
Lower Geriatric Nutritional Risk Index (GNRI) Is Associated with Higher Risk of Fractures in Patients Undergoing Hemodialysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Calculation of the GNRI
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Factors Associated with a Low GNRI (<92)
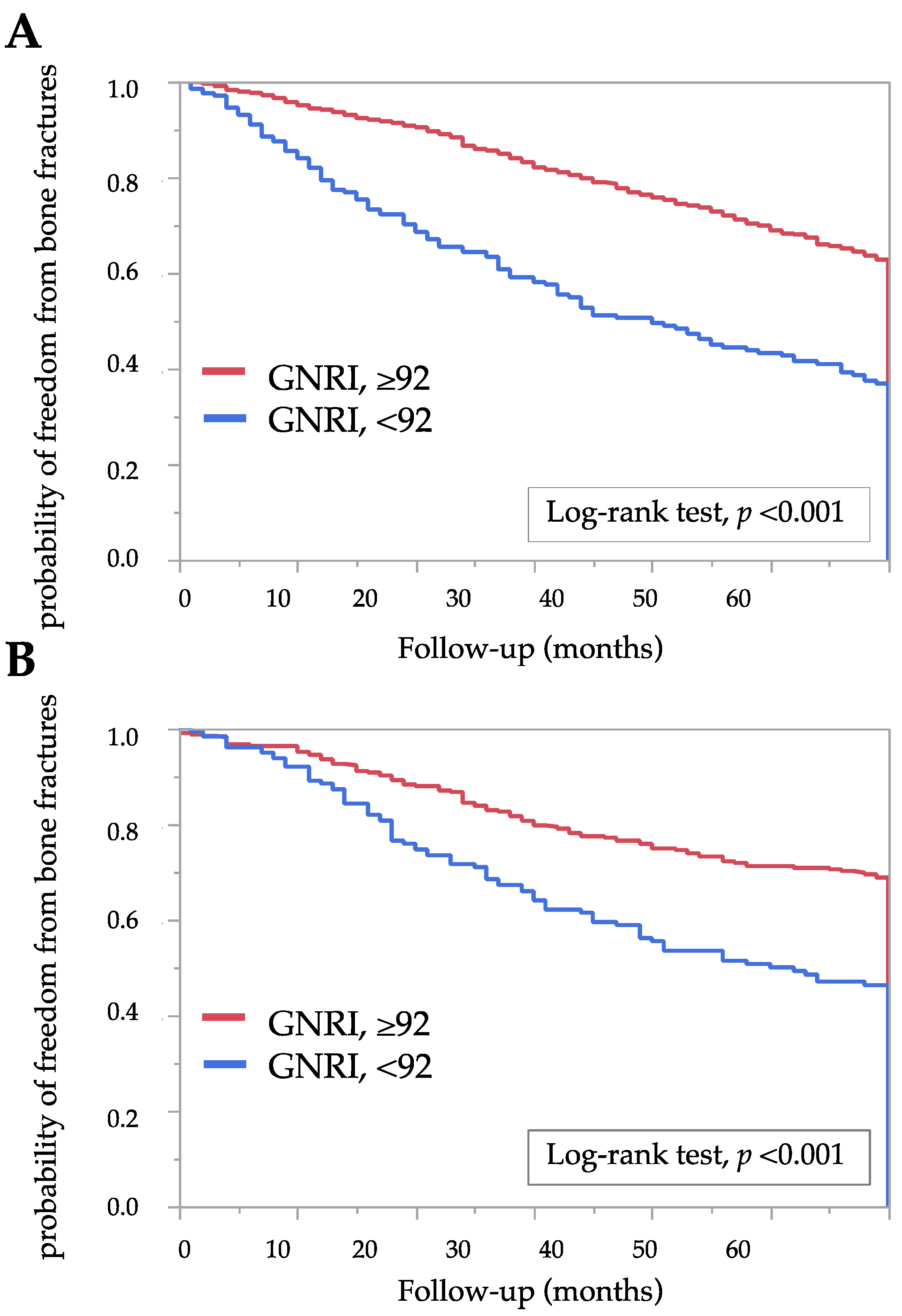
3.3. Association between the GNRI and Risk of Bone Fractures
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alem, A.M.; Sherrard, D.J.; Gillen, D.L.; Weiss, N.S.; Beresford, S.A.; Heckbert, S.R.; Wong, C.; Stehman-Breen, C. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int. 2000, 58, 396–399. [Google Scholar] [CrossRef] [Green Version]
- Danese, M.D.; Kim, J.; Doan, Q.V.; Dylan, M.; Griffiths, R.; Chertow, G.M. PTH and the Risks for Hip, Vertebral, and Pelvic Fractures Among Patients on Dialysis. Am. J. Kidney Dis. 2006, 47, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Tentori, F.; McCullough, K.; Kilpatrick, R.D.; Bradbury, B.D.; Robinson, B.M.; Kerr, P.G.; Pisoni, R.L. High rates of death and hospitalization follow bone fracture among hemodialysis patients. Kidney Int. 2014, 85, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, R.; Kopple, J.D. Nutritional management of maintenance dialysis patients: Why Aren’t We Doing Better? Annu. Rev. Nutr. 2001, 21, 343–379. [Google Scholar] [CrossRef] [PubMed]
- Pifer, T.B.; Mccullough, K.P.; Port, F.K.; Goodkin, D.A.; Maroni, B.J.; Held, P.J.; Young, E.W. Mortality risk in hemodialysis patients and changes in nutritional indicators: DOPPS. Kidney Int. 2002, 62, 2238–2245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Yamada, K.; Furuya, R.; Takita, T.; Maruyama, Y.; Yamaguchi, Y.; Ohkawa, S.; Kumagai, H. Simplified nutritional screening tools for patients on maintenance hemodialysis. Am. J. Clin. Nutr. 2008, 87, 106–113. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, H.; Ito, Y.; Ishii, H.; Aoyama, T.; Kamoi, D.; Kasuga, H.; Yasuda, K.; Maruyama, S.; Matsuo, S.; Murohara, T.; et al. Geriatric nutritional risk index accurately predicts cardiovascular mortality in incident hemodialysis patients. J. Cardiol. 2014, 64, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Wang, M.; Wang, J.; Yang, K.; Shi, Y.; Zhang, J.; Zhang, B.; Zhang, L.; Zhao, J. Geriatric nutrition risk index is associated with renal progression, cardiovascular events and all-cause mortality in chronic kidney disease. J. Nephrol. 2020, 33, 783–793. [Google Scholar] [CrossRef]
- Lin, Z.-Z.; Wang, J.-J.; Chung, C.-R.; Huang, P.-C.; Su, B.-A.; Cheng, K.-C.; Chio, C.-C.; Chien, C.-C. Epidemiology and mortality of hip fracture among patients on dialysis: Taiwan National Cohort Study. Bone 2014, 64, 235–239. [Google Scholar] [CrossRef]
- Wakasugi, M.; Kazama, J.J.; Kikuchi, K.; Yasuda, K.; Wada, A.; Hamano, T.; Masakane, I.; Narita, I. Hemodialysis Product and Hip Fracture in Hemodialysis Patients: A Nationwide Cohort Study in Japan. Ther. Apher. Dial. 2019, 23, 507–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, M.; Doi, S.; Nakashima, A.; Naito, T.; Masaki, T. N-terminal pro brain natriuretic peptide as a cardiac biomarker in Japanese hemodialysis patients. Int. J. Artif. Organs 2018, 41, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Panichi, V.; Cupisti, A.; Rosati, A.; Di Giorgio, A.; Scatena, A.; Menconi, O.; Bozzoli, L.; Bottai, A. Geriatric nutritional risk index is a strong predictor of mortality in hemodialysis patients: Data from the Riscavid cohort. J. Nephrol. 2014, 27, 193–201. [Google Scholar] [CrossRef]
- Kanis, J.A.; Borgstrom, F.; De Laet, C.; Johansson, H.; Johnell, O.; Jonsson, B.; Oden, A.; Zethraeus, N.; Pfleger, B.; Khaltaev, N. Assessment of fracture risk. Osteoporos. Int. 2005, 16, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Slatopolsky, E.; Brown, A.; Dusso, A. Pathogenesis of secondary hyperparathyroidism. Kidney Int. Suppl. 1999, 56, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruyama, Y.; Taniguchi, M.; Kazama, J.J.; Yokoyama, K.; Hosoya, T.; Yokoo, T.; Shigematsu, T.; Iseki, K.; Tsubakihara, Y. A higher serum alkaline phosphatase is associated with the incidence of hip fracture and mortality among patients receiving hemodialysis in Japan. Nephrol. Dial. Transplant. 2014, 29, 1532–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheeler, D.C.; Winkelmayer, W. CKDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2017, 7, 1–59. [Google Scholar] [CrossRef] [Green Version]
- Jadoul, M.; Albert, J.; Akiba, T.; Akizawa, T.; Arab, L.; Bragg-Gresham, J.; Mason, N.; Prutz, K.-G.; Young, E.; Pisoni, R. Incidence and risk factors for hip or other bone fractures among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2006, 70, 1358–1366. [Google Scholar] [CrossRef] [Green Version]
- Wakasugi, M.; Kazama, J.J.; Wada, A.; Hamano, T.; Masakane, I.; Narita, I. Hip Fracture Trends in Japanese Dialysis Patients, 2008–2013. Am. J. Kidney Dis. 2018, 71, 173–181. [Google Scholar] [CrossRef]
- Iimori, S.; Mori, Y.; Akita, W.; Kuyama, T.; Takada, S.; Asai, T.; Kuwahara, M.; Sasaki, S.; Tsukamoto, Y. Diagnostic usefulness of bone mineral density and biochemical markers of bone turnover in predicting fracture in CKD stage 5D patients--a single-center cohort study. Nephrol. Dial. Transplant. 2012, 27, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gärtner, S.; Kraft, M.; Krüger, J.; Vogt, L.J.; Fiene, M.; Mayerle, J.; Aghdassi, A.A.; Steveling, A.; Völzke, H.; Baumeister, S.E.; et al. Geriatric nutritional risk index correlates with length of hospital stay and inflammatory markers in older inpatients. Clin. Nutr. 2016, 36, 1048–1053. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.-Y.; Hung, S.-C. Geriatric Nutritional Risk Index Is Associated with Unique Health Conditions and Clinical Outcomes in Chronic Kidney Disease Patients. Nutrients 2019, 11, 2769. [Google Scholar] [CrossRef] [Green Version]
- Jamal, S.A.; West, S.L.; Nickolas, T.L. The clinical utility of FRAX to discriminate fracture status in men and women with chronic kidney disease. Osteoporos. Int. 2014, 25, 71–76. [Google Scholar] [CrossRef]
- Yamada, S.; Taniguchi, M.; Tokumoto, M.; Yoshitomi, R.; Yoshida, H.; Tatsumoto, N.; Hirakata, H.; Fujimi, S.; Kitazono, T.; Tsuruya, K. Modified Creatinine Index and the Risk of Bone Fracture in Patients Undergoing Hemodialysis: The Q-Cohort Study. Am. J. Kidney Dis. 2017, 70, 270–280. [Google Scholar] [CrossRef]
- Yamada, S.; Yamamoto, S.; Fukuma, S.; Nakano, T.; Tsuruya, K.; Inaba, M. Geriatric Nutritional Risk Index (GNRI) and Creatinine Index Equally Predict the Risk of Mortality in Hemodialysis Patients: J-DOPPS. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| (A) | |||
| Variables | GNRI | p Value | |
| ≥92 (n = 631) | <92 (n = 202) | ||
| Age, years | 63.4 ± 12.3 | 72.3 ± 11.1 | <0.001 |
| Dialysis vintage, months | 62 (26–124) | 67 (29–133) | 0.556 |
| Diabetes mellitus, n (%) | 251 (40.1) | 76 (37.8) | 0.564 |
| Smokers (ever, current), n (%) | 427 (67.8) | 143 (71.1) | 0.371 |
| Dry weight, kg | 61.7 ± 10.0 | 52.6 ± 9.4 | <0.001 |
| Hemoglobin level, g/dL | 11.0 ± 1.1 | 10.5 ± 1.2 | <0.001 |
| CRP level, mg/L | 0.9 (0.5–2.8) | 2.7 (0.8–7.8) | <0.001 |
| Total cholesterol level, mg/dL | 151.5 ± 30.0 | 144.0 ± 31.8 | <0.001 |
| Cr level, mg/dL | 11.6 ± 2.9 | 9.4 ± 2.6 | <0.001 |
| Ca level, mg/dL | 9.0 ± 0.7 | 8.7 ± 0.8 | <0.001 |
| Pi level, mg/dL | 5.2 ± 1.2 | 4.9 ± 1.4 | <0.001 |
| ALP level, U/L | 217 (171–274) | 242 (187–292) | 0.004 |
| Intact-PTH level, pg/mL | 122 (67–188) | 101 (47–153) | 0.002 |
| Use of statins, n (%) | 110 (17.4) | 26 (12.9) | 0.127 |
| Use of VDRAs, n (%) | 388 (61.5) | 113 (56.0) | 0.161 |
| Use of Pi-binders, n (%) | 560 (82.3) | 146 (72.3) | 0.002 |
| Use of ESAs, n (%) | 560 (88.8) | 191 (90.2) | 0.016 |
| (B) | |||
| Variables | GNRI | p Value | |
| ≥92 (n = 329) | <92 (n = 180) | ||
| Age, years | 64.2 ± 11.3 | 70.8 ± 12.5 | <0.001 |
| Dialysis vintage, months | 96 (33–175) | 71 (31–133) | 0.022 |
| Diabetes mellitus, n (%) | 112 (34.6) | 43 (24.6) | 0.021 |
| Smokers (ever, current), n (%) | 66 (20.1) | 33 (18.4) | 0.647 |
| Dry weight, kg | 51.8 ± 11.0 | 42.9 ± 8.2 | <0.001 |
| Hemoglobin level, g/dL | 10.7 ± 1.1 | 10.7 ± 1.3 | 0.763 |
| CRP level, mg/L | 0.7 (0.5–1.9) | 0.7 (0.5–2.9) | 0.261 |
| Total cholesterol level, mg/dL | 172.0 ± 31.1 | 167.0 ± 36.0 | 0.042 |
| Cr level, mg/dL | 10.2 ± 2.2 | 8.6 ± 2.0 | <0.001 |
| Ca level, mg/dL | 9.2 ± 0.7 | 8.9 ± 0.8 | <0.001 |
| Pi level, mg/dL | 5.4 ± 1.3 | 5.2 ± 1.4 | 0.045 |
| ALP level, U/L | 239 (183–313) | 273 (191–336) | 0.036 |
| Intact-PTH level, pg/mL | 124 (69–195) | 120 (55–180) | 0.106 |
| Use of statins, n (%) | 96 (29.2) | 30 (16.7) | 0.002 |
| Use of VDRAs, n (%) | 199 (60.7) | 116 (64.4) | 0.402 |
| Use of Pi-binders, n (%) | 285 (86.9) | 1313 (74.0) | <0.001 |
| Use of ESAs, n (%) | 301 (91.5) | 165 (91.7) | 0.945 |
| (A) | ||
| Variable | Odds Ratio | p Value |
| Intercept | <0.001 | |
| Age, ≥67 years | 2.02 (1.37–2.98) | <0.001 |
| Dialysis vintage, ≥73 months | 1.87 (1.25–2.82) | 0.003 |
| Diabetes mellitus, presence | 0.69 (0.47–1.03) | 0.070 |
| Smokers | 1.30 (0.87–1.94) | 0.200 |
| Hemoglobin level, ≥10.9 g/dL | 0.58 (0.40–0.83) | 0.003 |
| CRP level, ≥1.0 mg/L | 2.28 (1.56–3.34) | <0.001 |
| Total cholesterol level, ≥156 mg/dL | 0.70 (0.48–1.02) | 0.065 |
| Cr level, ≥10.5 mg/dL | 0.29 (0.19–0.45) | <0.001 |
| Ca level, ≥9.1 mg/dL | 0.59 (0.40–0.88) | 0.010 |
| Pi level, ≥5.2 mg/dL | 0.96 (0.66–1.41) | 0.847 |
| ALP level, ≥230 U/L | 1.32 (0.91–1.92) | 0.144 |
| Intact-PTH level, ≥118 pg/mL | 0.68 (0.46–1.01) | 0.055 |
| Use of statins, presence | 0.81 (0.48–1.37) | 0.438 |
| Use of VDRAs, presence | 0.83 (0.57–1.21) | 0.334 |
| Use of Pi-binders, presence | 0.85 (0.54–1.35) | 0.490 |
| Use of ESAs, presence | 2.14 (1.02–4.45) | 0.044 |
| (B) | ||
| Variables | Odds Ratios | p Value |
| Intercept | <0.001 | |
| Age, ≥67 years | 2.08 (1.32–3.28) | 0.002 |
| Dialysis vintage, ≥73 months | 0.81 (0.51–1.27) | 0.350 |
| Diabetes mellitus, presence | 0.48 (0.30–0.77) | 0.003 |
| Smokers | 0.92 (0.53–1.60) | 0.760 |
| Hemoglobin level, ≥10.9 g/dL | 1.30 (0.85–1.99) | 0.230 |
| CRP level, ≥1.0 mg/L | 1.01 (0.66–1.56) | 0.947 |
| Total cholesterol level, ≥156 mg/dL | 0.65 (0.41–1.00) | 0.050 |
| Cr level, ≥10.5 mg/dL | 0.33 (0.18–0.55) | <0.001 |
| Ca level, ≥9.1 mg/dL | 0.45 (0.29–0.70) | <0.001 |
| Pi level, ≥5.2 mg/dL | 0.88 (0.56–1.36) | 0.557 |
| ALP level, ≥230 U/L | 1.42 (0.91–2.24) | 0.121 |
| Intact-PTH level, ≥118 pg/mL | 0.83 (0.53–1.30) | 0.428 |
| Use of statins, presence | 0.37 (0.21–0.65) | <0.001 |
| Use of VDRAs, presence | 1.75 (1.10–2.78) | 0.017 |
| Use of Pi-binders, presence | 0.61 (0.35–1.05) | 0.073 |
| Use of ESAs, presence | 0.39 (0.18–0.85) | 0.018 |
| (A) | ||
| Univariate | HR (95% CI) | p Value |
| GNRI, <92 | 3.51 (1.91–6.42) | <0.001 |
| Covariate | HR (95% CI) | p Value |
| Age, ≥67 years | 1.99 (1.04–3.81) | 0.038 |
| Dialysis vintage, ≥73 months | 0.77 (0.39–1.50) | 0.439 |
| Smokers (ever, current), presence | 0.79 (0.43–1.48) | 0.470 |
| CRP level, ≥1.0 mg/L | 0.93 (0.50–1.72) | 0.815 |
| Ca level, ≥9.1 mg/dL | 0.82 (0.42–1.65) | 0.584 |
| Pi level, ≥5.2 mg/dL | 1.36 (0.73–2.55) | 0.337 |
| ALP level, ≥230 U/L | 1.54 (0.82–2.89) | 0.179 |
| Intact-PTH level, ≥118 pg/mL | 0.72 (0.37–1.38) | 0.323 |
| Use of VDRAs, presence | 1.32 (0.70–2.51) | 0.390 |
| Use of Pi-binders, presence | 0.62 (0.31–1.25) | 0.181 |
| GNRI, <92 | 2.94 (1.54–5.59) | 0.001 |
| (B) | ||
| Univariate | HR (95% CI) | p Value |
| GNRI, <92 | 2.47 (1.52–4.03) | <0.001 |
| Covariate | HR (95% CI) | p Value |
| Age, ≥67 years | 1.76 (1.02–3.04) | 0.042 |
| Dialysis vintage, ≥73 months | 0.93 (0.55–1.55) | 0.775 |
| Smokers (ever, current), presence | 0.65 (0.32–1.36) | 0.255 |
| CRP level, ≥1.0 mg/L | 1.03 (0.61–1.72) | 0.917 |
| Ca level, ≥9.1 mg/dL | 0.97 (0.56–1.66) | 0.908 |
| Pi level, ≥5.2 mg/dL | 1.36 (0.80–2.30) | 0.254 |
| ALP level, ≥230 U/L | 0.98 (0.57–1.67) | 0.943 |
| Intact-PTH level, ≥118 pg/mL | 0.88 (0.52–1.47) | 0.616 |
| Use of VDRAs, presence | 1.12 (0.66–1.90) | 0.666 |
| Use of Pi-binders, presence | 0.58 (0.32–1.05) | 0.072 |
| GNRI, <92 | 2.05 (1.20–3.51) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, M.; Nakashima, A.; Doi, S.; Maeda, K.; Ishiuchi, N.; Naito, T.; Masaki, T. Lower Geriatric Nutritional Risk Index (GNRI) Is Associated with Higher Risk of Fractures in Patients Undergoing Hemodialysis. Nutrients 2021, 13, 2847. https://doi.org/10.3390/nu13082847
Yoshida M, Nakashima A, Doi S, Maeda K, Ishiuchi N, Naito T, Masaki T. Lower Geriatric Nutritional Risk Index (GNRI) Is Associated with Higher Risk of Fractures in Patients Undergoing Hemodialysis. Nutrients. 2021; 13(8):2847. https://doi.org/10.3390/nu13082847
Chicago/Turabian StyleYoshida, Maria, Ayumu Nakashima, Shigehiro Doi, Kazuya Maeda, Naoki Ishiuchi, Takayuki Naito, and Takao Masaki. 2021. "Lower Geriatric Nutritional Risk Index (GNRI) Is Associated with Higher Risk of Fractures in Patients Undergoing Hemodialysis" Nutrients 13, no. 8: 2847. https://doi.org/10.3390/nu13082847