
Innovation Resistance and Resource Allocation Strategy of Medical Information Digitalization

Abstract
:1. Introduction
1.1. Literature Review
1.1.1. Medical Information Digitalization
1.1.2. Medical Information Digitalization Barriers
Digitalized Analysis and Process
Medical Data Sharing
Infrastructure Resources
Regulation and Constraints
Operational Issue
2. Methods
2.1. Decision-Making Trial and Evaluation Laboratory (DEMATEL) Method
2.2. Importance-Resistance Analysis–Network Relation Map (IRA–NRM) Analysis
3. Results
3.1. Content Analysis
3.2. DEMATEL
3.2.1. Main Dimensions
3.2.2. Digitalized Analysis and Process
3.2.3. Medical Data Sharing
3.2.4. Infrastructure Resources
3.2.5. Regulation and Constraints
3.2.6. Operational Issue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rigamonti, L.; Albrecht, U.V.; Lutter, C.; Tempel, M.; Wolfarth, B.; Back, D.A. Potentials of digitalization in sports medicine: A narrative review. Curr. Sports Med. Rep. 2020, 19, 157–163. [Google Scholar] [CrossRef]
- Kikuchi, S.; Kadama, K.; Sengoku, S. Characteristics and Classification of Technology Sector Companies in Digital Health for Diabetes. Sustainability 2021, 13, 4839. [Google Scholar] [CrossRef]
- McKee, M.; van Schalkwyk, M.C.; Stuckler, D. The second information revolution: Digitalization brings opportunities and concerns for public health. Eur. J. Public Health 2019, 29 (Suppl. S3), 3–6. [Google Scholar] [CrossRef]
- Russom, P. Managing Big Data. In TDWI Best Practices Report; The Data Warehousing Institute: Phoenix, AZ, USA, 2013; pp. 1–40. [Google Scholar]
- Gu, D.; Li, J.; Li, X.; Liang, C. Visualizing the knowledge structure and evolution of big data research in healthcare informatics. Int. J. Med. Inform. 2017, 98, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Grayson, S.; Doerr, M.; Yu, J.H. Developing pathways for community-led research with big data: A content analysis of stakeholder interviews. Health Res. Policy Syst. 2020, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Mao, S.; Liu, Y. Big data: A survey. Mob. Netw. Appl. 2014, 19, 171–209. [Google Scholar] [CrossRef]
- Oussous, A.; Benjelloun, F.Z.; Lahcen, A.A.; Belfkih, S. Big Data technologies: A survey. J. King Saud Univ. Comput. Inf. Sci. 2018, 30, 431–448. [Google Scholar]
- Gholizadeh, H.; Fazlollahtabar, H.; Khalilzadeh, M. A robust fuzzy stochastic programming for sustainable procurement and logistics under hybrid uncertainty using big data. J. Clean. Prod. 2020, 258, 120640. [Google Scholar] [CrossRef]
- Cano, I.; Tenyi, A.; Vela, E.; Miralles, F.; Roca, J. Perspectives on big data applications of health information. Curr. Opin. Syst. Biol. 2017, 3, 36–42. [Google Scholar] [CrossRef]
- Habl, C.; Renner, A.T.; Bobek, J.; Laschkolnig, A. Study on Big Data in Public Health, Telemedicine and Healthcare; European Commission: Brussels, Belgium, 2016. [Google Scholar]
- Shakhovska, N.; Fedushko, S.; Greguš ml, M.; Melnykova, N.; Shvorob, I.; Syerov, Y. Big Data analysis in development of personalized medical system. Procedia Comput. Sci. 2019, 160, 229–234. [Google Scholar] [CrossRef]
- Zhou, C.; Li, A.; Hou, A.; Zhang, Z.W.; Zhang, Z.H.; Dai, P.; Wang, F. Modeling Methodology for Early Warning of Chronic Heart Failure Based on Real Medical Big Data. Expert Syst. Appl. 2020, 151, 113361. [Google Scholar] [CrossRef]
- Frost, S. Drowning in Big Data? Reducing Information Technology Complexities and Costs for Healthcare Organizations; Frost & Sullivan: New York, NY, USA, 2015. [Google Scholar]
- Schaeffer, C.; Booton, L.; Halleck, J.; Studeny, J.; Coustasse, A. Big data management in US hospitals: Benefits and barriers. Health Care Manag. 2017, 36, 87–95. [Google Scholar] [CrossRef]
- Galetsi, P.; Katsaliaki, K.; Kuma, S. Values, challenges and future directions of big data analytics in healthcare: A systematic review. Soc. Sci. Med. 2019, 241, 112533. [Google Scholar] [CrossRef]
- Kostkova, P.; Brewer, H.; de Lusignan, S.; Fottrell, E.; Goldacre, B.; Hart, G.; Koczan, P.; Knight, P.; Marsolier, C.; McKendry, R.A.; et al. Who owns the data? Open data for healthcare. Front. Public Health 2016, 4, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.H.; Yoon, H.-J. Medical big data: Promise and challenges. Kidney Res. Clin. Pract. 2017, 36, 3. [Google Scholar] [CrossRef] [Green Version]
- Shilo, S.; Rossman, H.; Segal, E. Axes of a revolution: Challenges and promises of big data in healthcare. Nat. Med. 2020, 26, 29–38. [Google Scholar] [CrossRef]
- Nagi, R.; Van Katwyk, S.R.; Hoffman, S.J. Limitations in a rapid environmental scan of global health research expertise point to the need for more open data. Health Res. Policy Syst. 2020, 18, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, T.B.; Detsky, A.S. The inevitable application of big data to health care. JAMA 2013, 309, 1351–1352. [Google Scholar] [CrossRef]
- Elia, G.; Polimeno, G.; Solazzo, G.; Passiante, G. A multi-dimension framework for value creation through big data. Ind. Mark. Manag. 2020, 90, 617–632. [Google Scholar] [CrossRef]
- Line, N.D.; Dogru, T.; El-Manstrly, D.; Buoye, A.; Malthouse, E.; Kandampully, J. Control, use and ownership of big data: A reciprocal view of customer big data value in the hospitality and tourism industry. Tour. Manag. 2020, 80, 104106. [Google Scholar] [CrossRef]
- Sahal, R.; Breslin, J.G.; Ali, M.I. Big data and stream processing platforms for Industry 4.0 requirements mapping for a predictive maintenance use case. J. Manuf. Syst. 2020, 54, 138–151. [Google Scholar] [CrossRef]
- Bag, S.; Wood, L.C.; Xu, L.; Dhamija, P.; Kayikci, Y. Big data analytics as an operational excellence approach to enhance sustainable supply chain performance. Resour. Conserv. Recycl. 2020, 153, 104559. [Google Scholar] [CrossRef]
- Lin, Y.K.; Lin, M.; Chen, H. Do electronic health records affect quality of care? Evidence from the HITECH Act. Inf. Syst. Res. 2019, 30, 306–318. [Google Scholar] [CrossRef] [Green Version]
- Bakken, S.; Koleck, T.A. Big Data Challenges from A Nursing Perspective, in Big Data, Big Challenges: A Healthcare Perspective; Springer: Berlin/Heidelberg, Germany, 2019; pp. 3–16. [Google Scholar]
- Banerjee, A.; Chakraborty, C.; Kumar, A.; Biswas, D. Emerging Trends in IoT and Big Data Analytics for Biomedical and Health Care Technologies. In Handbook of Data Science Approaches for Biomedical Engineering; Elsevier: Amsterdam, The Netherlands, 2020; pp. 121–152. [Google Scholar]
- Zolbanin, H.M.; Delen, D. Processing electronic medical records to improve predictive analytics outcomes for hospital readmissions. Decis. Support Syst. 2018, 112, 98–110. [Google Scholar] [CrossRef]
- Chen, P.T. Medical big data applications: Intertwined effects and effective resource allocation strategies identified through IRA-NRM analysis. Technol. Forecast. Soc. Chang. 2018, 130, 150–164. [Google Scholar] [CrossRef]
- Wong, L.; Ryan, F.S.; Christensen, L.R.; Cunningham, S.J. Factors influencing satisfaction with the process of orthodontic treatment in adult patients. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.T.; Lin, C.L.; Wu, W.N. Big data management in healthcare: Adoption challenges and implications. Int. J. Inf. Manag. 2020, 53, 102078. [Google Scholar] [CrossRef]
- Nambisan, S.; Wright, M.; Feldman, M. The digital transformation of innovation and entrepreneurship: Progress, challenges and key themes. Res. Policy 2019, 48, 103773. [Google Scholar] [CrossRef]
- Huerta, T.R.; Thompson, M.A.; Ford, E.W.; Ford, W.F. Electronic health record implementation and hospitals’ total factor productivity. Decis. Support Syst. 2013, 55, 450–458. [Google Scholar] [CrossRef]
- Thune, T.; Mina, A. Hospitals as innovators in the health-care system: A literature review and research agenda. Res. Policy 2016, 45, 1545–1557. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.T.; Mills, M.E.; Bausell, B.; Lu, M.-H. Two-stage evaluation of the impact of a nursing information system in Taiwan. Int. J. Med. Inform. 2008, 77, 698–707. [Google Scholar] [CrossRef]
- Hulsen, T.; Jamuar, S.S.; Moody, A.R.; Karnes, J.H.; Varga, O.; Hedensted, S.; Spreafico, R.; Hafler, D.A.; McKinney, E.F. From big data to precision medicine. Front. Med. 2019, 6, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, C.L.; Agarwal, R. The digitization of healthcare: Boundary risks, emotion, and consumer willingness to disclose personal health information. Inf. Syst. Res. 2011, 22, 469–490. [Google Scholar] [CrossRef]
- Price, W.N.; Cohen, I.G. Privacy in the age of medical big data. Nat. Med. 2019, 25, 37–43. [Google Scholar] [CrossRef]
- McLeod, R.W. Human factors in barrier management: Hard truths and challenges. Process. Saf. Environ. Prot. 2017, 110, 31–42. [Google Scholar] [CrossRef]
- Shahbaz, M.; Gao, C.; Zhai, L.; Shahzad, F.; Hu, Y. Investigating the adoption of big data analytics in healthcare: The moderating role of resistance to change. J. Big Data 2019, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Blijleven, V.; Koelemeijer, K.; Wetzels, M.; Jasper, M. Workarounds emerging from electronic health record system usage: Consequences for patient safety, effectiveness of care, and efficiency of care. JMIR Hum. Factors 2017, 4, e27. [Google Scholar] [CrossRef]
- Luo, J.; Wu, M.; Gopukumar, D.; Zhao, Y.Q. Big data application in biomedical research and health care: A literature review. Biomed. Inform. Insights 2016, 8. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Li, Y.J.; Liu, Q.Q.; Li, L.; Feng, A.; Wang, T.Y.; Zheng, S.; Xu, A.; Lyu, J. Brief introduction of medical database and data mining technology in big data era. J. Evid. Based Med. 2020, 13, 57–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sligo, J.; Gauld, R.; Roberts, V.; Villa, L. A literature review for large-scale health information system project planning, implementation and evaluation. Int. J. Med. Inform. 2017, 97, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Piri, S. Missing care: A framework to address the issue of frequent missing values the case of a clinical decision support system for Parkinson’s disease. Decis. Support Syst. 2020, 136, 113339. [Google Scholar] [CrossRef]
- Shortreed, S.M.; Cook, A.J.; Coley, R.Y.; Bobb, J.F.; Nelson, J.C. Challenges and opportunities for using big health care data to advance medical science and public health. Am. J. Epidemiol. 2019, 188, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M.; Wehrens, R.; de Bont, A. Epistemic virtues and data-driven dreams: On sameness and difference in the epistemic cultures of data science and psychiatry. Soc. Sci. Med. 2020, 258, 113116. [Google Scholar] [CrossRef] [PubMed]
- Jee, K.; Kim, G.H. Potentiality of big data in the medical sector: Focus on how to reshape the healthcare system. Healthc. Inform. Res. 2013, 19, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Kingori, P.; Gerrets, R. Morals, morale and motivations in data fabrication: Medical research fieldworkers views and practices in two Sub-Saharan African contexts. Soc. Sci. Med. 2016, 166, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Kong, X.; Feng, M.; Wang, R. The current status and challenges of establishment and utilization of medical big data in China. Eur. Geriatr. Med. 2015, 6, 515–517. [Google Scholar] [CrossRef]
- Lee-Post, A.; Pakath, R. Numerical, secondary Big Data quality issues, quality threshold establishment, & guidelines for journal policy development. Decis. Support Syst. 2019, 126, 113135. [Google Scholar]
- Ghasemaghaei, M.; Calic, G. Can big data improve firm decision quality? The role of data quality and data diagnosticity. Decis. Support Syst. 2019, 120, 38–49. [Google Scholar] [CrossRef]
- Mehta, N.; Pandit, A. Concurrence of big data analytics and healthcare: A systematic review. Int. J. Med. Inform. 2018, 114, 57–65. [Google Scholar] [CrossRef]
- Fareed, N.; Bazzoli, G.J.; Mick, S.S.F.; Harless, D.W. The influence of institutional pressures on hospital electronic health record presence. Soc. Sci. Med. 2015, 133, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Chute, C.G.; Ullman-Cullere, M.; Wood, G.M.; Lin, S.M.; He, M.; Pathak, J. Some experiences and opportunities for big data in translational research. Genet. Med. 2013, 15, 802–809. [Google Scholar] [CrossRef] [Green Version]
- Raghupathi, W.; Raghupathi, V. Big data analytics in healthcare: Promise and potential. Health Inf. Sci. Syst. 2014, 2, 3. [Google Scholar] [CrossRef]
- Wills, M.J. Decisions through data: Analytics in healthcare. J. Healthc. Manag. 2014, 59, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Halamka, J.D. Early experiences with big data at an academic medical center. Health Aff. 2014, 33, 1132–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, C.; Schreyoegg, J.; von Reitzenstein, C. The moderating role of internal and external resources on the performance effect of multitasking: Evidence from the R&D performance of surgeons. Res. Policy 2013, 42, 1356–1365. [Google Scholar]
- Roski, J.; Bo-Linn, G.W.; Andrews, T.A. Creating value in health care through big data: Opportunities and policy implications. Health Aff. 2014, 33, 1115–1122. [Google Scholar] [CrossRef]
- Lovis, C. Unlocking the Power of Artificial Intelligence and Big Data in Medicine. J. Med. Internet Res. 2019, 21, e16607. [Google Scholar] [CrossRef] [PubMed]
- Garrety, K.; McLoughlin, I.; Wilson, R.; Zelle, G.; Martin, M. National electronic health records and the digital disruption of moral orders. Soc. Sci. Med. 2014, 101, 70–77. [Google Scholar] [CrossRef] [Green Version]
- McMahon, A.; Buyx, A.; Prainsack, B. Big data governance needs more collective responsibility: The role of harm mitigation in the governance of data use in medicine and beyond. Med. Law Rev. 2020, 28, 155–182. [Google Scholar] [CrossRef] [Green Version]
- Chang, R.M.; Kauffman, R.J.; Kwon, Y. Understanding the paradigm shift to computational social science in the presence of big data. Decis. Support Syst. 2014, 63, 67–80. [Google Scholar] [CrossRef]
- Car, J.; Sheikh, A.; Wicks, P.; Williams, M.S. Beyond the Hype of Big Data and Artificial Intelligence: Building Foundations for Knowledge and Wisdom; BioMed Central: London, UK, 2019. [Google Scholar]
- Gagnon, M.P.; Simonyan, D.; Ghandour, E.K.; Godin, G. Factors influencing electronic health record adoption by physicians: A multilevel analysis. Int. J. Inf. Manag. 2016, 36, 258–270. [Google Scholar] [CrossRef]
- Ram, S.; Sheth, J.N. Consumer resistance to innovations: The marketing problem and its solutions. J. Consum. Mark. 1989, 6, 5–14. [Google Scholar] [CrossRef]
- Chiu, Y.-J.; Chen, H.-C.; Tzeng, G.-H.; Shyu, J.Z. Marketing strategy based on customer behaviour for the LCD-TV. Int. J. Manag. Decis. Mak. 2006, 7, 143–165. [Google Scholar] [CrossRef]
- Liou, J.J.; Tzeng, G.H.; Chang, H.C. Airline safety measurement using a hybrid model. J. Air Transp. Manag. 2007, 13, 243–249. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Li, M.-L.; Yen, T.-M.; Huang, T.-H. Analysis of adopting an integrated decision making trial and evaluation laboratory on a technology acceptance model. Expert Syst. Appl. 2010, 37, 1745–1754. [Google Scholar] [CrossRef]
- Horng, J.S.; Liu, C.-H.S.; Chou, S.-F.; Tsai, C.-Y.; Hu, D.-C. Developing a sustainable service innovation framework for the hospitality industry. Int. J. Contemp. Hosp. Manag. 2018, 30, 455–474. [Google Scholar] [CrossRef]
- Martilla, J.A.; James, J.C. Importance-performance analysis. J. Mark. 1977, 41, 77–79. [Google Scholar] [CrossRef]
- Tzeng, G.H.; Chiang, C.H.; Li, C.W. Evaluating intertwined effects in e-learning programs: A novel hybrid MCDM model based on factor analysis and DEMATEL. Expert Syst. Appl. 2007, 32, 1028–1044. [Google Scholar] [CrossRef]
- Wang, L.; Jones, R. Big Data, Cybersecurity, and Challenges in Healthcare. In Proceedings of the 2019 SoutheastCon, Huntsville, AL, USA, 11–14 April 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 1–6. [Google Scholar]
- McLeod, A.; Dolezel, D. Cyber-analytics: Modeling factors associated with healthcare data breaches. Decis. Support Syst. 2018, 108, 57–68. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coder 1 | Coder 2 | ||
|---|---|---|---|
| Coder 3 | 0.88 | 0.79 | |
| Coder 2 | 0.87 | - | |
| Average mutual agreement: 0.85 | Reliability: 0.94 | ||
| Background | Number of Samples | Ratio |
|---|---|---|
| Physicians | 16 | 27% |
| Medical Staff | 31 | 53% |
| Scholars | 12 | 20% |
| Total | 59 | 100% |
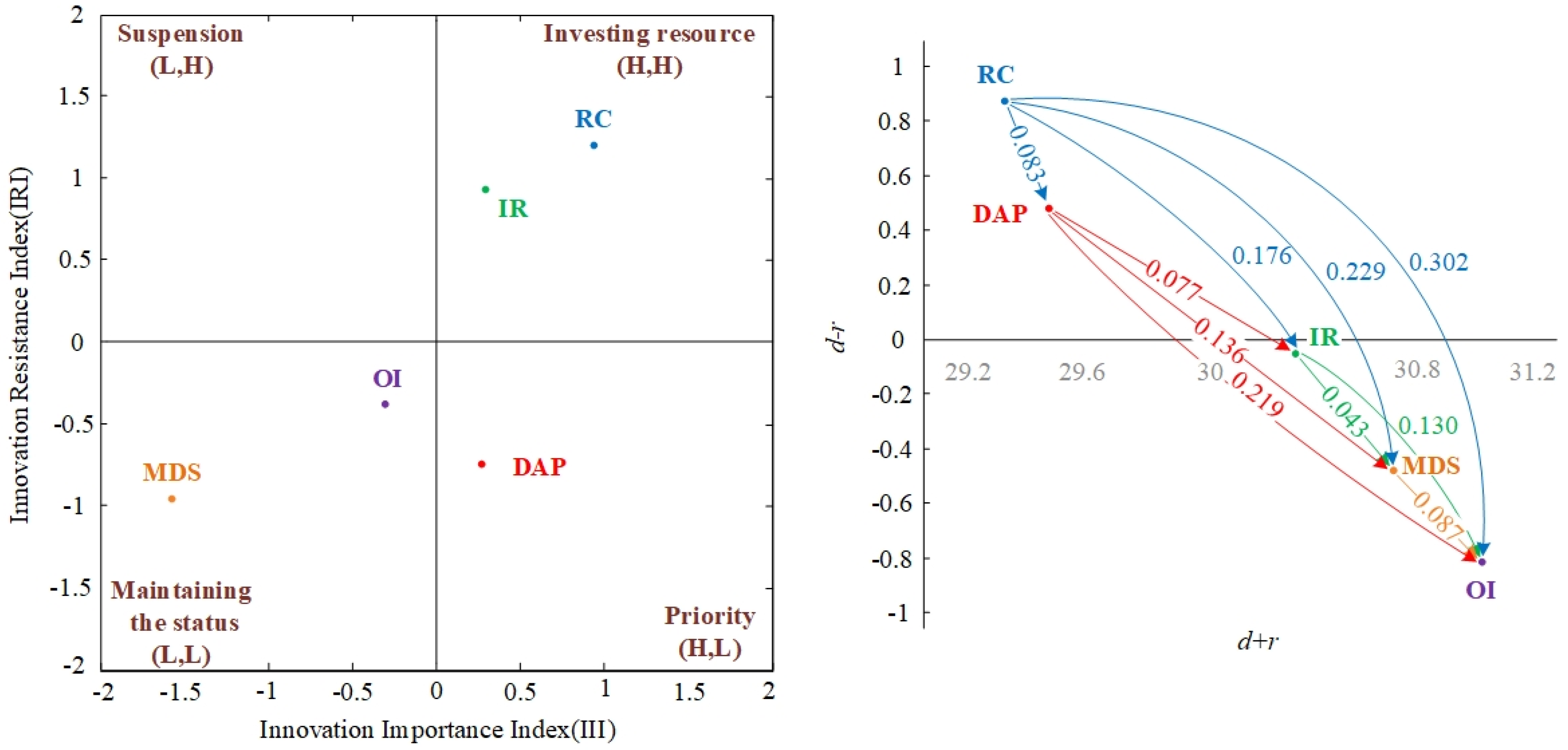
| Dimensions | IRA | NRM | Strategy | ||||
|---|---|---|---|---|---|---|---|
| III | IRI | (III, IRI) | d + r | d − r | (d + r, d − r) | ||
| Digitalized analysis and process | 0.312 | −0.896 | (H, L) | 30.978 | 0.349 | (+,+) | Priority |
| Medical data sharing | −1.627 | −0.961 | (L, L) | 32.033 | −0.321 | (+,−) | Maintaining the status |
| Infrastructure resources | 0.312 | 0.748 | (H, H) | 31.734 | −0.080 | (+,−) | Investing resources |
| Regulation and constraints | 1.074 | 1.296 | (H, H) | 30.870 | 0.790 | (+,+) | Investing resources |
| Operational issue | −0.071 | −0.187 | (L, L) | 32.4469 | −0.7373 | (+,−) | Maintaining the status |
| Net Influence Matrix | DAP | MDS | IR | RC | OI |
|---|---|---|---|---|---|
| Digitalized analysis and process | - | ||||
| Medical data sharing | −0.136 | - | |||
| Infrastructure resources | −0.077 | 0.043 | - | ||
| Regulation and constraints | 0.083 | 0.229 | 0.176 | - | |
| Operational issue | −0.219 | −0.087 | −0.130 | −0.302 | - |
| III | IRI | |
|---|---|---|
| Rank | RC[1] > IR[2] > DAP[3] > OI[4] > MDS[5] | MDS[1] > DAP[2] > OI[3] > IR[4] > RC[5] |
| Improvement paths |
|
|
| Recommended pathway |
| |
| Applications | IRA | NRM | Strategy | ||||
|---|---|---|---|---|---|---|---|
| III | IRI | (III, IRI) | d + r | d − r | (d + r, d − r) | ||
| Cooperation of the personnel | 0.605 | 1.268 | (H, H) | 35.923 | 1.022 | (+,+) | Investing resources |
| Analysis ability | −0.928 | −0.887 | (L, L) | 35.034 | 0.343 | (+,+) | Maintaining the status |
| Data application | −0.766 | −0.707 | (L, L) | 36.407 | −0.998 | (+,−) | Maintaining the status |
| Interdisciplinary team communication | 1.089 | 0.325 | (H, H) | 36.186 | −0.367 | (+,−) | Investing resources |
| Net Influence Matrix | DAP1 | DAP2 | DAP3 | DAP4 |
|---|---|---|---|---|
| Cooperation of the personnel | - | |||
| Analysis ability | −0.174 | - | ||
| Data application | −0.502 | −0.336 | - | |
| Interdisciplinary team communication | −0.345 | −0.181 | 0.159 | - |
| III | IRI | |
|---|---|---|
| Rank | DAP4[1] > DAP1[2] > DAP3[3] > DAP2[4] | DAP2[1] > DAP3[2] >DAP4[3] > DAP1[4] |
| Improvement paths |
|
|
| Recommended pathway |
| |
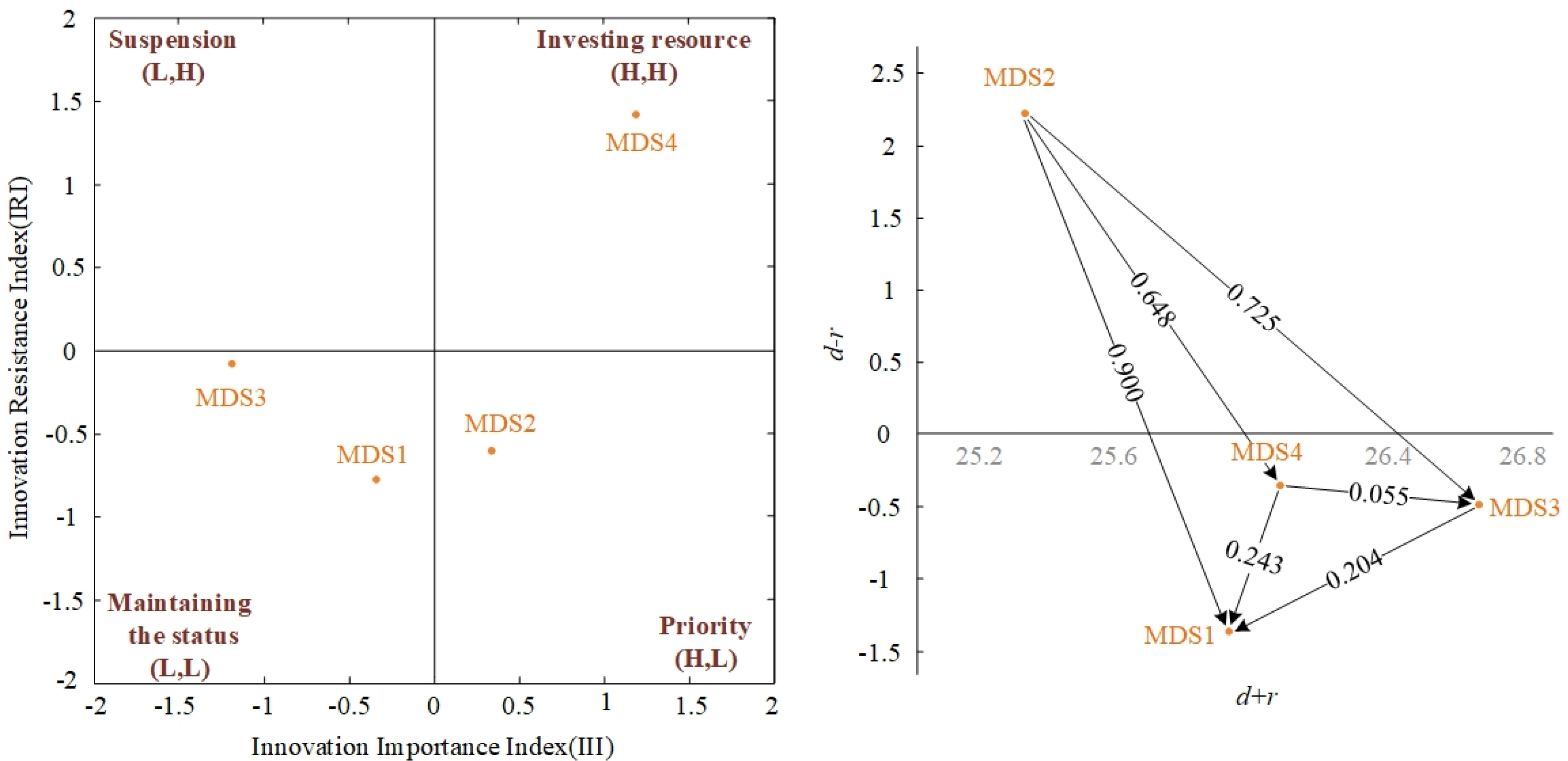
| Applications | IRA | NRM | Strategy | ||||
|---|---|---|---|---|---|---|---|
| III | IRI | (III, IRI) | d + r | d − r | (d + r, d − r) | ||
| Data collection | −0.308 | −0.670 | (L, L) | 28.320 | −1.346 | (+,−) | Maintaining the status |
| Patient cooperation | 0.286 | −0.633 | (H, L) | 27.558 | 2.273 | (+,+) | Priority |
| Information accessibility | −1.177 | −0.156 | (L, L) | 29.033 | −0.576 | (+,−) | Maintaining the status |
| Willingness of sharing | 1.199 | 1.458 | (H, H) | 28.374 | −0.351 | (+,−) | Investing resources |
| Net Influence Matrix | MDS1 | MDS2 | MDS3 | MDS4 |
|---|---|---|---|---|
| Data collection | - | |||
| Patient cooperation | 0.900 | - | ||
| Information accessibility | 0.204 | −0.725 | - | |
| Sharing will | 0.243 | −0.648 | 0.055 | - |
| III | IRI | |
|---|---|---|
| Rank | MDS4[1] > MDS2[2] > MDS1[3] > MDS3[4] | MDS1[1] > MDS2[2] > MDS3[3] > MDS4[4] |
| Improvement paths |
|
|
| Recommended pathway |
| |
| Applications | IRA | NRM | Strategy | ||||
|---|---|---|---|---|---|---|---|
| III | IRI | (III, IRI) | d + r | d − r | (d + r, d − r) | ||
| Technical resources demand | −1.085 | −1.038 | (L, L) | 14.291 | 0.938 | (+,+) | Maintaining the status |
| Information reliability | −0.613 | −0.552 | (L, L) | 12.905 | −0.478 | (+,−) | Maintaining the status |
| Implementation costs | 0.802 | 0.376 | (H, H) | 13.352 | −0.474 | (+,−) | Investing resources |
| Faculty loading | 0.896 | 1.215 | (H, H) | 14.205 | 0.014 | (+,+) | Investing resources |
| Net Influence Matrix | IR1 | IR2 | IR | IR4 |
|---|---|---|---|---|
| Technical resources demand | - | |||
| Information reliability | −0.339 | - | ||
| Implementation costs | −0.350 | 0.005 | - | |
| Faculty loading | −0.249 | 0.135 | 0.128 | - |
| III | IRI | |
|---|---|---|
| Improvement paths |
|
|
| Recommended pathway |
| |
| Applications | IRA | NRM | Strategy | ||||
|---|---|---|---|---|---|---|---|
| III | IRI | (III, IRI) | d + r | d − r | (d + r, d − r) | ||
| Regulation vagueness | 0.705 | 1.012 | (H, H) | 15.507 | 1.186 | (+,+) | Investing resources |
| Data accessibility | −1.416 | −1.287 | (L, L) | 15.280 | −0.305 | (+,−) | Maintaining the status |
| Data usage | 0.705 | −0.237 | (H, L) | 15.383 | −0.832 | (+,−) | Priority |
| Medical malpractice liability | 0.005 | 0.512 | (H, H) | 14.587 | −0.049 | (+,−) | Investing resources |
| Net Influence Matrix | RC1 | RC2 | RC3 | RC4 |
|---|---|---|---|---|
| Regulation vagueness | - | |||
| Data accessibility | −0.388 | - | ||
| Data usage | −0.511 | −0.142 | - | |
| Medical malpractice liability | −0.287 | 0.060 | 0.179 | - |
| III | IRI | |
|---|---|---|
| Rank | RC1[1] = RC3[1] > RC4[2] > RC2[3] | RC2[1] > RC3[2] > RC4[3] > RC1[4] |
| Improvement paths |
|
|
| Recommended pathway |
| |
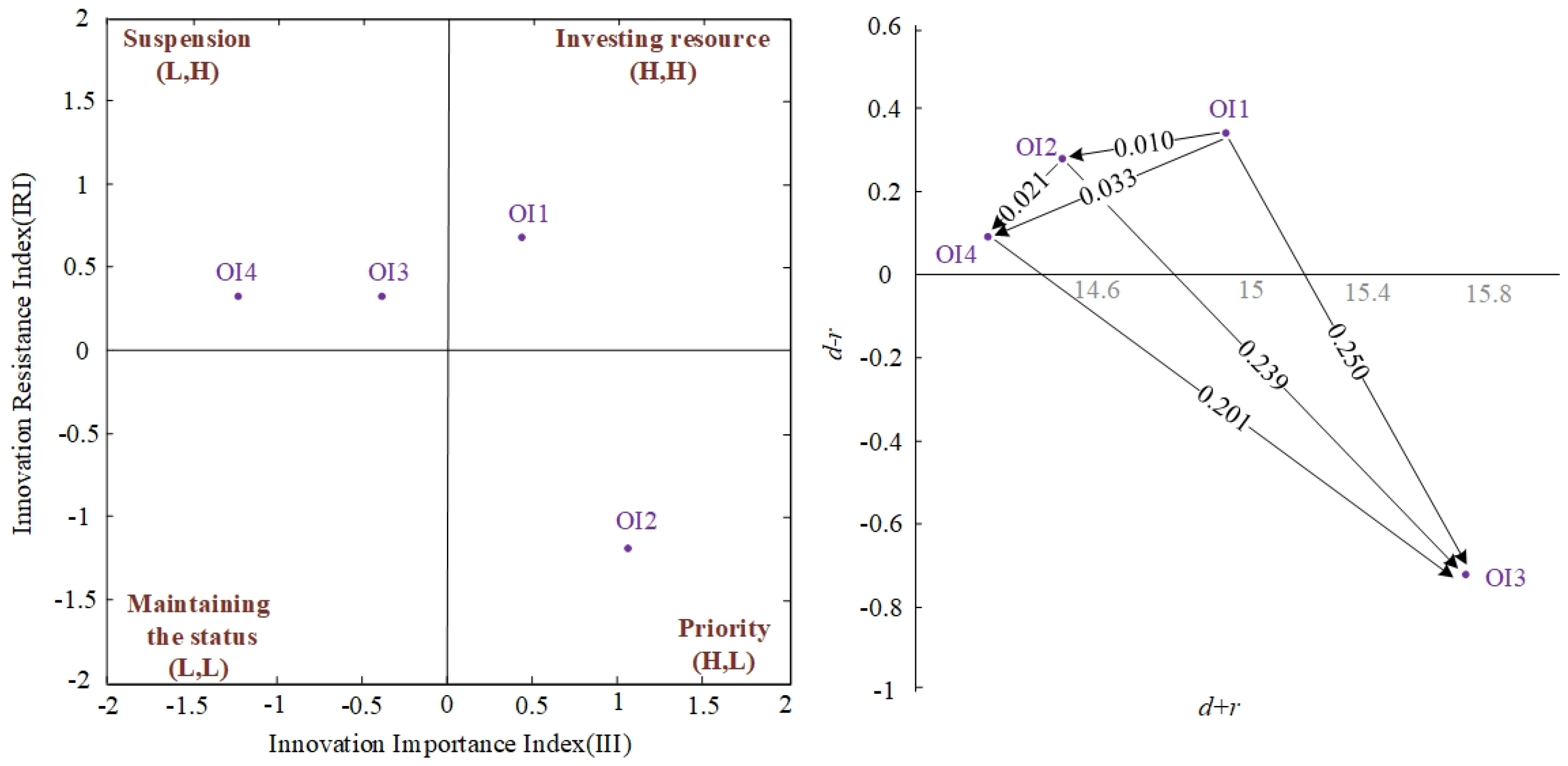
| Applications | IRA | NRM | Strategy | ||||
|---|---|---|---|---|---|---|---|
| III | IRI | (III, IRI) | d + r | d − r | (d + r, d − r) | ||
| Differences between divisions | 1.160 | 0.789 | (H, H) | 14.844 | 0.293 | (+,+) | Investing resources |
| Patients’ privacy | 0.311 | −1.466 | (H, L) | 14.424 | 0.249 | (+,+) | Priority |
| Worries regarding value-added service | −0.247 | 0.338 | (L, H) | 15.616 | −0.690 | (+,−) | Suspension |
| Lacking incentives | −1.224 | 0.338 | (L, H) | 14.313 | 0.148 | (+,+) | Suspension |
| Net Influence Matrix | OI1 | OI2 | OI3 | OI4 |
|---|---|---|---|---|
| Differences between divisions | - | |||
| Patients’ privacy | −0.010 | - | ||
| Worries regarding value-added service | −0.250 | −0.239 | - | |
| Lacking incentives | −0.033 | −0.021 | 0.201 | - |
| III | IRI | |
|---|---|---|
| Rank | OI2[1] > OI1[2] > OI3[3] > OI4[4] | OI2[1] > OI3[2] = OI4[2] > OI1[3] |
| Improvement paths |
|
|
| Recommended pathway |
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, W.-C.; Tsai, I.-C.; Wang, K.-C.; Tang, T.-A.; Li, K.-C.; Ke, Y.-C.; Chen, P.-T. Innovation Resistance and Resource Allocation Strategy of Medical Information Digitalization. Sustainability 2021, 13, 7888. https://doi.org/10.3390/su13147888
Lu W-C, Tsai I-C, Wang K-C, Tang T-A, Li K-C, Ke Y-C, Chen P-T. Innovation Resistance and Resource Allocation Strategy of Medical Information Digitalization. Sustainability. 2021; 13(14):7888. https://doi.org/10.3390/su13147888
Chicago/Turabian StyleLu, Wei-Chih, I-Ching Tsai, Kuan-Chung Wang, Te-Ai Tang, Kuan-Chen Li, Ya-Ci Ke, and Peng-Ting Chen. 2021. "Innovation Resistance and Resource Allocation Strategy of Medical Information Digitalization" Sustainability 13, no. 14: 7888. https://doi.org/10.3390/su13147888