
The Role of Inflammatory Diet and Vitamin D on the Link between Periodontitis and Cognitive Function: A Mediation Analysis in Older Adults

 ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
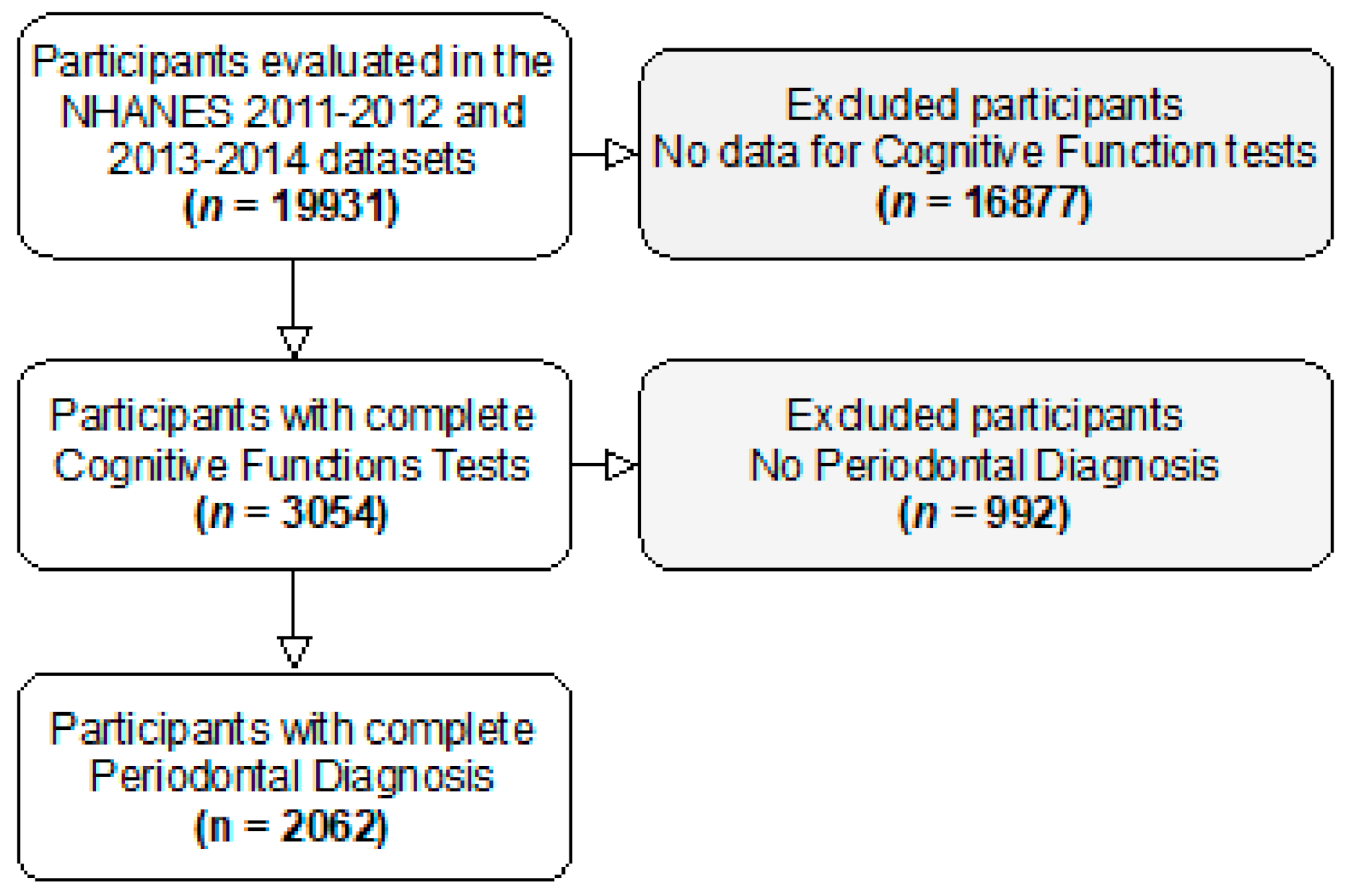
2.1. Study Design and Participants
2.2. Cognitive Assessment
2.3. Periodontal Assessment
2.4. Dietary Inflammatory Index (DII)
2.5. Sociodemographic and Health-Related Variables
2.6. Biochemical Parameters
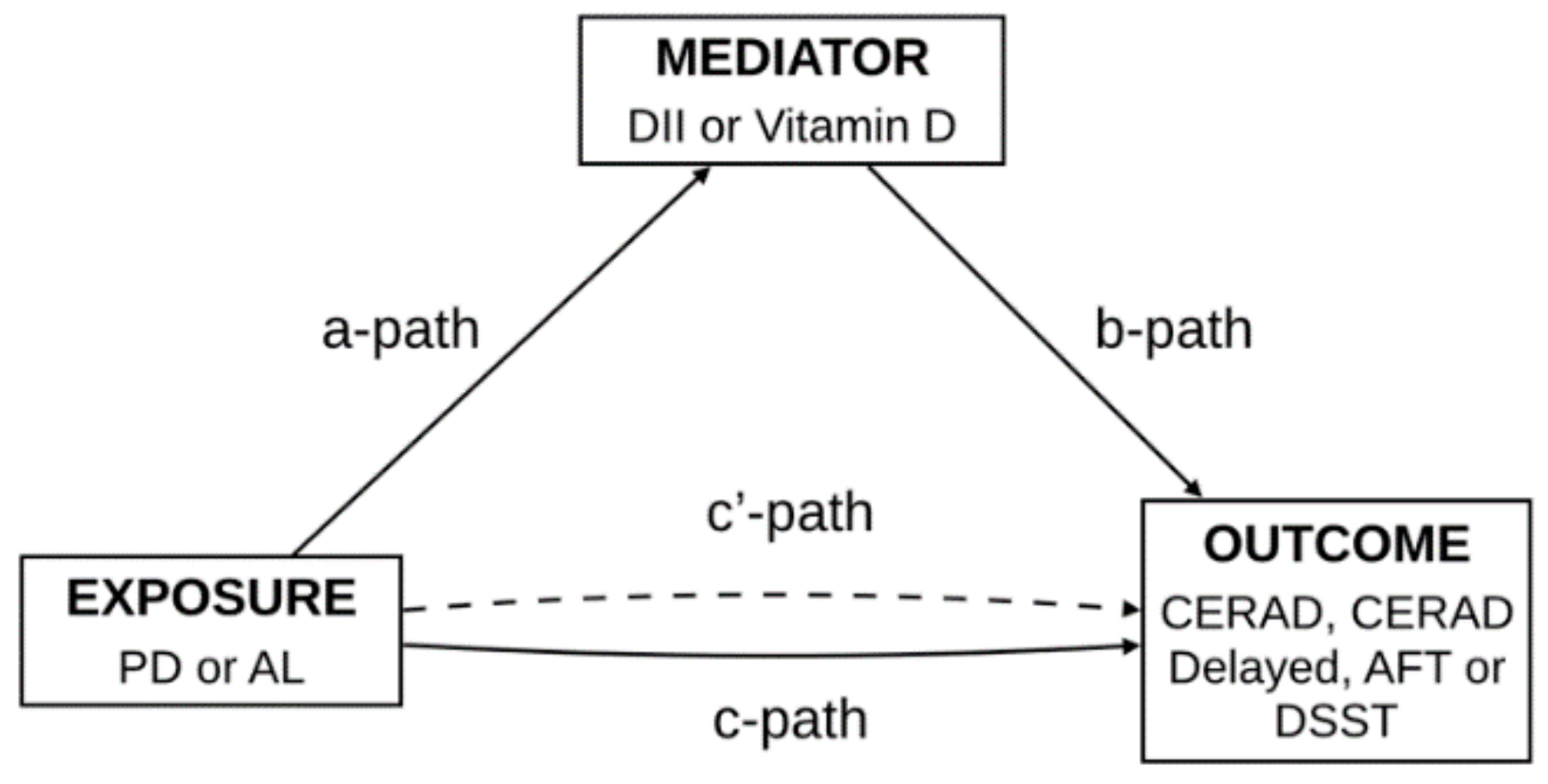
2.7. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Mediation Analysis
3.2.1. Proinflammatory Diet
3.2.2. Vitamin D Deficit
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dementia. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 19 October 2020).
- Alzheimer’s Disease International. World Alzheimer Report 2015, The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015; Available online: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf (accessed on 29 August 2020).
- Wu, Y.-T.; Beiser, A.S.; Breteler, M.M.B.; Fratiglioni, L.; Helmer, C.; Hendrie, H.C.; Honda, H.; Ikram, M.A.; Langa, K.M.; Lobo, A.; et al. The changing prevalence and incidence of dementia over time—Current evidence. Nat. Rev. Neurol. 2017, 13, 327–339. [Google Scholar] [CrossRef] [Green Version]
- Brayne, C.; Davis, D. Making Alzheimer’s and dementia research fit for populations. Lancet 2012, 380, 1441–1443. [Google Scholar] [CrossRef] [Green Version]
- Fang, W.-L.; Jiang, M.-J.; Gu, B.-B.; Wei, Y.-M.; Fan, S.-N.; Liao, W.; Zheng, Y.-Q.; Liao, S.-W.; Xiong, Y.; Li, Y.; et al. Tooth loss as a risk factor for dementia: Systematic review and meta-analysis of 21 observational studies. BMC Psychiatry 2018, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, K.; Ohara, T.; Furuta, M.; Takeshita, T.; Shibata, Y.; Hata, J.; Yoshida, D.; Yamashita, Y.; Ninomiya, T. Tooth loss and risk of dementia in the community: The Hisayama Study. J. Am. Geriatr. Soc. 2017, 65, e95–e100. [Google Scholar] [CrossRef]
- Chen, J.; Ren, C.-J.; Wu, L.; Xia, L.-Y.; Shao, J.; Leng, W.-D.; Zeng, X.-T. Tooth loss is associated with increased risk of dementia and with a dose-response relationship. Front. Aging Neurosci. 2018, 10, 415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, A.; Chen, Y.; van der Sluis, L.W.M.; Schuller, A.A.; Tjakkes, G.-H. White blood cell count mediates the association between periodontal inflammation and cognitive performance measured by digit symbol substitution test among older, U.S. adults. J. Gerontol. Ser. A 2009. [Google Scholar] [CrossRef]
- Demmer, R.T.; Norby, F.L.; Lakshminarayan, K.; Walker, K.A.; Pankow, J.S.; Folsom, A.R.; Mosley, T.; Beck, J.; Lutsey, P.L. Periodontal disease and incident dementia: The Atherosclerosis Risk in Communities Study (ARIC). Neurology. 2020, 95, 1660–1671. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Beydoun, H.A.; Hossain, S.; El-Hajj, Z.W.; Weiss, J.; Zonderman, A.B. Clinical and bacterial markers of periodontitis and their association with incident all-cause and alzheimer’s disease dementia in a large national survey. J. Alzheimer’s Dis. 2020, 75, 157–172. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Beydoun, H.A.; Weiss, J.; Hossain, S.; El-Hajj, Z.W.; Zonderman, A.B. Helicobacter pylori, periodontal pathogens, and their interactive association with incident all-cause and Alzheimer’s disease dementia in a large national survey. Mol. Psychiatry 2020, 1–16. [Google Scholar] [CrossRef]
- Kim, D.-H.; Jeong, S.-N.; Lee, J.-H. Severe periodontitis with tooth loss as a modifiable risk factor for the development of Alzheimer, vascular, and mixed dementia: National Health Insurance Service-National Health Screening Retrospective Cohort 2002–2015. J. Periodontal Implant. Sci. 2020, 50, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, N.-S.; Chung, C.-H.; Yeh, C.-B.; Huang, R.-Y.; Yuh, D.-Y.; Huang, S.-Y.; Lu, R.-B.; Chang, H.-A.; Kao, Y.-C.; Chiang, W.-S.; et al. Are chronic periodontitis and gingivitis associated with dementia? A nationwide, retrospective, matched-cohort study in Taiwan. Neuroepidemiology 2016, 47, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, J.L.; Dawson, D.; Emecen-Huja, P.; Nagarajan, R.; Howard, K.; Grady, M.E.; Thompson, K.; Peyyala, R.; Al-Attar, A.; Lethbridge, K.; et al. The periodontal war: Microbes and immunity. Periodontology 2000 2017, 75, 52–115. [Google Scholar] [CrossRef] [PubMed]
- Slots, J. Periodontitis: Facts, fallacies and the future. Periodontology 2000 2017, 75, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef]
- Darveau, R.P. Periodontitis: A polymicrobial disruption of host homeostasis. Nat. Rev. Microbiol. 2010, 8, 481–490. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Proença, L.; Bellini, D.H.; Chambrone, L.; Alcoforado, G.; Mendes, J.J. The impact of nonsurgical periodontal treatment on oral health-related quality of life: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 585–596. [Google Scholar] [CrossRef]
- Tonsekar, P.P.; Jiang, S.S.; Yue, G. Periodontal disease, tooth loss and dementia: Is there a link? A systematic review. Gerodontology 2017, 34, 151–163. [Google Scholar] [CrossRef]
- Maldonado, A.; Laugisch, O.; Bürgin, W.; Sculean, A.; Eick, S. Clinical periodontal variables in patients with and without de-mentia—A systematic review and meta-analysis. Clin Oral Investig. 2018, 22, 2463–2474. [Google Scholar] [CrossRef]
- Leigh, S.-J.; Morris, M.J. Diet, inflammation and the gut microbiome: Mechanisms for obesity-associated cognitive impairment. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165767. [Google Scholar] [CrossRef]
- Moretti, R.; Peinkhofer, C. B Vitamins and fatty acids: What do they share with small vessel disease-related dementia? Int. J. Mol. Sci. 2019, 20, 5797. [Google Scholar] [CrossRef] [Green Version]
- Hayden, K.M.; Beavers, D.P.; Steck, S.E.; Hebert, J.R.; Tabung, F.K.; Shivappa, N.; Casanova, R.; Manson, J.E.; Padula, C.B.; Salmoirago-Blotcher, E.; et al. The association between an inflammatory diet and global cognitive function and incident dementia in older women: The Women’s Health Initiative Memory Study. Alzheimer’s Dement. 2017, 13, 1187–1196. [Google Scholar] [CrossRef]
- Ozawa, M.; Shipley, M.; Kivimaki, M.; Singh-Manoux, A.; Brunner, E.J. Dietary pattern, inflammation and cognitive decline: The Whitehall II prospective cohort study. Clin. Nutr. 2017, 36, 506–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woelber, J.P.; Bremer, K.; Vach, K.; König, D.; Hellwig, E.; Ratka-Krüger, P.; Al-Ahmad, A.; Tennert, C. An oral health optimized diet can reduce gingival and periodontal inflammation in humans—A randomized controlled pilot study. BMC Oral Health 2016, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.; Tsapanou, A.; Manly, J.; Schupf, N.; Brickman, A.M.; Gu, Y. Vitamin D intake is associated with dementia risk in the Washington Heights-Inwood Columbia Aging Project (WHICAP). Alzheimer’s Dement. 2020, 16. [Google Scholar] [CrossRef]
- Soysal, P.; Dokuzlar, O.; Erken, N.; Günay, F.S.D.; Isik, A.T. The relationship between dementia subtypes and nutritional parameters in older adults. J. Am. Med. Dir. Assoc. 2020, 21, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Sultan, S.; Taimuri, U.; Basnan, S.A.; Ai-Orabi, W.K.; Awadallah, A.; Almowald, F.; Hazazi, A. Low vitamin d and its association with cognitive impairment and dementia. J. Aging Res. 2020, 2020, 6097820. [Google Scholar] [CrossRef]
- Machado, V.; Lobo, S.; Proença, L.; Mendes, J.J.; Botelho, J. Vitamin D and periodontitis: A systematic review and meta-analysis. Nutrients 2020, 12, 2177. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of obser-vational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, 1623–1627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brody, D.J.; Kramarow, E.A.; Taylor, C.A.; McGuire, L.C. Cognitive performance in adults aged 60 and Over: National Health and Nutrition Examination Survey, 2011–2014. Natl. Health. Stat. Rep. 2019, 126, 1–23. [Google Scholar]
- Moms, J.C.; Heyman, A.; Mohs, R.C.; Hughes, J.P.; Van Belle, G.; Fillenbaum, G.; Mellits, E.D.; Clark, C. The consortium to establish a registry for alzheimer’s disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology 1989, 39, 1159. [Google Scholar] [CrossRef]
- Strauss, E.; Sherman, E.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms and Commentary; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- Salthouse, T.A. What do adult age differences in the digit symbol substitution test reflect? J. Gerontol. 1992, 47, P121–P128. [Google Scholar] [CrossRef] [Green Version]
- Dye, B.A.; Thornton-Evans, G. A Brief history of national surveillance efforts for periodontal disease in the United States. J. Periodontol. 2007, 78, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Eke, P.I.; Page, R.C.; Wei, L.; Thornton-Evans, G.; Genco, R.J. Update of the case definitions for population-based surveillance of periodontitis. J. Periodontol. 2012, 83, 1449–1454. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Muñoz Aguilera, E.; Leira, Y.; Miró Catalina, Q.; Orlandi, M.; Czesnikiewicz-Guzik, M.; Guzik, T.J.; Hingorani, A.D.; Nart, J.; D’Aiuto, F. Is systemic inflammation a missing link between periodontitis and hypertension? Results from two large populations-based surveys. J. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Beck, J.D.; Moss, K.L.; Morelli, T.; Offenbacher, S. Periodontal profile class is associated with prevalent diabetes, coronary heart disease, stroke, and systemic markers of C-reactive protein and interleukin-6. J. Periodontol. 2018, 89, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yu, Y.; Nickel, J.C.; Iwasaki, L.R.; Duan, P.; Simmer-Beck, M.; Brown, L. Gender differences in the association of periodontitis and type 2 diabetes. Int. Dent. J. 2018, 68, 433–440. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simmone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention. MEC Laboratory Procedures Manual; Center for Disease Control and Prevention: Atlanta, GA, USA, 2016. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_15_16/2016_MEC_Laboratory_Procedures_Manual.pdf (accessed on 30 August 2020).
- Center for Disease Control and Prevention. NHANES Laboratory Procedures Manual; Center for Disease Control and Prevention: Atlanta, GA, USA, 2009. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_09_10/lab.pdf (accessed on 30 August 2020).
- Botelho, J.; Machado, V.; Proença, L.; Mendes, J.J. The 2018 periodontitis case definition improves accuracy performance of full-mouth partial diagnostic protocols. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef]
- Botelho, J.; Lyra, P.; Proença, L.; Godinho, C.; Mendes, J.J.; Machado, V. Relationship between blood and standard biochemistry levels with periodontitis in parkinson’s disease patients: Data from the NHANES 2011–2012. J. Pers. Med. 2020, 10, 69. [Google Scholar] [CrossRef]
- Leira, Y.; Carballo, Á.; Orlandi, M.; Aldrey, J.M.; Pías-Peleteiro, J.M.; Moreno, F.; Vázquez-Vázquez, L.; Campos, F.; D’Aiuto, F.; Castillo, J.; et al. Periodontitis and systemic markers of neurodegeneration: A case–control study. J. Clin. Periodontol. 2020, 47, 561–571. [Google Scholar] [CrossRef]
- Cavicchia, P.P.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Hébert, J.R. A new dietary inflammatory index predicts interval changes in serum high-sensitivity c-reactive protein. J. Nutr. 2009, 139, 2365–2372. [Google Scholar] [CrossRef]
- Carson, S.J.; Burns, J. Impact of smoking on tooth loss in adults. Evid. Based Dent. 2016, 17, 73–74. [Google Scholar] [CrossRef] [Green Version]
- Niegawa, T.; Takitani, K.; Takaya, R.; Ishiro, M.; Kuroyanagi, Y.; Okasora, K.; Minami, Y.; Matsuda, T.; Tamai, H. Evaluation of uric acid levels, thyroid function, and anthropometric parameters in Japanese children with Down syndrome. J. Clin. Biochem. Nutr. 2018, 62, 179–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; González-Gil, E.; Frederic, G.; et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61, 1–23. [Google Scholar] [CrossRef]
- Ramallal, R.; Toledo, E.; Martínez, J.A.; Shivappa, N.; Hébert, J.R.; Martínez-González, M.A.; Ruiz-Canela, M. Inflammatory potential of diet, weight gain, and incidence of overweight/obesity: The SUN cohort. Obesity 2017, 25, 997–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neufcourt, L.; Assmann, K.E.; Fezeu, L.; Touvier, M.; Graffouillère, L.; Shivappa, N.; Hebert, J.R.; Wirth, M.D.; Hercberg, S.; Galan, P.; et al. Prospective association between the dietary inflammatory index and metabolic syndrome: Findings from the SU.VI.MAX study. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 988–996. [Google Scholar] [CrossRef]
- Kheirouri, S.; Alizadeh, M. Dietary inflammatory potential and the risk of neurodegenerative diseases in adults. Epidemiol. Rev. 2019, 41, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Vasefi, M.; Hudson, M.; Ghaboolian-Zare, E. Diet Associated with Inflammation and Alzheimer’s Disease. J. Alzheimer’s Dis. Rep. 2019, 3, 299–309. [Google Scholar] [CrossRef] [Green Version]
- Botelho, J.; Machado, V.; Proença, L.; Delgado, A.S.; Mendes, J.J. Vitamin D deficiency and oral Health: A comprehensive review. Nutrients 2020, 12, 1471. [Google Scholar] [CrossRef]
- Etgen, T.; Chonchol, M.; Förstl, H.; Sander, D. Chronic kidney disease and cognitive impairment: A Systematic review and meta-analysis. Am. J. Nephrol. 2012, 35, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Balion, C.; Griffith, L.E.; Strifler, L.; Henderson, M.; Patterson, C.; Heckman, G.; Llewellyn, D.J.; Raina, P. Vitamin D, cognition, and dementia: A systematic review and meta-analysis. Neurology 2012, 79, 1397–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landel, V.; Annweiler, C.; Millet, P.; Morello, M.; Féron, F. Vitamin D, cognition and alzheimer’s Disease: The therapeutic benefit is in the d-tails. J. Alzheimer’s Dis. 2016, 53, 419–444. [Google Scholar] [CrossRef] [Green Version]
- Tran, D.T.; Gay, I.; Du, X.L.; Fu, Y.; Bebermeyer, R.D.; Neumann, A.S.; Streckfus, C.; Chan, W.; Walji, M.F. Assessing periodontitis in populations: A systematic review of the validity of partial-mouth examination protocols. J. Clin. Periodontol. 2013, 40, 1064–1071. [Google Scholar] [CrossRef]
- Eke, P.; Thornton-Evans, G.; Wei, L.; Borgnakke, W.; Dye, B. Accuracy of NHANES periodontal examination protocols. J. Dent. Res. 2010, 89, 1208–1213. [Google Scholar] [CrossRef]
- Deng, F.E.; Shivappa, N.; Tang, Y.; Mann, J.R.; Hebert, J.R. Association between diet-related inflammation, all-cause, all-cancer, and cardiovascular disease mortality, with special focus on prediabetics: Findings from NHANES III. Eur. J. Nutr. 2017, 56, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Kotsakis, G.A.; Chrepa, V.; Shivappa, N.; Wirth, M.; Hébert, J.; Koyanagi, A.; Tyrovolas, S. Diet-borne systemic inflammation is associated with prevalent tooth loss. Clin. Nutr. 2018, 37, 1306–1312. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No Periodontitis (n = 625) | Periodontitis (n = 1437) | p-Value | |
|---|---|---|---|
| Age (years), mean (SD) | 68.74 (0.27) | 69.0 (0.18) | 0.395 |
| Gender, n (%) | |||
| Males | 228 (36.5) | 816 (56.8) | <0.001 |
| Females | 397 (63.5) | 621 (43.2) | |
| Race/ethnicity, n (%) | |||
| Mexican American | 50 (8.0) | 162 (11.2) | <0.001 |
| Non-Hispanic White | 46 (7.3) | 173 (12.0) | |
| Non-Hispanic Black | 373 (59.7) | 559 (38.9) | |
| Other Hispanic | 92 (14.7) | 371 (25.8) | |
| Other race | 64 (10.2) | 172 (12) | |
| Education level, n (%) | |||
| <High school | 39 (6.2) | 215 (14.9) | <0.001 |
| High school | 179 (28.6) | 523 (36.3) | |
| >High school | 407 (65.1) | 699 (48.6) | |
| Smoking status, n (%) | |||
| Never | 390 (62.4) | 687 (48.5) | |
| Former | 204 (32.6) | 530 (36.9) | |
| Current | 31 (5.0) | 209 (14.6) | |
| BMI (kg/m2), mean (SD) | 28.8 (0.24) | 28.7 (0.16) | 0.408 |
| Family income/poverty ratio, mean (SD) | 2.98 (1.69) | 2.40 (1.62) | <0.001 |
| Marital status | |||
| Single | 39 (6.2) | 94 (6.5) | 0.012 |
| Married/living with a partner | 404 (64.6) | 831 (57.8) | |
| Divorced/separated/widowed | 182 (29.1) | 512 (35.6) | |
| Chronic medical conditions, mean (SD) | 0.73 (0.44) | 0.75 (0.43) | 0.351 |
| Diabetes, n (%) | 99 (15.8) | 340 (26.7) | 0.001 |
| Hypertension, n (%) | 159 (25.5) | 439 (30.9) | 0.014 |
| Minutes of sedentarism (min), mean (SD) | 435.4 (577.4) | 462.2 (895.7) | <0.001 |
| Cognitive function, mean (SD) | |||
| CERAD word learning | 19.2 (6.1) | 17.2 (6.8) | <0.001 |
| CERAD delayed recall | 6.2 (2.6) | 5.4 (2.7) | <0.001 |
| Animal fluency test | 17.1 (6.7) | 15.0 (6.9) | <0.001 |
| DSST | 50.2 (20.4) | 40.9 (21.1) | <0.001 |
| Periodontal measurements, mean (SD) | |||
| PD (mm) | 1.13 (0.32) | 1.87 (0.80) | <0.001 |
| AL (mm) | 1.34 (0.42) | 2.51 (1.23) | <0.001 |
| Missing teeth | 6.9 (7.3) | 9.1 (7.2) | <0.001 |
| DII, mean (SD) | −0.32 (1.81) | −0.05 (1.80) | <0.001 |
| Biochemical parameters, mean (SD) | |||
| Vitamin D (nmol/L) | 82.92 (30.47) | 72.87 (30.67) | <0.001 |
| WBC (109/L) | 6.57 (1.79) | 7.02 (2.56) | <0.001 |
| HDL (mg/dL) | 57.57 (16.29) | 55.20 (16.22) | <0.001 |
| LDL (mg/dL) | 112.00 (37.27) | 110.07 (36.49) | 0.438 |
| Total cholesterol (mg/dL) | 193.59 (42.49) | 190.68 (41.06) | 0.065 |
| Triglycerides (mg/dL) | 118.07 (63.25) | 121.25 (73.92) | 0.505 |
| Exposure: PD and Outcome: CERAD Word Learning Test | ||||||
|---|---|---|---|---|---|---|
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.21 (0.08) ** | −0.37 (0.11) *** | −0.41 (0.25) | −0.08 (0.04) * | −0.48 (0.25) | 16.2 |
| Vitamin D (nmol/L) | −6.24 (1.29) *** | 0.01 (0.01) | −0.36 (0.27) | −0.06 (0.04) | −0.42 (0.27) | - |
| Exposure: AL and Outcome: CERAD Word Learning Test | ||||||
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.14 (0.05) ** | −0.37 (0.11) *** | −0.20 (0.17) | −0.05 (0.02) * | −0.26 (0.17) | 19.9 |
| Vitamin D (nmol/L) | −3.80 (0.84) *** | 0.05 (0.03) | −0.24 (0.18) | −0.04 (0.03) | −0.28 (0.18) | - |
| Exposure: PD and Outcome: CERAD Delayed Recall Test | ||||||
|---|---|---|---|---|---|---|
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.21 (0.08) ** | −0.13 (0.05) *** | −0.10 (0.11) | −0.03 (0.01) * | −0.12 (0.11) | 22.8 |
| Vitamin D (nmol/L) | −6.24 (1.29) *** | 0.01 (0.00) * | −0.06 (0.11) | −0.05 (0.02) * | −0.11 (0.11) | 73.2 |
| Exposure: AL and Outcome: Delayed Recall Test | ||||||
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.14 (0.05) ** | −0.13 (0.05) ** | −0.03 (0.07) | −0.02 (0.01) * | −0.05 (0.07) | 36.4 |
| Vitamin D (nmol/L) | −3.80 (0.84) *** | 0.01 (0.00) * | −0.04 (0.07) | −0.03 (0.01) * | −0.06 (0.07) | 63.3 |
| Exposure: PD and Outcome: Animal Fluency Test | ||||||
|---|---|---|---|---|---|---|
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.21 (0.08) ** | −0.46 (0.11) *** | −0.49 (0.27) | −0.10 (0.05) * | −0.58 (0.27) * | 16.7 |
| Vitamin D (nmol/L) | −6.24 (1.29) *** | 0.01 (0.01) * | −0.42 (0.28) | −0.08 (0.05) * | −0.51 (0.28) | 12.2 |
| Exposure: AL and Outcome: Animal Fluency Test | ||||||
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.14 (0.05) ** | −0.46 (0.11) *** | −0.32 (0.18) | −0.07 (0.03) * | −0.39 (0.18) * | 16.5 |
| Vitamin D (nmol/L) | −3.80 (0.84) *** | 0.01 (0.01) | −0.34 (0.18) | −0.05 (0.03) | −0.39 (0.18) * | - |
| Exposure: PD and Outcome: DSST | ||||||
|---|---|---|---|---|---|---|
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.21 (0.08) ** | −1.70 (0.30) *** | −3.23 (0.72) *** | −0.36 (0.16) * | −3.24 (0.72) *** | 11.0 |
| Vitamin D (nmol/L) | −6.24 (1.29) *** | 0.06 (0.02) *** | −3.64 (0.76) *** | −0.40 (0.15) * | −4.03 (0.76) *** | 9.3 |
| Exposure: AL and Outcome: DSST | ||||||
| Mediator | Exposure to Mediator | Mediator to Outcome | Direct Effect | Mediated (Indirect) Effect | Total Effect (Exposure to Outcome) | Proportion Mediated (%) |
| DII | 0.14 (0.05) ** | −1.69 (0.30) *** | −2.33 (0.48) *** | −0.24 (0.10) * | −2.57 (0.48) *** | 9.2 |
| Vitamin D (nmol/L) | −3.80 (0.84) *** | 0.06 (0.02) *** | −2.56 (0.50) *** | −0.24 (0.09) * | −2.80 (0.49) *** | 8.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botelho, J.; Leira, Y.; Viana, J.; Machado, V.; Lyra, P.; Aldrey, J.M.; Pías-Peleteiro, J.M.; Blanco, J.; Sobrino, T.; Mendes, J.J. The Role of Inflammatory Diet and Vitamin D on the Link between Periodontitis and Cognitive Function: A Mediation Analysis in Older Adults. Nutrients 2021, 13, 924. https://doi.org/10.3390/nu13030924
Botelho J, Leira Y, Viana J, Machado V, Lyra P, Aldrey JM, Pías-Peleteiro JM, Blanco J, Sobrino T, Mendes JJ. The Role of Inflammatory Diet and Vitamin D on the Link between Periodontitis and Cognitive Function: A Mediation Analysis in Older Adults. Nutrients. 2021; 13(3):924. https://doi.org/10.3390/nu13030924
Chicago/Turabian StyleBotelho, João, Yago Leira, João Viana, Vanessa Machado, Patrícia Lyra, José Manuel Aldrey, Juan Manuel Pías-Peleteiro, Juan Blanco, Tomás Sobrino, and José João Mendes. 2021. "The Role of Inflammatory Diet and Vitamin D on the Link between Periodontitis and Cognitive Function: A Mediation Analysis in Older Adults" Nutrients 13, no. 3: 924. https://doi.org/10.3390/nu13030924