
Anterior Lumbar Interbody Fusion (ALIF) for Lumbar Hemivertebra in an Adult Using Three-Dimensional-Printed Patient-Specific Implants and Virtual Surgery Planning: A Technical Report
 , and
, and
Abstract
:1. Introduction
2. Technical Note
2.1. Case Presentation
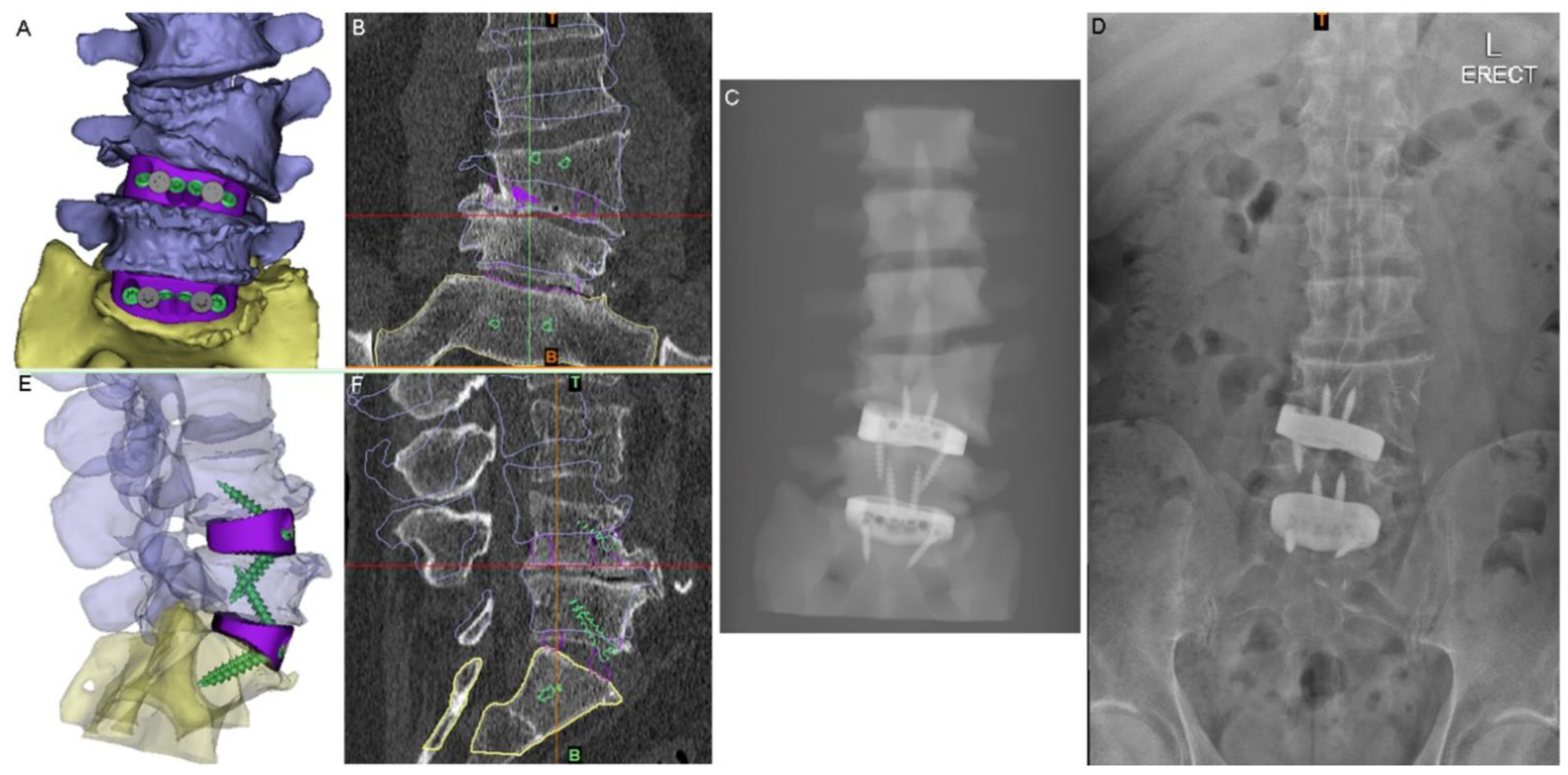
2.2. Surgical Planning and Implant Design
2.3. Surgery
2.4. Clinical Follow-Up
3. Discussion
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 3D | Three-Dimensional |
| 3DP | Three-Dimensional Printing |
| ABS | Acrylonitrile Butadiene Styrene |
| ALIF | Anterior Lumbar Interbody Fusion |
| AP | Anteroposterior |
| CT | Computed Tomography |
| MRI | Magnetic Resonance Imaging |
| NSURG | NeuroSpine Surgery Research Group |
| NSW | New South Wales |
| OTS | Off-The-Shelf |
| ODI | Oswestry Disability Index |
| PSIs | Patient-Specific Implants |
| SORL | Surgical and Orthopaedic Research Labs |
| UNSW | University of New South Wales |
| USA | United States of America |
| VAS | Visual Analogue Scale |
| VSP | Virtual Surgery Planning |
References
- Steinmetz, M.P.; Benzel, E.C. Benzel’s Spine Surgery E-Book: Techniques, Complication Avoidance, and Management; Elsevier Health Sciences: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Johal, J.; Loukas, M.; Fisahn, C.; Chapman, J.R.; Oskouian, R.J.; Tubbs, R.S. Hemivertebrae: A comprehensive review of embryology, imaging, classification, and management. Child’s Nerv. Syst. 2016, 32, 2105–2109. [Google Scholar] [CrossRef] [PubMed]
- Bao, B.; Yan, H.; Tang, J. A review of the hemivertebrae and hemivertebra resection. Br. J. Neurosurg. 2020, 36, 546–554. [Google Scholar] [CrossRef]
- McMaster, M.J.; Ohtsuka, K. The natural history of congenital scoliosis. A study of two hundred and fifty-one patients. J. Bone Jt. Surg Am. 1982, 64, 1128–1147. [Google Scholar] [CrossRef]
- Bollini, G.; Docquier, P.-L.; Viehweger, E.; Launay, F.; Jouve, J.-L. Lumbar Hemivertebra Resection. J. Bone Jt. Surg. Am. 2006, 88, 1043–1052. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.E.; Lenke, L.G. Adult degenerative scoliosis: Evaluation and management. Neurosurg. Focus 2010, 28, E1. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, B.; Mobbs, R.J.; Wu, A.-M.; Phan, K. Systematic review of 3D printing in spinal surgery: The current state of play. J. Spine Surg. 2017, 3, 433–443. [Google Scholar] [CrossRef]
- Parr, W.C.H.; Burnard, J.L.; Wilson, P.J.; Mobbs, R.J. 3D printed anatomical (bio)models in spine surgery: Clinical benefits and value to health care providers. J. Spine Surg. 2019, 5, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lim, J.-Y.; Shim, K.-W.; Han, J.W.; Yi, S.; Yoon, D.H.; Kim, K.N.; Ha, Y.; Ji, G.Y.; Shin, D.A. Sacral Reconstruction with a 3D-Printed Implant after Hemisacrectomy in a Patient with Sacral Osteosarcoma: 1-Year Follow-Up Result. Yonsei Med. J. 2017, 58, 453–457. [Google Scholar] [CrossRef]
- Xu, N.; Wei, F.; Liu, X.; Jiang, L.; Cai, H.; Li, Z.; Yu, M.; Wu, F.; Liu, Z. Reconstruction of the Upper Cervical Spine Using a Personalized 3D-Printed Vertebral Body in an Adolescent With Ewing Sarcoma. Spine 2016, 41, E50–E54. [Google Scholar] [CrossRef]
- Siu, T.L.; Rogers, J.M.; Lin, K.; Thompson, R.; Owbridge, M. Custom-Made Titanium 3-Dimensional Printed Interbody Cages for Treatment of Osteoporotic Fracture–Related Spinal Deformity. World Neurosurg. 2018, 111, 1–5. [Google Scholar] [CrossRef]
- Sheha, E.D.; Gandhi, S.D.; Colman, M.W. 3D printing in spine surgery. Ann. Transl. Med. 2019, 7 (Suppl. S5), S164. [Google Scholar] [CrossRef] [PubMed]
- Wallace, N.; Schaffer, N.E.; Aleem, I.S.M.; Patel, R. 3D-printed Patient-specific Spine Implantss: A systematic review. Clin. Spine Surgery A Spine Publ. 2020, 33, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Amin, T.; Parr, W.C.; Mobbs, R.J. Opinion Piece: Patient-Specific Implants May Be the Next Big Thing in Spinal Surgery. J. Pers. Med. 2021, 11, 498. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Barrey, C.; Massourides, H.; Perrin, G. Lumbar Hemivertebra in an Adult Treated by Transpedicular Osteotomy. World Neurosurg. 2012, 77, 592.e5–592.e9. [Google Scholar] [CrossRef] [PubMed]
- Ruf, M.; Jensen, R.; Letko, L.; Harms, J. Hemivertebra Resection and Osteotomies in Congenital Spine Deformity. Spine 2009, 34, 1791–1799. [Google Scholar] [CrossRef] [PubMed]
- Hedden, D. Management themes in congenital scoliosis. J. Bone Jt. Surg. Am. 2007, 89 (Suppl. S1), 72–78. [Google Scholar]
- Desborough, J. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef]
- Dobson, G.P. Addressing the Global Burden of Trauma in Major Surgery. Front. Surg. 2015, 2, 43. [Google Scholar] [CrossRef]
- Ueda, K.; Turner, P.; Gagner, M. Stress response to laparoscopic liver resection. HPB 2004, 6, 247–252. [Google Scholar] [CrossRef]
- Amin, T.; Lin, H.; Parr, W.C.H.; Lim, P.; Mobbs, R.J. Revision of a Failed C5-7 Corpectomy Complicated by Esophageal Fistula Using a 3-Dimensional−Printed Zero-Profile Patient-Specific Implant: A Technical Case Report. World Neurosurg. 2021, 151, 29–38. [Google Scholar] [CrossRef]
- Parr, W.C.H.; Burnard, J.L.; Singh, T.; McEvoy, A.; Walsh, W.R.; Mobbs, R.J. C3-C5 Chordoma Resection and Reconstruction with a Three-Dimensional Printed Titanium Patient-Specific Implant. World Neurosurg. 2020, 136, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Walsh, W.R.; Pelletier, M.H.; Bertollo, N.; Lovric, V.; Wang, T.; Morberg, P.; Parr, W.C.H.; Bergadano, D. Bone ongrowth and mechanical fixation of implants in cortical and cancellous bone. J. Orthop. Surg. Res. 2020, 15, 177. [Google Scholar] [CrossRef] [PubMed]
- Polly, D.W.; Rosner, M.K.; Monacci, W.; Moquin, R.R. Thoracic hemivertebra excision in adults via a posterior-only approach. Neurosurg. Focus 2003, 14, e9. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Kaplan, D.J.; Spivak, J.M.; Bendo, J.A. Three-dimensional printing in spine surgery: A review of current applications. Spine J. 2020, 20, 833–846. [Google Scholar] [CrossRef] [PubMed]
- Girolami, M.; Boriani, S.; Bandiera, S.; Barbanti-Bródano, G.; Ghermandi, R.; Terzi, S.; Tedesco, G.; Evangelisti, G.; Pipola, V.; Gasbarrini, A. Biomimetic 3D-printed custom-made prosthesis for anterior column reconstruction in the thoracolumbar spine: A tailored option following en bloc resection for spinal tumors: Preliminary results on a case-series of 13 patients. Eur. Spine J. 2018, 27, 3073–3083. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Li, Z.; Liu, Z.; Liu, X.; Jiang, L.; Yu, M.; Xu, N.; Wu, F.; Dang, L.; Zhou, H.; et al. Upper cervical spine reconstruction using customized 3D-printed vertebral body in 9 patients with primary tumors involving C2. Ann. Transl. Med. 2020, 8, 332. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, K.; Nizak, R.; Noordmans, H.J.; Castelein, R.M.; Weinans, H.; Kruyt, M.C. Challenges in the design and regulatory approval of 3D-printed surgical implants: A two-case series. Lancet Digit. Health 2019, 1, e163–e171. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Parr, W.C.H.; Choy, W.J.; McEvoy, A.; Walsh, W.R.; Phan, K. Anterior Lumbar Interbody Fusion Using a Personalized Approach: Is Custom the Future of Implants for Anterior Lumbar Interbody Fusion Surgery? World Neurosurg. 2019, 124, 452–458.e1. [Google Scholar] [CrossRef]
- Mobbs, R.; Coughlan, M.; Thompson, R.; Sutterlin, C.E.; Phan, K. The utility of 3D printing for surgical planning and patient-specific implant design for complex spinal pathologies: Case report. J. Neurosurg. Spine 2017, 26, 513–518. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative | Postoperative | ||||
|---|---|---|---|---|---|
| Timepoint (Month) | −1 | 0 | 1 | 2 | 3 |
| Mean Total Daily Step Count (Steps/Day) | 3030 | 1398 | 1797 | 4474 | 4314 |
| Mean Gait Speed (m/s) | 1.14 | 1.22 | 1.03 | 1.06 | 1.11 |
| Mean Step Length (cm) | 68.1 | 70.6 | 67.0 | 68.0 | 69.5 |
| Mean Double Support Time (%) | 30.5 | 29.6 | 32.1 | 31.6 | 30.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amin, T.; Parr, W.C.H.; Natarajan, P.; Lennox, A.; Koinis, L.; Mobbs, R.J. Anterior Lumbar Interbody Fusion (ALIF) for Lumbar Hemivertebra in an Adult Using Three-Dimensional-Printed Patient-Specific Implants and Virtual Surgery Planning: A Technical Report. Surg. Tech. Dev. 2023, 12, 199-210. https://doi.org/10.3390/std12040019
Amin T, Parr WCH, Natarajan P, Lennox A, Koinis L, Mobbs RJ. Anterior Lumbar Interbody Fusion (ALIF) for Lumbar Hemivertebra in an Adult Using Three-Dimensional-Printed Patient-Specific Implants and Virtual Surgery Planning: A Technical Report. Surgical Techniques Development. 2023; 12(4):199-210. https://doi.org/10.3390/std12040019
Chicago/Turabian StyleAmin, Tajrian, William C. H. Parr, Pragadesh Natarajan, Andrew Lennox, Lianne Koinis, and Ralph J. Mobbs. 2023. "Anterior Lumbar Interbody Fusion (ALIF) for Lumbar Hemivertebra in an Adult Using Three-Dimensional-Printed Patient-Specific Implants and Virtual Surgery Planning: A Technical Report" Surgical Techniques Development 12, no. 4: 199-210. https://doi.org/10.3390/std12040019