The Impact of Retrospective Childhood Maltreatment on Eating Disorders as Mediated by Food Addiction: A Cross-Sectional Study

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
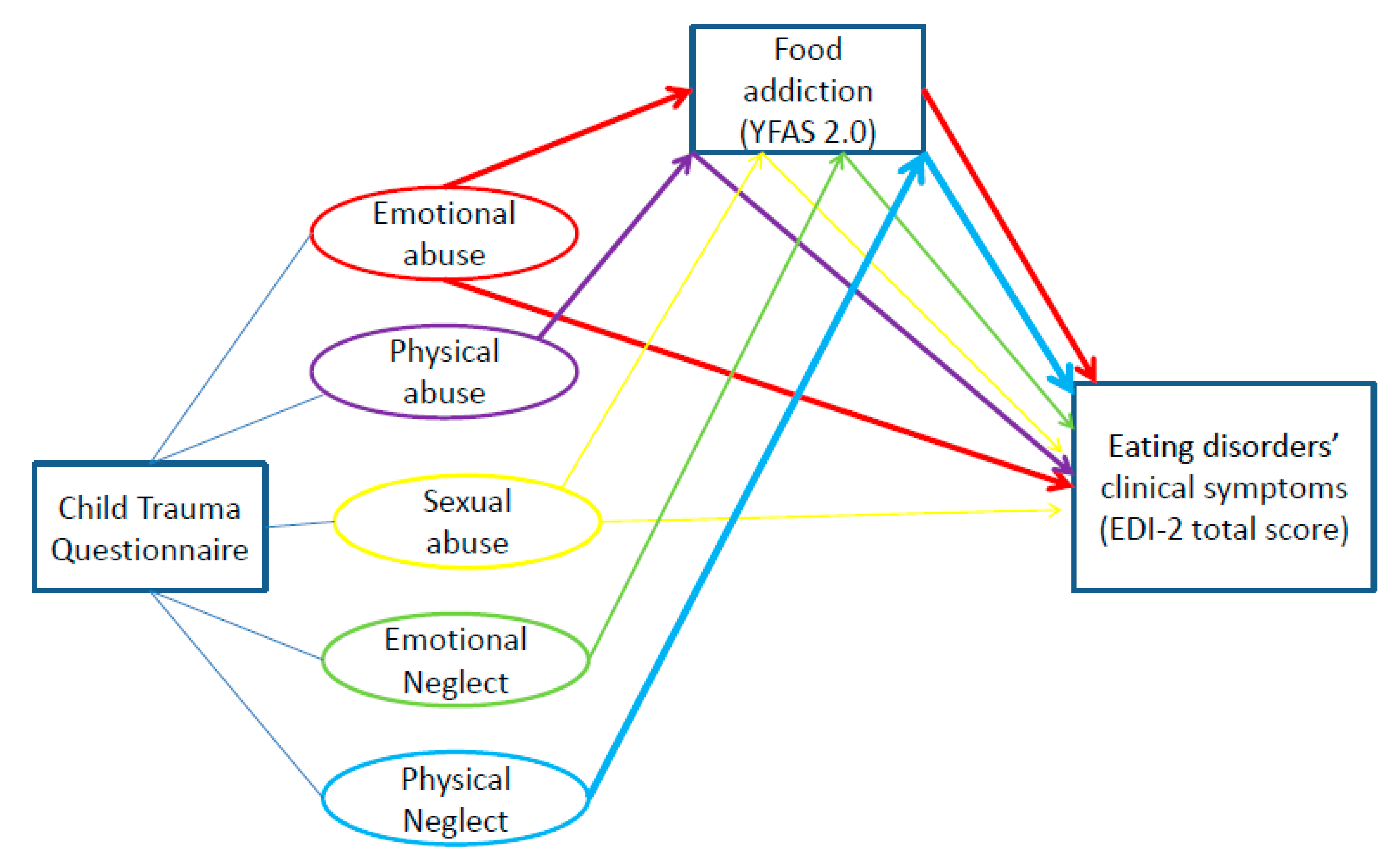
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Child Maltreatment. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment#:~:text=Child%20maltreatment%20is%20the%20abuse,under%2018%20years%20of%20age (accessed on 16 September 2020).
- Treasure, J.; Claudino, A.M.; Zucker, N. Eating disorders. Lancet 2010, 375, 583–593. [Google Scholar] [CrossRef]
- Caslini, M.; Bartoli, F.; Crocamo, C.; Dakanalis, A.; Clerici, M.; Carrà, G. Disentangling the association between child abuse and eating disorders: A systematic review and meta-analysis. Psychosom. Med. 2016, 78, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Molendijk, M.L.; Hoek, H.W.; Brewerton, T.D.; Elzinga, B.M. Childhood maltreatment and eating disorder pathology: A systematic review and dose-response meta-analysis. Psychol. Med. 2017, 47, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Guillaume, S.; Jaussent, I.; Maimoun, L.; Ryst, A.; Seneque, M.; Villain, L.; Hamroun, D.; Lefebvre, P.; Renard, E.; Courtet, P. Associations between adverse childhood experiences and clinical characteristics of eating disorders. Sci. Rep. 2016, 6, 3576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rijkers, C.; Schoorl, M.; van Hoeken, D.; Hoek, H.W. Eating disorders and posttraumatic stress disorder. Curr. Opin. Psychiatry 2019, 32, 510–517. [Google Scholar] [CrossRef]
- Racine, S.E.; Wildes, J.E. Emotion dysregulation and anorexia nervosa: An exploration of the role of childhood abuse. Intern. J. Eat. Dis. 2015, 48, 55–58. [Google Scholar] [CrossRef]
- Rai, T.; Mainali, P.; Raza, A.; Rashid, J.; Rutkofsky, I. Exploring the link between emotional child abuse and anorexia nervosa: A psychopathological correlation. Cureus 2019, 11, e5318. [Google Scholar] [CrossRef] [Green Version]
- Kong, S.; Bernstein, K. Childhood trauma as a predictor of eating psychopathology and its mediating variables in patients with eating disorders. J. Clin. Nurs. 2009, 18, 1897–1907. [Google Scholar] [CrossRef]
- Brewerton, T.D. Food addiction as a proxy for eating disorder and obesity severity, trauma history, PTSD symptoms, and comorbidity. Eat. Weight Disord. 2017, 22, 241–247. [Google Scholar] [CrossRef]
- Gordon, E.L.; Ariel-Donges, A.H.; Bauman, V.; Merlo, L.J. What is the evidence for ‘food addiction?’ A systematic review. Nutrients 2018, 10, 477. [Google Scholar] [CrossRef] [Green Version]
- Fauconnier, M.; Rousselet, M.; Brunault, P.; Thiabaud, E.; Lambert, S.; Rocher, B.; Challet-Bouju, G.; Grall-Bronnec, M. Food addiction among female patients seeking treatment for an eating disorder: Prevalence and associated factors. Nutrients 2020, 12, 1897. [Google Scholar] [CrossRef] [PubMed]
- Mason, S.M.; Flint, A.J.; Roberts, A.L.; Agnew-Blais, J.; Koenen, K.C.; Rich-Edwards, J.W. Posttraumatic stress disorder symptoms and food addiction in women by timing and type of trauma exposure. JAMA Psychiatry 2014, 71, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.; Steward, T.; Agüera, Z.; Mestre-Bach, G.; Magaña, P.; Granero, R.; Jiménez-Murcia, S.; Claes, L.; Gearhardt, A.N.; Menchón, J.M.; et al. Associations of food addiction and nonsuicidal self-injury among women with an eating disorder: A common strategy for regulating emotions? Eur. Eat. Disord. Rev. 2018, 26, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Hardy, R.; Fani, N.; Jovanovic, T.; Michopoulos, V. Food addiction and substance addiction in women: Common clinical characteristics. Appetite 2018, 120, 367–373. [Google Scholar] [CrossRef]
- Elton, A.; Smitherman, S.; Young, J.; Kilts, C.D. Effects of childhood maltreatment on the neural correlates of stress- and drug cue-induced cocaine craving. Addict. Biol. 2015, 20, 820–831. [Google Scholar] [CrossRef] [Green Version]
- Van Dam, N.T.; Rando, K.; Potenza, M.N.; Tuit, K.; Sinha, R. Childhood maltreatment, altered limbic neurobiology, and substance use relapse severity via trauma-specific reductions in limbic gray matter volume. JAMA Psychiatry 2014, 71, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M.; Olmstead, M.P.; Polivy, J. Development and validation of a multidimensional eating disorder inventory for anorexia nervosa and bulimia. Intern. J. Eat. Disord. 1983, 2, 15–34. [Google Scholar] [CrossRef]
- Criquillion-Doublet, S.; Divac, S.; Dardennes, R.; Guelfi, J. Le ‘Eating Disorder Inventory’ (EDI); Guelfi, J.D., Gaillac, V., Dardennes, R., Eds.; Psychopathologie Quantitative: Paris, Franch, 1995. [Google Scholar]
- Steward, T.; Mestre-Bach, G.; Agüera, Z.; Granero, R.; Martín-Romera, V.; Sánchez, I.; Riesco, N.; Tolosa-Sola, I.; Fernández-Formoso, J.A.; Fernández-García, J.C.; et al. Enduring changes in decision making in patients with full remission from anorexia nervosa. Eur. Eat. Disord. Rev. 2016, 24, 523–527. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Development of the yale food addiction scale Version 2.0. Psychol. Addict. Behav. 2016, 30, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Brunault, P.; Ballon, N.; Gaillard, P.; Réveillère, C.; Courtois, R. Validation of the French version of the yale food addiction scale: An examination of its factor structure, reliability, and construct validity in a nonclinical sample. Can. J. Psychiatry 2014, 59, 276–284. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, D.P.; Fink, L. Childhood Trauma Questionnaire: A Retrospective Self-Report; Psychological Corporation: Orlando, FL, USA, 1998. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis; Guildford Press: New York, NY, USA, 2013. [Google Scholar]
- Imperatori, C.; Innamorati, M.; Lamis, D.A.; Farina, B.; Pompili, M.; Contardi, A.; Fabbricatore, M. Childhood trauma in obese and overweight women with food addiction and clinical-level of binge eating. Child. Abuse. Negl. 2016, 58, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Stojek, M.M.; Maples-Keller, J.L.; Dixon, H.D.; Umpierrez, G.E.; Gillespie, C.F.; Michopoulos, V. Associations of childhood trauma with food addiction and insulin resistance in African-American women with diabetes mellitus. Appetite 2019, 141, 104317. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R. Role of addiction and stress neurobiology on food intake and obesity. Biol. Psychol. 2018, 131, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Pursey, K.M.; Stanwell, P.; Gearhardt, A.N.; Collins, C.E.; Burrows, T.L. The prevalence of food addiction as assessed by the Yale Food Addiction Scale: A systematic review. Nutrients 2014, 6, 4552–4590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiss, D.A.; Brewerton, T.D. Incorporating food addiction into disordered eating: The disordered eating food addiction nutrition guide (DEFANG). Eat. Weight Disord. 2017, 22, 49–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meule, A.; von Rezori, V.; Blechert, J. Food addiction and bulimia nervosa. Eur. Eat. Disord. Rev. 2014, 22, 331–337. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.K.; Meule, A. Food addiction and bulimia nervosa: New data based on the yale food addiction scale 2.0. Eur. Eat. Disord. Rev. 2016, 24, 518–522. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Murcia, S.; Agüera, Z.; Paslakis, G.; Munguia, L.; Granero, R.; Sánchez-González, J.; Sánchez, I.; Riesco, N.; Gearhardt, A.N.; Dieguez, C.; et al. Food addiction in eating disorders and obesity: Analysis of clusters and implications for treatment. Nutrients 2019, 11, 2633. [Google Scholar] [CrossRef] [Green Version]
- Loxton, N.J.; Tipman, R.J. Reward sensitivity and food addiction in women. Appetite 2017, 115, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Beyer, F.; García-García, I.; Heinrich, M.; Schroeter, M.L.; Sacher, J.; Luck, T.; Riedel-Heller, S.G.; Stumvoll, M.; Villringer, A.; Witte, A.V. Neuroanatomical correlates of food addiction symptoms and body mass index in the general population. Hum. Brain. Mapp. 2019, 40, 2747–2758. [Google Scholar] [CrossRef] [Green Version]
- Osadchiy, V.; Mayer, E.A.; Bhatt, R.; Labus, J.S.; Gao, L.; Kilpatrick, L.A.; Liu, C.; Tillisch, K.; Naliboff, B.; Chang, L.; et al. History of early life adversity is associated with increased food addiction and sex-specific alterations in reward network connectivity in obesity. Obes. Sci. Pract. 2019, 5, 416–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, K.S.; Wolf, E.J. PTSD, food addiction, and disordered eating in a sample of primarily older veterans: The mediating role of emotion regulation. Psychiatry Res. 2016, 243, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenzel, K.R.; Weinstock, J.; McGrath, A.B. The clinical significance of food addiction. J. Addict. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Kalon, E.; Hong, J.Y.; Tobin, C.; Schulte, T. Psychological and neurobiological correlates of food addiction. Int. Rev. Neurobiol. 2016, 129, 85–110. [Google Scholar] [PubMed] [Green Version]
- Mills, J.G.; Thomas, S.J.; Larkin, T.A.; Deng, C. Overeating and food addiction in Major Depressive Disorder: Links to peripheral dopamine. Appetite 2020, 148, 104586. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, A.M.; Cascino, G.; Pellegrino, F.; Ruzzi, V.; Patriciello, G.; Marone, L.; De Felice, G.; Monteleone, P.; Maj, M. The association between childhood maltreatment and eating disorder psychopathology: A mixed-model investigation. Eur. Psychiatry 2019, 61, 111–118. [Google Scholar] [CrossRef]
- Hazzard, V.M.; Bauer, K.W.; Mukherjee, B.; Miller, A.L.; Sonneville, K.R. Associations between childhood maltreatment latent classes and eating disorder symptoms in a nationally representative sample of young adults in the United States. Child Abuse. Negl. 2019, 98, 104171. [Google Scholar] [CrossRef]
- Burns, E.E.; Fischer, S.; Jackson, J.L.; Harding, H.G. Deficits in emotion regulation mediate the relationship between childhood abuse and later eating disorder symptoms. Child Abuse. Negl. 2012, 36, 32–39. [Google Scholar] [CrossRef]
- Grilo, C.M.; Masheb, R.M. Childhood maltreatment and personality disorders in adult patients with binge eating disorder. Acta. Psychiatr. Scand. 2002, 106, 183–188. [Google Scholar] [CrossRef]
- Zeanah, C.H.; Humphreys, K.L. Child abuse and neglect. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 637–644. [Google Scholar] [CrossRef]
- Arain, M.; Haque, M.; Johal, L.; Mathur, P.; Nel, W.; Rais, A.; Sandhu, R.; Sharma, S. Maturation of the adolescent brain. Neuropsychiatr. Dis. Treat. 2013, 9, 449–461. [Google Scholar] [PubMed] [Green Version]
- Rodenburg, G.; Kremers, S.P.; Oenema, A.; van de Mheen, D. Associations of children’s appetitive traits with weight and dietary behaviours in the context of general parenting. PLoS ONE 2012, 7, e50642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks White, A.A.; Pratt, K.J.; Cottrill, C. The relationship between trauma and weight status among adolescents in eating disorder treatment. Appetite 2018, 129, 62–69. [Google Scholar] [CrossRef]
- Rodgers, R.F.; DuBois, R.; Thiebaut, S.; Jaussent, I.; Maimoun, L.; Seneque, M.; Lefebvre, P.; Renard, E.; Courtet, P.; Guillaume, S. Structural differences in eating disorder psychopathology after history of childhood abuse: Insights from a Bayesian network analysis. J. Abnorm. Psychol. 2019, 128, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.C.; Nickow, M.S.; Arseneau, R.; Gisslow, M.T. A substance called food: Long-term psychodynamic group treatment for compulsive overeating. Int. J. Group Psychother. 2015, 65, 386–409. [Google Scholar] [CrossRef]
- Valbrun, L.P.; Zvonarev, V. The opioid system and food intake: Use of opiate antagonists in treatment of binge eating disorder and abnormal eating behavior. J. Clin. Med. Res. 2020, 12, 41–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Category | Statistic | All Participants |
|---|---|---|---|
| N | 231 | ||
| Age (years) | Me (IQR) | 24 (19–33) | |
| Gender | Male | N (%) | 18 (7.8%) |
| Female | N (%) | 213 (92.2%) | |
| ED | Diagnosis of AN | N (%) | 142 (61.5%) |
| Diagnosis of BN | N (%) | 39 (16.9%) | |
| Diagnosis of BED | N (%) | 21 (9.1%) | |
| Other diagnosis | N (%) | 29 (12.5%) | |
| Current and/or past history of PTSD | N (%) | 33 (14.3%) | |
| BMI (kg/m²) | Current | Me (IQR) | 18.7 (16.8–21.5) |
| CTQ | Emotional abuse | Me (IQR) | 9 (6–13) |
| Physical abuse | Me (IQR) | 5 (5–7) | |
| Sexual abuse | Me (IQR) | 5 (5–7) | |
| Emotional neglect | Me (IQR) | 12 (8–16) | |
| Physical neglect | Me (IQR) | 7 (5–9) | |
| EDI-2 | Drive for thinness | Me (IQR) | 22 (17–28) |
| Bulimia | Me (IQR) | 15 (5–24) | |
| Body dissatisfaction | Me (IQR) | 21 (17–24) | |
| Ineffectiveness | Me (IQR) | 23 (20–27) | |
| Perfectionism | Me (IQR) | 18 (12–22) | |
| Interpersonal distrust | Me (IQR) | 18 (15–20) | |
| Interoceptive awareness | Me (IQR) | 28 (20–34) | |
| Maturity fears | Me (IQR) | 19 (16–22) | |
| Asceticism | Me (IQR) | 19 (13–24) | |
| Impulse regulation | Me (IQR) | 20 (13–28) | |
| Social insecurity | Me (IQR) | 18 (16–21) | |
| Total score | Me (IQR) | 220 (188–254) | |
| Variable | Category | Statistic | FA(−) Group | FA(+) Group | Test | p-Value |
|---|---|---|---|---|---|---|
| N | 77 | 154 | ||||
| Age (years) | Me (IQR) | 28 (19–34) | 27.84 (20–32) | U | 0.263 | |
| Gender | Male | N (%) | 7 (38.9%) | 11 (61.1%) | ||
| Female | N (%) | 70 (32.9%) | 143 (67.1%) | Chi² | 0.603 | |
| ED | Diagnosis of AN | N (%) | 50 (35.2%) | 92 (64. 8%) | Chi² | 0.339 |
| Diagnosis of BN | N (%) | 6 (15.4%) | 33 (84.6%) | Chi² | 0.012 | |
| Diagnosis of BED | N (%) | 5 (23.8%) | 16 (76.2%) | Chi² | 0.352 | |
| Other diagnosis | N (%) | 7 (50%) | 7 (50%) | Chi² | 0.172 | |
| Current and/or past history of PTSD | N (%) | 2 (7.7%) | 24 (92.3%) | Y | 0.006 | |
| BMI (kg/m²) | Current | Me (IQR) | 17.8 (16.1–19.9) | 20.97 (16.9–22.1) | U | 0.005 |
| FA(−) Group | FA(+) Group | Test | p-Value | ||
|---|---|---|---|---|---|
| N | 77 | 154 | |||
| Scale | Subscale | ||||
| CTQ | Emotional abuse | 7 (5–10) | 10 (7–14.25) | U | <0.001 |
| Physical abuse | 5 (5–5) | 5 (5–8) | U | 0.005 | |
| Sexual abuse | 5 (5–5) | 5 (5–8) | U | 0.014 | |
| Emotional neglect | 10 (7–13.75) | 13 (9–17) | U | 0.005 | |
| Physical neglect | 6 (5–8) | 7 (6–10) | U | 0.006 | |
| EDI-2 | Drive for thinness | 18 (2–22) | 25 (10–29) | U | <0.001 |
| Bulimia | 4 (0–14) | 19 (2–25) | U | <0.001 | |
| Body dissatisfaction | 18 (7–21) | 22 (13–25) | U | <0.001 | |
| Ineffectiveness | 21 (13–24) | 25 (17–29) | U | <0.001 | |
| Perfectionism | 15 (4–21) | 20 (7–23) | U | 0.001 | |
| Interpersonal distrust | 17 (11–20) | 18 (13–20) | U | 0.357 | |
| Interoceptive awareness | 21 (6–27) | 32 (17–36) | U | <0.001 | |
| Maturity fears | 17 (8–20) | 19 (13–23) | U | <0.001 | |
| Asceticism | 13 (3–18) | 21 (8–26) | U | <0.001 | |
| Impulse regulation | 13 (2–19) | 25 (10–30) | U | <0.001 | |
| Social insecurity | 20 (13–23) | 18 (13–20) | U | 0.001 |
| CTQ r (95% CI); p-Value | |||||
|---|---|---|---|---|---|
| Emotional Abuse | Physical Abuse | Sexual Abuse | Emotional Neglect | Physical Neglect | |
| YFAS | 0.314 | 0.246 | 0.16 | 0.208 | 0.307 |
| r (95% CI) | (0.19–0.428) | (0.12–0.365) | (0.028–0.286) | (0.079–0.331) | (0.183–0.421) |
| p-Value | <0.001 | <0.001 | 0.018 | 0.002 | <0.001 |
| 0.608 | |||||
| (0.519–0.684) | |||||
| <0.001 | |||||
| EDI-2 | 0.349 | 0.199 | 0.25 | 0.227 | 0.161 |
| r (95% CI) | (0.228–0.459) | (0.071–0.322) | (0.121–0.37) | (0.098–0.348) | (0.031–0.287) |
| p-Value | <0.001 | 0.003 | <0.001 | <0.001 | 0.016 |
| CTQ Subscales | ||||||
|---|---|---|---|---|---|---|
| Type of Effect | ||||||
| (CI); | ||||||
| p-Value | ||||||
| Emotional Abuse | Physical Abuse | Sexual Abuse | Emotional Neglect | Physical Neglect | ||
| Total effect | 3.401 | 2.433 | 2.934 | 2.24 | 2.944 | |
| (Direct and indirect) | (2.2–4.6) | (0.83–4.03) | (1.42–4.44) | (1–3.49) | (0.52–5.35) | |
| <0.001 | 0.003 | <0.001 | <0.001 | 0.017 | ||
| EDI-2 | ||||||
| total score | Direct effect | 1.64 | 0.543 | 1.809 | 0.947 | −0.873 |
| (0.6–2.68) | (−0.77–1.85) | (0.6–3.01) | (−0.07–1.96) | (−2.89–1.14) | ||
| 0.002 | 0.417 | 0.003 | 0.069 | 0.396 | ||
| Indirect effect | 1.761 | 1.89 | 1.125 | 1.303 | 3.817 | |
| (1–2.66) | (1.04–2.88) | (0.11–2.28) | (0.54–2.16) | (2.26–5.53) | ||
| Standardized indirect effect | 0.183 | 0.153 | 0.097 | 0.136 | 0.208 | |
| (0.1–0.26) | (0.08–0.22) | (0.01–0.18) | (0.05–0.21) | (0.12–0.29) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bou Khalil, R.; Sleilaty, G.; Richa, S.; Seneque, M.; Iceta, S.; Rodgers, R.; Alacreu-Crespo, A.; Maimoun, L.; Lefebvre, P.; Renard, E.; et al. The Impact of Retrospective Childhood Maltreatment on Eating Disorders as Mediated by Food Addiction: A Cross-Sectional Study. Nutrients 2020, 12, 2969. https://doi.org/10.3390/nu12102969
Bou Khalil R, Sleilaty G, Richa S, Seneque M, Iceta S, Rodgers R, Alacreu-Crespo A, Maimoun L, Lefebvre P, Renard E, et al. The Impact of Retrospective Childhood Maltreatment on Eating Disorders as Mediated by Food Addiction: A Cross-Sectional Study. Nutrients. 2020; 12(10):2969. https://doi.org/10.3390/nu12102969
Chicago/Turabian StyleBou Khalil, Rami, Ghassan Sleilaty, Sami Richa, Maude Seneque, Sylvain Iceta, Rachel Rodgers, Adrian Alacreu-Crespo, Laurent Maimoun, Patrick Lefebvre, Eric Renard, and et al. 2020. "The Impact of Retrospective Childhood Maltreatment on Eating Disorders as Mediated by Food Addiction: A Cross-Sectional Study" Nutrients 12, no. 10: 2969. https://doi.org/10.3390/nu12102969