.F. Identification of Phenotypes in People with COPD: Influence of Physical Activity, Sedentary Behaviour, Body Composition and Skeletal Muscle Strength. Lung 2019, 197, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, P.; Tuomisto, L.E.; Niemelä, O.; Tommola, M.; Haanpää, J.; Kankaanranta, H. Cluster Analysis on Longitudinal Data of Patients with Adult-Onset Asthma. J. Allergy Clin. Immunol. Pract. 2017, 5, 967–978.e3. [Google Scholar] [CrossRef]
- Nakayama, T.; Asaka, D.; Yoshikawa, M.; Okushi, T.; Matsuwaki, Y.; Moriyama, H.; Otori, N. Identification of chronic rhinosinusitis phenotypes using cluster analysis. Am. J. Rhinol. Allergy 2012, 26, 172–176. [Google Scholar] [CrossRef]
- Kurukulaaratchy, R.J.; Zhang, H.; Raza, A.; Patil, V.; Karmaus, W.; Ewart, S.; Arshad, S.H. The diversity of young adult wheeze: A cluster analysis in a longitudinal birth cohort. Clin. Exp. Allergy 2014, 44, 724–735. [Google Scholar] [CrossRef] [Green Version]
- Milligan, G.W.; Cooper, M.C. An examination of procedures for determining the number of clusters in a data set. Psychometrika 1985, 50, 159–179. [Google Scholar] [CrossRef]
- Ward, W.J., Jr. Hierarchical Grouping to Optimize an Objective Function. JASA 1963, 58, 236–244. [Google Scholar] [CrossRef]
- Kaufman, L.; Rousseeuw, P.J. Finding Groups in Data: An Introduction to Cluster Analysis: DBLP; John Wiley & Sons: New York, NY, USA, 1990. [Google Scholar]
- Alhamdan, A.A.; Almuammar, M.N.; Bindawas, S.M.; Alshammari, S.A.; Al-Amoud, M.M.; Calder, P.C. Body composition analysis by bioelectrical impedance and its relationship with nutritional status in older adults: A cross-sectional descriptive study. Prog. Nutr. 2020, 23, e2021082. [Google Scholar]
- Haas, V.K.; Kohn, M.R.; Clarke, S.D.; Allen, J.R.; Madden, S.; Müller, M.J.; Gaskin, K.J. Body composition changes in female adolescents with anorexia nervosa. Am. J. Clin. Nutr. 2009, 89, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Walley, A.J.; Asher, J.E.; Froguel, P. The genetic contribution to non-syndromic human obesity. Nat. Rev. Genet. 2009, 10, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Argilés, J.M.; López-Soriano, J.; Almendro, V.; Busquets, S.; López-Soriano, F.J. Cross-talk between skeletal muscle and adipose tissue: A link with obesity? Med. Res. Rev. 2005, 25, 49–65. [Google Scholar] [CrossRef] [PubMed]
- Havekes, B.; Sauerwein, H.P. Adipocyte-myocyte crosstalk in skeletal muscle insulin resistance; is there a role for thyroid hormone? Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 641–646. [Google Scholar] [CrossRef]
- Lee, D.E.; Kehlenbrink, S.; Lee, H.; Hawkins, M.; Yudkin, J.S. Getting the message across: Mechanisms of physiological cross talk by adipose tissue. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E1210–E1229. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef]
- Taube, A.; Schlich, R.; Sell, H.; Eckardt, K.; Eckel, J. Inflammation and metabolic dysfunction: Links to cardiovascular diseases. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, H2148–H2165. [Google Scholar] [CrossRef]
- Trayhurn, P.; Drevon, C.A.; Eckel, J. Secreted proteins from adipose tissue and skeletal muscle—Adipokines, myokines and adipose/muscle cross-talk. Arch. Physiol. Biochem. 2011, 117, 47–56. [Google Scholar] [CrossRef]
- Kostikas, K.; Brindicci, C.; Patalano, F. Blood Eosinophils as Biomarkers to Drive Treatment Choices in Asthma and COPD. Curr. Drug Targets 2018, 19, 1882–1896. [Google Scholar] [CrossRef]
- Fitzpatrick, A.M.; Teague, W.G.; Meyers, D.A.; Peters, S.P.; Li, X.; Li, H.; Wenzel, S.E.; Aujla, S.; Castro, M.; Bacharier, L.B.; et al. Heterogeneity of severe asthma in childhood: Confirmation by cluster analysis of children in the National Institutes of Health/National Heart, Lung, and Blood Institute Severe Asthma Research Program. J. Allergy Clin. Immunol. 2011, 127, e1–e13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, T.J.; Cowan, J.O.; Young, S.; Goulding, A.; Grant, A.M.; Williamson, A.; Brassett, K.; Herbison, G.P.; Taylor, D.R. The association between obesity and asthma: Interactions between systemic and airway inflammation. Am. J. Respir. Crit. Care Med. 2008, 178, 469–475. [Google Scholar] [CrossRef] [PubMed]
- McDonald, V.M.; Hiles, S.A.; Godbout, K.; Harvey, E.S.; Marks, G.B.; Hew, M.; Peters, M.; Bardin, P.G.; Reynolds, P.N.; Upham, J.W.; et al. Treatable traits can be identified in a severe asthma registry and predict future exacerbations. Respirology 2019, 24, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Miranda, C.; Busacker, A.; Balzar, S.; Trudeau, J.; Wenzel, S.E. Distinguishing severe asthma phenotypes: Role of age at onset and eosinophilic inflammation. J. Allergy Clin. Immunol. 2004, 113, 101–108. [Google Scholar] [CrossRef]
- Juniper, E.F.; O’Byrne, P.M.; Guyatt, G.H.; Ferrie, P.J.; King, D.R. Development and validation of a questionnaire to measure asthma control. Eur. Respir. J. 1999, 14, 902–907. [Google Scholar] [CrossRef] [PubMed]
- Leite, M.; Ponte, E.V.; Petroni, J.; D’Oliveira Júnior, A.; Pizzichini, E.; Cruz, A.A. Evaluation of the asthma control questionnaire validated for use in Brazil. J. Bras. Pneumol. Publicacao Soc. Bras. Pneumol. Tisilogia 2008, 34, 756–763. [Google Scholar] [CrossRef] [Green Version]
- Juniper, E.F.; Bousquet, J.; Abetz, L.; Bateman, E.D. Identifying ‘well-controlled’ and ‘not well-controlled’ asthma using the Asthma Control Questionnaire. Respir. Med. 2006, 100, 616–621. [Google Scholar] [CrossRef] [Green Version]
- Juniper, E.F.; Guyatt, G.H.; Epstein, R.S.; Ferrie, P.J.; Jaeschke, R.; Hiller, T.K. Evaluation of impairment of health related quality of life in asthma: Development of a questionnaire for use in clinical trials. Thorax 1992, 47, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Gibson, P.G.; Yang, I.A.; Upham, J.W.; Reynolds, P.N.; Hodge, S.; James, A.L.; Jenkins, C.; Peters, M.J.; Marks, G.B.; Baraket, M.; et al. Effect of azithromycin on asthma exacerbations and quality of life in adults with persistent uncontrolled asthma (AMAZES): A randomised, double-blind, placebo-controlled trial. Lancet 2017, 390, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.P.; Boushey, H.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. An official American Thoracic Society/European Respiratory Society statement: Asthma control and exacerbations: Standardizing endpoints for clinical asthma trials and clinical practice. Am. J. Respir. Crit. Care Med. 2009, 180, 59–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, C.C.; Chumlea, W.C.; Roche, A. Stature, Recumbent Length, Weight; Human Kinetics Books: Champaign, IL, USA, 1988; pp. 3–8. [Google Scholar]
- Lohman, T.J.; Roache, A.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988. [Google Scholar]
- InBody770. Premium Solution for Your Health. Available online: https://www.inbodyusa.com/pages/inbodys10 (accessed on 1 March 2014).
- Wanger, J.; Clausen, J.L.; Coates, A.; Pedersen, O.F.; Brusasco, V.; Burgos, F.; Casaburi, R.; Crapo, R.; Enright, P.; van der Grinten, C.P.; et al. Standardisation of the measurement of lung volumes. Eur. Respir. J. 2005, 26, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.C.; Plummer, A.L.; Taylor, D.R. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.Y.; Zhang, X.; Wang, J.; Wang, G.; Oliver, B.G.; Zhang, H.P.; Kang, Y.; Wang, L.; Qiu, Z.X.; Li, W.M.; et al. Multidimensional Assessment of Asthma Identifies Clinically Relevant Phenotype Overlap: A Cross-Sectional Study. J. Allergy Clin. Immunol. Pract. 2021, 9, 349–362.e18. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Cluster T1 | Cluster T2 | Cluster T3 | Total | F/χ2/H | p-Value |
|---|---|---|---|---|---|---|
| n (%) | 159 (29.4) | 102 (18.9) | 280 (51.8) | 541 | - | - |
| Anthropometric/asthma data | ||||||
| Age, years, median (Q1, Q3) | 59.0 (51.0, 68.0) | 48.0 (40.0, 58.0) * | 46.0 (36.0, 53.0) * | 49.0 (39.0, 58.0) | 67.620 | <0.001 |
| Female, n (%) | 89 (56.0) | 68 (66.7) | 193 (68.9) † | 350 (64.7) | 7.664 | 0.022 |
| BMI, kg/m2 | ||||||
| Median (Q1, Q3) | 22.36 (19.97, 24.15) | 22.83 (20.59, 25.01) | 23.15 (20.95, 25.33) * | 22.73 (20.69, 24.77) | 8.196 | 0.017 |
| <25, n (%) | 133 (83.6) | 76 (74.5) | 205 (73.2) | 414 (76.5) | 7.675 | 0.104 |
| 25 ≤ BMI < 30, n (%) | 23 (14.5) | 21 (20.6) | 58 (20.7) | 102 (18.9) | ||
| ≥30, n (%) | 3 (1.9) | 5 (4.9) | 17 (6.1) | 25 (4.6) | ||
| WHR, median (Q1, Q3) | 0.89 (0.83, 0.93) | 0.87 (0.82, 0.92) | 0.87 (0.82, 0.92) | 0.87 (0.82, 0.92) | 4.251 | 0.119 |
| Atopy, n (%) | 52 (32.7) | 32 (31.4) | 155(55.4) ††† | 239 (44.2) | 29.459 | <0.001 |
| Asthma duration, years, median (Q1, Q3) | 7.0 (3.0, 16.0) | 8.0 (4.0, 15.0) | 6.0 (3.0 13.0) | 6.0 (3.0, 15.0) | 1.254 | 0.534 |
| Early-onset asthma, n (%) | 22 (13.8) | 17 (16.7) | 57 (20.4) | 96 (17.7) | 3.054 | 0.217 |
| History of family asthma, n (%) | 72 (45.3) | 30 (29.4) † | 89 (31.8) † | 191 (35.3) | 12.084 | 0.017 |
| Eosinophilic asthma, n (%) | 86 (54.1) | 70 (68.6) | 197 (70.4) †† | 353 (65.2) | 12.471 | 0.002 |
| Medications | ||||||
| ICS (BDP equivalent) dose, μg/day, median (Q1, Q3) | 400.0 (400.0, 1000.0) | 400.0 (400.0, 1000.0) | 400.0 (400.0, 1000.0) | 400.0 (400.0, 1000.0) | 2.404 | 0.301 |
| ICS/LABA, n (%) | 91 (57.2) | 58 (56.9) | 161 (57.5) | 310 (57.3) | 0.013 | 0.994 |
| Theophylline, n (%) | 28 (17.6) | 18 (17.6) | 35 (12.5) | 81 (15.0) | 2.787 | 0.248 |
| Leukotriene, n (%) | 48 (30.2) | 39 (38.2) | 103 (36.8) | 190 (35.1) | 2.472 | 0.291 |
| OCS, n (%) | 6 (3.8) | 2 (2.0) | 9 (3.2) | 17 (3.1) | 0.739 | 0.691 |
| Asthma control | ||||||
| Uncontrolled asthma (ACQ scores ≥ 0.75) | 88 (55.3) | 54 (52.9) | 106 (37.9) †††§ | 248 (45.8) | 15.046 | 0.001 |
| Health status | ||||||
| AQLQ scores, median (Q1, Q3) | 6.16 (5.58, 6.69) | 5.40 (5.00, 6.16) * | 6.25 (5.50, 6.61) ** | 5.96 (5.35, 6.47) | 13.069 | 0.001 |
| HADS-D | ||||||
| Median (Q1, Q3) | 1.0 (0, 1.5) | 6.0 (5.0, 9.0) * | 0.5 (0, 2.0) ** | 1.0 (0.0, 3.0) | 228.027 | <0.001 |
| ≥8, n (%) | 0 (0) | 37 (36.3) ††† | 0 (0) §§§ | 37 (6.8) | 170.936 | <0.001 |
| HADS-A | ||||||
| Median (Q1, Q3) | 1.0 (0, 2.0) | 6.0 (5.0, 8.0) * | 1.0 (0, 2.0) ** | 1.0 (0.0, 4.0) | 218.796 | <0.001 |
| ≥8, n (%) | 0 (0) | 35 (34.3) ††† | 0 (0.0) §§§ | 35 (6.5) | 161.057 | <0.001 |
| Both HADS-D and HADS-A ≥ 8, n (%) | 0 (0) | 18 (17.6) ††† | 0 (0.0) §§§ | 18 (3.3) | 80.137 | <0.001 |
| SAEs in the past 12 months, n (%) | 55 (34.6) | 35 (34.3) | 68 (24.3) | 158 (29.2) | 6.796 | 0.033 |
| Spirometry | ||||||
| Pre-FEV1, L, median (Q1, Q3) | 1.43 (1.15, 1.71) | 2.01 (1.62, 2.43) * | 2.49 (2.12, 2.95) *,** | 2.09 (1.56, 2.65) | 225.536 | <0.001 |
| Pre-FEV1 % predicted, median (Q1, Q3) | 56.0 (44.5, 68.0) | 72.0 (58.0, 86.0) * | 84.0 (72.0, 94.0) *,** | 74.0 (59.0, 88.0) | 182.736 | <0.001 |
| Pre-FEV1/FVC, %, median (Q1, Q3) | 55.91 (47.18, 62.97) | 66.02 (56.99, 75.07) * | 72.98 (65.97, 80.53) *,** | 67.19 (57.49, 76.03) | 161.758 | <0.001 |
| ΔFEV1, %, median (Q1, Q3) | 16.15 (9.10, 30.80) ** | 11.38 (6.30, 19.46) | 10.10 (4.58, 16.13) * | 11.90 (5.95, 19.39) | 39.457 | <0.001 |
| ΔFEV1/FVC, %, median (Q1, Q3) | 6.79 (1.23, 13.60) | 6.90 (1.00, 12.00) | 6.58 (3.57, 10.49) | 6.65 (2.52, 11.61) | 1.236 | 0.539 |
| FeNO, ppb, median (Q1, Q3) | 26.00 (16.00, 46.41) | 37.50 (22.00, 71.00) * | 52.50 (25.00, 96.50) *, ** | 40.0 (21.0, 75.00) | 53.732 | <0.001 |
| Comorbidities, n (%) | ||||||
| Rhinitis | 69 (43.4) | 63 (61.8) †† | 175 (62.5) ††† | 307 (56.7) | 16.368 | <0.001 |
| Nasal polyps | 15 (9.4) | 15 (14.7) | 20 (7.1) | 50 (9.2) | 5.108 | 0.078 |
| Bronchiectasis | 11 (6.9) | 8 (7.8) | 6 (2.1) †,§§ | 25 (4.6) | 8.500 | 0.014 |
| Sleep apnea | 2 (1.3) | 0 (0.0) | 4 (1.4) | 6 (1.1) | 2.545 | 0.280 |
| GERD | 9 (5.7) | 6 (5.9) | 11 (3.9) | 26 (4.8) | 0.984 | 0.612 |
| Diabetes | 8 (5.0) | 2 (2.0) | 3 (1.1) † | 13 (2.4) | 6.331 | 0.042 |
| Eczema | 20 (12.6) | 22 (21.6) | 49 (17.5) | 91 (16.8) | 3.781 | 0.151 |
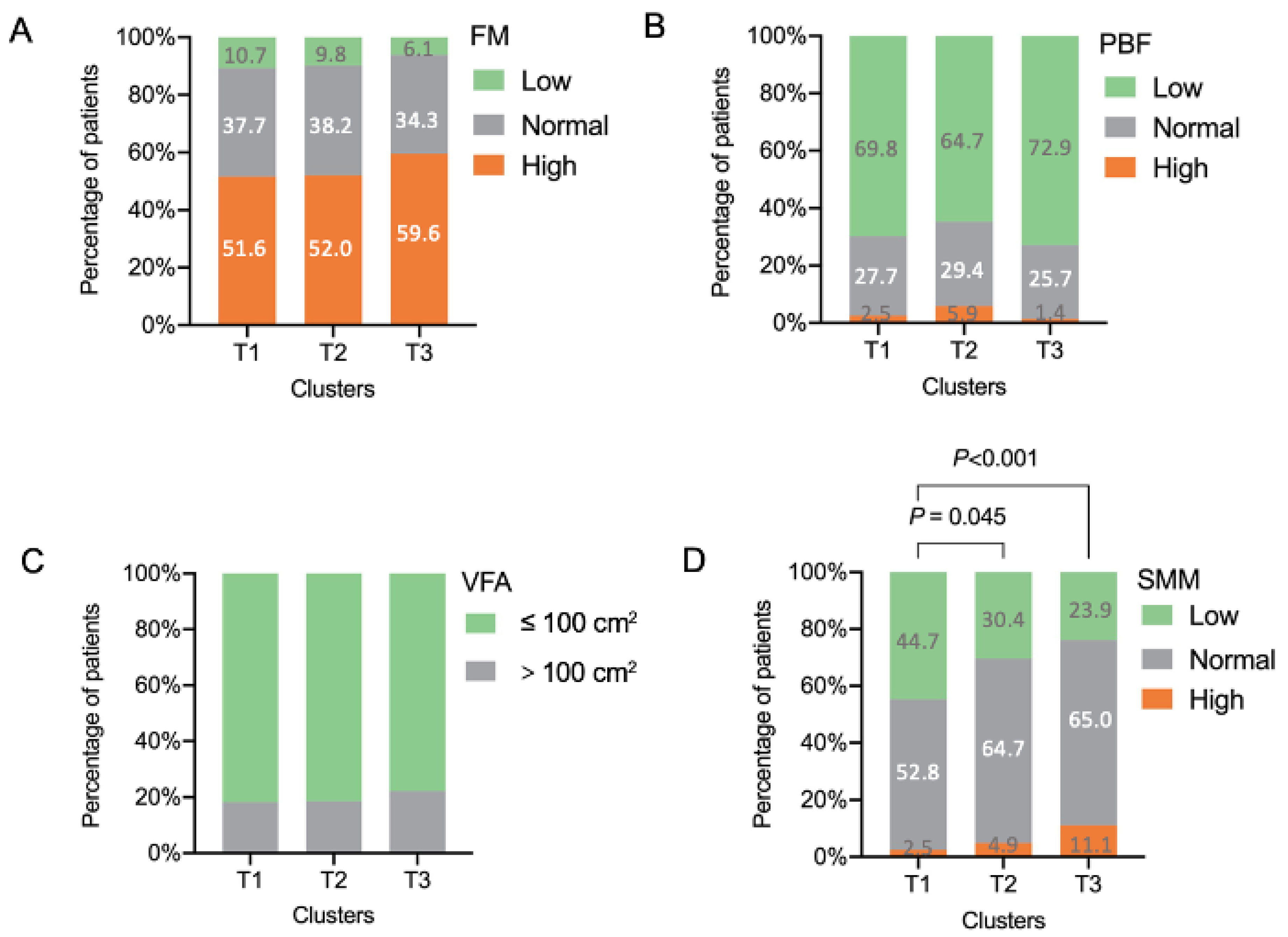
| Body composition, mean (SD) | ||||||
| FM, kg | 15.24 (5.41) | 16.52 (6.25) | 17.84 (6.27) # | 16.83 (6.13) | 9.591 | <0.001 |
| PBF, % | 27.24 (7.50) | 27.97 (8.19) | 29.15 (6.98) # | 28.36 (7.41) | 3.573 | 0.029 |
| VFA, cm2 | 70.66 (29.84) | 75.50 (34.13) | 78.52 (31.63) # | 75.64 (31.73) | 3.139 | 0.044 |
| SMM, kg | 21.57 (4.07) | 22.75 (4.71) | 23.29 (4.99) #,## | 22.69 (4.73) | 6.868 | 0.001 |
| Variables | Cluster T1 | Cluster T2 | Cluster T3 | Total | H | p-Value |
|---|---|---|---|---|---|---|
| n (%) | 159 (29.4) | 102 (18.9) | 280 (51.8) | 541 | - | - |
| Peripheral blood, median (Q1, Q3) | ||||||
| Eosinophils, × 109/L | 0.19 (0.11, 0.34) | 0.24 (0.13, 0.38) | 0.27 (0.15, 0.42) * | 0.21 (0.12, 0.33) | 11.581 | 0.003 |
| Neutrophils, × 109/L | 3.37 (2.57, 4.36) | 3.02 (2.46, 4.21) | 3.32 (2.67, 4.13) | 3.27 (2.63, 3.92) | 0.854 | 0.653 |
| Lymphocytes, × 109/L | 1.68 (1.39, 2.06) | 1.58 (1.31, 1.88) | 1.67 (1.40, 1.92) | 1.71 (1.40, 2.07) | 4.094 | 0.129 |
| Monocytes, × 109/L | 0.36 (0.27, 0.48) | 0.31 (0.24, 0.42) | 0.33 (0.27, 0.41) | 0.33 (0.27, 0.42) | 4.977 | 0.083 |
| Basophils, × 109/L, median (Q1, Q3) | 0.03 (0.02, 0.05) | 0.04 (0.02, 0.05) | 0.04 (0.02, 0.05) | 0.03 (0.02, 0.05) | 0.168 | 0.920 |
| IgE, IU/mL | 75.65 (33.60, 205.00) | 126.00 (41.97, 304.95) * | 164.50 (65.20, 359.00) * | 92.85 (36.67, 302.45) | 18.264 | <0.001 |
| Sputum, median (Q1, Q3) | ||||||
| Eosinophils, % | 0.25 (0, 1.75) | 0.25 (0, 1.50) | 0.50 (0.25, 1.50) | 0.25 (0, 3.00) | 2.212 | 0.331 |
| Neutrophils, % | 56.5 (31.00, 81.62) | 35.00 (13.25, 68.00) * | 32.88 (15.13, 62.25) * | 42.63 (17.00, 71.88) | 14.869 | 0.001 |
| Lymphocytes, % | 0.50 (0, 1.00) | 0.50 (0.25, 1.50) | 0.50 (0.25, 1.50) | 0.50 (0.25, 1.25) | 4.272 | 0.118 |
| Macrophages, % | 34.88 (11.50, 61.25) | 47.88 (17.00, 81.50) * | 58.13 (28.63, 78.99) * | 46.25 (19.38, 73.88) | 15.745 | <0.001 |
| Outcomes | Cluster T1 | Cluster T2 | Cluster T3 | Total | χ2/H | p-Value |
|---|---|---|---|---|---|---|
| n (%) | 149 (31.1) | 79 (16.5) | 251 (52.4) | 479 | ||
| Moderate-to-severe asthma exacerbation | ||||||
| n (%) | 39 (26.2) | 24 (30.4) | 61 (24.3) | 124 (25.9) | 1.166 | 0.558 |
| Mean (SD) | 2.53 (3.01) | 2.39 (1.84) | 2.03 (1.64) | 2.29 (2.23) | 1.467 | 0.480 |
| Severe asthma exacerbation | ||||||
| n (%) | 23 (15.4) | 15 (19.0) | 22 (8.8) § | 60 (12.6) | 7.230 | 0.027 |
| Mean (SD) | 1.92 (1.67) | 2.37 (1.64) | 1.38 (0.88) ** | 1.85 (1.46) | 9.178 | 0.010 |
| Systemic corticosteroid burst | ||||||
| n (%) | 13 (8.7) | 10 (12.7) | 16 (6.4) | 39 (8.1) | 3.271 | 0.195 |
| Mean (SD) | 1.58 (0.79) | 2.17 (1.4) | 1.38 (1.02) ** | 1.68 (1.12) | 6.025 | 0.049 |
| Hospitalization | ||||||
| n (%) | 16 (10.7) | 10 (12.7) | 12 (4.8) § | 38 (7.9) | 7.435 | 0.024 |
| Mean (SD) | 1.24 (0.56) | 1.92 (0.79) * | 1.08 (0.51) ** | 1.39 (0.7) | 9.981 | 0.007 |
| Emergency department visit | ||||||
| n (%) | 9 (6.0) | 6 (7.6) | 4 (1.6) †,§ | 19 (4.0) | 8.123 | 0.017 |
| Mean (SD) | 2.11 (2.62) | 2.5 (1.93) | 1 (0.1) ** | 2 (2.05) | 6.461 | 0.040 |
| Unscheduled visit | ||||||
| n (%) | 24 (16.1) | 15 (19.0) | 46 (18.3) | 85 (17.7) | 0.415 | 0.812 |
| Mean (SD) | 2.43 (2.26) | 2.15 (1.53) | 2.02 (1.58) | 2.18 (1.8) | 0.780 | 0.677 |
| Step | Variables | Tolerance | Sig. of F to Remove | Wilks’ Lambda |
|---|---|---|---|---|
| 1 | HADS-D | 1.000 | <0.001 | |
| 2 | HADS-D | 0.993 | <0.001 | 0.659 |
| Pre-FEV1% | 0.993 | <0.001 | 0.423 | |
| 3 | HADS-D | 0.991 | <0.001 | 0.498 |
| Pre-FEV1% | 0.984 | <0.001 | 0.302 | |
| Age | 0.991 | <0.001 | 0.277 | |
| 4 | HADS-D | 0.880 | <0.001 | 0.222 |
| Pre-FEV1% | 0.976 | <0.001 | 0.240 | |
| Age | 0.989 | <0.001 | 0.222 | |
| HADS-A | 0.883 | <0.001 | 0.209 | |
| 5 | HADS-D | 0.880 | <0.001 | 0.204 |
| Pre-FEV1% | 0.960 | <0.001 | 0.226 | |
| Age | 0.907 | <0.001 | 0.217 | |
| HADS-A | 0.877 | <0.001 | 0.194 | |
| VFA | 0.902 | <0.001 | 0.168 | |
| 6 | HADS-D | 0.878 | <0.001 | 0.200 |
| Pre-FEV1% | 0.957 | <0.001 | 0.222 | |
| Age | 0.906 | <0.001 | 0.212 | |
| HADS-A | 0.876 | <0.001 | 0.190 | |
| VFA | 0.895 | <0.001 | 0.163 | |
| SMM | 0.984 | <0.001 | 0.155 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Deng, K.; Yuan, Y.; Liu, L.; Zhang, S.; Wang, C.; Wang, G.; Zhang, H.; Wang, L.; Cheng, G.; et al. Body Composition-Specific Asthma Phenotypes: Clinical Implications. Nutrients 2022, 14, 2525. https://doi.org/10.3390/nu14122525
Zhang X, Deng K, Yuan Y, Liu L, Zhang S, Wang C, Wang G, Zhang H, Wang L, Cheng G, et al. Body Composition-Specific Asthma Phenotypes: Clinical Implications. Nutrients. 2022; 14(12):2525. https://doi.org/10.3390/nu14122525
Chicago/Turabian StyleZhang, Xin, Ke Deng, Yulai Yuan, Lei Liu, Shuwen Zhang, Changyong Wang, Gang Wang, Hongping Zhang, Lei Wang, Gaiping Cheng, and et al. 2022. "Body Composition-Specific Asthma Phenotypes: Clinical Implications" Nutrients 14, no. 12: 2525. https://doi.org/10.3390/nu14122525