
Posterior Cervical Unilateral Biportal Endoscopic One-Block Resection Technique for Cervical Ossified Ligamentum Flavum


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Relevant Surgical Anatomy
2. Technique Description
2.1. Clinical Examination and Radiological Investigation for Identifying the Cause of Cervical Myelopathy
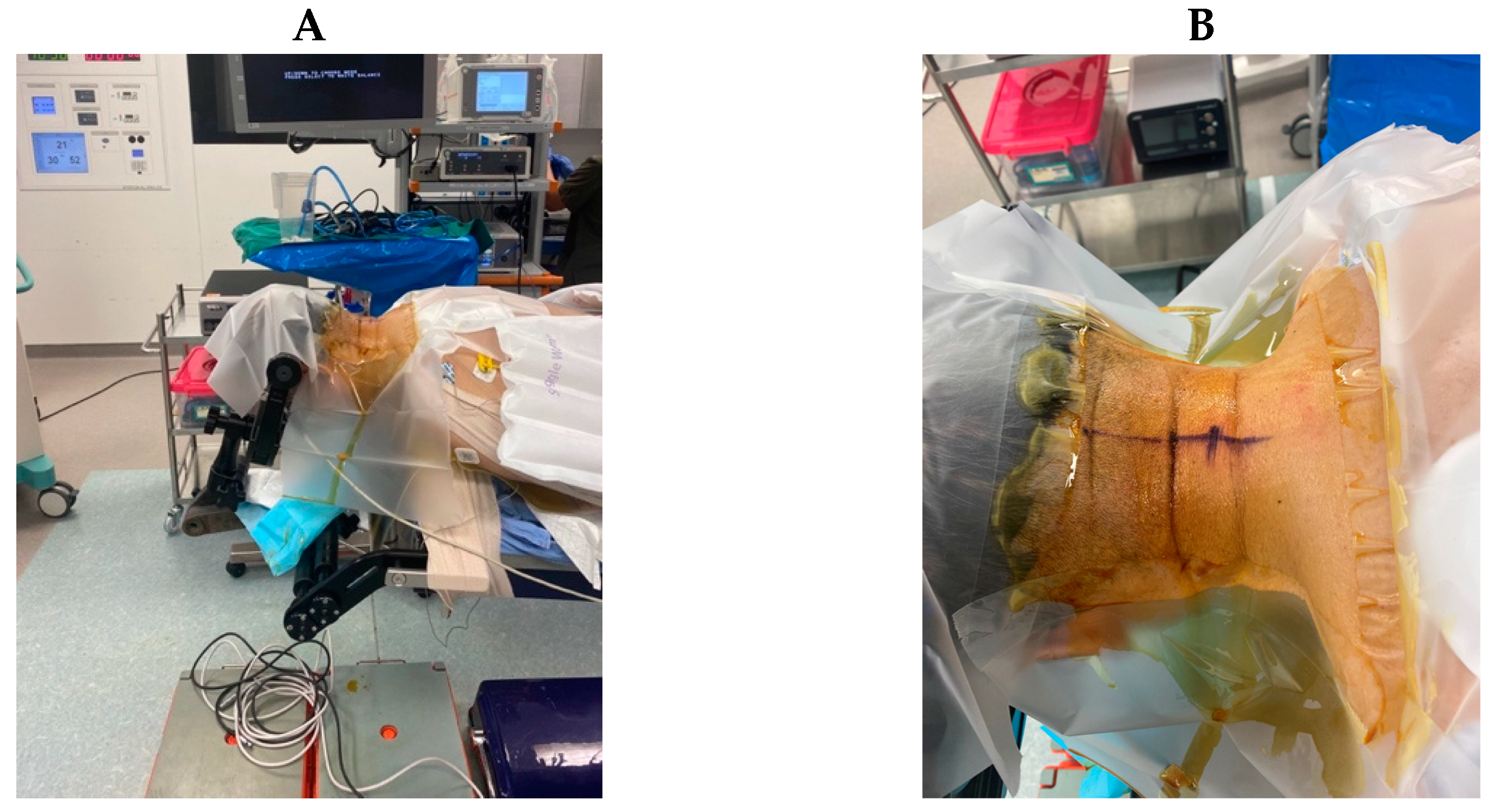
2.2. Anesthesia and Positioning
2.3. Skin Marking
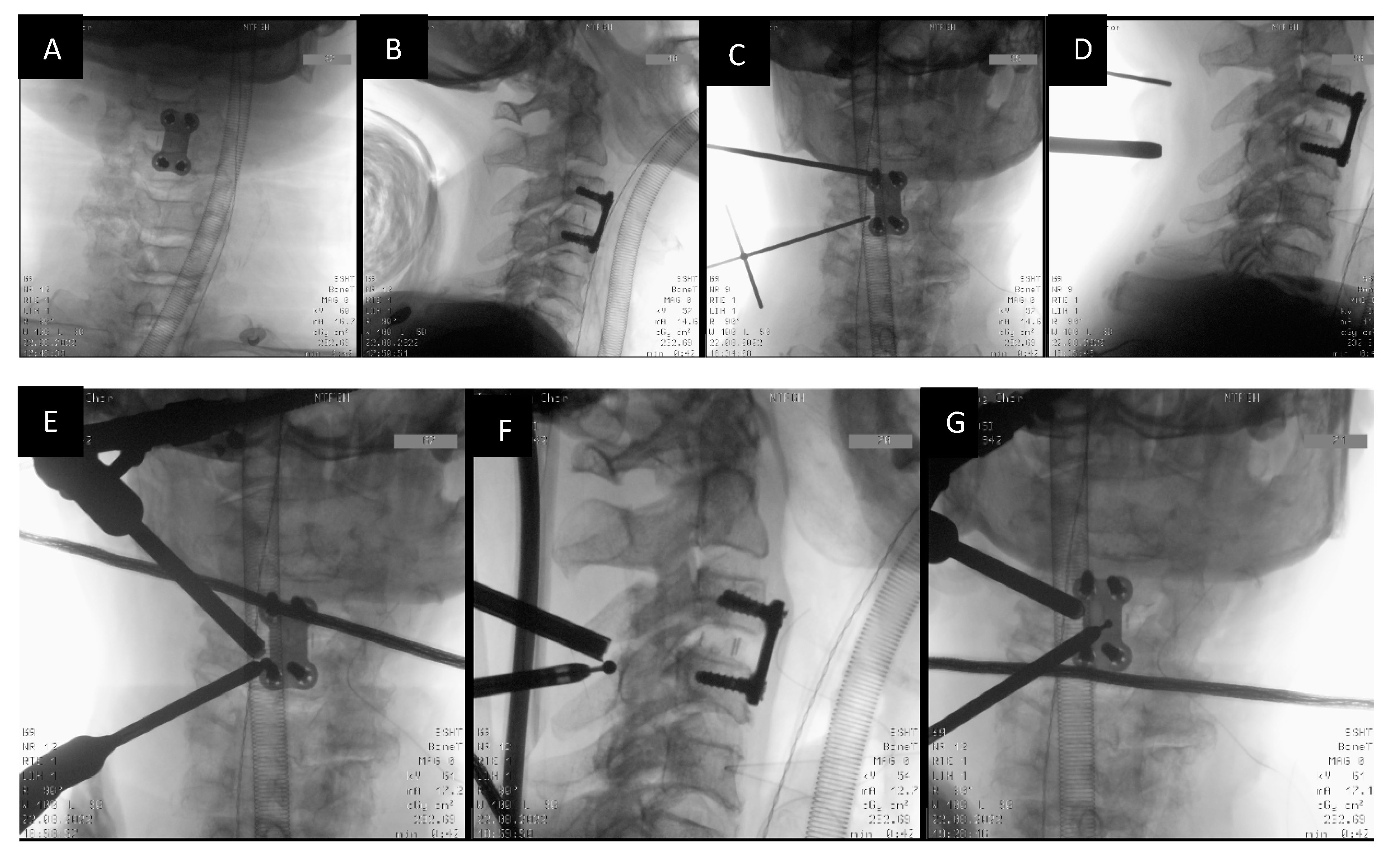
2.4. Docking and Working Channel Placement
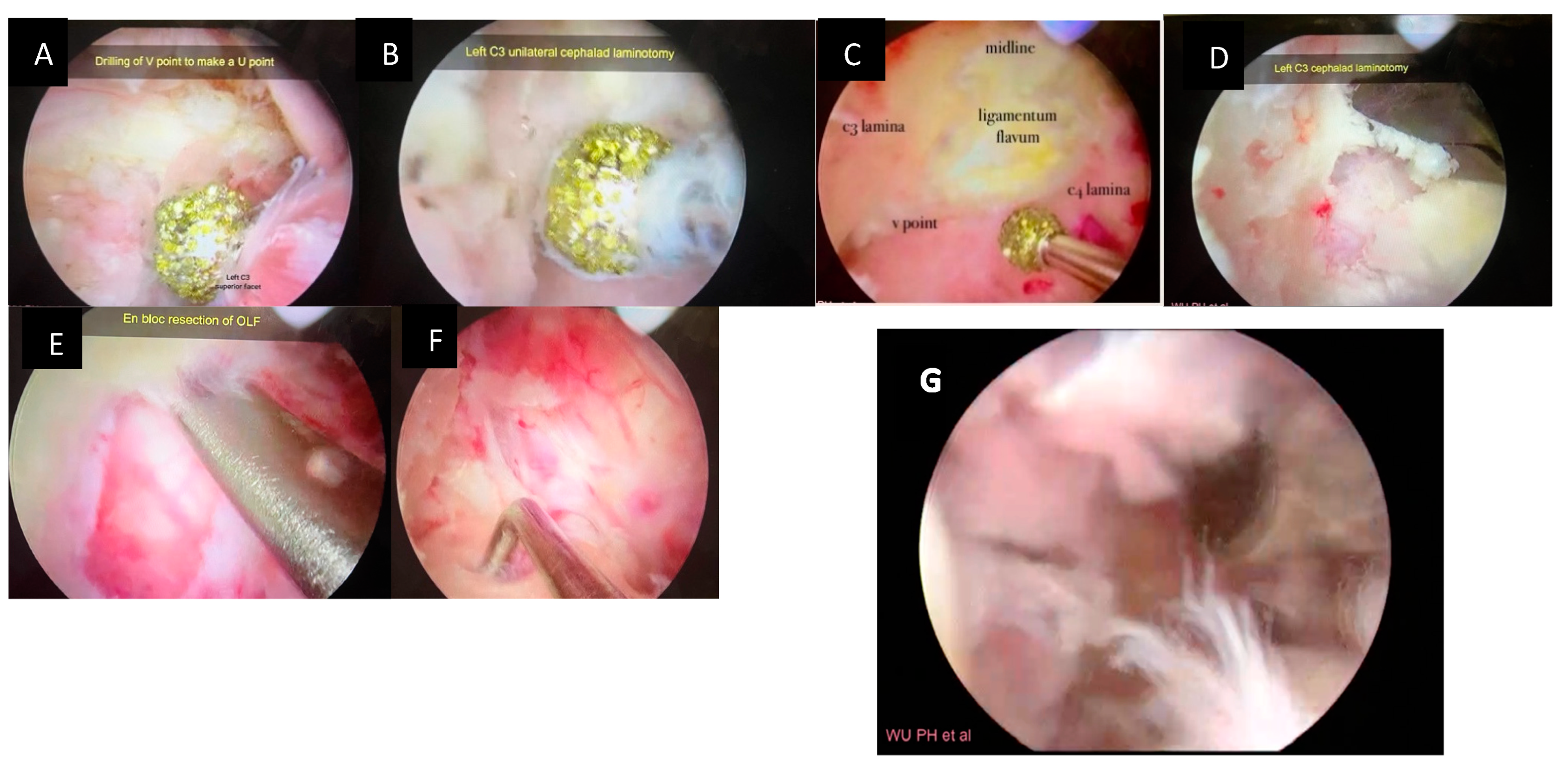
2.5. Identification of the V Point
2.6. Drilling of the Ipsilateral Lamina and Laminectomy
2.7. Sublaminar Drilling of the Contralateral Lamina
2.8. Detaching the Ligamentum Flavum en Bloc
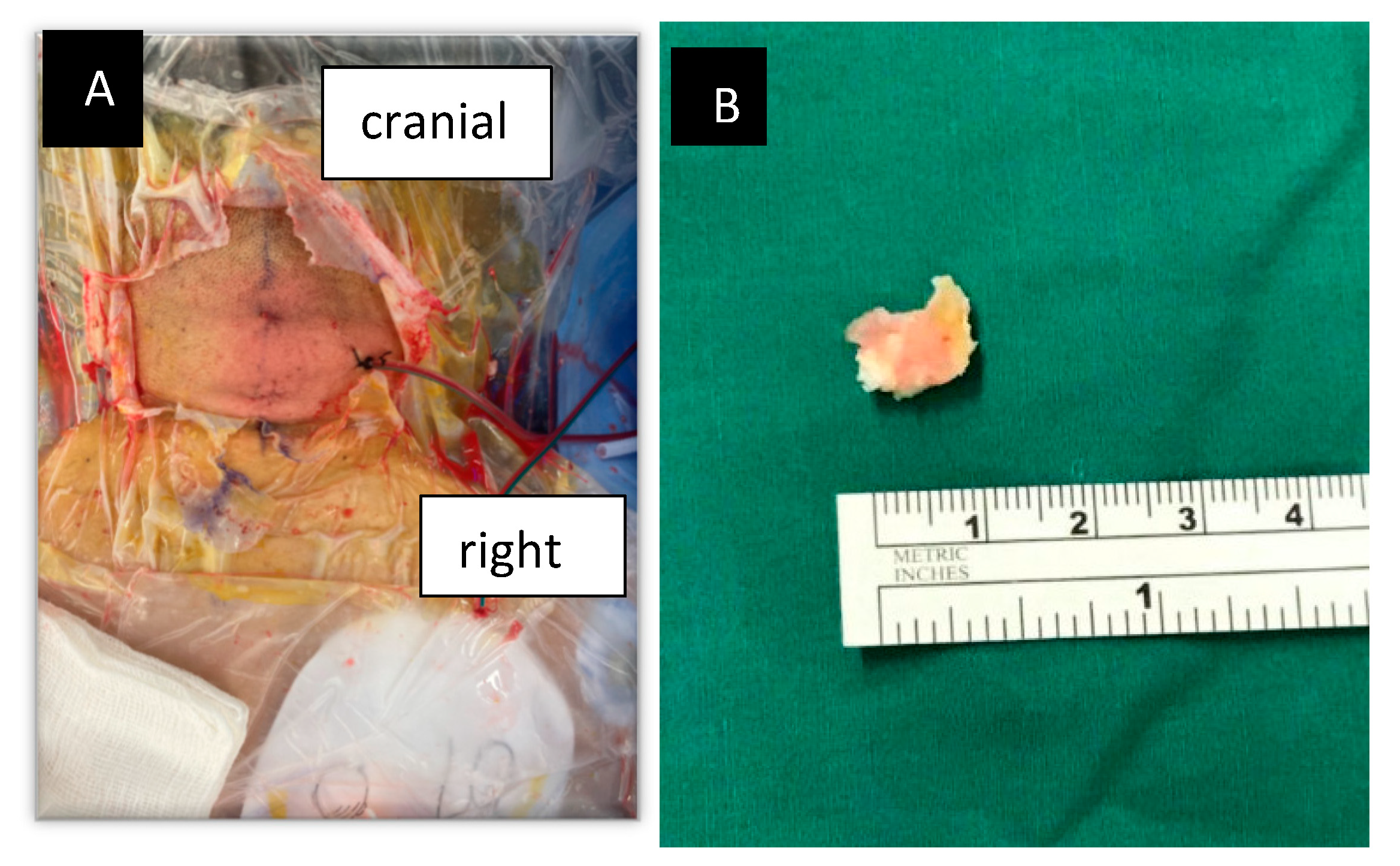
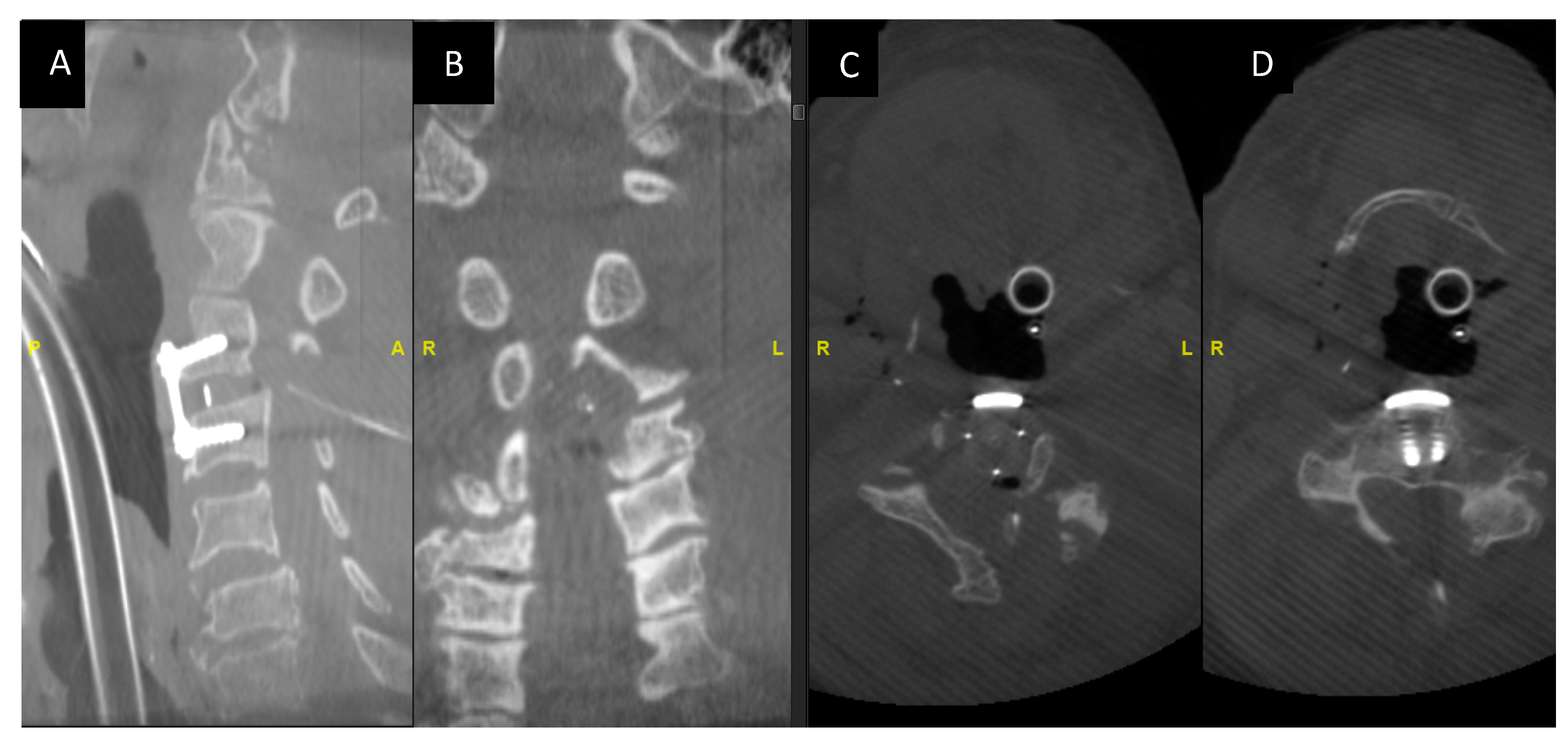
2.9. Confirmation of Decompression Using Intraoperative Computer Tomographic (O Arm) SCAN
2.10. Wound Closure with Drain
3. Indications
4. Limitations
5. How to Avoid Complications
- Preoperative radiological imaging such as MRI for evaluating the level and extent of stenosis and myelopathy.
- Identification of the calcified ligamentum flavum on the CT scan and knowing the extent and location of the calcification.
- Using a high-speed drill to gradually thin the ossified ligamentum flavum until there is a translucent thin layer left. Before the resection of the ossified ligamentum flavum, the normal boundary of the ligamentum flavum should be clearly revealed [7].
- A technique performed through the stepwise approach can help in the identification of key anatomical structure checkpoints and in highlighting the targets for decompression required to achieve good radiological and clinical outcomes [8].
- The ligament flavum can be preserved until the bone work is finished.
- An intraoperative 3D CT scan confirming the adequacy of decompression.
6. Specific Perioperative Considerations
7. Patient Education about Surgery and the Potential Risks Involved
8. Summary of 10 Key Points
- The advantages of biportal endoscopic approaches over conventional open surgery include the preservation of the normal structures, less intraoperative bleeding and fast postoperative recovery [9].
- Biportal endoscopy allows for a direct, magnified and closeup view of the pathology.
- Systematic evaluation of the MRI and CT scans to plan the surgery.
- Usage of intraoperative fluoroscopy to localize the drilling and the extent of decompression.
- Use of a 3.5 mm high-speed diamond drill to thin out the lamina, and use of dissectors and a 1 mm Kerrison for the final flavectomy.
- Before the resection of the ossified ligamentum flavum, the normal boundary of the ligamentum flavum is to be clearly revealed.
- The flavum is to be preserved until the bone work is finished.
- Hemostasis with radiofrequency is preferred rather than increasing the pump pressure. Keeping the pump pressure at 30–40 mmHg in most parts of the operation is preferred.
- Intraoperative 3D CT scan to confirm adequate decompression.
- Usage of the drain is preferred to avoid hematoma at the spinal cord level.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, S.I.; Ha, K.Y.; Lee, J.W.; Kim, Y.H. Prevalence and related clinical factors of thoracic ossification of the ligamentum flavum-a computed tomography-based cross-sectional study. Spine J. 2018, 18, 551–557. [Google Scholar] [CrossRef] [PubMed]
- Kubota, M.; Baba, I.; Sumida, T. Myelopathy due to ossification of the ligamentum flavum of the cervical spine. A report of two cases. Spine 1981, 6, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.J.; Luk, K.D.; Karppinen, J.; Yang, H.; Cheung, K.M. Prevalence, distribution, and morphology of ossification of the ligamentum flavum: A population study of one thousand seven hundred thirty-six magnetic resonance imaging scans. Spine 2010, 35, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Ahn, D.K.; Lee, S.; Moon, S.H.; Boo, K.H.; Chang, B.K.; Lee, J.I. Ossification of the ligamentum flavum. Asian Spine J. 2014, 8, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Nouri, A.; Tetreault, L.; Singh, A.; Karadimas, S.K.; Fehlings, M.G. Degenerative Cervical Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine 2015, 40, E675–E693. [Google Scholar] [CrossRef] [PubMed]
- Baron, E.M.; Young, W.F. Cervical spondylotic myelopathy: A brief review of its pathophysiology, clinical course, and diagnosis. Neurosurgery 2007, 60, S35–S41. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Rao, S.; Li, Y.; Zhao, S.; Chen, B. Posterior percutaneous full-endoscopic cervical laminectomy and decompression for cervical stenosis with myelopathy: A technical note. World Neurosurg. 2019, 124, 350357. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H.; Kim, H.S.; Lee, Y.J.; Kim, D.H.; Lee, J.H.; Yang, K.-H.; Raorane, H.D.; Jang, I.-T. Posterior endoscopic cervical foramiotomy and discectomy: Clinical and radiological computer tomography evaluation on the bony effect of decompression with 2 years follow-up. Eur. Spine J. 2021, 30, 534–546. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Heo, D.H.; Lee, D.C.; Chung, H.T. Biportal endoscopic unilateral laminotomy with bilateral decompression for the treatment of cervical spondylotic myelopathy. Acta Neurochir. 2021, 163, 2537–2543. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
George, R.; Wu, P.H. Posterior Cervical Unilateral Biportal Endoscopic One-Block Resection Technique for Cervical Ossified Ligamentum Flavum. Surg. Tech. Dev. 2023, 12, 80-86. https://doi.org/10.3390/std12020007
George R, Wu PH. Posterior Cervical Unilateral Biportal Endoscopic One-Block Resection Technique for Cervical Ossified Ligamentum Flavum. Surgical Techniques Development. 2023; 12(2):80-86. https://doi.org/10.3390/std12020007
Chicago/Turabian StyleGeorge, Rajeesh, and Pang Hung Wu. 2023. "Posterior Cervical Unilateral Biportal Endoscopic One-Block Resection Technique for Cervical Ossified Ligamentum Flavum" Surgical Techniques Development 12, no. 2: 80-86. https://doi.org/10.3390/std12020007