
The Impact of Submicroscopic Parasitemia on Malaria Rapid Diagnosis in Northeastern Tanzania, an Area with Diverse Transmission Patterns

Abstract
:1. Introduction
2. Materials and Methods
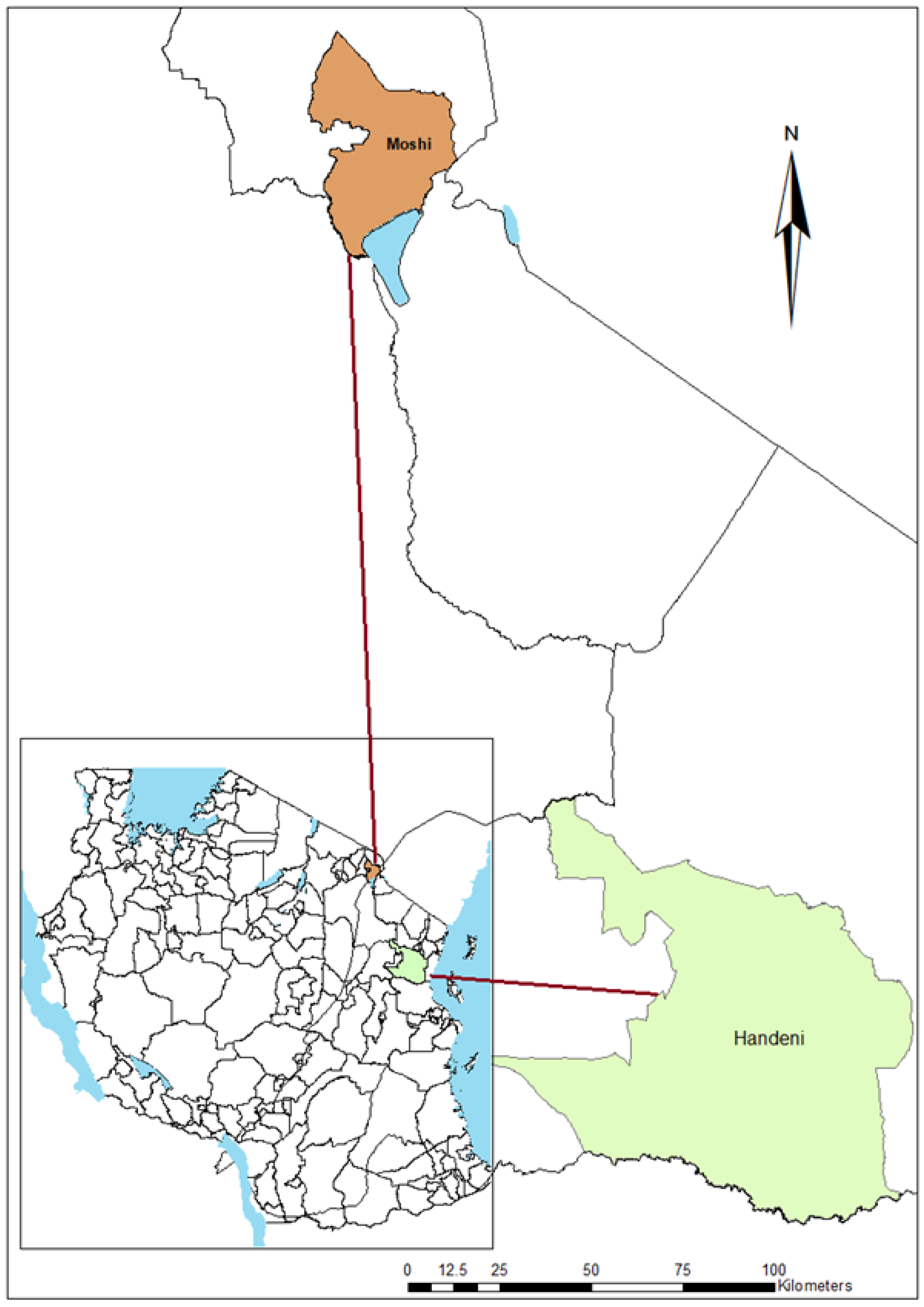
2.1. Description of the Study Areas
2.2. Participants Recruitment and Sample Collection
2.3. Malaria Rapid Diagnosis (mRDT)
2.4. Light Microscopy
2.5. Polymerase Chain Reaction (PCR)
2.6. Statistical Analysis
3. Results
3.1. Malaria Prevalence by mRDT, LM, and PCR
3.2. Parasitemia Levels across Age Groups
3.3. Sub-Microscopic Parasitemia
3.4. Diagnostic Accuracy of the LM, mRDT and PCR
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2021; electronic version; World Health Organization: Geneva, Switzerland, 2021; ISBN 9789240040496. [Google Scholar]
- World Health Organization. Malaria Surveillance, Monitoring and Evaluation: A Reference Manual; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241565578. [Google Scholar]
- Ouédraogo, A.L.; de Vlas, S.J.; Nébié, I.; Ilboudo-Sanogo, E.; Bousema, J.T.; Ouattara, A.S.; Verhave, J.P.; Cuzin-Ouattara, N.; Sauerwein, R.W. Seasonal Patterns of Plasmodium Falciparum Gametocyte Prevalence and Density in a Rural Population of Burkina Faso. Acta Trop. 2008, 105, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Geiger, C.; Agustar, H.K.; Compaoré, G.; Coulibaly, B.; Sié, A.; Becher, H.; Lanzer, M.; Jänisch, T. Declining Malaria Parasite Prevalence and Trends of Asymptomatic Parasitaemia in a Seasonal Transmission Setting in North-Western Burkina Faso between 2000 and 2009–2012. Malar. J. 2013, 12, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dent, A.E.; Nakajima, R.; Liang, L.; Baum, E.; Moormann, A.M.; Sumba, P.O.; Vulule, J.; Babineau, D.; Randall, A.; Davies, D.H.; et al. Plasmodium Falciparum Protein Microarray Antibody Profiles Correlate with Protection from Symptomatic Malaria in Kenya. J. Infect. Dis. 2015, 212, 1429–1438. [Google Scholar] [CrossRef] [Green Version]
- Niang, M.; Bei, A.K.; Madnani, K.G.; Pelly, S.; Dankwa, S.; Kanjee, U.; Gunalan, K.; Amaladoss, A.; Yeo, K.P.; Bob, N.S.; et al. STEVOR Is a Plasmodium Falciparum Erythrocyte Binding Protein That Mediates Merozoite Invasion and Rosetting. Cell Host Microbe 2014, 16, 81–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzales, S.J.; Reyes, R.A.; Braddom, A.E.; Batugedara, G.; Bol, S.; Bunnik, E.M. Naturally Acquired Humoral Immunity Against Plasmodium Falciparum Malaria. Front. Immunol. 2020, 11, 2809. [Google Scholar] [CrossRef] [PubMed]
- Noor, A.M.; Kirui, V.C.; Brooker, S.J.; Snow, R.W. The Use of Insecticide Treated Nets by Age: Implications for Universal Coverage in Africa. BMC Public Health 2009, 9, 369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, F.P.; Gil, L.H.S.; Marrelli, M.T.; Ribolla, P.E.M.; Camargo, E.P.; Da Silva, L.H.P. Asymptomatic Carriers of Plasmodium spp. as Infection Source for Malaria Vector Mosquitoes in the Brazilian Amazon. J. Med. Entomol. 2005, 42, 777–779. [Google Scholar] [CrossRef]
- Zaw, M.T.; Thant, M.; Hlaing, T.M.; Aung, N.Z.; Thu, M.; Phumchuea, K.; Phusri, K.; Saeseu, T.; Yorsaeng, R.; Nguitragool, W.; et al. Asymptomatic and Sub-Microscopic Malaria Infection in Kayah State, Eastern Myanmar. Malar. J. 2017, 16, 138. [Google Scholar] [CrossRef] [Green Version]
- Zoghi, S.; Mehrizi, A.A.; Raeisi, A.; Haghdoost, A.A.; Turki, H.; Safari, R.; Kahanali, A.A.; Zakeri, S. Survey for Asymptomatic Malaria Cases in Low Transmission Settings of Iran under Elimination Programme. Malar. J. 2012, 11, 126. [Google Scholar] [CrossRef] [Green Version]
- Shekalaghe, S.A.; Bousema, J.T.; Kunei, K.K.; Lushino, P.; Masokoto, A.; Wolters, L.R.; Mwakalinga, S.; Mosha, F.W.; Sauerwein, R.W.; Drakeley, C.J. Submicroscopic Plasmodium Falciparum Gametocyte Carriage Is Common in an Area of Low and Seasonal Transmission in Tanzania. Trop. Med. Int. Health 2007, 12, 547–553. [Google Scholar] [CrossRef]
- Zhou, Z.; Mitchell, R.M.; Kariuki, S.; Odero, C.; Otieno, P.; Otieno, K.; Onyona, P.; Were, V.; Wiegand, R.E.; Gimnig, J.E.; et al. Assessment of Submicroscopic Infections and Gametocyte Carriage of Plasmodium Falciparum during Peak Malaria Transmission Season in a Community-Based Cross-Sectional Survey in Western Kenya, 2012. Malar. J. 2016, 15, 421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, P.; Bousema, J.T.; Gouagna, L.C.; Otieno, S.; van de Vegte-Bolmer, M.; Omar, S.A.; Sauerwein, R.W. Submicroscopic Plasmodium Falciparum Gametocyte Densities Frequently Result in Mosquito Infection. Am. J. Trop. Med. Hyg. 2007, 76, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Masanja, I.M.; Selemani, M.; Amuri, B.; Kajungu, D.; Khatib, R.; Kachur, S.P.; Skarbinski, J. Increased Use of Malaria Rapid Diagnostic Tests Improves Targeting of Anti-Malarial Treatment in Rural Tanzania: Implications for Nationwide Rollout of Malaria Rapid Diagnostic Tests. Malar. J. 2012, 11, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albertini, A.; Lee, E.; Coulibaly, S.O.; Sleshi, M.; Faye, B.; Mationg, M.L.; Ouedraogo, K.; Tsadik, A.G.; Feleke, S.M.; Diallo, I.; et al. Malaria Rapid Diagnostic Test Transport and Storage Conditions in Burkina Faso, Senegal, Ethiopia and the Philippines. Malar. J. 2012, 11, 406. [Google Scholar] [CrossRef] [Green Version]
- WHO. Malaria Rapid Diagnostic Test Performance. Results of WHO Product Testing of Malaria RDTs: Round 8; WHO: Geneva, Switzerland, 2018; p. 172. [Google Scholar]
- Milne, L.M.; Kyi, M.S.; Chiodini, P.L.; Warhurst, D.C. Accuracy of Routine Laboratory Diagnosis of Malaria in the United Kingdom. J. Clin. Pathol. 1994, 47, 740–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, P.; Zhao, Z.; Wang, Y.; Xing, H.; Parker, D.M.; Yang, Z.; Baum, E.; Li, W.; Sattabongkot, J.; Sirichaisinthop, J.; et al. Nested PCR Detection of Malaria Directly Using Blood Filter Paper Samples from Epidemiological Surveys. Malar. J. 2014, 13, 175. [Google Scholar] [CrossRef] [Green Version]
- Kaaya, R.D.; Kajeguka, D.C.; Matowo, J.J.; Ndaro, A.J.; Mosha, F.W.; Chilongola, J.O.; Kavishe, R.A. Predictive Markers of Transmission in Areas with Different Malaria Endemicity in North-Eastern Tanzania Based on Seroprevalence of Antibodies against Plasmodium Falciparum. BMC Res. Notes 2021, 14, 404. [Google Scholar] [CrossRef]
- Kassam, N.A.; Kaaya, R.D.; Damian, D.J.; Schmiegelow, C.; Kavishe, R.A.; Alifrangis, M.; Wang, C.W. Ten Years of Monitoring Malaria Trend and Factors Associated with Malaria Test Positivity Rates in Lower Moshi. Malar. J. 2021, 20, 193. [Google Scholar] [CrossRef]
- World Health Organization. Basic Malaria Microscopy 2010; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Miguel, R.B.; Coura, J.R.; Samudio, F.; Suárez-Mutis, M.C. Evaluation of Three Different DNA Extraction Methods from Blood Samples Collected in Dried Filter Paper in Plasmodium Subpatent Infections from the Amazon Region in Brazil. Rev. Inst. Med. Trop. Sao Paulo 2013, 55, 205–208. [Google Scholar] [CrossRef]
- Snounou, G.; Singh, B. Nested PCR Analysis of Plasmodium Parasites. Methods Mol. Med. 2002, 72, 189–203. [Google Scholar] [CrossRef]
- Altman, D.G.; Bland, J.M. Diagnostic Tests 2: Predictive Values. BMJ 1994, 309, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emidi, B.; Kisinza, W.N.; Kaaya, R.D.; Malima, R.; Mosha, F.W. Insecticide Susceptibility Status of Human Biting Mosquitoes in Muheza, Tanzania. Tanzan. J. Health Res. 2017, 19, 1–10. [Google Scholar] [CrossRef]
- Kaindoa, E.W.; Matowo, N.S.; Ngowo, H.S.; Mkandawile, G.; Mmbando, A.; Finda, M.; Okumu, F.O. Interventions That Effectively Target Anopheles Funestus Mosquitoes Could Significantly Improve Control of Persistent Malaria Transmission in South-Eastern Tanzania. PLoS ONE 2017, 12, e0177807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitau, J.; Oxborough, R.M.; Tungu, P.K.; Matowo, J.; Malima, R.C.; Magesa, S.M.; Bruce, J.; Mosha, F.W.; Rowland, M.W. Species Shifts in the Anopheles Gambiae Complex: Do LLINs Successfully Control Anopheles Arabiensis? PLoS ONE 2012, 7, e31481. [Google Scholar] [CrossRef] [Green Version]
- Hayuma, P.M.; Wang, C.W.; Liheluka, E.; Baraka, V.; Madebe, R.A.; Minja, D.T.R.; Misinzo, G.; Alifrangis, M.; Lusingu, J.P.A. Prevalence of Asymptomatic Malaria, Submicroscopic Parasitaemia and Anaemia in Korogwe District, North-Eastern Tanzania. Malar. J. 2021, 20, 424. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple, U.; Arambepola, R.; Gething, P.W.; Cameron, E. How Long Do Rapid Diagnostic Tests Remain Positive after Anti-Malarial Treatment? Malar. J. 2018, 17, 228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatton, M.L.; Ciketic, S.; Barnwell, J.W.; Cheng, Q.; Chiodini, P.L.; Incardona, S.; Bell, D.; Cunningham, J.; González, I.J. An Assessment of False Positive Rates for Malaria Rapid Diagnostic Tests Caused by Non-Plasmodium Infectious Agents and Immunological Factors. PLoS ONE 2018, 13, e0197395. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, J.; Sher, A.; Rab, A. Plasmodium Falciparum Histidine-Rich Protein 2-Based Immunocapture Diagnostic Assay for Malaria: Cross-Reactivity with Rheumatoid Factors. J. Clin. Microbiol. 2000, 38, 1184–1186. [Google Scholar] [CrossRef] [Green Version]
- Watson, O.J.; Sumner, K.M.; Janko, M.; Goel, V.; Winskill, P.; Slater, H.C.; Ghani, A.; Meshnick, S.R.; Parr, J.B. False-Negative Malaria Rapid Diagnostic Test Results and Their Impact on Community-Based Malaria Surveys in Sub-Saharan Africa. BMJ Glob. Health 2019, 4, e001582. [Google Scholar] [CrossRef] [Green Version]
- Unwin, V.T.; Ahmed, R.; Noviyanti, R.; Puspitasari, A.M.; Utami, R.A.S.; Trianty, L.; Lukito, T.; Syafruddin, D.; Poespoprodjo, J.R.; Santana-Morales, M.A.; et al. Use of a Highly-Sensitive Rapid Diagnostic Test to Screen for Malaria in Pregnancy in Indonesia. Malar. J. 2020, 19, 28. [Google Scholar] [CrossRef]
- Anthony, M. Rapid Diagnostic Tests for Malaria Parasites. Clin. Microbiol. Rev. 2002, 15, 66–78. [Google Scholar] [CrossRef] [Green Version]
- Tadesse, E.; Workalemahu, B.; Shimelis, T. Diagnostic performance evaluation of the sd bioline malaria antigen ag pf/pan test (05fk60) in a malaria endemic area of southern Ethiopia. Rev. Inst. Med. Trop. Sao Paulo 2016, 58, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseroni, M.; Pervanidou, D.; Tserkezou, P.; Rachiotis, G.; Pinaka, O.; Baka, A.; Georgakopoulou, T.; Vakali, A.; Dionysopoulou, M.; Terzaki, I.; et al. Field Application of SD Bioline Malaria Ag Pf/Pan Rapid Diagnostic Test for Malaria in Greece. PLoS ONE 2015, 10, e0120367. [Google Scholar] [CrossRef] [PubMed]
- Cohee, L.M.; Nankabirwa, J.I.; Greenwood, B.; Djimde, A.; Mathanga, D.P. Time for Malaria Control in School-Age Children. Lancet Child Adolesc. Health 2021, 5, 537–538. [Google Scholar] [CrossRef]
- Olapeju, B.; Choiriyyah, I.; Lynch, M.; Acosta, A.; Blaufuss, S.; Filemyr, E.; Harig, H.; Monroe, A.; Selby, R.A.; Kilian, A.; et al. Age and Gender Trends in Insecticide-Treated Net Use in Sub-Saharan Africa: A Multi-Country Analysis. Malar. J. 2018, 17, 423. [Google Scholar] [CrossRef] [PubMed]
- Chacky, F.; Runge, M.; Rumisha, S.F.; Machafuko, P.; Chaki, P.; Massaga, J.J.; Mohamed, A.; Pothin, E.; Molteni, F.; Snow, R.W.; et al. Nationwide School Malaria Parasitaemia Survey in Public Primary Schools, the United Republic of Tanzania. Malar. J. 2018, 17, 452. [Google Scholar] [CrossRef] [Green Version]
- Cohee, L.M.; Opondo, C.; Clarke, S.E.; Halliday, K.E.; Cano, J.; Shipper, A.G.; Barger-Kamate, B.; Djimde, A.; Diarra, S.; Dokras, A.; et al. Preventive Malaria Treatment among School-Aged Children in Sub-Saharan Africa: A Systematic Review and Meta-Analyses. Lancet Glob. Health 2020, 8, e1499–e1511. [Google Scholar] [CrossRef]
- Mathanga, D.P.; Halliday, K.E.; Jawati, M.; Verney, A.; Bauleni, A.; Sande, J.; Ali, D.; Jones, R.; Witek-McManus, S.; Roschnik, N.; et al. The High Burden of Malaria in Primary School Children in Southern Malawi. Am. Soc. Trop. Med. Hyg. 2015, 93, 779–789. [Google Scholar] [CrossRef] [Green Version]
- Okell, L.C.; Bousema, T.; Griffin, J.T.; Ouédraogo, A.L.; Ghani, A.C.; Drakeley, C.J. Factors Determining the Occurrence of Submicroscopic Malaria Infections and Their Relevance for Control. Nat. Commun. 2012, 3, 1237. [Google Scholar] [CrossRef] [Green Version]
- Walldorf, J.A.; Cohee, L.M.; Coalson, J.E.; Bauleni, A.; Nkanaunena, K.; Kapito-Tembo, A.; Seydel, K.B.; Ali, D.; Mathanga, D.; Taylor, T.E.; et al. School-Age Children Are a Reservoir of Malaria Infection in Malawi. PLoS ONE 2015, 10, e0134061. [Google Scholar] [CrossRef]
- Yazdani, S.S.; Mukherjee, P.; Chauhan, V.S.; Chitnis, C.E. Immune Responses to Asexual Blood-Stages of Malaria Parasites. Curr. Mol. Med. 2006, 6, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Boyd, M.F.; Stratman-Thomas, W.K.; Kitchen, S.F. On Acquired Immunity to Plasmodium Falciparum1. Am. J. Trop. Med. Hyg. 1936, 1, 139–145. [Google Scholar] [CrossRef]
- Cabrera, E.J.; Barr, M.L.; Silverman, P.H. Long-Term Studies on Rhesus Monkeys (Macaca Mulatta) Immunized against Plasmodium Knowlesi. Infect. Immun. 1977, 15, 461–465. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.J.; Phillips, R.S. Method to Test Inhibitory Antibodies in Human Sera to Wild Populations of Plasmodium Falciparum. Nature 1976, 263, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.T.; Déirdre Hollingsworth, T.; Reyburn, H.; Drakeley, C.J.; Riley, E.M.; Ghani, A.C. Gradual Acquisition of Immunity to Severe Malaria with Increasing Exposure. Proc. R. Soc. B Biol. Sci. 2015, 282, 20142657. [Google Scholar] [CrossRef] [Green Version]
- van den Hoogen, L.L.; Walk, J.; Oulton, T.; Reuling, I.J.; Reiling, L.; Beeson, J.G.; Coppel, R.L.; Singh, S.K.; Draper, S.J.; Bousema, T.; et al. Antibody Responses to Antigenic Targets of Recent Exposure Are Associated With Low-Density Parasitemia in Controlled Human Plasmodium Falciparum Infections. Front. Microbiol. 2019, 9, 3300. [Google Scholar] [CrossRef]
- Mensah, B.A.; Myers-Hansen, J.L.; Obeng Amoako, E.; Opoku, M.; Abuaku, B.K.; Ghansah, A. Prevalence and Risk Factors Associated with Asymptomatic Malaria among School Children: Repeated Cross-Sectional Surveys of School Children in Two Ecological Zones in Ghana. BMC Public Health 2021, 21, 1697. [Google Scholar] [CrossRef]
- Worku, L.; Damtie, D.; Endris, M.; Getie, S.; Aemero, M. Asymptomatic Malaria and Associated Risk Factors among School Children in Sanja Town, Northwest Ethiopia. Int. Sch. Res. Not. 2014, 2014, 303269. [Google Scholar] [CrossRef] [Green Version]
- Berzosa, P.; de Lucio, A.; Romay-Barja, M.; Herrador, Z.; González, V.; García, L.; Fernández-Martínez, A.; Santana-Morales, M.; Ncogo, P.; Valladares, B.; et al. Comparison of Three Diagnostic Methods (Microscopy, RDT, and PCR) for the Detection of Malaria Parasites in Representative Samples from Equatorial Guinea. Malar. J. 2018, 17, 333. [Google Scholar] [CrossRef]
- Acquah, F.K.; Donu, D.; Obboh, E.K.; Bredu, D.; Mawuli, B.; Amponsah, J.A.; Quartey, J.; Amoah, L.E. Diagnostic Performance of an Ultrasensitive HRP2-Based Malaria Rapid Diagnostic Test Kit Used in Surveys of Afebrile People Living in Southern Ghana. Malar. J. 2021, 20, 125. [Google Scholar] [CrossRef]
- Poti, K.E.; Sullivan, D.J.; Dondorp, A.M.; Woodrow, C.J. HRP2: Transforming Malaria Diagnosis, but with Caveats. Trends Parasitol. 2020, 36, 112–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oladosu, O.; Adedokun Victoria, A.; Adeniyi Akinkunle, V.; Oyibo Wellington, A. Performance Evaluation of Malaria HRP-2 Rapid Diagnostic Test among Febrile Patients with Malaria in Iwo, Osun State, Nigeria. Int. J. Trop. Dis. 2021, 4, 46. [Google Scholar] [CrossRef]
- Baum, E.; Sattabongkot, J.; Sirichaisinthop, J.; Kiattibutr, K.; Jain, A.; Taghavian, O.; Lee, M.C.; Huw Davies, D.; Cui, L.; Felgner, P.L.; et al. Common Asymptomatic and Submicroscopic Malaria Infections in Western Thailand Revealed in Longitudinal Molecular and Serological Studies: A Challenge to Malaria Elimination. Malar. J. 2016, 15, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Eijk, A.M.; Sutton, P.L.; Ramanathapuram, L.; Sullivan, S.A.; Kanagaraj, D.; Priya, G.S.L.; Ravishankaran, S.; Asokan, A.; Sangeetha, V.; Rao, P.N.; et al. The Burden of Submicroscopic and Asymptomatic Malaria in India Revealed from Epidemiology Studies at Three Varied Transmission Sites in India. Sci. Rep. 2019, 9, 17095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, L.; Pereira, N.R.; Andrade, P.; Dias, P.F.; Alves, C.L.; Abreu, C.; Serrão, R.; Ribeiro, M.; Sarmento, A. Prozone-like Phenomenon in Travellers with Fatal Malaria: Report of Two Cases. J. Infect. Dev. Ctries. 2015, 9, 321–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luchavez, J.; Baker, J.; Alcantara, S.; Belizario, V.; Cheng, Q.; McCarthy, J.S.; Bell, D. Laboratory Demonstration of a Prozone-like Effect in HRP2-Detecting Malaria Rapid Diagnostic Tests: Implications for Clinical Management. Malar. J. 2011, 10, 286. [Google Scholar] [CrossRef] [Green Version]
- Sutanto, I.; Kosasih, A.; Elyazar, I.R.F.; Simanjuntak, D.R.; Larasati, T.A.; Dahlan, M.S.; Wahid, I.; Mueller, I.; Koepfli, C.; Kusriastuti, R.; et al. Negligible Impact of Mass Screening and Treatment on Mesoendemic Malaria Transmission at West Timor in Eastern Indonesia: A Cluster-Randomized Trial. Clin. Infect. Dis. 2018, 67, 1364–1372. [Google Scholar] [CrossRef] [Green Version]
- Cook, J.; Xu, W.; Msellem, M.; Vonk, M.; Bergström, B.; Gosling, R.; Al-Mafazy, A.-W.; McElroy, P.; Molteni, F.; Abass, A.K.; et al. Mass Screening and Treatment on the Basis of Results of a Plasmodium Falciparum-Specific Rapid Diagnostic Test Did Not Reduce Malaria Incidence in Zanzibar. J. Infect. Dis. 2015, 211, 1476–1483. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| mRDT | LM | PCR | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 998 | Prevalence n (%) | 95% C.I. | p-Value | Prevalence n (%) | 95% C.I. | p-Value | Prevalence n (%) | 95% C.I. | p-Value | |||
| Lower | Upper | Lower | Upper | Lower | Upper | |||||||
| Sex | ||||||||||||
| Male | 54 (19.9) | 15.1 | 24.6 | 0.723 | 21 (7.7) | 4.5 | 10.9 | 0.298 | 35 (12.9) | 8.9 | 16.8 | 0.7816 |
| Female | 148 (20.9) | 17.9 | 23.9 | 70(9.9) | 7.7 | 12.1 | 96 (13.5) | 11.0 | 16.1 | |||
| Age in years | ||||||||||||
| <5 | 55 (25.3) | 19.6 | 31.1 | <0.001 | 26 (12.0) | 7.7 | 16.3 | 0.001 * | 34 (15.7) | 10.8 | 20.5 | <0.001 * |
| 5–15 | 97 (42.5) | 36.1 | 49.0 | 39 (17.1) | 12.2 | 22.0 | 58 (25.4) | 19.8 | 31.1 | |||
| >15 | 51 (9.7) | 7.2 | 12.3 | 28 (5.3) | 3.4 | 7.3 | 40 (7.6) | 5.4 | 9.9 | |||
| Study site (n) | ||||||||||||
| Handeni (513) | 203 (39.6) | 35.3 | 43.8 | <0.001 | 89 (16.9) | 13.7 | 20.1 | <0.001 | 116 (22.1) | 18.5 | 25.6 | <0.001 |
| Moshi (472) | 1 (0.2) | −0.2 | 0.6 | 6 (1.3) | 0.3 | 2.3 | 19 (4.0) | 2.3 | 5.8 | |||
| Sensitivity Value 95% C.I. | Specificity Value 95% C.I. | PPV Value 95% C.I. | NPV Value 95% C.I. | Likelihood ratio | Agreement (%) | Kappa Value 95% C.I. | ||
|---|---|---|---|---|---|---|---|---|
| Positive Test Value 95% C.I. | Negative Test Value 95% C.I. | |||||||
| PCR vs. LM | 88.42 | 94.35 | 62.22 | 98.73 | 15.65 | 8.15 | 93.79 | 0.70 |
| 86.44–90.41 | 92.92–95.78 | 59.21–65.23 | 98.03–99.42 | 12.21–21.42 | 6.85–9.99 | 0.63–0.77 | ||
| PCR vs. mRDT | 75.27 | 84.98 | 34.31 | 97.06 | 5.01 | 3.44 | 84.67 | 0.39 |
| 72.57–77.96 | 82.75–87.21 | 31.35–37.28 | 96.00–98.11 | 4.21–6.10 | 3.02–3.96 | 0.32–0.47 | ||
| LM vs. mRDT | 34.31 | 97.06 | 75.27 | 84.98 | 11.67 | 1.48 | 84.06 | 0.39 |
| 31.35–37.28 | 96.00–98.11 | 72.57–77.96 | 82.75–87.21 | 7.84–19.72 | 1.40–1.56 | 0.32–0.47 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaaya, R.D.; Matowo, J.; Kajeguka, D.; Tenu, F.; Shirima, B.; Mosha, F.; Kavishe, R. The Impact of Submicroscopic Parasitemia on Malaria Rapid Diagnosis in Northeastern Tanzania, an Area with Diverse Transmission Patterns. Infect. Dis. Rep. 2022, 14, 798-809. https://doi.org/10.3390/idr14060082
Kaaya RD, Matowo J, Kajeguka D, Tenu F, Shirima B, Mosha F, Kavishe R. The Impact of Submicroscopic Parasitemia on Malaria Rapid Diagnosis in Northeastern Tanzania, an Area with Diverse Transmission Patterns. Infectious Disease Reports. 2022; 14(6):798-809. https://doi.org/10.3390/idr14060082
Chicago/Turabian StyleKaaya, Robert Diotrephes, Johnson Matowo, Debora Kajeguka, Filemoni Tenu, Boniface Shirima, Franklin Mosha, and Reginald Kavishe. 2022. "The Impact of Submicroscopic Parasitemia on Malaria Rapid Diagnosis in Northeastern Tanzania, an Area with Diverse Transmission Patterns" Infectious Disease Reports 14, no. 6: 798-809. https://doi.org/10.3390/idr14060082