Temporal Progression of Fatty Acids in Preterm and Term Human Milk of Mothers from Switzerland

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical and Legal Considerations
2.2. Study Settings and Subjects
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection
2.5. Human Milk Sampling, Handling, and Storage
2.6. Quantification of Total Lipids in Human Milk
2.7. Direct Method Procedure to Prepare Fatty Acid Methyl Esters (FAME) from Human Milk
2.8. Statistics
3. Results
3.1. Subject Characteristics
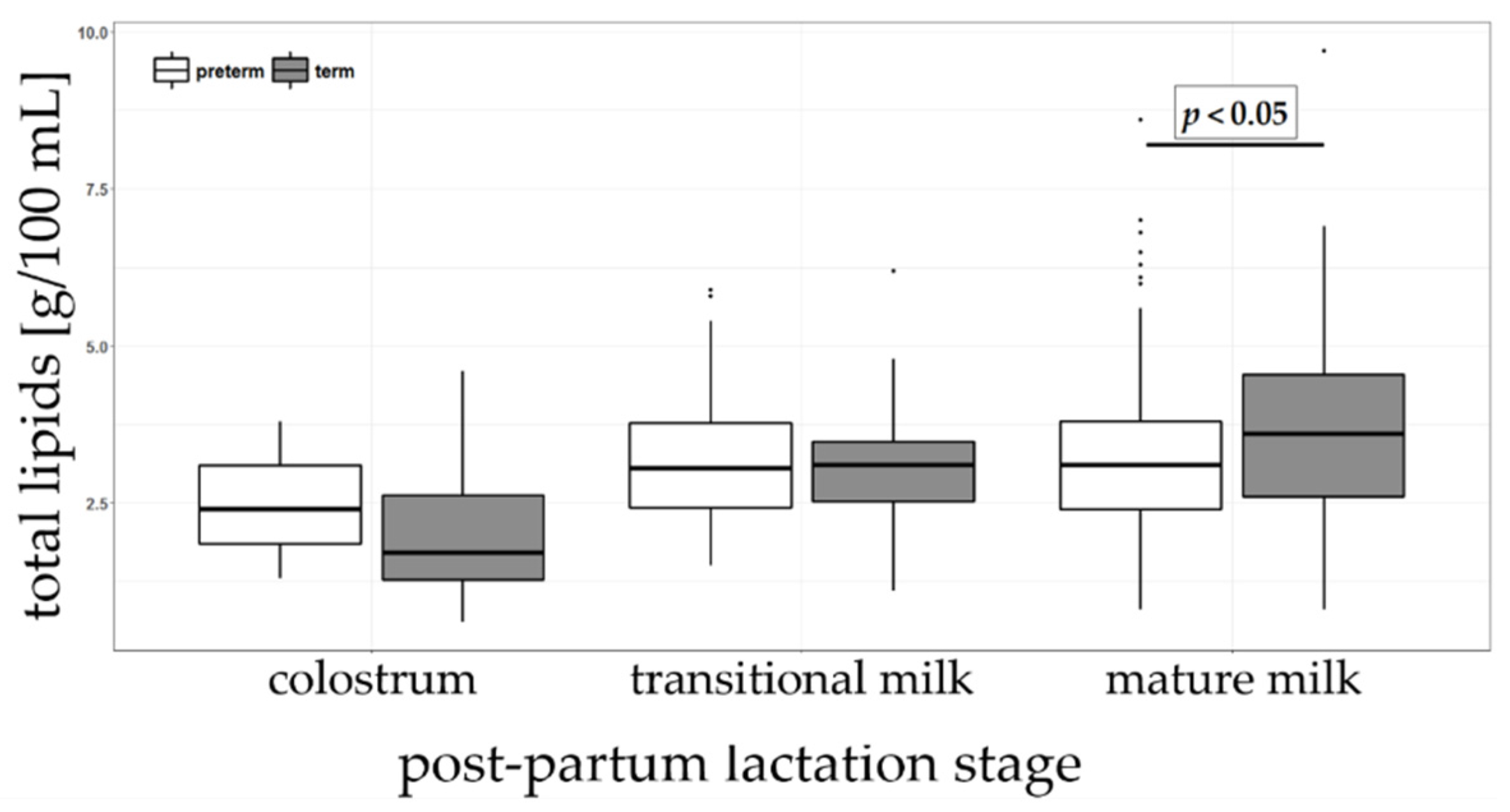
3.2. Total Lipids in Preterm and Term Human Milk
3.3. Fatty Acids in Preterm and Term Human Milk
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gartner, L.M.; Morton, J.; Lawrence, R.A.; Naylor, A.J.; O’Hare, D.; Schanler, R.J.; Eidelman, A.I. Breastfeeding and the use of human milk. Pediatrics 2005, 115, 496–506. [Google Scholar] [PubMed]
- Kramer, M.S.; Kakuma, R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst. Rev. 2012, CD003517. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Quigley, M.; Embleton, N.D.; McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2018, 6, CD002971. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, E.E. 3.14 Preterm and low-birth-weight infants. World Rev. Nutr. Diet 2015, 113, 214–217. [Google Scholar]
- Kumar, R.K.; Singhal, A.; Vaidya, U.; Banerjee, S.; Anwar, F.; Rao, S. Optimizing nutrition in preterm low birth weight infants—Consensus summary. Front. Nutr. 2017, 4, 20. [Google Scholar] [CrossRef]
- Heird, W.C.; Lapillonne, A. The role of essential fatty acids in development. Annu. Rev. Nutr. 2005, 25, 549–571. [Google Scholar] [CrossRef]
- Molloy, C.; Doyle, L.W.; Makrides, M.; Anderson, P.J. Docosahexaenoic acid and visual functioning in preterm infants: A review. Neuropsychol. Rev. 2012, 22, 425–437. [Google Scholar] [CrossRef]
- Schneider, N.; Garcia-Rodenas, C. Early nutritional interventions for brain and cognitive development in preterm infants: A review of the literature. Nutrients 2017, 9, 187. [Google Scholar] [CrossRef]
- Ziegler, E.E. Human milk and human milk fortifiers. World Rev. Nutr. Diet. 2014, 110, 215–227. [Google Scholar]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. Optimization of human milk fortification for preterm infants: New concepts and recommendations. J. Perinat. Med. 2010, 38, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Rochow, N.; Fusch, G.; Choi, A.; Chessell, L.; Elliott, L.; McDonald, K.; Kuiper, E.; Purcha, M.; Turner, S.; Chan, E.; et al. Target fortification of breast milk with fat, protein, and carbohydrates for preterm infants. J. Pediatr. 2013, 163, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Dror, D.K.; Allen, L.H. Overview of Nutrients in Human Milk. Adv. Nutr. 2018, 9 (Suppl.1), 278S–294S. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, S.K.; Giuffrida, F.; Cristina, C.H.; De Castro, C.A.; Mukherjee, R.; Tran, L.A.; Steenhout, P.; Lee, L.Y.; Destaillats, F. Dynamics of human milk nutrient composition of women from Singapore with a special focus on lipids. Am. J. Hum. Biol. 2013, 25, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Giuffrida, F.; Cruz-Hernandez, C.; Bertschy, E.; Fontannaz, P.; Masserey Elmelegy, I.; Tavazzi, I.; Marmet, C.; Sanchez-Bridge, B.; Thakkar, S.K.; De Castro, C.A.; et al. Temporal changes of human breast milk lipids of chinese mothers. Nutrients 2016, 8, 715. [Google Scholar] [CrossRef] [PubMed]
- Mimouni, F.B.; Lubetzky, R.; Yochpaz, S.; Mandel, D. Preterm human milk macronutrient and energy composition: A systematic review and meta-analysis. Clin. Perinatol. 2017, 44, 165–172. [Google Scholar] [CrossRef]
- Fields, D.A.; Schneider, C.R.; Pavela, G. A narrative review of the associations between six bioactive components in breast milk and infant adiposity. Obesity 2016, 24, 1213–1221. [Google Scholar] [CrossRef] [Green Version]
- Meier, P.; Patel, A.L.; Wright, K.; Engstrom, J.L. Management of breastfeeding during and after the maternity hospitalization for late preterm infants. Clin. Perinatol. 2013, 40, 689–705. [Google Scholar] [CrossRef]
- Berenhauser, A.C.; Pinheiro do Prado, A.C.; da Silva, R.C.; Gioielli, L.A.; Block, J.M. Fatty acid composition in preterm and term breast milk. Int. J. Food Sci. Nutr. 2012, 63, 318–325. [Google Scholar] [CrossRef]
- Granot, E.; Ishay-Gigi, K.; Malaach, L.; Flidel-Rimon, O. Is there a difference in breast milk fatty acid composition of mothers of preterm and term infants? J. Matern. Fetal Neonatal Med. 2016, 29, 832–835. [Google Scholar] [CrossRef]
- Bobinski, R.; Mikulska, M.; Mojska, H.; Simon, M. Comparison of the fatty acid composition of transitional and mature milk of mothers who delivered healthy full-term babies, preterm babies and full-term small for gestational age infants. Eur. J. Clin. Nutr. 2013, 67, 966–971. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Hernandez, C.; Goeuriot, S.; Giuffrida, F.; Thakkar, S.K.; Destaillats, F. Direct quantification of fatty acids in human milk by gas chromatography. J. Chromatogr. A 2013, 1284, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Giuffrida, F.; Austin, S.; Cuany, D.; Sanchez-Bridge, B.; Longet, K.; Bertschy, E.; Sauser, J.; Thakkar, S.K.; Lee, L.Y.; Affolter, M. Comparison of macronutrient content in human milk measured by mid-infrared human milk analyzer and reference methods. J. Perinatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B.; Rodriguez-Palmero, M. Polyunsaturated fatty acids in human milk and their role in early infant development. J. Mammary Gland Biol. Neoplasia 1999, 4, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Lapillonne, A. Enteral and parenteral lipid requirements of preterm infants. World Rev. Nutr. Diet. 2014, 110, 82–98. [Google Scholar] [PubMed]
- Bauer, J.; Gerss, J. Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants. Clin. Nutr. 2011, 30, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Narang, A.P.; Bains, H.S.; Kansal, S.; Singh, D. Serial composition of human milk in preterm and term mothers. Indian J. Clin. Biochem. 2006, 21, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.H.; Atkinson, S.A.; Bryan, M.H. Energy and macronutrient content of human milk during early lactation from mothers giving birth prematurely and at term. Am. J. Clin. Nutr. 1981, 34, 258–265. [Google Scholar] [CrossRef]
- Corvaglia, L.; Martini, S.; Aceti, A.; Capretti, M.G.; Galletti, S.; Faldella, G. Cardiorespiratory events with bolus versus continuous enteral feeding in healthy preterm infants. J. Pediatr. 2014, 165, 1255–1257. [Google Scholar] [CrossRef]
- Gross, S.J.; David, R.J.; Bauman, L.; Tomarelli, R.M. Nutritional composition of milk produced by mothers delivering preterm. J. Pediatr. 1980, 96, 641–644. [Google Scholar] [CrossRef]
- Molto-Puigmarti, C.; Castellote, A.I.; Carbonell-Estrany, X.; López-Sabater, M.C. Differences in fat content and fatty acid proportions among colostrum, transitional, and mature milk from women delivering very preterm, preterm, and term infants. Clin. Nutr. 2011, 30, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.; Chawla, D.; Kaur, J.; Jain, S. Macronutrients in breastmilk of mothers of preterm infants. Indian Pediatr. 2017, 54, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Saint, L.; Maggiore, P.; Hartmann, P.E. Yield and nutrient content of milk in eight women breast-feeding twins and one woman breast-feeding triplets. Br. J. Nutr. 1986, 56, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, R.S.; Luxwolda, M.F.; Dijck-Brouwer, D.J.; Muskiet, F.A. Fatty acid compositions of preterm and term colostrum, transitional and mature milks in a sub-Saharan population with high fish intakes. Prostaglandins Leukot. Essent. Fatty Acids 2012, 86, 201–207. [Google Scholar] [CrossRef]
- Kovacs, A.; Funke, S.; Marosvölgyi, T.; Burus, I.; Decsi, T. Fatty acids in early human milk after preterm and full-term delivery. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Luukkainen, P.; Salo, M.K.; Nikkari, T. The fatty acid composition of banked human milk and infant formulas: The choices of milk for feeding preterm infants. Eur. J. Pediatr. 1995, 154, 316–319. [Google Scholar] [CrossRef]
- Genzel-Boroviczeny, O.; Wahle, J.; Koletzko, B. Fatty acid composition of human milk during the 1st month after term and preterm delivery. Eur. J. Pediatr. 1997, 156, 142–147. [Google Scholar] [CrossRef]
- Rueda, R.; Ramírez, M.; García-Salmerón, J.L.; Maldonado, J.; Gil, A. Gestational age and origin of human milk influence total lipid and fatty acid contents. Ann. Nutr. Metab. 1998, 42, 12–22. [Google Scholar] [CrossRef]
- Sabel, K.G.; Lundqvist-Persson, C.; Bona, E.; Petzold, M.; Strandvik, B. Fatty acid patterns early after premature birth, simultaneously analysed in mothers’ food, breast milk and serum phospholipids of mothers and infants. Lipids Health Dis. 2009, 8, 20. [Google Scholar] [CrossRef]
- Francois, C.A.; Connor, S.L.; Wander, R.C.; Connor, W.E. Acute effects of dietary fatty acids on the fatty acids of human milk. Am. J. Clin. Nutr. 1998, 67, 301–308. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population | Preterm | Term | p-value |
|---|---|---|---|
| Maternal | n = 27 | n = 34 | |
| Age (years), mean ± SD | 32.4 ± 5.6 | 31.2 ± 4.2 | 0.3173 |
| Height (cm), mean ± SD | 165.2 ± 7.1 | 166.8 ± 6.6 | 0.3601 |
| Weight before pregnancy (kg), mean ± SD | 62.1 ± 9.5 | 64.3 ± 12.0 | 0.4479 |
| Weight at birth (kg), mean ± SD | 70.3 ± 10.6 | 74.5 ± 11.3 | 0.1426 |
| BMI before pregnancy (kg/m2), mean ± SD | 22.8 ± 3.4 | 23.2 ± 4.9 | 0.6990 |
| BMI at birth (kg/m2), mean ± SD | 25.8 ± 3.7 | 26.9 ± 4.7 | 0.3141 |
| Caesarean delivery, % | 63.0 | 23.5 | 0.0019 |
| Infant | n = 33 | n = 34 | |
| Gestational age at birth (weeks), mean ± SD | 30.8 ± 1.4 | 39.5 ± 1.0 | <0.0001 |
| Males, % | 54.5 | 52.9 | 0.8952 |
| Twins, % | 36.4 | 0.0 | 0.0001 |
| Height (cm), mean ± SD | 40.4 ± 3.2 | 49.4 ± 1.7 | <0.0001 |
| Weight (g), mean ± SD | 1421.4 ± 372.8 | 3277.6 ± 353.6 | <0.0001 |
| Head circumference (cm), mean ± SD | 27.8 ± 2.1 | 34.4 ± 1.5 | <0.0001 |
| Fatty Acids | Colostrum | Transitional Milk | Mature Milk | |||
|---|---|---|---|---|---|---|
| Preterm | Term | Preterm | Term | Preterm | Term | |
| total lipids (g/100 mL) | 2.40 (1.25) | 1.70 (1.35) | 3.05 (1.35) | 3.10 (0.95) | 3.10 c (1.40) | 3.60 c (1.95) |
| 8:0 (caprylic acid) | 0.08 a (0.08) | 0.03 a (0.05) | 0.20 (0.09) | 0.22 (0.04) | 0.21 (0.08) | 0.22 (0.06) |
| 10:0 (capric acid) | 0.60 a (0.44) | 0.29 a (0.3) | 1.58 (0.58) | 1.64 (0.47) | 1.48 (0.47) | 1.46 (0.38) |
| 12:0 (lauric acid) | 3.14 a (2.22) | 2.24 a (1.28) | 6.76 (2.41) | 6.33 (2.02) | 5.91 c (2.44) | 5.26 c (2.10) |
| 14:0 (myristic acid) | 6.20 (1.52) | 5.83 (1.77) | 7.86 (3.35) | 7.62 (1.8) | 7.36 c (2.9) | 6.27 c (1.93) |
| 16:0 (palmitic acid) | 24.02 (1.97) | 25.68 (2.83) | 22.75 (4.86) | 23.49 (3.11) | 23.10 (3.46) | 23.29 (3.31) |
| 16:1 n-7 (palmitoleic acid) | 2.34 (0.88) | 2.18 (0.51) | 1.96 (1.24) | 2.34 (0.74) | 2.17 c (0.82) | 2.44 c (0.77) |
| 18:0 (stearic acid) | 6.30 (1.55) | 6.79 (1.51) | 6.27 (1.86) | 6.23 (1.03) | 7.03 (2.06) | 6.75 (1.69) |
| 18:1 n-9 (oleic acid) | 37.64 (2.73) | 39.36 (3.02) | 34.62 (5.77) | 35.85 (4.06) | 35.22 c (5.16) | 37.67 c (4.82) |
| 18:1 n-7 (vaccenic acid) | 2.62 (0.62) | 2.67 (0.48) | 2.06 (0.44) | 2.13 (0.4) | 1.83 c (0.45) | 1.96 c (0.38) |
| 18:1 trans fatty acids | 0.70 (0.28) | 0.75 (0.19) | 0.68 (0.3) | 0.75 (0.31) | 0.71 c (0.42) | 0.82 c (0.36) |
| 18:2 n-6 (linoleic acid) | 9.61 (2.19) | 7.92 (1.17) | 9.55 b (2.98) | 8.70 b (2.23) | 10.21 c (3.64) | 9.35 c (2.90) |
| 18:3 n-3 (α-linolenic acid) | 0.77 a (0.25) | 0.51 a (0.15) | 0.72 (0.28) | 0.67 (0.26) | 0.75 (0.43) | 0.74 (0.30) |
| 18:3 n-6 (γ-linolenic acid) | 0.03 (0.02) | 0.03 (0.02) | 0.05 (0.03) | 0.08 (0.04) | 0.09 (0.04) | 0.10 (0.06) |
| 20:0 (arachidic acid) | 0.21 a (0.05) | 0.27 a (0.09) | 0.20 (0.06) | 0.21 (0.04) | 0.20 (0.07) | 0.20 (0.04) |
| 20:1 n-9 (eicosenoic acid) | 0.76 (0.23) | 0.99 (0.20) | 0.60 b (0.17) | 0.54 b (0.09) | 0.47 (0.14) | 0.45 (0.12) |
| 20:2 n-6 (eicosadienoic acid) | 0.52 (0.22) | 0.58 (0.16) | 0.42 b (0.12) | 0.34 b (0.06) | 0.29 (0.12) | 0.26 (0.07) |
| 20:3 n-6 (dihomo-γ-linolenic acid) | 0.51 a (0.17) | 0.66 a (0.35) | 0.41 (0.10) | 0.48 (0.18) | 0.35 (0.12) | 0.38 (0.13) |
| 20:5 n-3 (EPA) | 0.07 (0.07) | 0.07 (0.03) | 0.06 (0.05) | 0.07 (0.03) | 0.06 (0.04) | 0.06 (0.04) |
| 22:1 n-9 (erucic acid) | 0.19 a (0.06) | 0.25 a (0.06) | 0.12 (0.06) | 0.12 (0.02) | 0.09 (0.03) | 0.08 (0.03) |
| 20:4 n-6 (ARA) | 0.71 (0.36) | 0.78 (0.32) | 0.55 (0.19) | 0.53 (0.11) | 0.40 (0.12) | 0.42 (0.12) |
| 24:0 (lignoceric acid) | 0.19 (0.05) | 0.23 (0.1) | 0.14 (0.05) | 0.12 (0.04) | 0.08 (0.04) | 0.08 (0.03) |
| 24:1 n-9 (nervonic acid) | 0.30 a (0.09) | 0.39 a (0.14) | 0.13 (0.09) | 0.13 (0.03) | 0.07 (0.04) | 0.07 (0.03) |
| 22:6 n-3 (DHA) | 0.61 (0.41) | 0.64 (0.28) | 0.35 (0.19) | 0.42 (0.15) | 0.27 (0.16) | 0.28 (0.17) |
| Sum SFA | 43.49 (7.03) | 42.03 (2.84) | 47.14(7.76) | 46.08 (6.37) | 45.88 c (7.45) | 43.86 c (5.93) |
| Sum MUFA | 44.59 (2.90) | 46.51 (3.72) | 40.65 (6.19) | 42.12 (4.88) | 40.44 c (5.6) | 43.84 c (4.96) |
| Sum MCFA (< 14:0) | 3.95 a (2.52) | 2.51 a (1.65) | 8.52 (2.67) | 7.93 (2.66) | 7.63 c (2.89) | 6.94 c (2.38) |
| Sum PUFA | 12.90 (2.95) | 11.33 (1.95) | 12.19 (3.05) | 11.29 (2.03) | 12.76 (4.00) | 11.77 (3.43) |
| Sum PUFA n-3 | 1.48 (0.91) | 1.16 (0.36) | 1.24 (0.54) | 1.15 (0.23) | 1.15 (0.62) | 1.11 (0.36) |
| Sum PUFA n-6 | 10.16 (2.68) | 9.92 (1.66) | 10.88 (2.96) | 10.20 (2.22) | 11.37 (3.82) | 10.61 (3.17) |
| n-6 to n-3 ratio | 7.29 (2.49) | 8.67 (2.24) | 8.68 (4.56) | 8.58 (1.93) | 9.72 (4.94) | 9.58 (3.31) |
| ARA to DHA ratio | 1.36 a (0.71) | 1.40 a (0.53) | 1.52 (0.59) | 1.40 (0.41) | 1.77 (1.15) | 1.51 (0.68) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thakkar, S.K.; De Castro, C.A.; Beauport, L.; Tolsa, J.-F.; Fischer Fumeaux, C.J.; Affolter, M.; Giuffrida, F. Temporal Progression of Fatty Acids in Preterm and Term Human Milk of Mothers from Switzerland. Nutrients 2019, 11, 112. https://doi.org/10.3390/nu11010112
Thakkar SK, De Castro CA, Beauport L, Tolsa J-F, Fischer Fumeaux CJ, Affolter M, Giuffrida F. Temporal Progression of Fatty Acids in Preterm and Term Human Milk of Mothers from Switzerland. Nutrients. 2019; 11(1):112. https://doi.org/10.3390/nu11010112
Chicago/Turabian StyleThakkar, Sagar K., Carlos Antonio De Castro, Lydie Beauport, Jean-François Tolsa, Céline J. Fischer Fumeaux, Michael Affolter, and Francesca Giuffrida. 2019. "Temporal Progression of Fatty Acids in Preterm and Term Human Milk of Mothers from Switzerland" Nutrients 11, no. 1: 112. https://doi.org/10.3390/nu11010112