
Intake of Vitamin E and C in Women of Reproductive Age: Results from the Latin American Study of Nutrition and Health (ELANS)

 , , , , , ,
, , , , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Anthropometric Measurements
2.3. Sociodemographic and Lifestyle Population Variables
2.4. Dietary Assessment
2.5. Estimation of Vitamin E and C Intake and Inadequacy
2.6. Food Sources
2.7. Statistical Analyses
2.8. Ethics
3. Results
3.1. Participant’s Characteristics
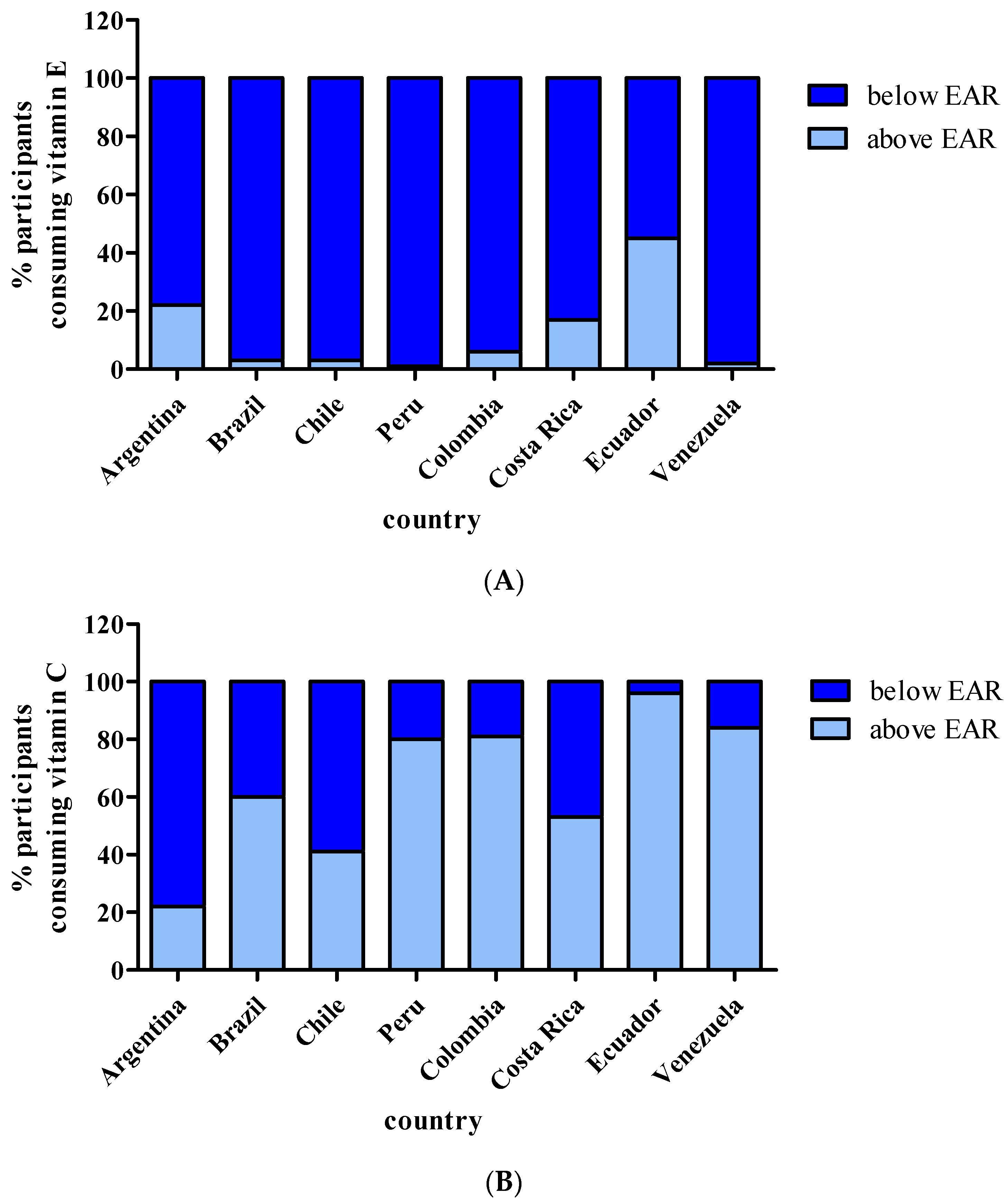
3.2. Vitamin E Daily Intake and Assessment of Adequacy
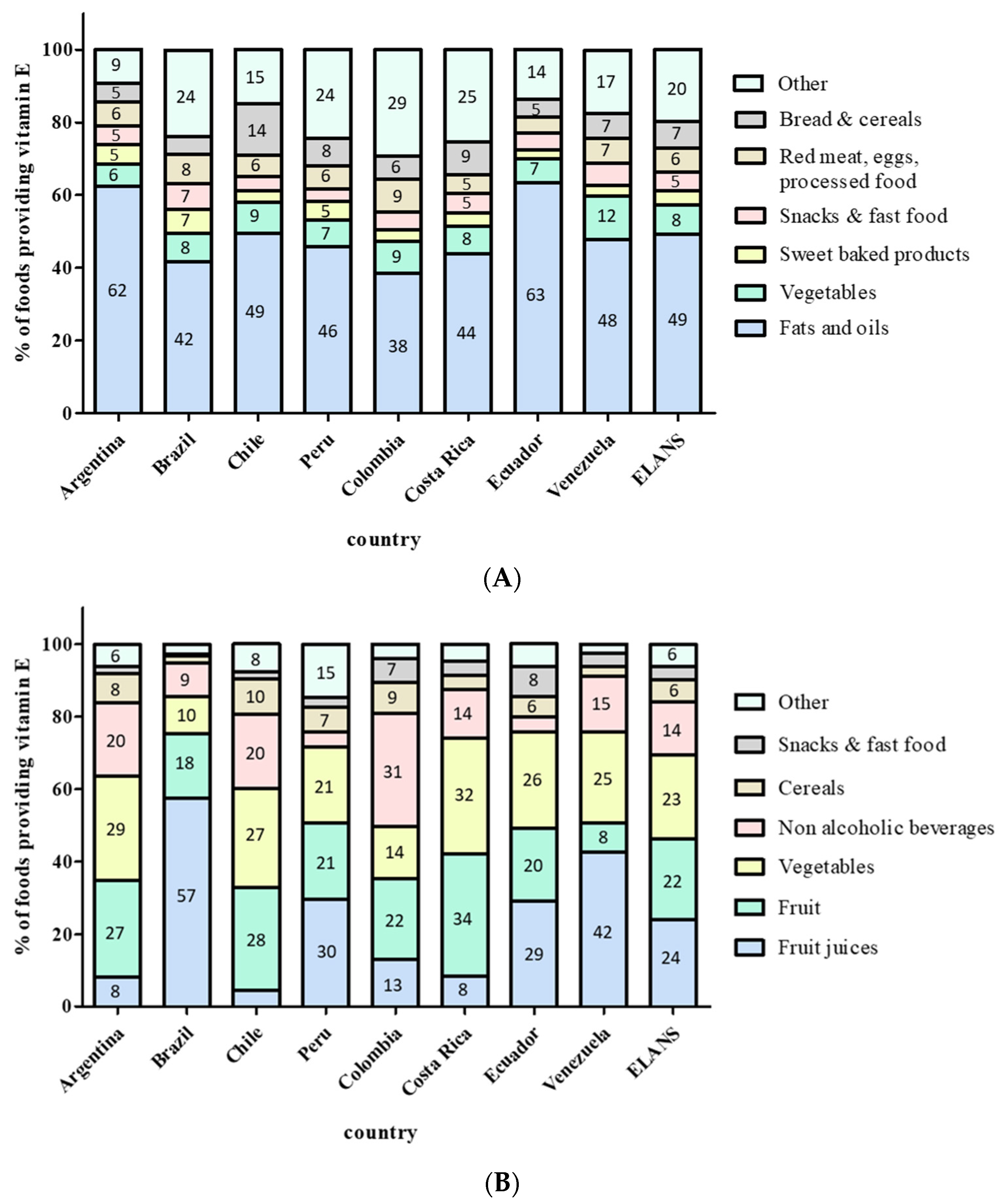
3.3. Vitamin E Food Sources
3.4. Vitamin C Daily Intake and Assessment of Adequacy
3.5. Vitamin C Food Sources
3.6. Combined Vitamin E and Vitamin C Inadequacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evans, H.M.; Bishop, K.S. On the Existence of a Hitherto Unrecognized Dietary Factor Essential for Reproduction. Science 1922, 56, 650–651. [Google Scholar] [CrossRef] [Green Version]
- Sure, B. Dietary requirements for reproduction. 2.—The existence of a specific vitamin for reproduction. J. Biol. Chem. 1924, 58, 693. [Google Scholar] [CrossRef]
- Mattill, H.A. The effectiveness of the X-substance in preventing sterility in rats on milk rations high in fat. J. Biol. Chem. 1924, 44, 137. [Google Scholar] [CrossRef]
- Niki, E.; Traber, M.G. A history of vitamin E. Ann. Nutr. Metab. 2012, 61, 207–212. [Google Scholar] [CrossRef]
- Rigotti, A. Absorption, transport, and tissue delivery of vitamin E. Mol. Asp. Med. 2007, 28, 423–436. [Google Scholar] [CrossRef] [PubMed]
- Brigelius-Flohe, R. Vitamin E: The shrew waiting to be tamed. Free. Radic. Biol. Med. 2009, 46, 543–554. [Google Scholar] [CrossRef]
- Zingg, J.M.; Azzi, A. Non-antioxidant activities of vitamin E. Curr. Med. Chem. 2004, 11, 1113–1133. [Google Scholar] [CrossRef]
- Zingg, J.M. Vitamin E: A Role in Signal Transduction. Annu. Rev. Nutr. 2015, 35, 135–173. [Google Scholar] [CrossRef]
- US Institute of Medicine. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; The National Academies Press: Washington, DC, USA, 2000; p. 528. [Google Scholar] [CrossRef]
- Bruno, R.S.; Ramakrishnan, R.; Montine, T.J.; Bray, T.M.; Traber, M.G. Alpha-Tocopherol disappearance is faster in cigarette smokers and is inversely related to their ascorbic acid status. Am. J. Clin. Nutr. 2005, 81, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. Antioxidants Related, Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press (U.S.) by the National Academy of Sciences: Washington, DC, USA, 2000. [Google Scholar] [CrossRef]
- Péter, S.; Friedel, A.; Roos, F.F.; Wyss, A.; Eggersdorfer, M.; Hoffmann, K.; Weber, P. A Systematic Review of Global Alpha-Tocopherol Status as Assessed by Nutritional Intake Levels and Blood Serum Concentrations. Int. J. Vitam. Nutr. Res. Int. Z. Vitam. Ernahr. J. Int. Vitaminol. Nutr. 2015, 85, 261–281. [Google Scholar] [CrossRef]
- Maras, J.E.; Bermudez, O.I.; Qiao, N.; Bakun, P.J.; Boody-Alter, E.L.; Tucker, K.L. Intake of alpha-tocopherol is limited among US adults. J. Am. Diet. Assoc. 2004, 104, 567–575. [Google Scholar] [CrossRef]
- Olza, J.; Aranceta-Bartrina, J.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported Dietary Intake and Food Sources of Zinc, Selenium, and Vitamins A, E and C in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 697. [Google Scholar] [CrossRef]
- Brauchla, M.; Dekker, M.J.; Rehm, C.D. Trends in Vitamin C Consumption in the United States: 1999–2018. Nutrients 2021, 13, 420. [Google Scholar] [CrossRef] [PubMed]
- Dror, D.K.; Allen, L.H. Vitamin E deficiency in developing countries. Food Nutr. Bull. 2011, 32, 124–143. [Google Scholar] [CrossRef] [PubMed]
- Traber, M.G. Vitamin E inadequacy in humans: Causes and consequences. Adv. Nutr. 2014, 5, 503–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Violet, P.C.; Ebenuwa, I.C.; Wang, Y.; Niyyati, M.; Padayatty, S.J.; Head, B.; Wilkins, K.; Chung, S.; Thakur, V.; Ulatowski, L.; et al. Vitamin E sequestration by liver fat in humans. JCI Insight 2020, 5. [Google Scholar] [CrossRef]
- Traber, M.G.; Mah, E.; Leonard, S.W.; Bobe, G.; Bruno, R.S. Metabolic syndrome increases dietary α-tocopherol requirements as assessed using urinary and plasma vitamin E catabolites: A double-blind, crossover clinical trial. Am. J. Clin. Nutr. 2017, 105, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Sanyal, A.J.; Chalasani, N.; Kowdley, K.V.; McCullough, A.; Diehl, A.M.; Bass, N.M.; Neuschwander-Tetri, B.A.; Lavine, J.E.; Tonascia, J.; Unalp, A.; et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. New Engl. J. Med. 2010, 362, 1675–1685. [Google Scholar] [CrossRef] [Green Version]
- Miller, G.W.; Ulatowski, L.; Labut, E.M.; Lebold, K.M.; Manor, D.; Atkinson, J.; Barton, C.L.; Tanguay, R.L.; Traber, M.G. The alpha-tocopherol transfer protein is essential for vertebrate embryogenesis. PLoS ONE 2012, 7, e47402. [Google Scholar] [CrossRef]
- Kaempf-Rotzoll, D.E.; Horiguchi, M.; Hashiguchi, K.; Aoki, J.; Tamai, H.; Linderkamp, O.; Arai, H. Human placental trophoblast cells express alpha-tocopherol transfer protein. Placenta 2003, 24, 439–444. [Google Scholar] [CrossRef]
- Kaempf-Rotzoll, D.E.; Igarashi, K.; Aoki, J.; Jishage, K.; Suzuki, H.; Tamai, H.; Linderkamp, O.; Arai, H. Alpha-tocopherol transfer protein is specifically localized at the implantation site of pregnant mouse uterus. Biol. Reprod. 2002, 67, 599–604. [Google Scholar] [CrossRef] [Green Version]
- Jauniaux, E.; Cindrova-Davies, T.; Johns, J.; Dunster, C.; Hempstock, J.; Kelly, F.J.; Burton, G.J. Distribution and transfer pathways of antioxidant molecules inside the first trimester human gestational sac. J. Clin. Endocrinol. Metab. 2004, 89, 1452–1458. [Google Scholar] [CrossRef] [PubMed]
- Jishage, K.; Arita, M.; Igarashi, K.; Iwata, T.; Watanabe, M.; Ogawa, M.; Ueda, O.; Kamada, N.; Inoue, K.; Arai, H.; et al. Alpha-tocopherol transfer protein is important for the normal development of placental labyrinthine trophoblasts in mice. J. Biol. Chem. 2001, 276, 1669–1672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rengaraj, D.; Hong, Y.H. Effects of dietary vitamin E on fertility functions in poultry species. Int. J. Mol. Sci. 2015, 16, 9910–9921. [Google Scholar] [CrossRef] [Green Version]
- McDougall, M.; Choi, J.; Truong, L.; Tanguay, R.; Traber, M.G. Vitamin E deficiency during embryogenesis in zebrafish causes lasting metabolic and cognitive impairments despite refeeding adequate diets. Free. Radic. Biol. Med. 2017, 110, 250–260. [Google Scholar] [CrossRef]
- Santander, N.; Lizama, C.; Parga, M.J.; Quiroz, A.; Pérez, D.; Echeverría, G.; Ulloa, L.; Palma, V.; Rigotti, A.; Busso, D. Deficient Vitamin E Uptake During Development Impairs Neural Tube Closure in Mice Lacking Lipoprotein Receptor SR-BI. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Shamim, A.A.; Schulze, K.; Merrill, R.D.; Kabir, A.; Christian, P.; Shaikh, S.; Wu, L.; Ali, H.; Labrique, A.B.; Mehra, S.; et al. First-trimester plasma tocopherols are associated with risk of miscarriage in rural Bangladesh. Am. J. Clin. Nutr. 2015, 101, 294–301. [Google Scholar] [CrossRef] [Green Version]
- Simşek, M.; Naziroğlu, M.; Simşek, H.; Cay, M.; Aksakal, M.; Kumru, S. Blood plasma levels of lipoperoxides, glutathione peroxidase, beta carotene, vitamin A and E in women with habitual abortion. Cell Biochem. Funct. 1998, 16, 227–231. [Google Scholar] [CrossRef]
- Fares, S.; Sethom, M.M.; Khouaja-Mokrani, C.; Jabnoun, S.; Feki, M.; Kaabachi, N. VitaminA, E, and D deficiencies in tunisian very low birth weight neonates: Prevalence and risk factors. Pediatrics Neonatol. 2014, 55, 196–201. [Google Scholar] [CrossRef] [Green Version]
- Kositamongkol, S.; Suthutvoravut, U.; Chongviriyaphan, N.; Feungpean, B.; Nuntnarumit, P. Vitamin A and E status in very low birth weight infants. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2011, 31, 471–476. [Google Scholar] [CrossRef]
- Bastani, P.; Hamdi, K.; Abasalizadeh, F.; Navali, N. Effects of vitamin E supplementation on some pregnancy health indices: A randomized clinical trial. Int. J. Gen. Med. 2011, 4, 461–464. [Google Scholar] [CrossRef] [Green Version]
- Hauth, J.C.; Clifton, R.G.; Roberts, J.M.; Spong, C.Y.; Myatt, L.; Leveno, K.J.; Pearson, G.D.; Varner, M.W.; Thorp, J.M., Jr.; Mercer, B.M.; et al. Vitamin C and E supplementation to prevent spontaneous preterm birth: A randomized controlled trial. Obstet. Gynecol. 2010, 116, 653–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rumbold, A.; Ota, E.; Hori, H.; Miyazaki, C.; Crowther, C.A. Vitamin E supplementation in pregnancy. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies. Scientific Opinion on Dietary Reference Values for vitamin E as α-tocopherol. EFSA J. 2015, 13, 4149. [Google Scholar] [CrossRef]
- Medicine, I.O. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; The National Academies Press: Washington, DC, USA, 2006; p. 1344. [Google Scholar] [CrossRef]
- Alvarez, J.J.; Montelongo, A.; Iglesias, A.; Lasunción, M.A.; Herrera, E. Longitudinal study on lipoprotein profile, high density lipoprotein subclass, and postheparin lipases during gestation in women. J. Lipid Res. 1996, 37, 299–308. [Google Scholar] [CrossRef]
- Herrera, E.; Ortega, H.; Alvino, G.; Giovannini, N.; Amusquivar, E.; Cetin, I. Relationship between plasma fatty acid profile and antioxidant vitamins during normal pregnancy. Eur. J. Clin. Nutr. 2004, 58, 1231–1238. [Google Scholar] [CrossRef]
- Bailey, R.L.; Pac, S.G.; Fulgoni, V.L., III; Reidy, K.C.; Catalano, P.M. Estimation of Total Usual Dietary Intakes of Pregnant Women in the United States. JAMA Netw. Open 2019, 2, e195967. [Google Scholar] [CrossRef] [Green Version]
- Fisberg, M.; Kovalskys, I.; Gómez, G.; Rigotti, A.; Cortés, L.Y.; Herrera-Cuenca, M.; Yépez, M.C.; Pareja, R.G.; Guajardo, V.; Zimberg, I.Z.; et al. Latin American Study of Nutrition and Health (ELANS): Rationale and study design. BMC Public Health 2016, 16, 93. [Google Scholar] [CrossRef]
- Committee, W.E. WHO Expert Committee on Physical Status: The Use and Interpretation of Anthropometry; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Herrera-Cuenca, M.; Previdelli, A.N.; Koletzko, B.; Hernandez, P.; Landaeta-Jimenez, M.; Sifontes, Y.; Gómez, G.; Kovalskys, I.; García, M.C.Y.; Pareja, R.; et al. Childbearing Age Women Characteristics in Latin America. Building Evidence Bases for Early Prevention. Results from the ELANS Study. Nutrients 2020, 13, 45. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef]
- Kovalskys, I.; Fisberg, M.; Gómez, G.; Rigotti, A.; Cortés, L.Y.; Yépez, M.C.; Pareja, R.G.; Herrera-Cuenca, M.; Zimberg, I.Z.; Tucker, K.L.; et al. Standardization of the Food Composition Database Used in the Latin American Nutrition and Health Study (ELANS). Nutrients 2015, 7, 7914–7924. [Google Scholar] [CrossRef] [Green Version]
- Kovalskys, I.; Fisberg, M.; Gómez, G.; Pareja, R.G.; Yépez García, M.C.; Cortés Sanabria, L.Y.; Herrera-Cuenca, M.; Rigotti, A.; Guajardo, V.; Zalcman Zimberg, I.; et al. Energy intake and food sources of eight Latin American countries: Results from the Latin American Study of Nutrition and Health (ELANS). Public Health Nutr. 2018, 21, 2535–2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lean, S.C.; Derricott, H.; Jones, R.L.; Heazell, A.E.P. Advanced maternal age and adverse pregnancy outcomes: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186287. [Google Scholar] [CrossRef] [Green Version]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalán, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and maternal obesity: Epidemiology and health consequences. Lancet Diabetes Endocrinol. 2016, 4, 1025–1036. [Google Scholar] [CrossRef]
- Lewandowska, M.; Sajdak, S.; Więckowska, B.; Manevska, N.; Lubiński, J. The Influence of Maternal BMI on Adverse Pregnancy Outcomes in Older Women. Nutrients 2020, 12, 2838. [Google Scholar] [CrossRef] [PubMed]
- Previdelli, A.N.; Gómez, G.; Kovalskys, I.; Fisberg, M.; Cortés, L.Y.; Pareja, R.G.; Liria, M.R.; García, M.C.Y.; Herrera-Cuenca, M.; Rigotti, A.; et al. Prevalence and determinants of misreporting of energy intake among Latin American populations: Results from ELANS study. Nutr. Res. 2019, 68, 9–18. [Google Scholar] [CrossRef]
- US Department of Agriculture and US Department of Health and Human Services. Dietary Guidelines for Americans 2020–2025, 9th ed.; December 2020. Available online: DietaryGuidelines.gov (accessed on 1 May 2021).
- Clark, J.; Holgan, N.; Craig, L.; Morgan, H.; Danielian, P.; Devereux, G. Development and piloting of a food-based intervention to increase vitamin E intake in pregnant women in a randomized controlled trial. Food Sci. Nutr. 2016, 4, 848–851. [Google Scholar] [CrossRef] [Green Version]
- Clark, J.; Craig, L.; McNeill, G.; Smith, N.; Norrie, J.; Devereux, G. A novel dietary intervention to optimize vitamin E intake of pregnant women to 15 mg/day. J. Acad. Nutr. Diet. 2012, 112, 297–301. [Google Scholar] [CrossRef]
- Busso, D.; Echeverría, G.; Passi-Solar, A.; Morales, F.; Farías, M.; Margozzini, P. Folate status in women of childbearing age in the Urban Metropolitan Region of Chile: Results from the National Health Survey 2016–2017. Public Health Nutr. 2021, 24, 385–392. [Google Scholar] [CrossRef]
- Gómez, G.; Nogueira Previdelli, Á.; Fisberg, R.M.; Kovalskys, I.; Fisberg, M.; Herrera-Cuenca, M.; Cortés Sanabria, L.Y.; Yépez García, M.C.; Rigotti, A.; Liria-Domínguez, M.R.; et al. Dietary Diversity and Micronutrients Adequacy in Women of Childbearing Age: Results from ELANS Study. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization of the United Nations. Minimum Dietary Diversity for Women—A Guide to Measurement; University of California: Davis, CA, USA, 2016. [Google Scholar]
- Dubuisson, C.; Lioret, S.; Touvier, M.; Dufour, A.; Calamassi-Tran, G.; Volatier, J.L.; Lafay, L. Trends in food and nutritional intakes of French adults from 1999 to 2007: Results from the INCA surveys. Br. J. Nutr. 2010, 103, 1035–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schleicher, R.L.; Carroll, M.D.; Ford, E.S.; Lacher, D.A. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003–2004 National Health and Nutrition Examination Survey (NHANES). Am. J. Clin. Nutr. 2009, 90, 1252–1263. [Google Scholar] [CrossRef] [PubMed]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2019. Safeguarding against economic slowdowns and downturns. In Building Climate Resilience for Food Security and Nutrition; UNICEF: Rome, Italy, 2019. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Number (n) | Frequency (%) |
|---|---|---|
| Country | ||
| Argentina | 521 | 14.1 |
| Brazil | 798 | 21.5 |
| Chile | 345 | 9.3 |
| Perú | 480 | 13.0 |
| Colombia | 464 | 12.5 |
| Costa Rica | 309 | 8.3 |
| Ecuador | 324 | 8.7 |
| Venezuela | 463 | 12.5 |
| Age (years old) | ||
| 15 to 19 | 539 | 14.6 |
| 20 to 34 | 1771 | 47.8 |
| 35 to 49 | 1394 | 37.6 |
| Socioeconomic level (SEL) | ||
| High | 529 | 14.3 |
| Medium | 1593 | 43.0 |
| Low | 1582 | 42.7 |
| Nutritional status | ||
| Underweight | 128 | 3.5 |
| Normal weight | 1444 | 39.0 |
| Overweight | 1177 | 31.8 |
| Obesity | 953 | 25.7 |
| Vitamin E (mg/day) | Vitamin C (mg/day) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD. | p | Percentiles | Mean ± SD. | p | Percentiles | ||||||
| 10th | 50th | 90th | 10th | 50th | 90th | ||||||
| ELANS total sample | 7.9 ± 3.2 | - | 4.6 | 7.3 | 12.1 | 94.4 ± 90.3 | - | 31.2 | 72.9 | 167.5 | |
| Country | Argentina | 9.9 ± 2.9 a | <0.001 | 6.3 | 9.7 | 14.0 | 46.6 ± 23.2 a | <0.001 | 24.5 | 41.5 | 73.9 |
| Brazil | 6.2 ± 2.3 b | 3.6 | 5.8 | 9.2 | 120.8 ± 163.3 b | 24.6 | 72.9 | 252.3 | |||
| Chile | 6.9 ± 2.4 c | 4.4 | 6.5 | 9.6 | 60.5 ± 33.7 a,c | 26.2 | 51.4 | 105.1 | |||
| Perú | 6.9 ± 1.9 c | 4.8 | 6.6 | 9.2 | 98.8 ± 57.6 d | 46.8 | 89.0 | 159.1 | |||
| Colombia | 7.9 ± 2.6 d | 5.1 | 7.7 | 11.0 | 100.7 ± 48.2 d | 48.5 | 94.0 | 163.6 | |||
| Costa Rica | 9.0 ± 2.7 e | 5.8 | 8.6 | 12.8 | 71.9 ± 45.4 c | 28.2 | 61.2 | 126.4 | |||
| Ecuador | 12.1 ± 4.2 f | 7.2 | 11.5 | 17.6 | 127.1 ± 53.9 b | 69.3 | 118.5 | 190.1 | |||
| Venezuela | 6.9 ± 2.2 c | 4.3 | 6.7 | 9.6 | 109.6 ± 51.7 b,d | 47.7 | 103.2 | 180.7 | |||
| Age (years old) | 15 to 19 | 8.4 ± 3.3 a | <0.001 | 4.9 | 7.7 | 12.9 | 91.2 ± 70.8 | 0.645 | 30.2 | 71.5 | 170.0 |
| 20 to 34 | 8.0 ± 3.2 b | 4.6 | 7.4 | 12.0 | 95.4 ± 92.8 | 31.8 | 77.1 | 166.1 | |||
| 35 to 49 | 7.6 ± 3.1 c | 4.4 | 7.1 | 11.9 | 94.5 ± 93.7 | 30.9 | 72.6 | 168.2 | |||
| SEL | High | 7.4 ± 3.1 a | <0.001 | 4.3 | 6.9 | 11.5 | 114.1 ± 93.9 a | <0.001 | 34.8 | 90.5 | 204.2 |
| Medium | 8.2 ± 3.4 b | 4.6 | 7.7 | 12.7 | 96.6 ± 110 b | 29.3 | 72.8 | 168.9 | |||
| Low | 7.8 ± 2.9 a | 4.5 | 7.2 | 11.7 | 85.7 ± 61.1 c | 31.8 | 72.5 | 152.1 | |||
| Nutritional status | Underweight | 8.7 ± 3.3 | 0.004 | 5.2 | 8.0 | 13.4 | 90.7 ± 64.9 | 0.935 | 31.1 | 70.9 | 174.7 |
| Normal weight | 8.0 ± 3.1 | 4.6 | 7.5 | 12.2 | 94.2 ± 82.3 | 30.9 | 74.7 | 170.9 | |||
| Overweight | 7.8 ± 3.2 | 4.5 | 7.2 | 12.0 | 95.5 ± 84.8 | 32.6 | 79.6 | 163.2 | |||
| Obese | 7.8 ± 3.1 | 4.4 | 7.2 | 11.9 | 94.0 ± 109.5 | 30.1 | 70.2 | 162.9 | |||
| Vitamin E | Vitamin C | |||||||
|---|---|---|---|---|---|---|---|---|
| % of EAR | Below 100% | % of EAR | Below 100% | |||||
| Mean ± SD | p | Mean ± SD | p | |||||
| ELANS total sample | 3704 | 66.0 ± 26.4 | 89.6% | 158.6 ± 151.2 | 36.3% | |||
| Country | Argentina | 521 | 82.3 ± 24.5 a | <0.001 | 77.9% | 78.1 ± 38.7 a | <0.001 | 78.1% |
| Brazil | 798 | 51.7 ± 19.3 b | 97.5% | 202.4 ± 272.8 b | 40.1% | |||
| Chile | 345 | 57.3 ± 19.7 c | 97.1% | 101.8 ± 57.1 a,d | 58.8% | |||
| Perú | 480 | 57.7 ± 15.4 c | 98.8% | 166.3 ± 98.1 c | 20.2% | |||
| Colombia | 464 | 65.8 ± 21.5 d | 94.4% | 169.1 ± 81 c | 18.5% | |||
| Costa Rica | 309 | 74.9 ± 22.5 e | 82.8% | 120.7 ± 76 d | 46.9% | |||
| Ecuador | 324 | 100.5 ± 34.9 f | 55.2% | 213.8 ± 90.6 b | 4.0% | |||
| Venezuela | 463 | 57.2 ± 18.5 c | 97.6% | 184.4 ± 87.3 b,c | 16.0% | |||
| Age (years old) | 15 to 19 | 539 | 69.9 ± 27.5 a | <0.001 | 86.1% | 160.4 ± 124.7 | 0.921 | 36.0% |
| 20 to 34 | 1771 | 66.5 ± 26.5 b | 90.0% | 159.0 ± 154.6 | 35.2% | |||
| 35 to 49 | 1394 | 63.7 ± 25.7 c | 90.4% | 157.5 ± 156.2 | 37.8% | |||
| SEL | High | 529 | 61.7 ± 26.1 a | <0.001 | 92.6% | 191.4 ± 157.4 a | <0.001 | 27.8% |
| Medium | 1593 | 68.5 ± 28 b | 87.1% | 162.3 ± 184.2 b | 38.0% | |||
| Low | 1582 | 64.8 ± 24.5 a | 91.1% | 144.0 ± 102.5 c | 37.5% | |||
| Nutritional status | Underweight | 128 | 72.7 ± 27.4 a | 0.004 | 83.6% | 154.4 ± 110.7 | 0.960 | 39.8% |
| Normal weight | 1444 | 66.9 ± 26.1 ab | 89.3% | 158.9 ± 138.6 | 37.1% | |||
| Overweight | 1177 | 64.8 ± 26.8 b | 90.0% | 160.0 ± 141.7 | 31.0% | |||
| Obese | 953 | 65.1 ± 26.2 b | 90.2% | 157.1 ± 182.7 | 41.2% | |||
| Inadequacy of Vitamin E EAR | Adequacy of Vitamin E EAR | |||
|---|---|---|---|---|
| Country | Inadequacy of Vitamin C EAR | Adequacy of Vitamin C EAR | Inadequacy of Vitamin C EAR | Adequacy of Vitamin C EAR |
| Argentina | 63.1% | 14.8% | 15.0% | 7.1% |
| Brazil | 40.1% | 57.4% | 0.0% | 2.5% |
| Chile | 57.7% | 39.4% | 1.2% | 1.7% |
| Perú | 20.2% | 78.5% | 0.0% | 1.3% |
| Colombia | 18.3% | 76.1% | 0.2% | 5.4% |
| Costa Rica | 42.4% | 40.5% | 4.5% | 12.6% |
| Ecuador | 3.7% | 51.5% | 0.3% | 44.4% |
| Venezuela | 16.0% | 81.6% | 0.0% | 2.4% |
| ELANS total sample | 33.7% | 55.9% | 2.6% | 7.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busso, D.; David, A.; Penailillo, R.; Echeverría, G.; Rigotti, A.; Kovalskys, I.; Gómez, G.; Cortés Sanabria, L.Y.; Yépez García, M.C.; Pareja, R.G.; et al. Intake of Vitamin E and C in Women of Reproductive Age: Results from the Latin American Study of Nutrition and Health (ELANS). Nutrients 2021, 13, 1954. https://doi.org/10.3390/nu13061954
Busso D, David A, Penailillo R, Echeverría G, Rigotti A, Kovalskys I, Gómez G, Cortés Sanabria LY, Yépez García MC, Pareja RG, et al. Intake of Vitamin E and C in Women of Reproductive Age: Results from the Latin American Study of Nutrition and Health (ELANS). Nutrients. 2021; 13(6):1954. https://doi.org/10.3390/nu13061954
Chicago/Turabian StyleBusso, Dolores, Andrea David, Reyna Penailillo, Guadalupe Echeverría, Attilio Rigotti, Irina Kovalskys, Georgina Gómez, Lilia Yadira Cortés Sanabria, Martha Cecilia Yépez García, Rossina G. Pareja, and et al. 2021. "Intake of Vitamin E and C in Women of Reproductive Age: Results from the Latin American Study of Nutrition and Health (ELANS)" Nutrients 13, no. 6: 1954. https://doi.org/10.3390/nu13061954