
Early Nutrition during Hospitalization in Relation to Bone Health in Preterm Infants at Term Age and Six Months Corrected Age


Abstract
:
1. Introduction
2. Methods
2.1. Study Population
2.2. Study Procedures
2.3. Nutrition
2.4. DXA
2.5. Potential Confounders
- Necrotizing enterocolitis: according to the modified Bell’s staging criteria; definite: necrotizing enterocolitis (NEC) from stage IIA onwards [32].
- Bronchopulmonary dysplasia: lung injury from oxygen therapy and mechanical ventilation; 28 days of oxygen administration [33].
- Late onset sepsis: neonatal sepsis occurring after 3 days of age [34].
2.6. Statistical Analysis
3. Results
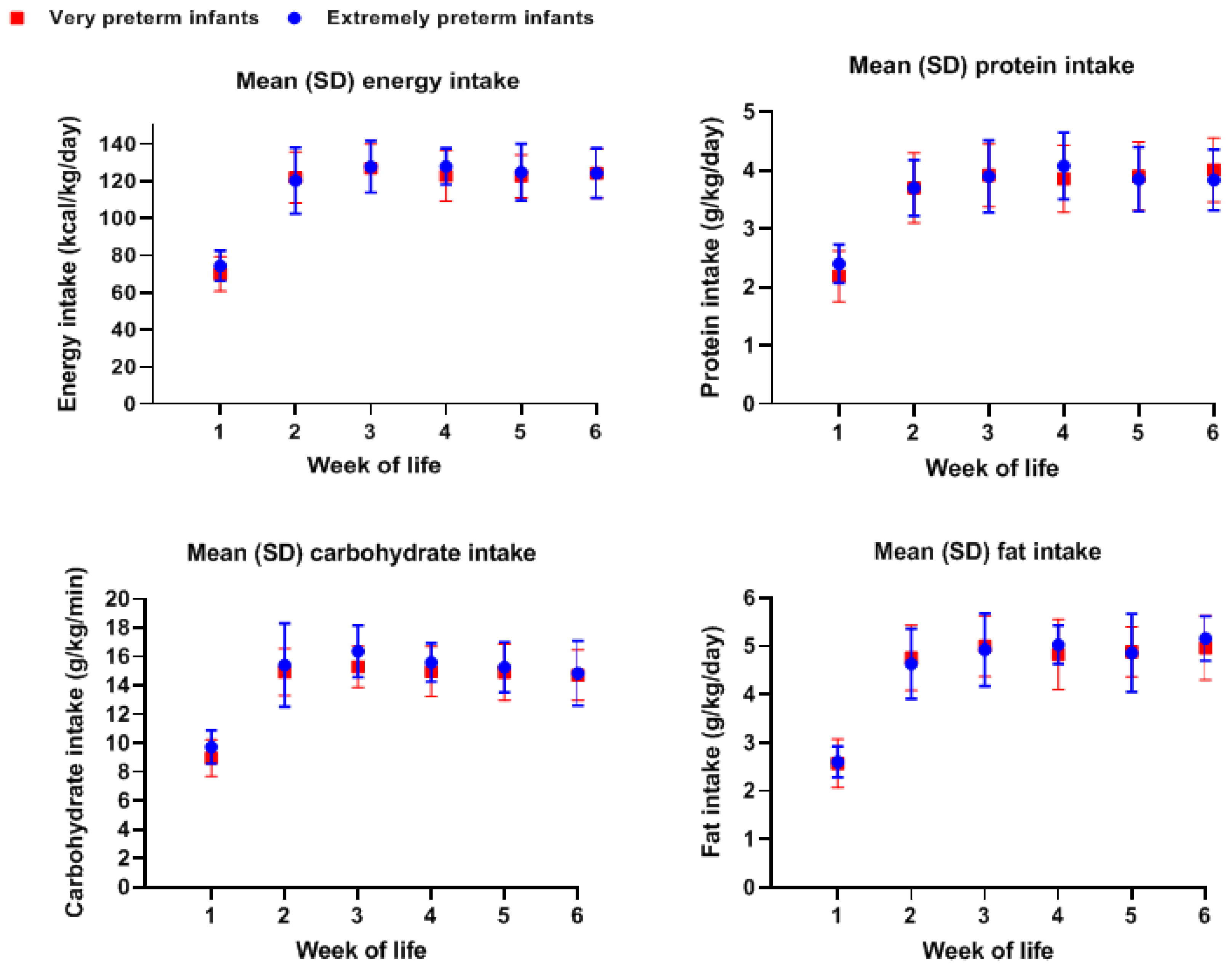
3.1. Nutrient Intake in the First Weeks of Life
3.2. BMD and BMC in Extremely and Very Preterm Infants
3.3. Macronutrient Intake in the First Postnatal Weeks and BMC at TCA
3.4. Macronutrient Intake in the First Postnatal Weeks and BMD at TCA
3.5. Macronutrient Intake in the First Postnatal Weeks and BMC at Six Months CA
3.6. Macronutrient Intake in the First Postnatal Weeks and BMD at Six Months CA
4. Discussion
4.1. BMC and BMD in Preterm Infants
4.2. Nutrient Intake in the First Postnatal Weeks on BMC and BMD in Preterm Infants Weeks
4.3. Sepsis in Early Life and Bone Health
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMC | Bone Mineral Content |
| BMD | Bone Mineral Density |
| BPD | Bronchopulmonary Dysplasia |
| CA | Corrected Age |
| DXA | Dual-Energy X-Ray Absorptiometry |
| GA | Gestational Age |
| LOS | Late Onset Sepsis |
| NEC | Necrotizing Enterocolitis |
| PMA | Postmenstrual Age |
| SDS | Standard Deviation Scores |
| TCA | Term Corrected Age |
References
- Chacham, S.; Pasi, R.; Chegondi, M.; Ahmad, N.; Mohanty, S.B. Metabolic Bone Disease in Premature Neonates: An Unmet Challenge. J. Clin. Res. Pediatr. Endocrinol. 2020, 12, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Javaid, M.K.; Taylor, P.; Walker-Bone, K.; Dennison, E.; Arden, N. The fetal origins of osteoporotic fracture. Calcif. Tissue Int. 2002, 70, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Koo, W.W.; Sherman, R.; Succop, P.; Oestreich, A.E.; Tsang, R.C.; Krug-Wispe, S.K.; Steichen, J.J. Sequential bone mineral content in small preterm infants with and without fractures and rickets. J. Bone Miner. Res. 1988, 3, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Ramot, R.; Kachhawa, G.; Kulshreshtha, V.; Varshney, S.; Sankar, M.J.; Devasenathipathy, K.; Sreenivas, V.; Khadgawat, R. Bone Mass in Newborns Assessed by DXA—A Systematic Review and Meta-analysis. Indian J. Endocrinol. Metab. 2019, 23, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, M.S. Does early nutrition program later bone health in preterm infants? Am. J. Clin. Nutr. 2011, 94, 1870–1873. [Google Scholar] [CrossRef] [Green Version]
- Chan, G.M.; Armstrong, C.; Moyer-Mileur, L.; Hoff, C. Growth and bone mineralization in children born prematurely. J. Perinatol. 2008, 28, 619–623. [Google Scholar] [CrossRef] [Green Version]
- Abrams, S.A.; Nutrition, C.O. Calcium and vitamin d requirements of enterally fed preterm infants. Pediatrics 2013, 131, e1676–e1683. [Google Scholar] [CrossRef] [Green Version]
- Embleton, N.; Wood, C.L. Growth, bone health, and later outcomes in infants born preterm. J. Pediatr. (Rio J.) 2014, 90, 529–532. [Google Scholar] [CrossRef]
- Quintal, V.S.; Diniz, E.M.; Caparbo Vde, F.; Pereira, R.M. Bone densitometry by dual-energy X-ray absorptiometry (DXA) in preterm newborns compared with full-term peers in the first six months of life. J. Pediatr. (Rio J.) 2014, 90, 556–562. [Google Scholar] [CrossRef] [Green Version]
- Kalkwarf, H.J.; Zemel, B.S.; Yolton, K.; Heubi, J.E. Bone mineral content and density of the lumbar spine of infants and toddlers: Influence of age, sex, race, growth, and human milk feeding. J. Bone Miner. Res. 2013, 28, 206–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefano Mora, L.B.; Gilsanz, V. Pediatric Bone: Biology & Diseases; Elsevier Inc.: Milan, Italy, 2003; p. 22. [Google Scholar]
- Fewtrell, M. Early nutritional predictors of long-term bone health in preterm infants. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 297–301. [Google Scholar] [CrossRef]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef] [Green Version]
- Harding, J.E.; Wilson, J.; Brown, J. Calcium and phosphorus supplementation of human milk for preterm infants. Cochrane. Database. Syst. Rev. 2017, 2, CD003310. [Google Scholar] [CrossRef]
- Macri, E.V.; Gonzales Chaves, M.M.; Rodriguez, P.N.; Mandalunis, P.; Zeni, S.; Lifshitz, F.; Friedman, S.M. High-fat diets affect energy and bone metabolism in growing rats. Eur. J. Nutr. 2012, 51, 399–406. [Google Scholar] [CrossRef]
- Tian, L.; Yu, X. Fat, Sugar, and Bone Health: A Complex Relationship. Nutrients 2017, 9, 506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lac, G.; Cavalie, H.; Ebal, E.; Michaux, O. Effects of a high fat diet on bone of growing rats. Correlations between visceral fat, adiponectin and bone mass density. Lipids Health Dis. 2008, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Malvi, P.; Piprode, V.; Chaube, B.; Pote, S.T.; Mittal, M.; Chattopadhyay, N.; Wani, M.R.; Bhat, M.K. High fat diet promotes achievement of peak bone mass in young rats. Biochem. Biophys. Res. Commun. 2014, 455, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dellatore, P.; Douard, V.; Qin, L.; Watford, M.; Ferraris, R.P.; Lin, T.; Shapses, S.A. High fat diet enriched with saturated, but not monounsaturated fatty acids adversely affects femur, and both diets increase calcium absorption in older female mice. Nutr. Res. 2016, 36, 742–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darling, A.L.; Manders, R.J.F.; Sahni, S.; Zhu, K.; Hewitt, C.E.; Prince, R.L.; Millward, D.J.; Lanham-New, S.A. Dietary protein and bone health across the life-course: An updated systematic review and meta-analysis over 40 years. Osteoporos. Int. 2019, 30, 741–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darling, A.L.; Millward, D.J.; Torgerson, D.J.; Hewitt, C.E.; Lanham-New, S.A. Dietary protein and bone health: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2009, 90, 1674–1692. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [Green Version]
- University of Nebraska Medical Center. Understanding Corrected Age. Available online: https://www.unmc.edu/media/mmi/jackson/TIPS-Intro/Understanding_Corrected_Age.pdf (accessed on 2 March 2021).
- WHO. Calculator: WHO igrowup Z-Scores. Available online: https://apps.cpeg-gcep.net/igrowup_cpeg/ (accessed on 15 January 2021).
- Yumani, D.F.J.; Calor, A.K.; van Weissenbruch, M.M. The Course Of IGF-1 Levels and Nutrient Intake in Extremely and Very Preterm Infants During Hospitalisation. Nutrients 2020, 12, 675. [Google Scholar] [CrossRef] [Green Version]
- Boyce, C.; Watson, M.; Lazidis, G.; Reeve, S.; Dods, K.; Simmer, K.; McLeod, G. Preterm human milk composition: A systematic literature review. Br. J. Nutr. 2016, 116, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Van Toledo, L.v.d.L.M. Parenterale Voeding VKC-NICU; Gereviseerde richtlijn adhv ESPHAN 2018 richtlijn; Amsterdam University Medical Center: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Scafoglieri, A.; Provyn, S.; Wallace, J. Whole Body Composition by Hologic QDR 4500/A DXA: System Reliability Versus User Accuracy and Precision. In Applications and Experiences of Quality Control; InTech: Milan, Italy, 2011; pp. 45–62. [Google Scholar] [CrossRef] [Green Version]
- Shahbazi-Gahrouei, D.; Gholami, M.; Setayandeh, S. A review on natural background radiation. Adv. Biomed. Res. 2013, 2, 65. [Google Scholar] [CrossRef]
- Faerk, J.; Petersen, S.; Peitersen, B.; Michaelsen, K.F. Diet and bone mineral content at term in premature infants. Pediatr. Res. 2000, 47, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Gianni, M.L.; Sannino, P.; Bezze, E.; Plevani, L.; di Cugno, N.; Roggero, P.; Consonni, D.; Mosca, F. Effect of co-morbidities on the development of oral feeding ability in pre-term infants: A retrospective study. Sci. Rep. 2015, 5, 16603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kliegman, R.M.; Walsh, M.C. Neonatal necrotizing enterocolitis: Pathogenesis, classification, and spectrum of illness. Curr. Probl. Pediatr. 1987, 17, 213–288. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Bekhof, J.; Reitsma, J.B.; Kok, J.H.; Van Straaten, I.H. Clinical signs to identify late-onset sepsis in preterm infants. Eur. J. Pediatr. 2013, 172, 501–508. [Google Scholar] [CrossRef]
- Rupich, R.C.; Specker, B.L.; Lieuw, A.F.M.; Ho, M. Gender and race differences in bone mass during infancy. Calcif. Tissue Int. 1996, 58, 395–397. [Google Scholar] [CrossRef]
- Horlick, M.; Thornton, J.; Wang, J.; Levine, L.S.; Fedun, B.; Pierson, R.N., Jr. Bone mineral in prepubertal children: Gender and ethnicity. J. Bone Miner. Res. 2000, 15, 1393–1397. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, C.; Chan, G.M.; Moyer-Mileur, L.; Archuleta, M. Seven year follow-up of preterm infant’s bone mineralization. Pediatric. Res. 1997, 41, 190. [Google Scholar] [CrossRef] [Green Version]
- McVey, M.K.; Geraghty, A.A.; O’Brien, E.C.; McKenna, M.J.; Kilbane, M.T.; Crowley, R.K.; Twomey, P.J.; McAuliffe, F.M. The impact of diet, body composition, and physical activity on child bone mineral density at five years of age-findings from the ROLO Kids Study. Eur. J. Pediatr. 2020, 179, 121–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Lagemaat, M.; Rotteveel, J.; van Weissenbruch, M.M.; Lafeber, H.N. Increased gain in bone mineral content of preterm infants fed an isocaloric, protein-, and mineral-enriched postdischarge formula. Eur. J. Nutr. 2013, 52, 1781–1785. [Google Scholar] [CrossRef]
- Fewtrell, M.S.; Williams, J.E.; Singhal, A.; Murgatroyd, P.R.; Fuller, N.; Lucas, A. Early diet and peak bone mass: 20 year follow-up of a randomized trial of early diet in infants born preterm. Bone 2009, 45, 142–149. [Google Scholar] [CrossRef]
- Hovi, P.; Andersson, S.; Jarvenpaa, A.L.; Eriksson, J.G.; Strang-Karlsson, S.; Kajantie, E.; Makitie, O. Decreased bone mineral density in adults born with very low birth weight: A cohort study. PLoS Med. 2009, 6, e1000135. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.M.; Wright, N.P.; Wales, J.K.; Mackenzie, C.; Primhak, R.A.; Eastell, R.; Walsh, J.S. Very low birth weight survivors have reduced peak bone mass and reduced insulin sensitivity. Clin. Endocrinol. (Oxf.) 2011, 75, 443–449. [Google Scholar] [CrossRef]
- Hernandez, C.J.; Beaupre, G.S.; Carter, D.R. A theoretical analysis of the relative influences of peak BMD, age-related bone loss and menopause on the development of osteoporosis. Osteoporos. Int. 2003, 14, 843–847. [Google Scholar] [CrossRef]
- Rigo, J.; Pieltain, C.; Salle, B.; Senterre, J. Enteral calcium, phosphate and vitamin D requirements and bone mineralization in preterm infants. Acta. Paediatr. 2007, 96, 969–974. [Google Scholar] [CrossRef]
- Zhao, Z.; Ding, M.; Hu, Z.; Dai, Q.; Satija, A.; Zhou, A.; Xu, Y.; Zhang, X.; Hu, F.B.; Xu, H. Trajectories of length, weight, and bone mineral density among preterm infants during the first 12 months of corrected age in China. BMC Pediatr. 2015, 15, 91. [Google Scholar] [CrossRef] [Green Version]
- Bitman, J.; Wood, L.; Hamosh, M.; Hamosh, P.; Mehta, N.R. Comparison of the lipid composition of breast milk from mothers of term and preterm infants. Am. J. Clin. Nutr. 1983, 38, 300–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rings, E.H.; Minich, D.M.; Vonk, R.J.; Stellaard, F.; Fetter, W.P.; Verkade, H.J. Functional development of fat absorption in term and preterm neonates strongly correlates with ability to absorb long-chain Fatty acids from intestinal lumen. Pediatr. Res. 2002, 51, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heird, W.C. Determination of nutritional requirements in preterm infants, with special reference to ’catch-up’ growth. Semin. Neonatol. 2001, 6, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Ramel, S.E.; Brown, L.D.; Georgieff, M.K. The Impact of Neonatal Illness on Nutritional Requirements-One Size Does Not Fit All. Curr. Pediatr. Rep. 2014, 2, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Hongo, T.; Kotake, K.; Muramatsu, H.; Omura, D.; Yano, Y.; Hasegawa, D.; Momoki, N.; Takahashi, K.; Nozaki, S.; Fujiwara, T. Loss of bone mineral density following sepsis using Hounsfield units by computed tomography. Acute Med. Surg. 2019, 6, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.M.; Cuthbertson, B.; Harvie, J.; Webster, N.; Robins, S.; Ralston, S.H. Increased bone resorption in the critically ill: Association with sepsis and increased nitric oxide production. Crit. Care Med. 2002, 30, 837–840. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | OMM | OMM + BMF (4.4 g/100 mL) | DHM | DHM + BMF | PF |
|---|---|---|---|---|---|
| Energy (kcal) | 68.5 | 83.8 | 60 | 75 | 66 |
| Protein (g) | 1.5 | 2.6 | 0.8 | 1.9 | 2.6 |
| Carbohydrates (g) | 7.3 | 10.0 | 7.5 | 10.2 | 8.9 |
| Fat (g) | 3.3 | 3.3 | 2.9 | 2.9 | 2 |
| Extremely Preterm, n = 21 | Very Preterm, n = 37 | p-Value | |
|---|---|---|---|
| (<28 Weeks GA) | (28–<32 Weeks GA) | ||
| Gestational age (weeks), mean (SD) | 26.9 (0.9) | 29.8 (1) | <0.001 1 |
| Gender, n (%) | |||
| Male | 10 (48) | 20 (54) | 0.119 2 |
| Female | 11 (52) | 17 (46) | |
| Ethnicity, n (%) | |||
| White | 14 (67) | 29 (78) | 0.774 2 |
| Other | 7 (33) | 8 (22) | |
| Birthweight (g), mean (SD) | 963.9 (143.2) | 1269.9 (306) | <0.001 1 |
| Birthweight SDS, mean (SD) | 0.3 (0.6) | −0.1 (0.8) | 0.049 1 |
| Weight at TCA (g), mean (SD) | 4208.6 (669.1) | 4065.2 (644.8) | 0.856 1 |
| Weight SDS at TCA, mean (SD) | 0.4 (1.1) | −0.1 (1.2) | 0.029 1 |
| Weight at 6 months CA (g), mean (SD) | 7099.2 (791.9) | 7379.5 (864.1) | 0.423 1 |
| Weight SDS at 6 month CA, mean (SD) | −0.6 (1.3) | −0.7 (1) | 0.829 1 |
| Comorbidities, n (%) | |||
| BPD | 14 (67) | 10 (27) | 0.003 2 |
| LOS | 11 (52) | 13 (35) | 0.157 2 |
| NEC | 2 (1) | 3 (1) | 0.397 2 |
| Extremely Preterm (n = 21) | Very Preterm (n = 37) | ||
|---|---|---|---|
| Macronutrient Intake in % of Energy, Mean (SD) | |||
| Week 1 | Fat | 17.6 (0.09) | 18.4 (0.2) |
| Protein | 16.5 (0.09) | 15.7 (0.2.) | |
| Carbohydrate | 64.9 (0.16) | 63.9 (0.6) | |
| Week 2 | Fat | 19.2 (0.06) | 19.1 (0.2) |
| Protein | 15.7 (0.14) | 15.2 (0.1) | |
| Carbohydrate | 63.4 (0.6) | 62.2 (0.5) | |
| Week 3 | Fat | 19.4 (0.05) | 19.3 (0.2) |
| Protein | 15.6 (0.1) | 15.6 (0.1) | |
| Carbohydrate | 63.1 (0.6) | 61.3 (0.5) | |
| Week 4 | Fat | 19.6 (0.07) | 19.2 (0.2) |
| Protein | 15.7 (0.1) | 15.6 (0.09) | |
| Carbohydrate | 61.9 (0.6) | 62 (0.6) | |
| Extremely Preterm, n = 14 | Very Preterm, n = 23 | p Value 1 | ||
|---|---|---|---|---|
| BMC (g), mean (SD) | TCA | 62.2 (14.9) | 56.3 (14.0) | 0.69 |
| 6 months CA | 129.7 (35.1) | 115.5 (24.9) | 0.09 | |
| p-value 2 | 0.29 | 0.84 | ||
| BMD (g/cm2), mean (SD) | TCA | 0.17 (0.02) | 0.16 (0.02) | 0.91 |
| 6 months CA | 0.23 (0.04) | 0.21 (0.04) | 0.88 | |
| p-value 3 | 0.29 | 0.84 |
| Variables | Model R2 | Model p-Value | B (SE) | β | p-Value |
|---|---|---|---|---|---|
| BMC (g) at TCA, n = 58 | |||||
| Model 1 | 0.496 | 0.004 | |||
| Constant | 19.08 (47.89) | 0.694 | |||
| GA | −1.35 (1.28) | −0.172 | 0.303 | ||
| Gender | −5.80 (4.33) | −0.210 | 0.193 | ||
| Ethnicity | −0.97 (1.03) | −0.148 | 0.355 | ||
| LOS | −7.79 (4.67) | −0.293 | 0.108 | ||
| Mean energy intake in kcal kg−1 day−1 week 1–4 | 0.83 (0.25) | 0.546 | 0.002 | ||
| Model 2 | 0.46 | 0.001 | |||
| Constant | 42.09 (40.82) | 0.312 | |||
| GA | −1.45 (1.25) | −0.185 | 0.259 | ||
| LOS | −9.66 (4.47) | −0.363 | 0.04 | ||
| Mean fat intake in g kg−1 day−1 week 1–4 | 14.40 (4.39) | 0.508 | 0.003 | ||
| BMD (g/cm2) at TCA, n = 58 | |||||
| Model 3 | 0.45 | 0.021 | |||
| Constant | 0.56 (0.05) | 0.274 | |||
| Gender | −0.01 (0.01) | −0.281 | 0.137 | ||
| Ethnicity | −0.00 (0.00) | −0.154 | 0.372 | ||
| BPD | 0.01 (0.01) | 0.25 | 0.186 | ||
| NEC | −0.01 (0.01) | −0.221 | 0.368 | ||
| Birthweight SDS | −0.00 (0.00) | −0.153 | 0.409 | ||
| Mean energy intake in kcal kg−1 day−1 week 1–4 | 0.00 (0.00) | 0.57 | 0.019 | ||
| Model 4 | 0.474 | 0.014 | |||
| Constant | 0.14 (0.06) | 0.022 | |||
| GA | −0.00 (0.00) | −0.226 | 0.217 | ||
| Gender | −0.01 (0.01) | −0.271 | 0.14 | ||
| Ethnicity | −0.00 (0.00) | −0.147 | 0.395 | ||
| LOS | −0.01 (0.01) | −0.221 | 0.237 | ||
| Birthweight SDS | −0.01 (0.00) | −0.192 | 0.302 | ||
| Mean fat intake in g kg−1 day−1 week 1–4 | 0.03 (0.01) | 0.687 | 0.001 | ||
| Variables | Model R2 | Model p-Value | B (SE) | β | p-Value |
|---|---|---|---|---|---|
| BMC (g) at 6 months CA, n = 58 | |||||
| Model 1 | 0.394 | 0.021 | |||
| Constant | 99.07 (103.12) | 0.345 | |||
| GA | −4.08 (2.77) | −0.222 | 0.151 | ||
| Ethnicity | 1.12 (2.23) | 0.08 | 0.621 | ||
| Birthweight SDS | 2.65 (6.40) | 0.07 | 0.682 | ||
| Weight SDS 6 m CA | 10.62 (4.06) | 0.417 | 0.014 | ||
| NEC | 19.37 (14.78) | 0.232 | 0.201 | ||
| Mean energy intake in kcal kg−1 day−1 week 1–4 | 1.28 (0.57) | 0.406 | 0.033 | ||
| Model 2 | 0.337 | 0.013 | |||
| Constant | 127.43 (101.60) | 0.219 | |||
| GA | −3.69 (2.77) | −0.201 | 0.194 | ||
| Weight SDS 6 m CA | 11.33 (3.86) | 0.437 | 0.007 | ||
| NEC | 13.56 (14.26) | 0.163 | 0.349 | ||
| Mean protein intake in g kg−1 day−1 week 1–4 | 30.59 (24.71) | 0.354 | 0.046 | ||
| Model 3 | 0.247 | 0.011 | |||
| Constant | 161.67 (93.78) | 0.095 | |||
| GA | −4.47(2.76) | −0.243 | 0.115 | ||
| Weight SDS 6 m CA | 10.78 (3.87) | 0.423 | 0.009 | ||
| NEC | 14.15 (14.66) | 0.17 | 0.342 | ||
| Mean fat intake in g kg−1 day−1 week 1–4 | 22.14 (11.22) | 0.343 | 0.05 | ||
| BMD (g/cm2) at 6 months CA, n = 58 | |||||
| Model 4 | 0.238 | 0.036 | |||
| Constant | −0.05 (0.09) | 0.609 | |||
| Gender | 0.015 (0.01) | 0.199 | 0.218 | ||
| NEC | 0.03 (0.02) | 0.276 | 0.143 | ||
| Mean energy intake in kcal kg−1 day−1 week 1–4 | 0.01 (0.00) | 0.501 | 0.01 | ||
| Model 5 | 0.207 | 0.127 | |||
| Constant | 0.02 (0.08) | 0.767 | |||
| Gender | 0.02 (0.01) | 0.298 | 0.109 | ||
| NEC | 0.03 (0.02) | 0.232 | 0.224 | ||
| Weight SDS 6 m CA | 0.01 (0.01) | 0.213 | 0.252 | ||
| Mean protein intake in g kg−1 day−1 week 1–4 | 0.05 (0.02) | 0.404 | 0.036 | ||
| Model 6 | 0.177 | 0.105 | |||
| Constant | 0.04 (0.07) | 0.601 | |||
| Gender | 0.02 (0.01) | 0.204 | 0.223 | ||
| NEC | 0.03 (0.02) | 0.23 | 0.236 | ||
| Mean fat intake in g kg−1 day−1 week 1–4 | 0.04 (0.02) | 0.411 | 0.037 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calor, A.K.; Yumani, D.F.J.; van Weissenbruch, M.M. Early Nutrition during Hospitalization in Relation to Bone Health in Preterm Infants at Term Age and Six Months Corrected Age. Nutrients 2021, 13, 1192. https://doi.org/10.3390/nu13041192
Calor AK, Yumani DFJ, van Weissenbruch MM. Early Nutrition during Hospitalization in Relation to Bone Health in Preterm Infants at Term Age and Six Months Corrected Age. Nutrients. 2021; 13(4):1192. https://doi.org/10.3390/nu13041192
Chicago/Turabian StyleCalor, Alexandra K., Dana F. J. Yumani, and Mirjam M. van Weissenbruch. 2021. "Early Nutrition during Hospitalization in Relation to Bone Health in Preterm Infants at Term Age and Six Months Corrected Age" Nutrients 13, no. 4: 1192. https://doi.org/10.3390/nu13041192