

Life-Cycle Spatial Strategy for Multidimensional Health-Oriented Medical Care Community—From the Perspective of Sustainable Marketing
Abstract
:1. Introduction
2. Literature Review
3. Theoretical Framework and Research Hypotheses
3.1. Sort Out the Dimensions of Health and Establish the Interactive Relationship between Health and Space
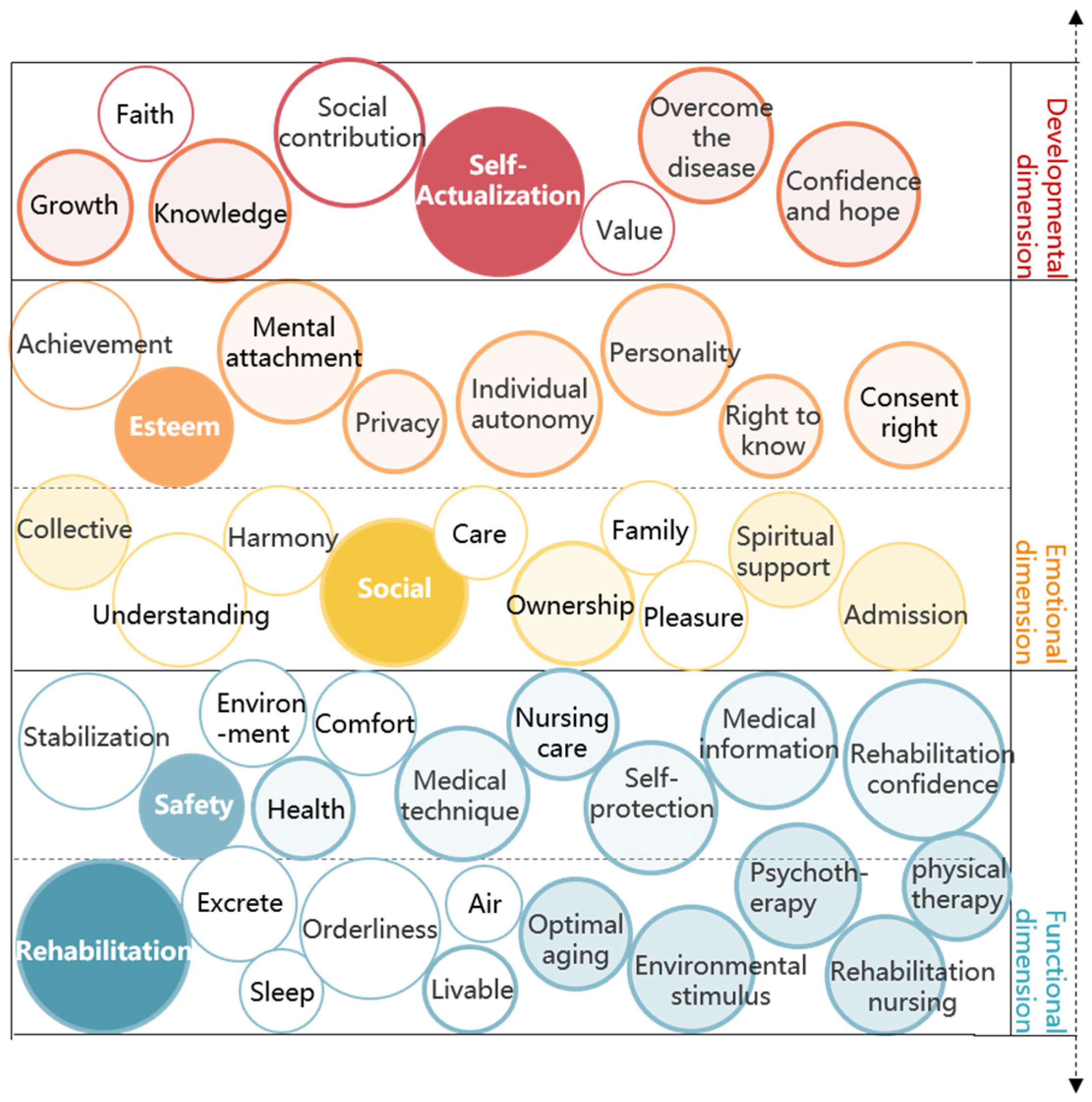
3.2. Deducing the Medical Care Maslow’s Hierarchy of Needs System and Constructing the Theoretical Model of HBSI
3.3. HBSI Theoretical Model Interpretation and Spatial Application
4. Materials and Methods
4.1. Construction of Spatial Factor Index System Based on Multidimensional Health
4.1.1. Research Methods
- (1)
- Empirical case analysis
- (2)
- Index selection and index consultation table
- (3)
- Index screening
4.1.2. Results and Discussion
- (1)
- Influencing factors of life safety dimension
- (2)
- Influencing factors of physical health dimension
- (3)
- Influencing factors of mental health dimension
- (4)
- Influence factors of social adaptation dimension
- (5)
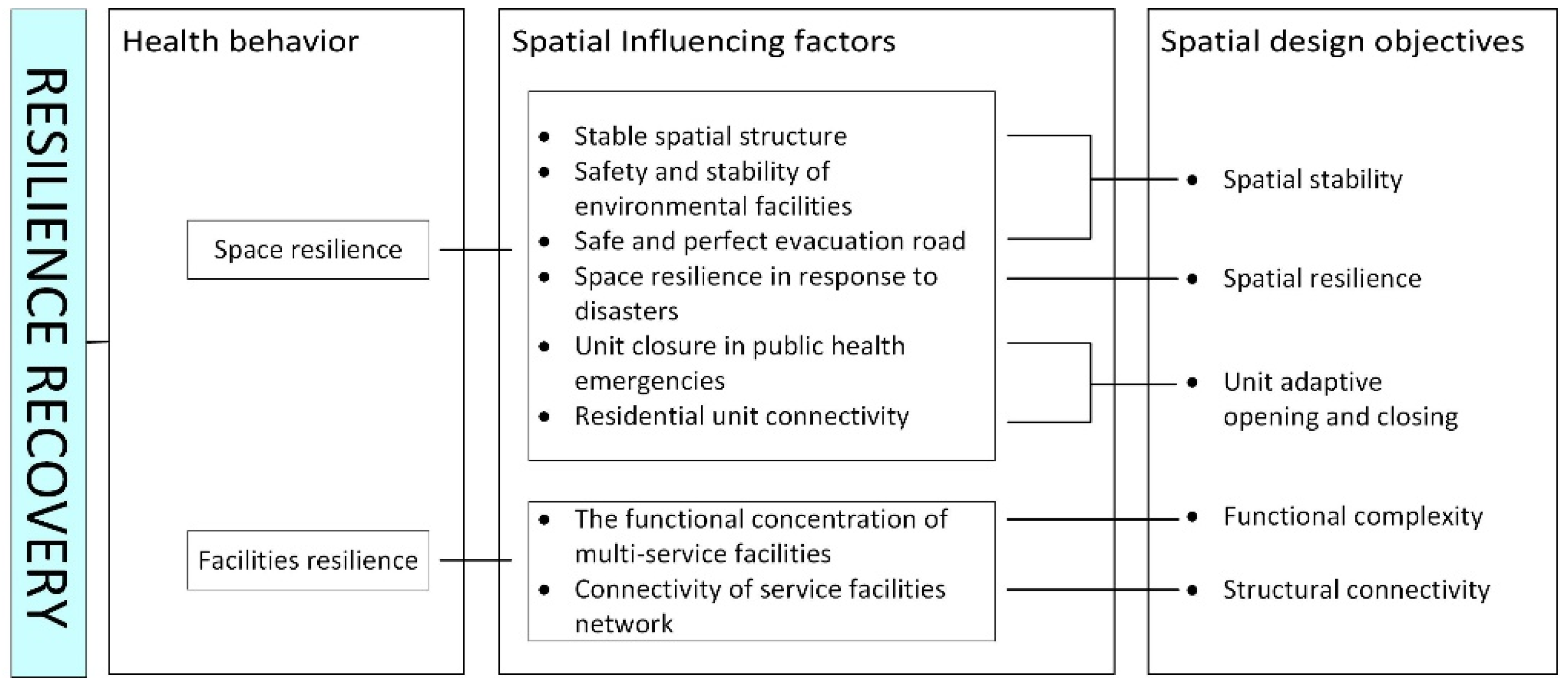
- Influencing factors of resilience recovery dimension
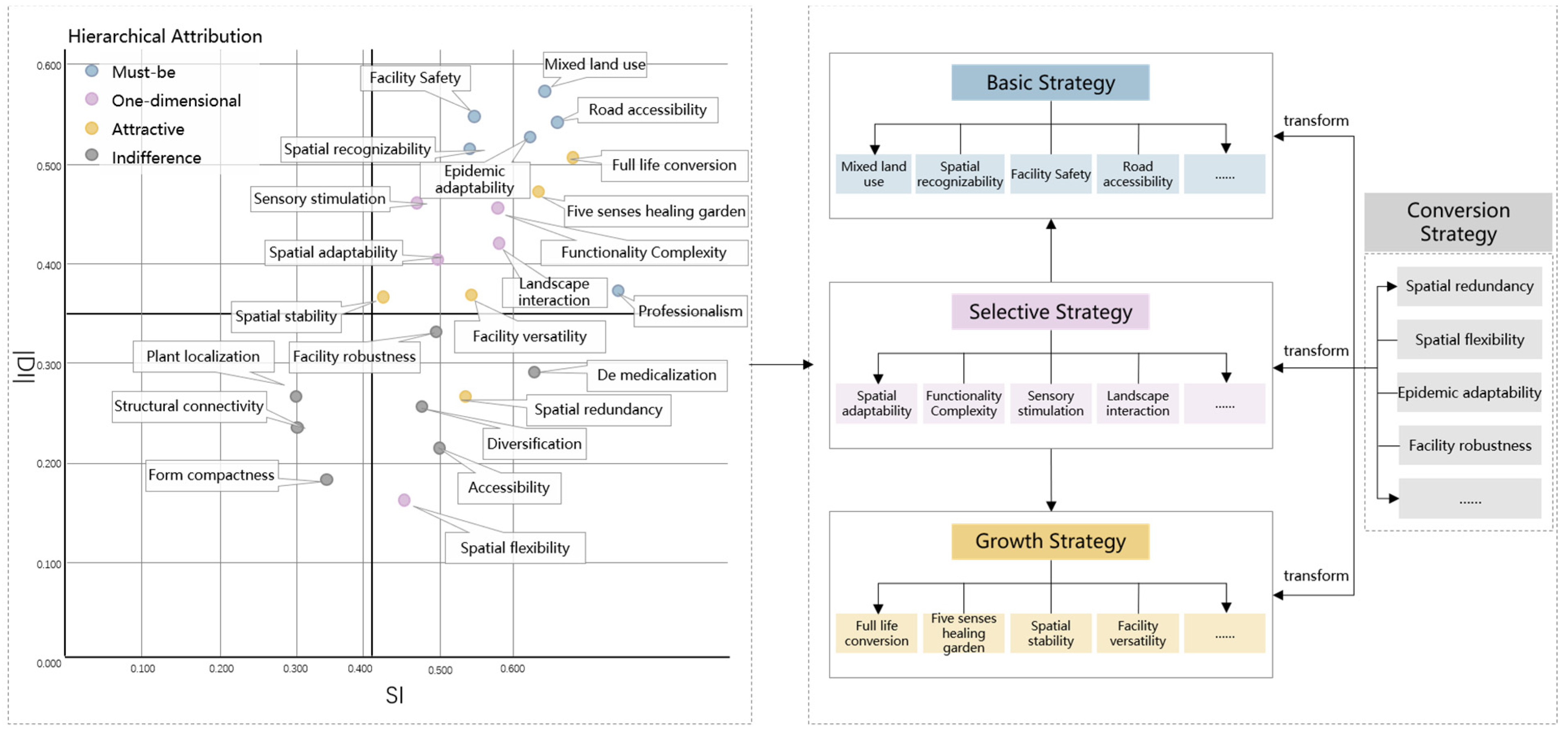
4.2. HBSI Design Strategy and Guidelines
- (1)
- Theme differentiation, moderately mixed land functional layout
- (2)
- Organic, cooperative and stable spatial settlement patten
- (3)
- Diversified and healthy open space network
- (4)
- General and professional health care supporting service facilities
- (5)
- Flexible, dynamic and adaptative design of medical care house
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Dimension | Health Behavior Path | Space Design Objectives | Spatial Influence Factor | Very Unimportant 0 Point | Relatively Unimportant 3 Points | Regular 5 Points | Relatively Important 7 Points | Very Important 10 Points |
|---|---|---|---|---|---|---|---|---|
| Life safety | Reducing crime | Visibility | Unobstructed vision of activity space | |||||
| The visual attraction of the activity space | ||||||||
| Spatial hierarchy | Clear boundaries between public space and private space | |||||||
| Behavior safety | Identifiability | Identification of space environment | ||||||
| Territoriality | Semi-private space domain | |||||||
| Space buffering | Buffer space reserved around the entrance and exit of motor vehicles | |||||||
| Isolation and protection of landscape greening around roads | ||||||||
| Facility security | Environmental facilities for safety protection | |||||||
| Path security | Path safety in pedestrian space | |||||||
| Safe connection between motor traffic and slow traffic | ||||||||
| Disaster response | Traffic unblocked degree | The degree of patency of evacuation passages | ||||||
| Spatial redundancy | The possibility of being converted into an emergency shelter during a disaster | |||||||
| Physical health | Reducing pollution exposure | Low pollution | Site away from pollution | |||||
| Motor traffic pollution isolation and protection | ||||||||
| Road density and flow control | ||||||||
| Permeability | Lower building density | |||||||
| Good ventilation corridor | ||||||||
| Street spatial configuration | The ratio of the height of buildings on both sides of a street to the width of the street | |||||||
| Roof form | ||||||||
| Architectural layout | FAR | |||||||
| Building density | ||||||||
| Building height | ||||||||
| Road organization | ||||||||
| Integration and dispersion of buildings | ||||||||
| Greening rate | The proportion of greening land in total space | |||||||
| Air Pollution Index | Grade evaluation index of pollutant content in the air | |||||||
| Enhancing physical activity | Functional complexity | Degree of mixed use of land | ||||||
| Road network density suitable for travel | ||||||||
| Full range of services within walking distance | ||||||||
| Walking accessibility | Connectivity of slow traffic systems | |||||||
| Clear and easily identifiable walking paths | ||||||||
| Suitable walking length | ||||||||
| Walking suitability | Comfortable walking space and facilities | |||||||
| Comfortable and pleasant walking environment | ||||||||
| Safe walking paths and space facilities | ||||||||
| Spatial adaptability | Works well in different seasons and weather conditions | |||||||
| Get close to nature | Green visibility | Proportion of green landscape in public space view range | ||||||
| Proportion of green landscape in master bedroom view area | ||||||||
| Clustering | The proportion of centralized green space in the total green space | |||||||
| Vertical greening accounts for the proportion of total green space | ||||||||
| Natural ecology | Intimate contact with the natural landscape space | |||||||
| Mental health | Visual comfort | Spatial aesthetics | The visual sense of space environment is beautiful and comfortable | |||||
| Space openness | Length-width ratio of public space | |||||||
| The permeability of space | ||||||||
| Apparent green rate | The proportion of green plants in the visual environment | |||||||
| Health cognition | Healthy cognition | Health education and guidance of space | ||||||
| Landscape healing | Layout diversity | Diversity of landscape plant types and disposition | ||||||
| Sensory experience | Perceptibility and experience of landscape environment | |||||||
| Natural ecology | The continuity of the corridor with the surrounding natural landscape | |||||||
| Facility richness | Diversification of types of environmental facilities | |||||||
| Natural experience | Terrain richness | Topographic changes in the landscape environment | ||||||
| Proportion of native plants | Proportion of native plants in landscape configuration | |||||||
| Social adaptation | Social interaction | Spatial inclusion | Accommodate people of different ages and genders | |||||
| Spatial vitality | Aggregation and continuity of environment and facilities | |||||||
| Spatial hierarchy | An open, private and orderly level of communication space | |||||||
| Leisure activities | Functional complexity | Multiple uses of external public space functions | ||||||
| Diversified and flexible use of the interior space of the house | ||||||||
| Spatial adaptability | Space usability throughout the day and all ages | |||||||
| Adaptability of capacity | ||||||||
| Spatial richness | Diversity of space activities and facilities | |||||||
| Resilience recovery | Spatial resilience | Spatial stability | Stable community spatial structure | |||||
| Stability of medical and residential spatial elements | ||||||||
| Unit adaptability | The relative independence of nursing units | |||||||
| The interconnectedness of health care groups | ||||||||
| Spatial redundancy | The possibility of changing the space among rescue, epidemic prevention and daily activities | |||||||
| Facility resilience | Structural connectivity | Structural connectivity of rehabilitation infrastructure | ||||||
| Functional complexity | Diversified and concentrated functions of medical and caring service facilities |
References
- Zhu, J. The Demand and Satisfaction about “Combined Medical and Nursing” in the Community Care for the Elderly: Take Xuanwu District of Nanjing as an Example. Master’s Thesis, Nanjing University, Nanjing, China, 2016. [Google Scholar]
- ITO, M.; Zhou, Y.; Qin, L. Inspirations from the Deployment and Development Experiences of the Community-based Elderly Facilities in Japan for China. Urban Plan. Int. 2020, 35, 20–28. [Google Scholar]
- Chen, Y.; Kang, J.; Lian, F. An Analysis of the Model of Integrated Health and Social Care for the Elderly Facilities in the UK and Its Impact. Archit. J. 2016, 11, 84–88. [Google Scholar]
- Li, C. Health City: A Singapore Model for Integrating Health Care. China Eng. Consult. 2016, 6, 52–55. [Google Scholar]
- Tong, C.; Wang, S. Review on the Combination of Medical Care and Pension. Sci. Res. Aging 2016, 4, 63–72. [Google Scholar]
- Yu, Z.; Xu, Y. Cutting-edge Research and Hotspot Issues of in the Sphere of Elderly Care Service in China (1998–2018): An Analysis Based on CiteSpace. Sci. Res. Aging 2020, 8, 33–45. [Google Scholar]
- Wu, Y.; Yang, J.; Chen, Q. Research Progress and Key Dimension Exploration of Healthy Community Construction: Based on the Analysis of International Knowledge Map. Urban Plan. Int. 2020, 35, 80–90. [Google Scholar]
- King, L.A.; Hood, V.L. Ecosystem Health and Sustainable Communities: North and South. Ecosyst. Health 1999, 5, 49–57. [Google Scholar] [CrossRef]
- Ellaway, A.; Macintyre, S.; Kearns, A. Perceptions of Place and Health in Socially Contrasting Neighbourhoods. Urban Stud. 2001, 38, 2299–2316. [Google Scholar] [CrossRef]
- Vojnovic, I. Building Communities to Promote Physical Activity: A Multi-Scale Geographical Analysis. Geogr. Ann. 2006, 88, 67–90. [Google Scholar] [CrossRef]
- Tan, S.; Guo, J.; Jiang, Y. Impact of Human Settlements on Public Health: New Frontier in Urban Planning Research. Urban Plan. Forum 2010, 4, 66–70. [Google Scholar]
- Wang, L.; Liao, S.; Zhao, X. Exploration of Approaches and Factors of Healthy City Planning. Urban Plan. Int. 2016, 31, 4–9. [Google Scholar] [CrossRef]
- Matlovicová, K.; Mocák, P.; Kolesárová, J. Environment of estates and crime prevention through urban environment formation and modification. Geogr. Pannonnica 2016, 20, 168–180. [Google Scholar] [CrossRef]
- Au-Yong-Oliveira, M.; Sousa, M.J. Sustainable Marketing and Strategy. Sustainability 2022, 14, 3642. [Google Scholar] [CrossRef]
- Matlovičová, K.; Mocák, P. Intraurbánna kriminalita a jej prevencia v konceptuálnom rámci CPTED (príklad mesta Prešov). Geogr. Časopis 2014, 66, 199–223. [Google Scholar]
- Dong, J. The Construction of Urban Healthy Living Unit Based on Behavior Change Theory. Ph.D. Thesis, Harbin Institute of Technology, Shenzhen, China, 2010. [Google Scholar]
- Liu, J. Community Epidemic Prevention Planning and Governance System against COVID-19 Epidemic. Planners 2020, 36, 86–89. [Google Scholar]
- Pachura, P.; Nitkiewicz, T.; Matlovičová, K.; Matlovič, R. Identification of Intellectual Capital Performance Using Data Envelopment Analysis; Springer International Publishing: Cham, Switzerland, 2018; pp. 115–130. [Google Scholar]
- Niwash, M.N.K.; Cek, K.; Eyupoglu, S.Z. Intellectual Capital and Competitive Advantage and the Mediation Effect of Innovation Quality and Speed, and Business Intelligence. Sustainability 2022, 14, 3497. [Google Scholar] [CrossRef]
- Alexandre, T.D.S.; Cordeiro, R.C.; Ramos, L.R. Factors associated to quality of life in active elderly. Rev. Saude Publ. 2009, 43, 613–621. [Google Scholar] [CrossRef]
- Grönroos, C. Service Management and Marketing; Lexington Books: Lexington, MA, USA, 1990; Volume 27. [Google Scholar]
- Zhang, X.; Liu, B. Study on Quality Model of Community Home Care Service: A case study of Shanghai. Chin. J. Popul. Sci. 2011, 3, 83–92. [Google Scholar]
- Grönroos, C. A service quality model and its marketing implications. Eur. J. Mark. 1993, 18, 36–44. [Google Scholar] [CrossRef]
- He, W. Research on Architectural Design of Old-Age Facilities under the Combination of Medical Treatment and Health Care in Urban Community. Master’s Thesis, Xi’an University of Architecture and Technology, Xi’an, China, 2017. [Google Scholar]
- Waldron, V.R.; Gitelson, R.; Kelley, D.L. Gender differences in social adaptation to a retirement community: Longitudinal changes and the role of mediated communication. J. Appl. Gerontol. 2005, 24, 283–298. [Google Scholar] [CrossRef]
- Chen, Z. A Study on the Adaptation of Existing Communities Based on Environmental Behavior. Master’s Thesis, Nanjing University of Science & Technology, Nanjing, China, 2018. [Google Scholar]
- Wang, Y. Research on the Impact of Urban Community Public Space on Residents’ Emotions. Master’s Thesis, Huazhong University of Science and Technology, Wuhan, China, 2020. [Google Scholar]
- Du, M. A Study on Functional Design Strategy of Community Elderly Health-Care Facilities from Maslow’s Hierarchy of Needs. Master’s Thesis, Shenzhen University, Shenzhen, China, 2020. [Google Scholar]
- McKenzie-Mohr, D. Fostering sustainable behavior through community-based social marketing. Am. Psychol. 2000, 55, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Xie, X.; Zhang, Y. Review and Prospect on the Research of the Relationship between Built Environment and Mental Health: Literature Review Based on the Perspective of Restorative Environment. J. Hum. Settl. West China 2020, 35, 34–42. [Google Scholar]
- Li, X. Research on Design Strategy of Urban Community Health and Care Complex for the Elderly. Master’s Thesis, Shenzhen University, Shenzhen, China, 2020. [Google Scholar]
- Zhang, K. Research on Planning and Design of Whole Age Community—A Case Study of Zhengding Community in Shijiazhuang. Master’s Thesis, Beijing Jiaotong University, Beijing, China, 2020. [Google Scholar]
- Zhang, Y.; Qin, B. The impact of urban built environment on residential physical health: Based on propensity score matching. Acta Geogr. Sin. 2018, 73, 333–345. [Google Scholar]
- Hua, Y. Research on the Vitality Shaping of Living Street Space Based Behavioral Psychology—A Case Study of Dongguan Street in Yangzhou. Master’s Thesis, East China University of Science and Technology, Shanghai, China, 2020. [Google Scholar]
- Yu, S.; Liu, Y.; Cui, C.; Xia, B. Influence of outdoor living environment on elders’ quality of life in old residential communities. Sustainability. 2019, 11, 6638. [Google Scholar] [CrossRef]
- Luque-Reca, O.; Augusto-Landa, J.M.; Pulido-Martos, M. Emotional intelligence and depressive symptoms in Spanish institutionalized elders: Does emotional self-efficacy act as a mediator? PeerJ 2016, 4, e2246. [Google Scholar] [CrossRef]
- Othman, A.R.; Fadzil, F. Influence of Outdoor Space to the Elderly Wellbeing in a Typical Care Centre. Procedia Soc. Behav. Sci. 2015, 170, 320–329. [Google Scholar] [CrossRef]
- Afshar, P.F.; Foroughan, M.; Vedadhir, A.; Tabatabaie, M.G. Psychometric properties of the Persian version of Social Adaptation Self-evaluation Scale in community-dwelling older adults. Clin. Interv. Aging 2017, 12, 579. [Google Scholar] [CrossRef]
- Wang, L.; Li, X.; Yang, X. Health in 15-minute Life Sphere: Community Response to Public Health Emergency. Planners 2020, 36, 102–106. [Google Scholar]
- Fransen, J.; Peralta, D.O.; Vanelli, F.; Edelenbos, J.; Olvera, B.C. The emergence of urban community resilience initiatives during the COVID-19 pandemic: An international exploratory study. Eur. J. Dev. Res. 2022, 34, 432–454. [Google Scholar] [CrossRef]
- Conroy, K.M.; Krishnan, S.; Mittelstaedt, S.; Patel, S.S. Technological advancements to address elderly loneliness: Practical considerations and community resilience implications for COVID-19 pandemic. Work. Older People 2020, 24, 257–264. [Google Scholar] [CrossRef]
- Du, S.; Tan, H. Location Is Back: The Influence of COVID-19 on Chinese Cities and Urban Governance. Sustainability 2022, 14, 3347. [Google Scholar] [CrossRef]
- Lv, B.; Sun, T. Study on Spatial form Compactness from Low-Carbon Perspective. Geogr. Res. 2013, 32, 1057–1067. [Google Scholar]
- Wang, S.; Wei, C.; Yuan, Y.; Shan, Z.; Xiang, K.; Huang, J.; Zhang, T. Academic Discussions on Human Settlement Environmental Plan and Design in the Background of COVID-19 Epidemics. South Archit. 2020, 3, 49–56. [Google Scholar]
- Hou, B. Research on the Demand Level and Satisfaction Strategy of Community Home-Based Care Service for Urban Elderlv. Ph.D. Thesis, East China Normal University, Shanghai, China, 2018. [Google Scholar]



















| Community Name | Shuiyunju | Wuzhishanju | Forest Lake | Rendishan Rainforest Health Care Base | Feicuitiancheng | ||
|---|---|---|---|---|---|---|---|
| Basic information and marketing status | Location | Rural | Suburban | Downtown | Downtown | Suburban | |
| Positioning | Ecological rehabilitation community | Spa rehabilitation community | Rehabilitation community | Medical care community | Comprehensive medical and nursing community | ||
| Product type | Health nursing multistory residences, Elderly-care villa | Nursing apartment, Healing villa | Nursing apartment, Health nursing villa, Wellness hotel | Medical care apartment, recovery hotels | Medical care apartment, Multistory residences, Nursing villa | ||
| Marketing strategy | International health resort community Living in slow water and fragrance | Live by Wuzhishan mountain Enjoy longevity gene, enjoy the hot spring of longevity | The Center of the Forest high-end wellness community | National Rainforest Recreation Base Life and recreation community | Let nature take its course, four seasons health care, “health care, recreation and learning” one-stop community with housekeeper | ||
| Price (RMB/Square meters) | 16,000–20,000 Daily rent: 200–800 | 12,000–15,000 | 16,000–18,000 | 16,000–18,000 Daily rent: 300–700 Monthly rent: 8000–9900 | 15,000–19,000 Daily rent 8000–9900 20-year tenure: 750–1300 thousand RMB | ||
| Scale | Site area | 8.69 ha | 8.43 ha | 31.3 ha | 13.3 ha | 27 ha | |
| Building area | 30,400 m2 | 27,016 m2 | 400,000 m2 | 250,000 m2 | 337,500 m2 | ||
| FAR | 0.35 | 0.29 | 1.28 | 1.88 | 1.25 | ||
| Green coverage ratio | 60% | 55% | 52% | 45% | 60% | ||
| Number of households | 220 | 321 | 4000 | 3000 wellness apartments | 3750 | ||
| Features of space and service | Land functional layout | Living function, Hotel function, Medical care service function, Leisure function is relatively independent. | Living function and the healing function are arranged independently. | Mainly living groups and it is equipped with a relatively complete business and health service. | The mixing degree of residential function, wellness function and medical care service function is high. | The plane layout is compatible with commercial, residential, medical complex, leisure and entertainment, etc. In the vertical layout, split-level space is used to set up public spaces such as shared meeting room, health activity room, rest room for health care, rainforest dining bar, etc. | |
| Spatial settlement organization | Spatial settlements are organically organized, maintaining good independence within the clusters, and weak connection between clusters. | Divided into coconut beach, Oak Bay, palm group of three settlements according to the natural terrain space. | It is composed of high-level cluster settlements and low-level enclosure settlements, which are naturally separated by a lake. | It is arranged around the medical care facilities in a free embrace style. The corridor system on the second and third floors connects the apartments with the facilities. | The group adopts an adaptive split layout, with a corridor linking medical and other facilities to the houses. | ||
| Open space network | The open space system is well combined with external resources and has built-in experiential health functions such as Binglang garden and Chenxiang garden. However, it is not well matched with demand, lacks consideration of user behavior characteristics, and is set too far away from daily use facilities. | Open space system consists of internal garden landscape composed of a variety of tropical plants and external natural landscape composed of local tropical mountains, tropical rainforests and other natural resources as the main line, which can meet the basic leisure needs of users, but lacks vitality elements in terms of functional implantation. | Open space system is complete, complete function configuration, creating a good health atmosphere and healing situation. | Open space considers the diverse demands of diversified medical and nursing population, and the network of open space is closely combined with the network of P-supporting service facilities, which reflect strong regional characteristics. | Three-dimensional open space network, that is, roof garden, multi-floor shared space and ground open space integrated configuration; With full consideration of diversity and suitable for aging people, it is equipped with a five-sense healing garden, medical-nursing-walking path, art and nursing-research room, etc., to enrich the slow walking experience and meet the needs of the whole age medical and nursing-care groups to carry out multi-dimensional health activities. | ||
| Supporting service facilities | Mainly prepared for wellness- and elderly care-related leisure activities, with Chenxiang health garden, multimedia conference room, coffee shop, music tea house, hair and beauty massage center, leisure fishing center, swimming pool, etc. | Spa treatments installed in every home; Comprehensive leisure and entertainment clubs; Other supporting facilities are lacking. | To meet the users’ rich life and health care service needs, lacking nursing, rehabilitation support functions. | To meet the needs of self-care elderly or chronic disease patients, there is less consideration for the support and care of the crowd; Although the configuration of medical and nursing facilities is diversified, the utilization rate of some facilities is low, such as molecular hydrogen immunization chamber, hyperbaric oxygen chamber, etc. The demands for traditional Chinese medicine, Li Miao health care, are huge. | The supporting facilities are divided into groups and configured in a classified way. According to the positioning of the group, facilities are configured for healthy people, chronic disease conditioning, sub-health diagnosis and treatment and rehabilitation, nursing support for semi-intermediary groups, and full-day medical care for intermediary personnel, with special emphasis on the treatment of traditional Chinese medicine and Li Miao Southern medicine. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Che, L.; Guo, Z.; Yang, Y.; Kang, H.; Cao, S. Life-Cycle Spatial Strategy for Multidimensional Health-Oriented Medical Care Community—From the Perspective of Sustainable Marketing. Sustainability 2022, 14, 11081. https://doi.org/10.3390/su141711081
Che L, Guo Z, Yang Y, Kang H, Cao S. Life-Cycle Spatial Strategy for Multidimensional Health-Oriented Medical Care Community—From the Perspective of Sustainable Marketing. Sustainability. 2022; 14(17):11081. https://doi.org/10.3390/su141711081
Chicago/Turabian StyleChe, Le, Zhijian Guo, Yi Yang, Honghao Kang, and Shangqing Cao. 2022. "Life-Cycle Spatial Strategy for Multidimensional Health-Oriented Medical Care Community—From the Perspective of Sustainable Marketing" Sustainability 14, no. 17: 11081. https://doi.org/10.3390/su141711081