1. Introduction
The use of active transport modes (walking and cycling) has multiple benefits to health and the environment by contributing to increased physical activity (PA) levels [
1], reducing air and noise pollution (e.g., CO
2 emissions), and alleviating congestion problems [
2,
3]. Walking and cycling are considered the most sustainable and accessible modes for any journey from A to B [
3]. The use and promotion of active transportation, such as walking and cycling, has been scientifically proven to play a pivotal role in directly influencing global sustainable development goals. These sustainable development goals include the following [
4]:
Reducing air pollution (Sustainable Development Goals, SDG 3) and providing access to sustainable urban transport for all citizens (SDG 11).
Beyond their direct impact on these critical sustainable development goals, active transportation modes deliver a cascade of additional indirect benefits. These benefits encompass improved access to health and education (SDG 4), reduced inequality (SDG 10), enhanced gender inclusion (SDG 5), and support for poverty reduction strategies (SDG 1).
Land use and transport policies wield parallel influences on both human health and environmental sustainability [
5]. PA helps with reducing the prevalence of chronic diseases, improving mental health, reducing the rates of cognitive decline, and consequently reducing overall mortality rates [
6,
7,
8,
9]. Active transport and walking in particular are feasible for many people [
10]. The use of active transportation benefits health and transportation sciences as they are a convenient and accessible way to increase PA levels. For example, achieving the recommended dose of PA by walking and cycling has proven to have significant health effects [
11,
12]. In general, adults should perform at least 150–300 min of moderate-intensity PA [
13]. While the health benefits of PA are well documented, approximately 28% of adults (18–64) do not reach the World Health Organization’s (WHO) recommended PA levels [
13]. The WHO advocates for the use of non-motorised transport modes such as walking and cycling, as they can reduce health risks and mortality levels by increasing PA levels [
13,
14].
Moreover, the transport sector’s heavy reliance on fossil fuels, particularly in Europe, poses a significant challenge to meeting international sustainable policies for climate change. Despite the slow transition to alternative fuels, there is a growing consensus that promoting active travel, such as walking and cycling, holds promise in mitigating carbon emissions, emphasizing its importance over relying solely on technological substitution [
3].
Owing to the aforementioned benefits, the promotion of walking and cycling for travel purposes or active transportation has become an integral part of global and regional level policies; e.g., European Green Deal [
15], Transport, Health, and Environment Pan-European Programme (THE PEP) [
16], and Sustainable Mobility for all (SuM4all) [
17]. Therefore, research on the identification and evaluation of interventions to increase PA via active transport is necessary. Theory-based interventions (e.g., Transtheoretical Model, Social Cognitive Theory, Protection Motivation Theory) to promote PA have a strong evidence base in the medical and public health domain [
18,
19]. The application of theory-based intervention to promote active transport is limited by comparison [
20]. Additionally, to develop customised strategies for enhancing health through active transportation, it is essential to initially comprehend the motivating factors behind individuals’ engagement in active transport. A viable approach involves employing well-established social psychological models to measure people’s readiness to embrace this concept. One such model that is extensively used in exploring the willingness to change is the Transtheoretical Model (TTM) [
21,
22,
23]. This research aims to explore the utility of the TTM in an attempt to measure the readiness of individuals to change, or to be more specific, their readiness to increase PA levels through active transport use. The TTM has been most popular within the realm of health-related and addictive behaviours such as exercise, smoking cessation, and alcohol and drug use behaviour research [
24,
25,
26,
27]. Limited exploration of the model’s applicability in the area of transport [
28], and specifically active transport [
20,
29], is available.
1.1. Overview of Transtheoretical Model
Prochaska and DiClemente’s (1983) TTM of behaviour change is one of the most popular and widely used stage models in health research [
30,
31,
32]. The TTM denotes the following: (1) single behavioural theory is insufficient to comprehend the complexity of behaviour change processes, (2) the process of behaviour change unwinds through different stages over time, (3) the stages of change are stable and welcoming to change, and (4) the efficacy of behaviour change can be augmented by exploiting specific change processes and techniques to specific stages [
33,
34].
The stage theory is an essential part of the TTM. It is based on the idea that individuals undergo behaviour change as they advance through a defined sequence of stages [
22,
35]. The TTM typically consists of five stages: pre-contemplation (where individuals perceive the consequences of their behaviour as insignificant or remain unaware of any problem), contemplation (where people recognize the benefits of behavioural change but view the cost of change as high thus leading to apprehension), preparation (where individuals decide to change in the future and start taking small steps towards that goal), action (where individuals actively engage in changing their current behaviour or adopting the desired behaviour), and maintenance (where behavioural change is established and sustained over time) [
22,
36,
37,
38]. The TTM conceptualizes behaviour change within a temporal framework, suggesting that individuals undergo progression over time [
39]. It is acknowledged that individuals may go through multiple cycles across the stages before attaining lasting behavioural changes. Consequently, the TTM offers a structured approach for designing personalized interventions tailored to individuals at various stages [
34].
Advancement through the stages of change (SOCs) is shaped by key mediators of change, which are conceptual frameworks including decisional balance (DB), self-efficacy, and processes of change (POCs) [
40]. DB refers to an individual’s assessment of the advantages and disadvantages associated with choosing to adopt a particular behaviour or not [
40]. Studies have consistently shown predictable relationships between the pros and cons across DB stages [
22,
41,
42,
43]. To elaborate, individuals in the pre-contemplation stage typically lean towards recognizing the drawbacks or negative aspects of behaviour change. In contrast, those in the action or maintenance stages tend to perceive the advantages as outweighing the disadvantages [
22]. This evolution in decisional balance underscores the dynamic nature of one’s perception as they progress through the stages of change, reflecting a shifting emphasis on either the challenges or benefits associated with behaviour modification. Understanding these nuanced shifts in decisional balance is crucial for tailoring effective interventions that align with individuals’ specific needs and stages in the change process [
22].
Self-efficacy refers to an individual’s confidence in their capability to execute actions leading to a specific level of performance [
22,
40]. Examination across different stages, from preparation to maintenance, indicates a general trend of increasing self-efficacy [
22,
34,
44]. Consistent patterns have been observed in the relationship between the stages of the Transtheoretical Model (TTM) and its mediators, such as DB and self-efficacy, across various behaviours [
40,
41,
45].
Finally, the ten Processes of Change (POCs) encompass both covert and overt activities employed by individuals to advance through the stages of change. These activities are further categorised into experiential processes and behavioural processes. Experiential POCs are focused on acquiring knowledge through personal experiences, primarily applied during early-stage transitions. Examples of experiential processes include consciousness-raising, dramatic relief, self-re-evaluation, environmental re-evaluation, and social liberation.
On the other hand, behavioural processes are deployed during later-stage transitions, involving individuals actively engaging in specific actions to modify their behaviour. Key behavioural processes comprise self-liberation, establishing helpful relationships, counterconditioning, reinforcement management, and stimulus control. These processes collectively contribute to the dynamic and multifaceted nature of the change journey, addressing different aspects of personal development and behavioural modification [
39,
40].
1.2. Criticism Related to the Transtheoretical Model
Like other social-psychological models, TTM is not free from criticism. A few important criticisms include limited clarity and consistency of factors influencing the transitions between stages. However, the important critic of TTM is about the SOCs and their measurement. It was criticized that the SOCs are quite discrete and arbitrary [
28,
46]. In response to this criticism, Velicer and Prochaska described the stages as periods of temporal stability [
22]. They have drawn the similarity between the concept of distinct stages and punctuated equilibrium models of evolution used in natural sciences. These models allude to extended intervals of stability or equilibrium interrupted by shorter episodes of imbalance or change [
47]. In a similar pattern, stages such as pre-contemplation, contemplation, and maintenance present longer periods of equilibrium which are punctuated by disequilibria or change [
47]. However, in real life, an individual categorised in one stage is capable of having feelings and thoughts from other stages. For example, a subject may achieve high scores in multiple stages at the same time. This is why multidimensional or continuous scale measures (e.g., University of Rhode Island Change Assessment, URICA, URICA for exercise, URICA-E2) were developed to capture the continuity of motivations to perform certain behaviours across all stages [
35]. A higher total score indicates that an individual has a higher readiness to change (RTC) [
48]. RTC is determined by subtracting the scores of the pre-contemplation subscale from the sum of the contemplation, action, and maintenance subscales. Alternatively, the staging algorithms provide less insight into the underlying psychological determinants of behaviour as the scale is simplified. On the other hand, the tool adheres to the original conceptualization of the TTM and its discrete stages. The majority of the studies in the travel behaviour domain have utilised the staging algorithms, and the utility of the multidimensional scale measure is lacking [
45,
49,
50].
1.3. Study Aims
The innovation of this study lies in its pioneering effort to address a significant gap in the existing literature on the use of active transport modes. While prior studies have predominantly focused on isolated aspects of the Transtheoretical Model (TTM) when examining interventions related to active transport use, this research takes a step forward. It not only fills the void in the limited number of studies exploring the motivational mechanisms defined by TTM in the context of active transport use but goes beyond by comprehensively examining multiple constructs inherent to the model and the relationships between the constructs are also evaluated. For example, the majority of the studies that exist utilise either POCs or SOCs or a combination of both and it is rare to use outcome measures that relate these constructs as defined in TTM [
28]. The current study, however, tests the relationship between the three constructs of TTM including SOCs, DB (perception of pros and cons), and self-efficacy and with the use of active transportation. In this study, the overarching goal is to empirically examine the Transtheoretical Model’s (TTM) assumptions and assess its prospective utility in highlighting the motivational mechanisms underpinning the use of active transport modes. The following aims based on primary assumptions of the TTM are investigated:
If the continuous measure of stages of change can identify the five stages of change measuring the readiness to change in the use of active transport modes to increase PA.
Determining whether the DB (i.e., pros of the behaviour outweigh the cons of the behaviour) and self-efficacy increase as respondents progress through the stages (SOCs).
Determining whether stages of change, self-efficacy, and DB also progress with the increase in self-reported use of active transport modes.
2. Research Methodology
To test readiness to change in relation to increased active transport modes in a student population, this study uses three TTM measurement instruments, namely: the URICA scale, the DB scale [
51], and the Situational Confidence Questionnaire (SCQ) to measure self-efficacy [
52]. Two important criteria for participation included that participants must be above the age of 18 and physically able to carry out trips to and from work/school/shopping. Moreover, as the behaviour explored in the current study relates to the use of active transport, only people capable of unassisted mobility were included. A convenience sample was collected by contacting the students and staff of Hasselt University, Belgium. The population of Hasselt University comprises nearly 7500 students aged 18–35 and a faculty of 1400 individuals spanning the age range of 30–65. After initial analysis and data cleaning, the usable obtained count of responses was 260 from a total of 314. Only complete cases for TTM constructs measures were kept as required for analysis.
The standard questionnaires of TTM constructs (i.e., URICA, DB scale, and SCQ) were back-translated into the Netherlands language. Afterwards, a survey (
Appendix A) consisting of the TTM constructs (40 survey items) and sociodemographic questionnaires (10 survey items) was prepared in the online software program Qualtrics 2019. The sociodemographic information consisted of key personal factors such as age, education level, gender, etc. (
Appendix A). In addition, questions measuring the duration spent on the use of active transport modes (minutes per week) were incorporated, together with other transport modes choice-related questions. A summary of the sociodemographic and transport modes choice-related questions is provided in
Section 4.1. The online link was disseminated through the administration staff of Hasselt University to the students and staff via email. One week later a reminder email was sent. The data collection period continued for 3 weeks after which the survey was disabled. This study was approved by the social ethics committee Sociaal-Maatschappelijke Ethische Commissie (SMEC) of Hasselt University (REC/SMEC/VRAI/189/122).
2.1. Measures
The standard measures were adapted from the previous studies for all three TTM constructs (i.e., SOCs, DB scale, SCQ) used in the current study and are explained in the following sections.
2.1.1. SOCs Measure
URICA is a continuous scale measure to capture the SOCs or readiness to change of individuals. At first, it was proposed by McConnaughy, Prochaska, and Velicer (1983) and consisted of 32 items [
53]. This instrument has been characterized as user-friendly and does not necessitate training beforehand for its administration [
48]. The URICA has proven effective in assessing outcomes and variables related to various health and addictive behaviours, as evidenced in previous studies [
48,
54,
55]). However, various subscales developed for specific behaviours were developed as well (e.g., REFs. Relevant to our aim, for instance, is the URICA-E2. URICA-E2 was developed by Reed (1995) as a 24-item scale measure to capture continuous SOCs for exercise behaviour [
35,
56] and is downloadable from the website of the University of Rhode Island Cancer Prevention Research Centre [
57]. The URICA-E2 instrument was selected because of its established reliability across various TTM studies [
56,
58,
59,
60]. This particular version of the URICA measures all the stages of the TTM, including pre-contemplation non-believers (PCNB), pre-contemplation believers (PCB), and Contemplation, Preparation, Action, and Maintenance. For the current study, the URICA-E2 was adapted for active transport mode use. The adapted version of URICA-E2 for the use of active transport is provided in
Appendix A. The questionnaire itself is a 24-item continuous measure with a 5-point scale, with 1 for ‘strongly disagree’ and 5 for ‘strongly agree’. The participants were required to indicate the responses that they believed to match their feelings towards a particular statement.
2.1.2. Decisional Balance Scale
A scale designed by Nigg et al. (1998) to gauge Decisional Balance (DB) for Physical Activity (PA) behaviour was adapted for the present study [
51]. This 10-item measure is utilised to evaluate the perceived advantages (pros) and disadvantages (cons) by an individual when considering increasing their PA levels through active transport. The identification of pros and cons related to the heightened use of active transport modes was informed by relevant literature [
29]. The scale comprises five items categorised as ‘pros’ and five items categorised as ‘cons’. Participants were instructed to assess the importance of each item in their decision to enhance their PA levels through active transport using a five-point scale ranging from 1 (not important) to 5 (extremely important). The adapted DB measure for active transport use is provided in
Appendix A.
To calculate the DB score, participants’ scores for “pros” and “cons” were separately summed and averaged. The difference between these two scores was then computed by subtracting the cons from the pros. A positive final score indicated that the individual endorsed more pros than cons regarding the target behaviour. Conversely, a negative score signified a higher perception of cons by the participant.
2.1.3. Situational-Confidence Questionnaire
A six-item questionnaire for self-efficacy, called the situational confidence questionnaire (SCQ), has been adapted in the current study [
52]. The SCQ typically presents individuals with scenarios or situations related to the behaviour of interest which in this case is active transport use. Participants are asked to rate their confidence in successfully adopting active transport in challenging situations, providing nuanced insights into their perceived capability. The chosen scenarios encompass readiness to increase physical activity through active transport, social influence, weather impact, busy schedules, distance considerations, and the willingness to replace motorised transport. These scenarios represent common environmental constraints, aiming to gauge participants’ confidence in relation to their actual transport use. Participants were presented with six scenarios representing situations in which they encounter difficulty using active transport to enhance their physical activity (PA) levels. They were instructed to rate their confidence for each scenario on a five-point scale, ranging from 1 (not confident at all) to 5 (completely confident). The modified version of the SCQ for active transport modes is included in
Appendix A.
To calculate the SCQ score, the sum of each participant’s responses was computed, and then the average was determined. The maximum achievable score was five, with a higher score indicating an elevated level of self-efficacy, while lower scores suggested the opposite.
3. Data Analysis
The initial analysis of the TTM constructs questionnaire results was conducted in Microsoft Excel, 2016. The rest of the analyses were performed with IBM Corp., released 2019, IBM SPSS Statistics for Windows, version 26.0, and Studio Version 1.2.1335, 2009–2019 RStudio, Inc. The data were first tested for normality. The Shapiro Wilk and Kolmogorov–Smirnov tests yielded significant values (
p < 0.05) for maintenance and DBI scores as well as pre-contemplation and SCQ. Due to the relatively large sample size (n = 260), the violation from the normality assumption was not considered problematic [
61]. The results section is divided into two subsections. First, we performed Explanatory Factor Analysis (EFA) to examine the structure of the URICA instrument or in simple words to explore the number of SOCs present in the sample population. Second, we performed a series of one-way analysis of variance (ANOVAs) to determine the differences in both DB and SCQ scores across SOCs, and likewise to determine the differences of both DB and SCQ scores across the level of use of active transportation modes. Afterwards, a contingency table analysis was performed to assess the correlation between the use of active transport modes and the five stages determined by URICA.
3.1. Step-1: URICA-Based SOCs
At first, a straightforward RTC-based classification was worked out in MS Excel as proposed in standard practices [
57,
62,
63]. Each item on the questionnaire was associated with one of the five Transtheoretical Model (TTM) stages. The scores for each stage were totalled and then averaged. For instance, the responses to the four questions assigned to the contemplation stage were summed and divided by 4. Subsequently, the sum of the scores from each stage was computed. The final RTC Score was configured by subtracting the mean score of the pre-contemplation stage from the sum of all the scores across stages. Individuals scoring 8 or lower were categorised as being in the pre-contemplation stage. Scores between 9 and 11 were classified as the contemplation stage, while scores from 12 to 14 were attributed to the preparation or action stages. Scores exceeding 14 were designated as the maintenance stage.
Following this, the reliability of URICA items to measure the common factor (SOCs) was assessed using McDonald’s Omega (ωh), a reliable measure with values above 0.65 expected for good reliability and an acceptable classification error of <10% [
64,
65]. Subsequently, Exploratory Factor Analysis (EFA) was conducted. The Kaiser-Meyer-Olkin (KMO) test, assessing common variance within the dataset, was performed with a value between 0.80–0.90 considered meritorious or good. Bartlett’s Test of Sphericity was applied to ensure the appropriateness of data for EFA, with significance (
p ≤ 0.05) indicating suitability [
66,
67]. Two criteria, namely the scree plot and parallel analysis, were considered to retain factors [
66,
67,
68]. Additionally, the Oblimin rotation method was utilised to enhance factor interpretation, allowing for correlated factors, and is considered satisfactory in performance [
66,
67].
In the URICA-E2 survey, the pre-contemplators are further divided into subgroups of believers and non-believers. The results of an initial parallel analysis suggested only a four-factor solution and indicated that the stages of pre-contemplation non-believer (PCNB) and maintenance were loaded on the same factor but in opposite dimensions. The factor loadings of maintenance items were positive and of PCNB were negative which is explainable as the maintenance stage represents the people with already established behaviour activity and the people in the PCNB stage simply do not have any motivation to perform the behaviour. However, when another EFA was conducted excluding the survey items related to PCNB (U1, U3, U6, and U9, U refers to the URICA-based survey item in
Appendix A), while parallel analysis and scree test suggested a five-factor solution. The results and explanation of the final EFA are provided in
Section 4.
3.2. Step-2: Determining Differences of Both DB and Self-Efficacy across SOCs and the Use of Active Transportation
Aa a second step, the assumptions of ANOVA analysis, including requirements for sample size and independence of observations, were assessed. The normality for both the DB and SCQ scores was first checked through skewness and Kurtosis and found normally distributed with skewness of DBI = −0.267 (SE = 0.151) and SCQ = −0.077 (SE = 0.151) and Kurtosis of DBI = 0.312 (SE = 301) and SCQ = −0.390 (SE = 301), respectively. Likewise, Levene’s test of equality of error variances showed no significant levels (
p > 0.05) for each outcome variable. To gain deeper insight into the omnibus differences between stages and behaviour categories, the post hoc analysis of Tukey’s Honestly Significance Difference (HSD) was performed as it is better for unequal samples across groups [
69,
70].
The scale items 1,3,5,7,9 were classified as ‘pros’ whilst items 2,4,6,8,10 were classified as ‘cons’ (
Appendix A). However, the ten-item scale of DB was reduced to an eight-item measure to calculate the DB score. The survey analysis showed that a significant proportion of participants did not respond to question 10. To ensure balance between ‘pro’ and ‘con’ items, question number 3 was omitted considering question 9 as the suitable alternative to it.
5. Discussion
Our main objective was to assess the overall suitability of the Transtheoretical Model (TTM) and its constructs as a viable measure of Readiness to Change (RTC) in individuals utilising active transport to enhance their physical activity (PA) levels. Consequently, this study aimed to investigate the psychometric properties of the adapted URICA-E2 for assessing readiness to change concerning the use of active transport. Moreover, the important assumption of TTM, that the DB and self-efficacy of individuals increase as they progress through earlier to later stages of change, was assessed as well in this study.
5.1. Stage Allocation by URICA for the Use of Active Transport Modes
The initial allocation of the respondents of URICA through the RTC score was successful in identifying each of the five SOCs described in the TTM framework within the sample. Based on the conceptual grouping of each item within its corresponding component, we identified the following TTM dimensions: pre-contemplation believer, contemplation, preparation, action, and maintenance by a twenty survey item URICA for active transport modes use. The RTC scores based on URICA allocated the majority of participants in the earlier stages, i.e., pre-contemplation and contemplation. Only two respondents were present in the maintenance stage. Additionally, the result of the EFA carried out on the URICA questionnaire identified five factors when excluding the PCNB. The previous studies using URICA-E2, however, reported six SOCs in contrast to the current study [
35,
56,
59]. In an initial EFA, PCNB did not turn out as a separate factor for instead the related survey items were loaded on the maintenance factor but in an opposite direction. This refers to the lower means of responses to PCNB survey items by the respondents who were already in the maintenance stage. The main reason behind this can be the type of behaviour and population in the current study. The use of active transport modes is an essential part of the majority of students’ daily travel routine despite their lack of motivation for it. Previous studies show higher percentages of university students have reported active travel [
72,
73].
The overall component loadings were lower than those recorded by a previous study [
35,
56].
Table 3 shows the factor loadings of all twenty survey items of URICA. One of the survey items from the action stage (U4) is loaded better on the maintenance stage than on the action stage. Likewise, two survey items related to the preparation stage (U14 and U23) are better loaded on contemplation and action stages, respectively. Lerdal et al. (2009) observed a similar result in terms of factor loadings. For instance, the factor loadings for preparation-related items (U14 and U23) were observed relatively lower than the other two survey items. Correspondingly, the same was true for the survey item relating to the action stage (Q4UA). It was also observed that only one survey item related to action loaded more significantly on the maintenance stage. This contrasts with the findings of Lerdal et al. (2009), where all items associated with the action and maintenance stages were represented by a single factor. The explanation provided in that study was that the concepts underlying responses related to action involved the notion of ‘keeping up with exercise,’ which could then be linked to the idea of the maintenance stage. Moreover, the translation of the questionnaire into Norwegian influenced the phrasing of question items, contributing to the observed result. A similar phenomenon might have occurred in the current study. For instance, the phrasing of certain question items was, in some cases, quite similar, such as “I am finally regularly increasing physical activity levels by using active transport modes” (U4 from URICA) and “I have been increasing my physical activity levels by using active transport modes for a long time and I plan to continue” (Q2 from URICA, maintenance). The former item loaded more heavily on the component corresponding to the maintenance stage. The same situations are true for the items related to the preparation stage. The remaining items presenting the preparation stage (U17 and U20 from URICA) both include planning activity with a friend so probably this factor is more representative of a new factor (e.g., preparing with social circle) than the preparatory stage itself. We performed various Confirmatory Factor Analyses (CFAs) using URICA’s twenty survey items for active transport modes use. The indicators of the model fit were deemed satisfactory, with Goodness-of-Fit Indices exceeding 0.9, Tucker-Lewis Index surpassing 0.9, and the standardized Root-Mean-Square Residual (RMSR) below 0.05, along with a Root-Mean-Square Error of Approximation (RMSEA) below 0.08 [
58,
74]. The three above-mentioned items related to action and preparation stages were excluded. This suggests the potential need for a reassessment of the language and phrasing, particularly in the double-back translation process, for subsequent questionnaires in both the English and Dutch versions. This consideration aims to ensure the linguistic accuracy and cultural equivalence of the items, warranting further attention to enhance the reliability and validity of the measurement instrument.
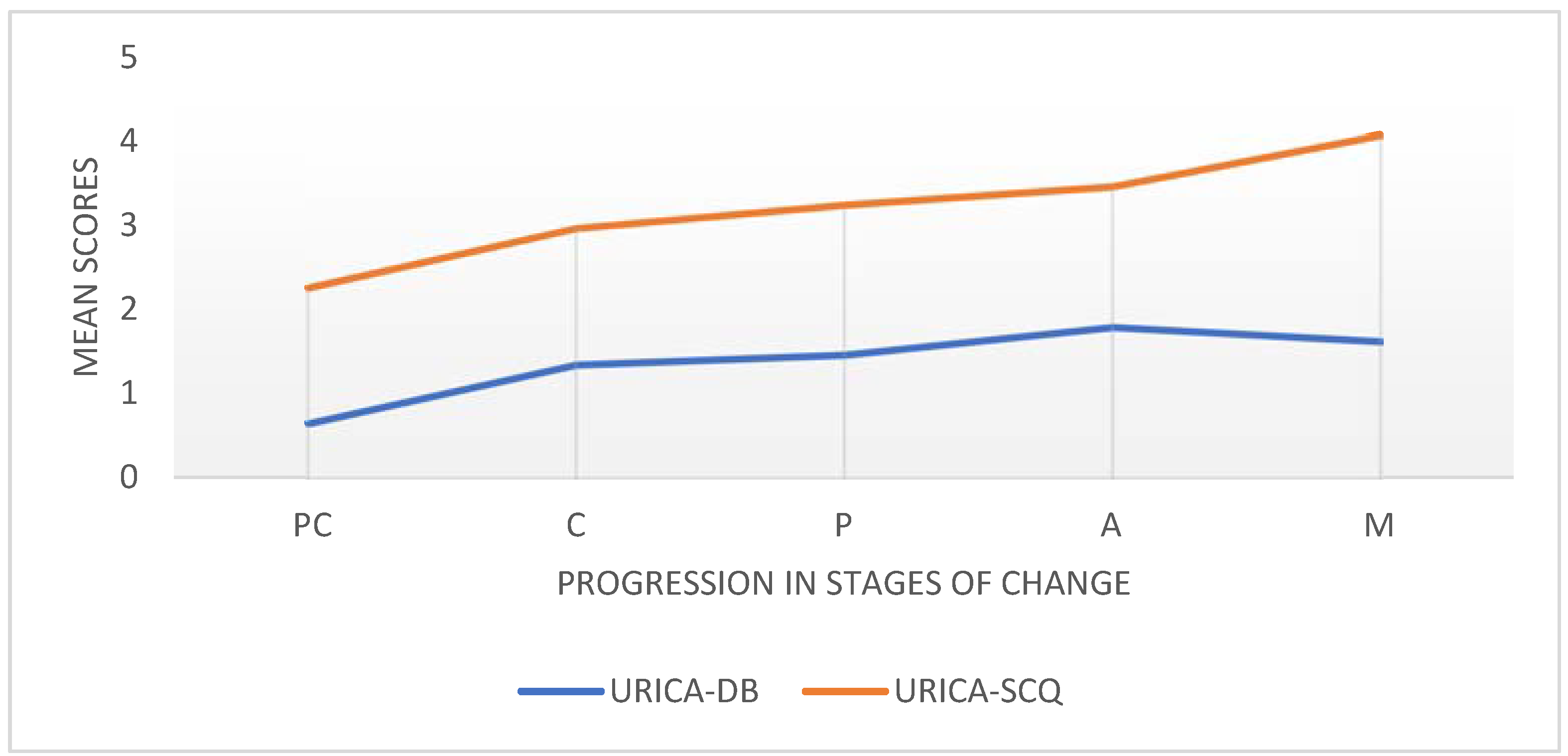
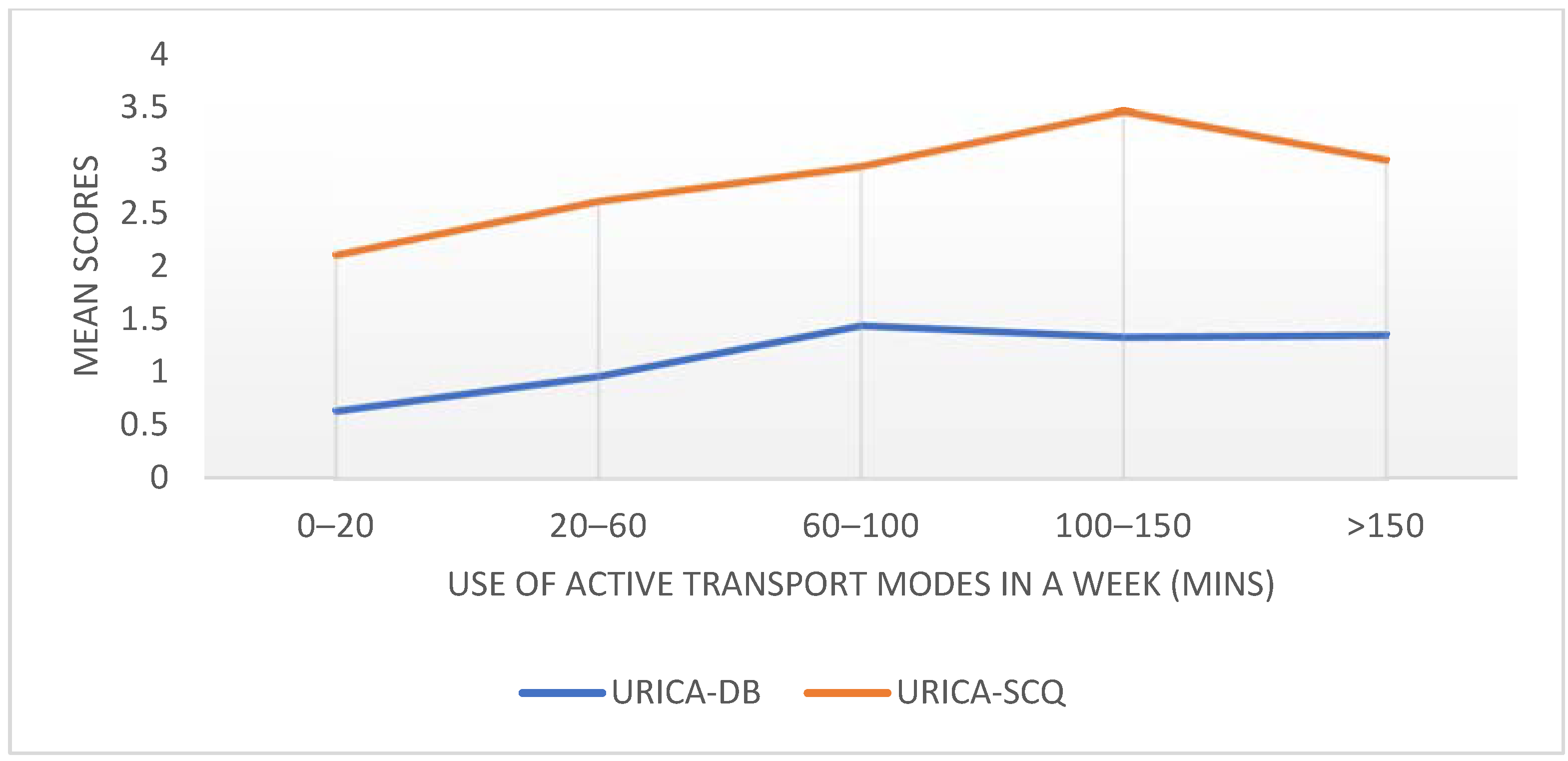
5.2. Decisional Balance and Self-Efficacy across SOCs and Use of Active Transport Mode Behaviour
In agreement with the assumption of TTM, the mean scores of DBI and SCQ increase with the progress in the later stages as well as with increased use of active transport modes. Furthermore, post hoc analyses showed a separating of the earlier stages from the later stages. The scores for DB pros have been observed to increase from the contemplation or preparation stages in previous research [
32]. This observation suggests that individuals may adjust their attitudes toward a behaviour before actually making the change [
22]. Therefore, the increasing pattern in Decisional Balance (DBI) scores across Transtheoretical Model (TTM) stages aligns with the theory, indicating that individuals undergo an attitude change before initiating behaviour change. A similar pattern is noted in self-efficacy, implying that individuals experience a boost in confidence related to the target behaviour as they advance through the stages. Moreover, it was also confirmed that the positive perception of pros (advantages) and cons (disadvantages) of behaviour and self-efficacy of enacting behaviour are both linked to the higher use of active transport modes. Finally, the significant correlation between the categories of self-reported behaviour and TTM stage allocation by URICA was positive indicating that SOCs can determine the use of active transport modes. As already explained in the introduction, the studies using TTM in the use of active transportation behaviour typically used staging algorithms, which allocate the individual in discrete SOCs [
45,
49,
50]. In this case, to the best knowledge of the authors, the significant association of continuous measure URICA-based SOCs with the use of active transport is a unique finding.
The URICA, as a continuous measure, enables individuals to attain high scores on one stage while concurrently achieving scores on other subscales. This arguably mirrors the fluctuating nature of, in this instance, physical activity (PA) through active transport. Such an approach may align with the notion of engaging in active modes that depend on various external factors like weather, access, and health, among others [
75]. To bridge the gap created by constraints, future research could consider incorporating real-time or ecological momentary assessment methods. These approaches capture individuals’ experiences in the context of their daily lives, providing a more nuanced understanding of how external factors influence their readiness to engage in active transportation. An individual might continuously cycle through the stages, contingent on their life circumstances. Notably, previous applications of the Transtheoretical Model (TTM) have primarily focused on individuals committing to discontinuing a behaviour rather than initiating a new one [
35]. Therefore, starting or improving the use of active transport modes might consist of different underlying change mechanisms and stages of the model.
The successful application of TTM to the use of active transport modes can help highlight the underlying motivation factors to predict behavioural change. This study validates that the individual perception of the pros, cons, and self-efficacy of being physically active can influence the use of active transport modes. The URICA can be useful in identifying the different profiles based on the motivation stages to ensure sufficient use of active transport and consequent physical activity and alignment with the sustainable development goals. This study underscores the significance of population segmentation and the application of customized behavioural processes to facilitate effective change. A pertinent example supporting the efficacy of population segmentation and the applicability of the three-stage Transtheoretical Model (TTM) in the context of active transport is derived from a study conducted in Stockholm. This study validated the three-stage TTM model specifically for bicycle use. The findings underscored the utility of understanding distinct motivational profiles and tailoring interventions to individuals in the pre-motivation, motivation, and volition stages, providing empirical support for the effectiveness of targeted strategies in promoting bicycle use in urban environments [
76]. The utility of the Transtheoretical Model (TTM) in behaviour change extends beyond active transport; it can also be applied, for instance, in promoting sustainable travel behaviour through smartphones [
77] and advocating for sustainable driving [
78].
5.3. Limitations and Future Directions
This study has two main limitations: the use of a convenience sample, with the majority being students, and reliance on a self-report measure of behaviour. To address these limitations, future studies are recommended to test the URICA for the use of active transport modes in a more diverse population, possibly with an even larger sample size. Introducing an objective measure and incorporating an element of concurrent validity could enhance the robustness of testing.
Despite the back-translation procedure, some of the URICA questions might be somewhat confusing, especially when translated into Dutch. Therefore, it is suggested to employ a more collaborative and iterative approach [
79] to identify redundant items in the URICA scale. This approach can help refine the questionnaire and im-prove its clarity and applicability across different language versions. A recommendation for future intervention design would be to identify the behaviour change techniques relevant to POC and further extend the utility of TTM in the use of active transport modes. It can also highlight the requirement for designing need-based tailored interventions to achieve effective enactment of behaviour [
40,
80].
6. Conclusions
The outcomes of this study bear significance for individuals and societies alike, as the promotion of active transportation emerges as a key driver toward attaining the health and sustainability goals of global cities. More importantly, this study adds to the comprehension of active transport modes, recognized for their potential in mitigating the advancement of numerous chronic diseases, while also addressing pressing environmental issues like congestion and emissions. In particular, the findings imply that the URICA can effectively discern respondents’ change profiles across various stages. The participants of the study were categorised into five SOCs defined in TTM as pre-contemplation, contemplation, preparation, action, and maintenance. Well-known assumptions concerning the TTM framework were confirmed in the current study. The DB and self-efficacy of the use of active transport modes behaviour increase as individuals progress through the stages. The same is also true for the self-reported level of the use of active transport modes to increase physical activity. In summary, these observations hold the potential to not only predict the likelihood of respondents changing their active travel behaviours but also to pinpoint appropriate and customized behaviour change strategies aimed at enhancing travel-related physical activity. Modifications to the URICA instrument items could enhance its applicability for future studies in more diverse populations.


 ,
, 
{kind=link}
{kind=link}

