1. Introduction
The areas around washbasins in hospital wards used by staff and patients are contaminated by pathogenic bacteria [
1,
2]. An outbreak of drug-resistant
Acinetobacter baumannii occurred in the intensive care unit of our Advanced Emergency and Critical Care Center of Tokai University Hospital due to a biofilm of drug-resistant
Acinetobacter baumannii, which adhered to the inside of a washbasin tap and contaminated the water supply pipe for a prolonged period [
3]. Immunosuppressed patients are prone to develop opportunistic infections caused by environmental bacteria [
4]; therefore, it is important to keep washbasins, including taps, clean in hospital wards.
We conducted an environmental survey of washbasin units, including the taps, in the high-care unit (HCU, 36 beds) of the Advanced Emergency and Critical Care Center of Tokai University Hospital in 2018. We detected the presence of
Enterobacter cloacae, a carbapenem-resistant Enterobacterales (CRE), in a tap. CRE is highly drug resistant, and CRE infections lead to longer hospital stays and higher medical costs than non-CRE infections [
5]. The treatment and cure of pneumonia as well as bloodstream infections caused by CRE can be difficult owing to the limited availability of effective antibiotics, and the reported mortality is high [
6]. Furthermore, CRE has the propensity to spread via plasmids, thus posing the risk of causing nosocomial outbreaks [
7]. Therefore, the prevention of horizontal transmission of CRE is crucial for infection control.
Biofilms and scales that adhere to taps are difficult to clean because they harbor numerous bacteria [
8,
9], and some biofilms and scales contain CRE. Methods for cleaning taps effectively and efficiently remain unclear. This study aimed to investigate effective methods for cleaning and disinfecting taps using commonly used detergents and disinfectants by conducting a bacteriological survey for areas around washbasins, including taps.
2. Materials and Methods
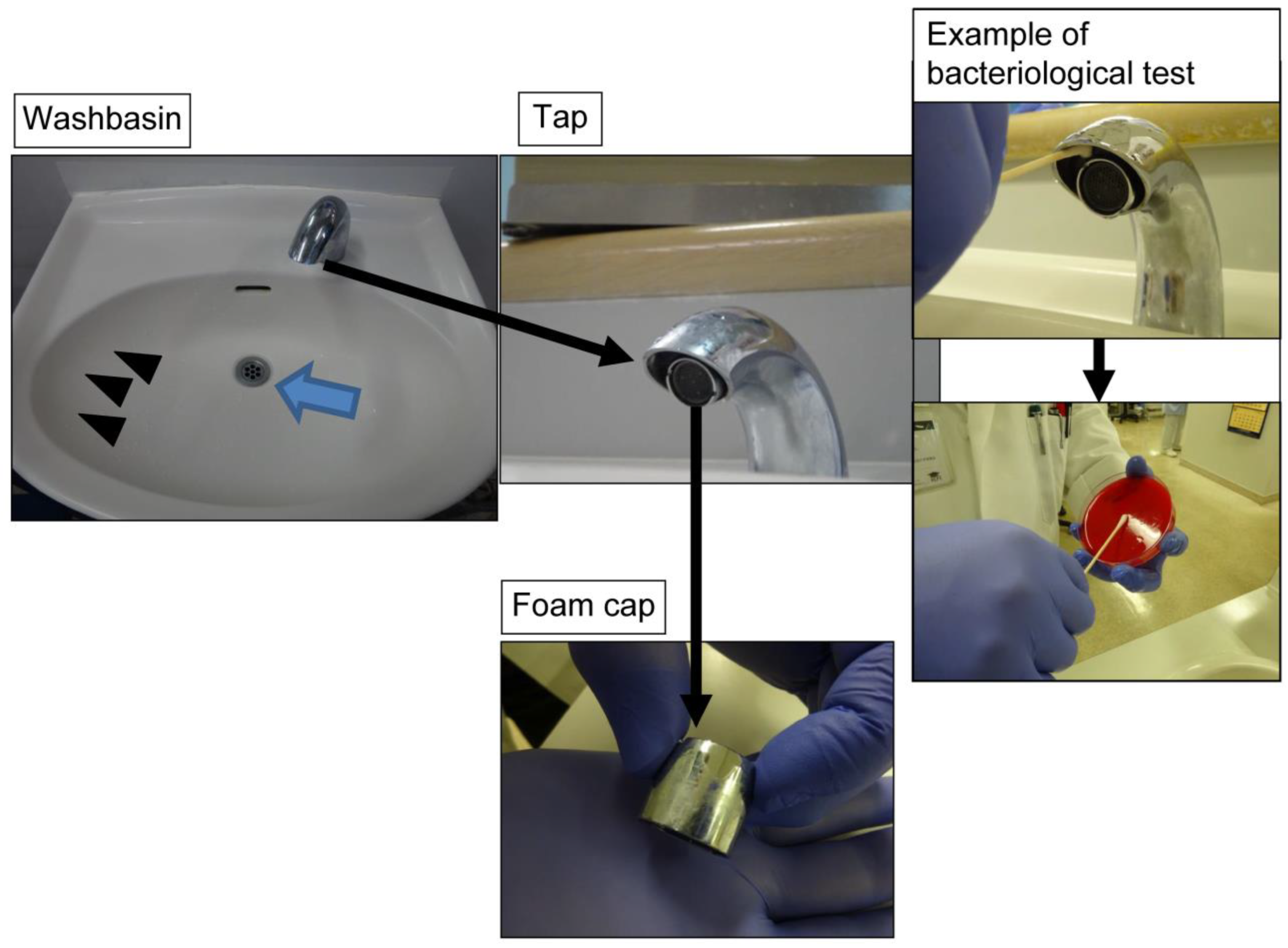
We conducted a bacteriological survey around four washbasins in the HCU shared by patients for brushing their teeth and gargling (
Figure 1). Swab samples were collected from drains, sink sides, and taps, including the inside surface of the tap and foam caps, using one sterilised cotton Nissui swab (Nissui Pharmaceutical Co., Ltd., Tokyo, Japan) per environmental surface. After sample collection, the swabs were immediately applied to blood agar, cultured in an incubator at 37 °C for 24 h, and then allowed to stand at room temperature for 24 h. The bacterial count was measured according to a semi-quantitative culture method [
10,
11], and the number of bacteria on culture was quantified according to the
Clinical Microbiology Procedures Handbook guidelines as follows: colony growth on less than 1/3 of the medium = 1+; 1/3 to less than 2/3 = 2+; 2/3 or more = 3+; and the entire medium = 4+ [
12]. Bacterial identification and susceptibility testing of the isolates were performed to obtain minimum inhibitory concentration (MIC) values using a microdilution method (CLSI, 2018) and a DxM Microscan WalkAway (Beckman Coulter Inc., Brea, CA, USA) microorganism identification susceptibility analyser. Genotyping was conducted to identify drug-resistant bacteria, as described previously [
13].
Based on the results of the bacteriological survey, we focused on evaluating different methods for cleaning taps using various cleaning agents, including an environmentally neutral detergent (Mypet, Kao Corporation, Tokyo, Japan), citric acid, baking soda, a cleanser (Kaneyo Soap Co., Ltd., Fukui, Japan), 80% ethanol, 0.1% sodium hypochlorite, and an environmental detergent (Space Shot rust remover/toilet cleaner, Orb Tech Co., Ltd., Tokyo, Japan), hereinafter referred to as Space Shot. Space Shot, a strongly acidic phosphoric acid-based environmental cleaning agent, is composed of phosphoric acid, ethanol, hydrochloric acid, zinc, dye, and water. Space Shot has a pH of approximately 1.6, which is lower than that of citric acid. The cleaning effect was evaluated based mainly on its effect on removing hard scale from taps.
3. Results
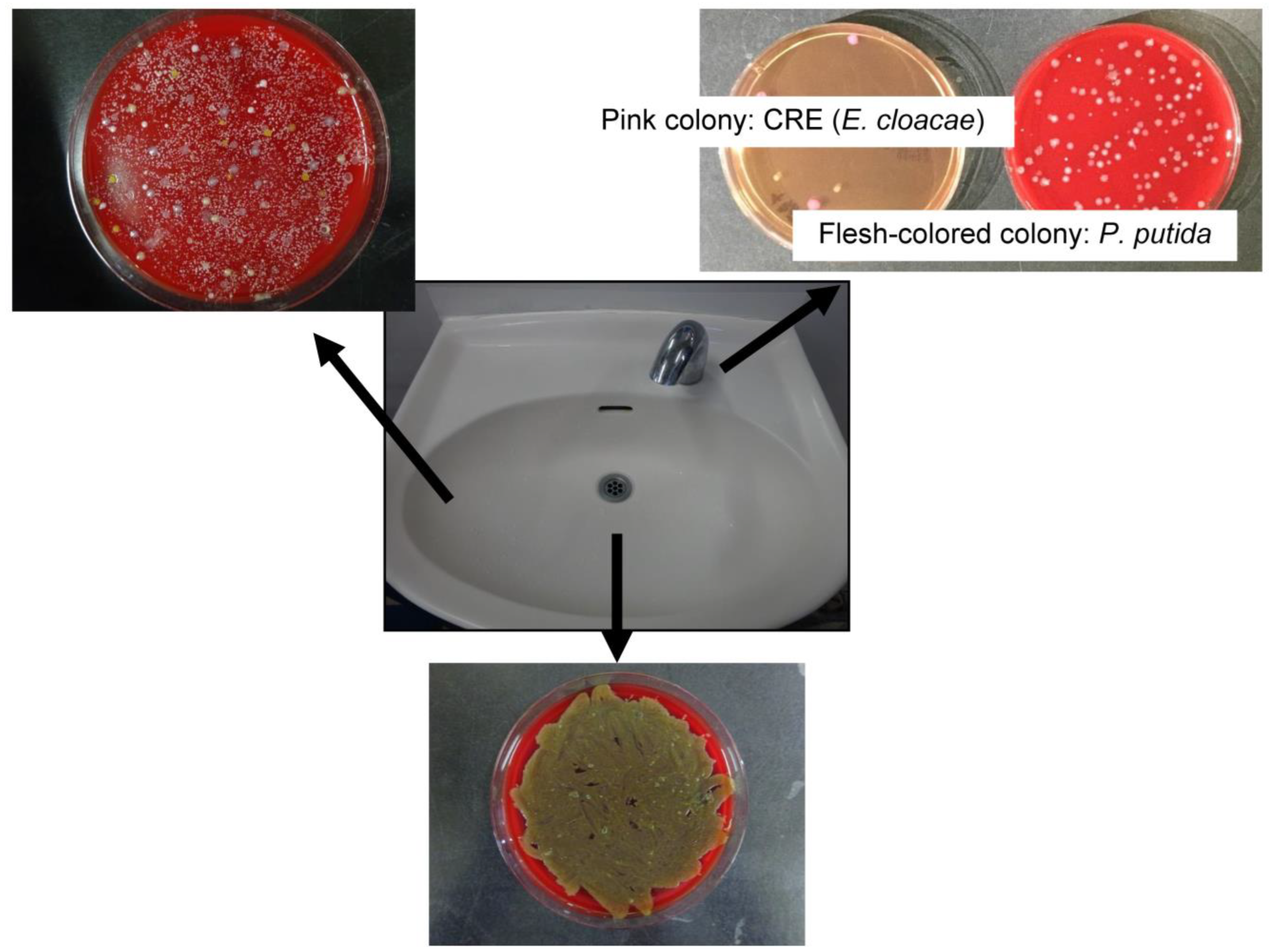
The taps of the washbasins in hospital rooms were extremely contaminated (
Figure 2). In the bacteriological survey of the environment, many bacteria were cultured from washbasin drains. The bacterial count was high on the sides of sinks and taps (including the inside surface of the tap and the outside surface of the foam cup). The following pathogenic bacteria were identified:
Micrococcus sp.,
Bacillus sp., coagulase-negative
Staphylococcus,
Staphylococcus aureus, gram-positive rods,
Stenotrophomonas maltophilia,
Corynebacterium sp., glucose non-fermentative gram-negative bacilli,
Enterobacter cloacae,
Exophiala sp.,
Candida sp.,
Pantoea agglomerans,
Pseudomonas sp.,
Citrobacter braakii,
Pseudomonas aeruginosa, alpha-hemolytic
Streptococcus,
Acremonium sp.,
Aspergillus niger,
Fusarium sp.,
Rhizobium radiobacter,
Weeksella virosa,
Acinetobacter lwoffii group, and
Cladosporium sp. Bacteria detected on taps included pathogenic
Enterobacter cloacae and
Pseudomonas putida (
Table 1). These were detected in the drain, on the sides of the basin, and on the tap. The
Enterobacter cloacae isolate harbored
AmpC and
CTX-M resistance genes.
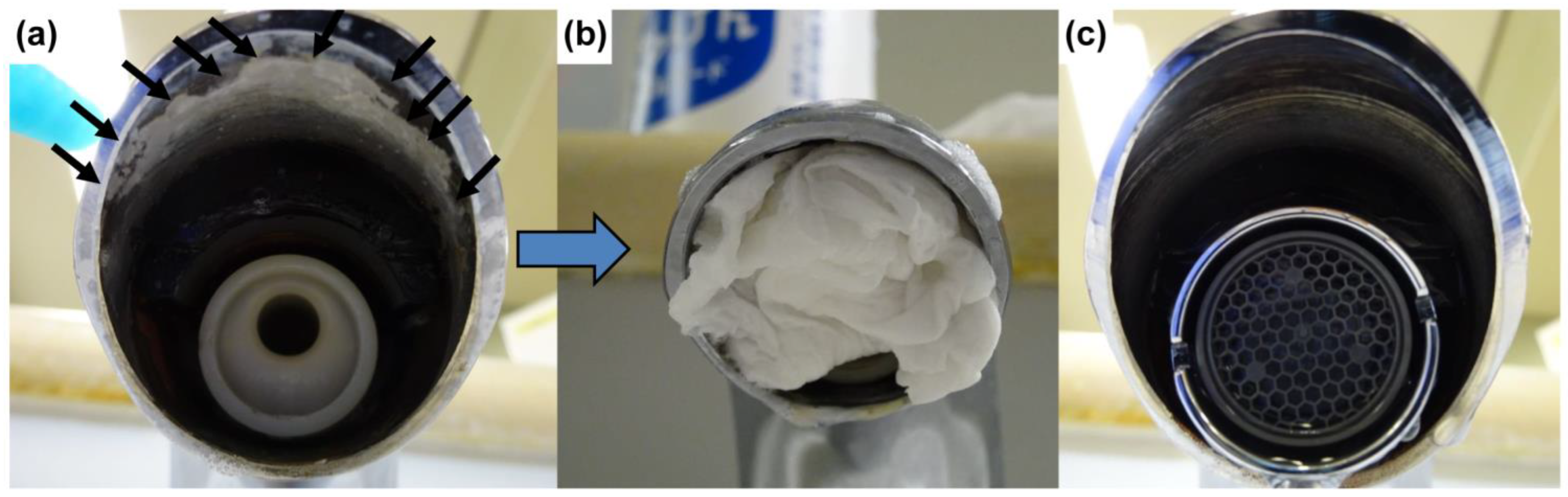
The hard scale on the taps could not be removed by physically scraping it off with a clip or screwdriver nor by soaking tissue paper with a chemical solution, applying it to the scale, and leaving it for over 30 min. Cleaning the taps with an environmentally neutral detergent, citric acid, baking soda, a cleanser, 80% ethanol, or 0.1% sodium hypochlorite also had little impact on the scale on both the inner surface of the tap and the foam cap (
Table 2). Application of tissue paper soaked with Space Shot for 30 min resulted in a softening of the hard scale and allowed easy removal of the scale without using physical force. We visually confirmed that the tap was clean (
Figure 3), and a bacteriological survey cultured a few bacteria (
Table 3). No CRE or other pathogens were detected. Space Shot was the only cleaning agent that was effective in removing hard scale. Despite its strong detergent effect, Space Shot did not result in corrosion or discoloration of the taps.
4. Discussion
The hard scale adhering to taps consists mainly of alkaline deposits such as calcium carbonate. According to our findings, Space Shot was the only agent tested that could effectively remove hard scale. This is probably because the low pH of this product acts on alkaline deposits.
According to a survey by the Ministry of Land, Infrastructure, Transport and Tourism in Japan, there are only nine countries where tap water is drinkable [
14]. In Japan, tap water is hygienic and is considered potable [
15]. Hospitalised, ambulatory patients wash their hands, brush their teeth, and gargle at the washbasins. Therefore, the detection of even a small number of pathogenic microorganisms in tap water used by patients, such as in high-care units where immunocompromised patients are hospitalised, poses an infection risk. Outbreaks have been reported due to the contamination of tap and drinking water with various microorganisms [
3,
16,
17,
18,
19,
20,
21]. Notably, a previous report suggests that more than half of the bacteria detected in tap water showed antimicrobial resistance [
22], as did our findings. Hand and equipment contamination from the taps and surrounding sink surfaces can promote transmission of antimicrobial-resistant pathogenic bacteria, which may result in hospital-associated infections. In a study investigating the genotype of
P. aeruginosa contaminating the tap of a surgical intensive care ward, 5 of 17 cases (29%) had the same genotype as
P. aeruginosa detected in the tap over a 7-month period [
21]. This suggests that the tap serves as an environmental reservoir of pathogenic microorganisms. It is clear that it is important to remove bacteria adhering to taps to prevent infections caused by pathogens in the environment. In this study, we immediately implemented cleaning after CRE was detected in the environmental survey. The Advanced Emergency and Critical Care Center actively conducts bacteriological tests on patients on hospital admission and discharge; however, to date, no CRE has been detected on discharge in patients who used the taps in the centre. CRE may have adhered to taps due to splash-back from the washbasin during hand washing and gargling by patients with CRE colonisation. When drug-resistant bacteria, such as CRE, adhere to a tap, it is possible that patients who use water from the tap contract CRE infection. No pathogenic bacteria, including CRE, were detected in patients who used the washbasins after effective cleaning of the taps, suggesting that effective cleaning can prevent horizontal infection from the environment.
In an outbreak of CRE detected in the water supply of an intensive care unit (ICU), it was reported that even deep cleansing with sodium hypochlorite and pressurised steam decontamination at 170 °C could not remove CRE [
23]. A strength of our study is that we found an effective and efficient cleaning method for removing CRE. Introducing this method may be useful in other medical facilities with CRE in the water supply.
Our study has some limitations. First, the bacterial count values were not determined and a quantitative comparison was not possible. Second, the investigation of various detergents did not include a bacteriological investigation and the cleaning effect was judged only with the naked eye. Third, we did not determine the optimal interval at which Space Shot should be used for disinfection. Further research is required to address these questions.
To maintain hygiene, sinks should be cleaned daily, and taps should be cleaned regularly. The appropriate interval for cleaning taps is currently unclear. At our facility, due to human resource and cost issues, taps are cleaned once every 6 months using Space Shot. During the past 4 years since the implementation of this cleaning method, we have not detected new hard scale build-up or associated pathogenic bacteria on taps and have not detected any hospital-associated infections attributable to tap water contamination. Establishing an effective method of cleaning taps as part of hygiene management is important for hospital infection control.
5. Conclusions
Taps can serve as an environmental reservoir for pathogenic microorganisms, such as CRE. A phosphoric acid-based detergent (Space Shot) effectively removed hard scale from taps and washbasins. Effective cleaning of the taps as part of the hygiene management of washbasins is important for hospital infection control.
Author Contributions
Conceptualisation, S.A.; methodology, S.A., M.H.; investigation, M.H., K.U., R.T., M.M., M.K., Y.K. and Y.S. (Yoshika Sekine); resources, S.A.; data curation, M.H., R.T. and M.M.; writing—original draft preparation, M.H.; writing—review and editing, S.A.; supervision, Y.S. (Yuji Suzuki) and K.O.; project administration, H.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The paper provides all the relevant data supporting the results.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Buchan, B.W.; Graham, M.B.; Lindmair-Snell, J.; Arvan, J.; Ledeboer, N.A.; Nanchal, R.; Munoz-Price, L.S. The relevance of sink proximity to toilets on the detection of Klebsiella pneumoniae carbapenemase inside sink drains. Am. J. Infect. Control 2019, 47, 98–100. [Google Scholar] [CrossRef] [Green Version]
- Parkes, L.O.; Hota, S.S. Sink-related outbreaks and mitigation strategies in healthcare facilities. Curr. Infect. Dis. Rep. 2018, 20, 42. [Google Scholar] [CrossRef] [PubMed]
- Umezawa, K.; Asai, S.; Inokuchi, S.; Miyachi, H. A comparative study of the bactericidal activity and daily disinfection housekeeping surfaces by a new portable pulsed UV radiation device. Curr. Microbiol. 2012, 64, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Corti, M.; Palmero, D.; Eiguchi, K. Respiratory infections in immunocompromised patients. Curr. Opin. Pulm. Med. 2009, 15, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.J.; Susi, A.; Nylund, C.M. Clinical characteristics, risk factors, and outcomes of patients hospitalized in the US military health system with carbapenem-resistant Enterobacteriaceae infection. Am. J. Infect. Control 2020, 48, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Durante-Mangoni, E.; Andini, R.; Zampino, R. Management of carbapenem-resistant Enterobacteriaceae infections. Clin. Microbiol. Infect. 2019, 25, 943–950. [Google Scholar] [CrossRef] [PubMed]
- US Centers for Disease Control and Prevention (CDC). Facility Guidance for Control of Carbapenem-Resistant Enterobacteriaceae (CRE)—November 2015 Update CRE Toolkit. Available online: https://www.cdc.gov/hai/pdfs/cre/cre-guidance-508.pdf (accessed on 11 October 2022).
- Donlan, R.M. Biofilm formation: A clinically relevant microbiological process. Clin. Infect. Dis. 2001, 33, 1387–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balcázar, J.L.; Subirats, J.; Borrego, C.M. The role of biofilms as environmental reservoirs of antibiotic resistance. Front. Microbiol. 2015, 6, 1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asai, S.; Ohshima, T.; Umezawa, K.; Inokuchi, S.; Miyachi, H. The horizontal transmission of drug-resistant Pseudomonas aeruginosa in the patients with burn injury through sharing of the shower room and its infection control. Jpn. J. Burn. Inj. 2011, 37, 105. (In Japanese) [Google Scholar]
- Iwashita, H.; Asai, S.; Umezawa, K.; Ohhashi, M.; Sasaki, M.; Ohshima, T.; Kaneko, A.; Miyachi, H. A study on effective disinfection of clinical contract surface in dental practice based on bacteriological culture. Jpn. J. Infect. Prev. Control 2013, 28, 273–278. (In Japanese) [Google Scholar] [CrossRef] [Green Version]
- Leber, A.L. (Ed.) Clinical Microbiology Procedures Handbook, 4th ed.; ASM Press: Washington, DC, USA, 2016. [Google Scholar]
- Asai, S.; Ohshima, T.; Iwashita, H.; Ishii, Y.; Aoki, K.; Minakawa, Y.; Machida, S.; Umezawa, K.; Tateda, K.; Miyachi, H. Carbapenem-resistant Klebsiella pneumoniae in a febrile neutropenia patient with acute myelogenous leukemia after hematopoietic stem cell transplantation. Infect. Dis. Clin. Pract. 2018, 26, e38–e39. [Google Scholar] [CrossRef] [PubMed]
- International Initiatives Concerning Water Resources. Available online: https://www.mlit.go.jp/common/001257609.pdf (accessed on 9 February 2023).
- Waterworks Law in Japan Article 4. Available online: https://elaws.e-gov.go.jp/document?lawid=332AC0000000177 (accessed on 30 December 2022).
- Moreira, N.A.; Bondelind, M. Safe drinking water and waterborne outbreaks. J. Water Health 2017, 15, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Karanis, P.; Kourenti, C.; Smith, H. Waterborne transmission of protozoan parasites: A worldwide review of outbreaks and lessons learnt. J. Water Health 2007, 5, 1–38. [Google Scholar] [CrossRef] [PubMed]
- Tagashira, Y.; Kozai, Y.; Yamasa, H.; Sakurada, M.; Kashiyama, T.; Honda, H. A cluster of central line-associated bloodstream infections due to rapidly growing nontuberculous mycobacteria in patients with hematologic disorders at a Japanese tertiary care center: An outbreak investigation and review of the literature. Infect. Control Hosp. Epidemiol. 2015, 36, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Livni, G.; Yaniv, I.; Samra, Z.; Kaufman, L.; Solter, E.; Ashkenazi, S.; Levy, I. Outbreak of Mycobacterium mucogenicum bacteraemia due to contaminated water supply in a paediatric haematology-oncology department. J. Hosp. Infect. 2008, 70, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Aumeran, C.; Paillard, C.; Robin, F.; Kanold, J.; Baud, O.; Bonnet, R.; Souweine, B.; Traore, O. Pseudomonas aeruginosa and Pseudomonas putida outbreak associated with contaminated water outlets in an oncohaematology paediatric unit. J. Hosp. Infect. 2007, 65, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Trautmann, M.; Michalsky, T.; Wiedeck, H.; Radosavljevic, V.; Ruhnke, M. Tap water colonization with Pseudomonas aeruginosa in a surgical intensive care unit (ICU) and relation to Pseudomonas infections of ICU patients. Infect. Control Hosp. Epidemiol. 2001, 22, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Vincenti, S.; Quaranta, G.; De Meo, C.; Bruno, S.; Ficarra, M.G.; Carovillano, S.; Ricciardi, W.; Laurenti, P. Non-fermentative gram-negative bacteria in hospital tap water and water used for haemodialysis and bronchoscope flushing: Prevalence and distribution of antibiotic resistant strains. Sci. Total Environ. 2014, 499, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Kotsanas, D.; Wijesooriya, W.R.; Korman, T.M.; Gillespie, E.E.; Wright, L.; Snook, K.; Williams, N.; Bell, J.M.; Li, H.Y.; Stuart, R.L. “Down the drain”: Carbapenem-resistant bacteria in intensive care unit patients and handwashing sinks. Med. J. Aust. 2013, 198, 267–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}
{kind=link}