
Linked Color Imaging of Barrett’s Esophageal Adenocarcinoma: Effects on Visibility
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials for Visibility Evaluation
2.2. Esophagogastroduodenoscopy and Endoscopic Findings
2.3. Evaluator of Visibility Score
2.4. Scoring for Visibility
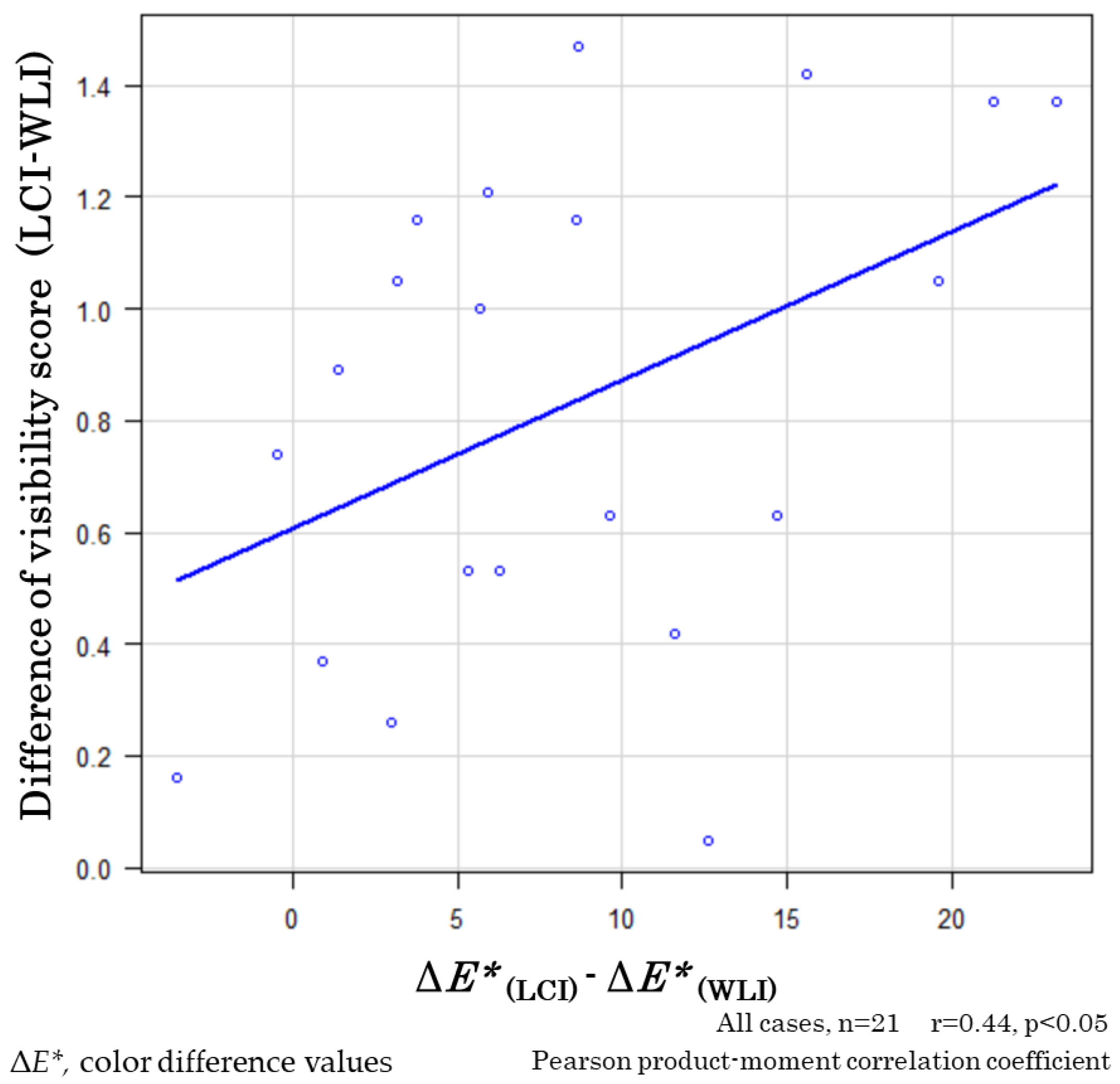
2.5. Comparing Visibility Scores and Color Difference (ΔE*)
2.6. Statistical Analysis
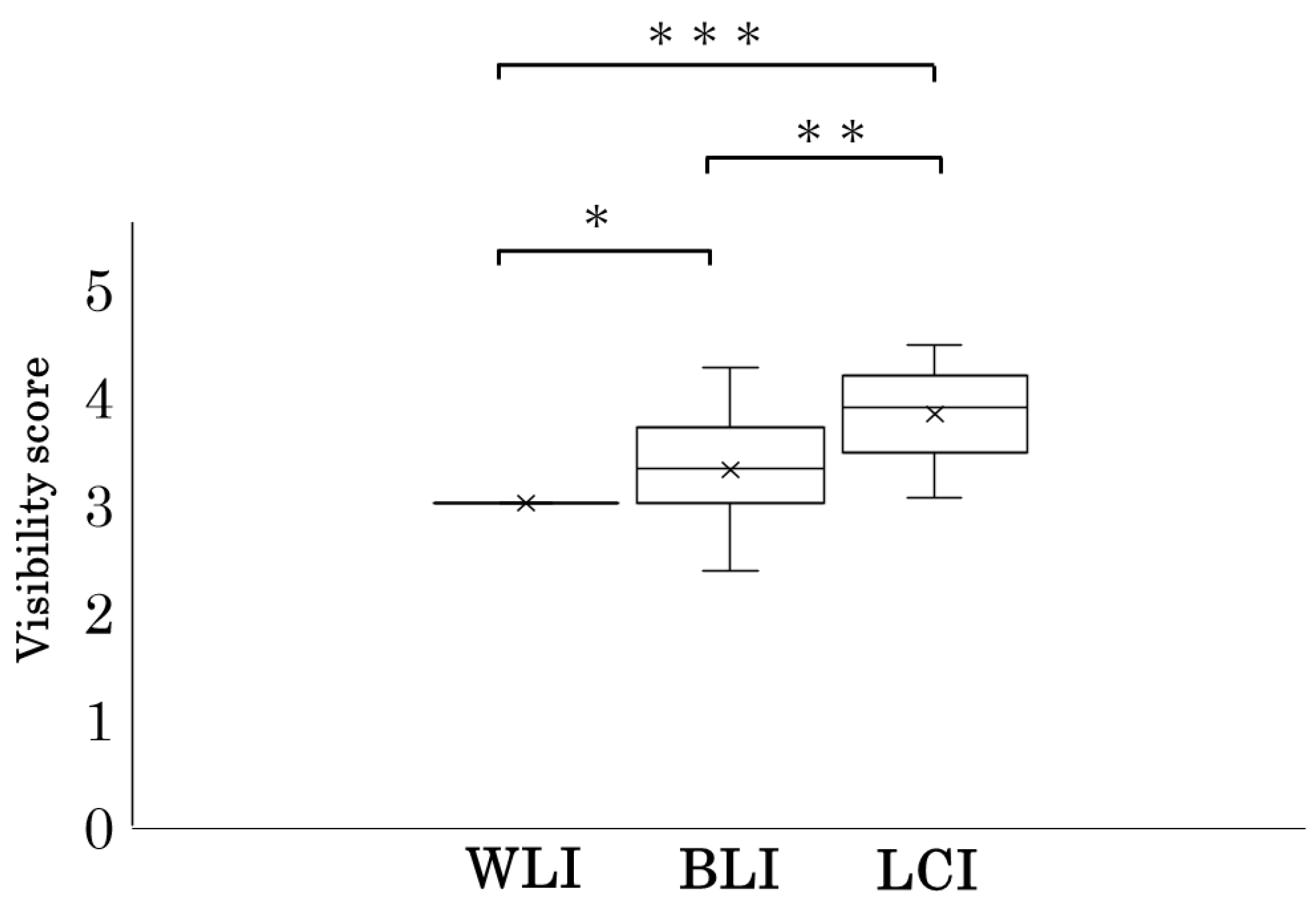
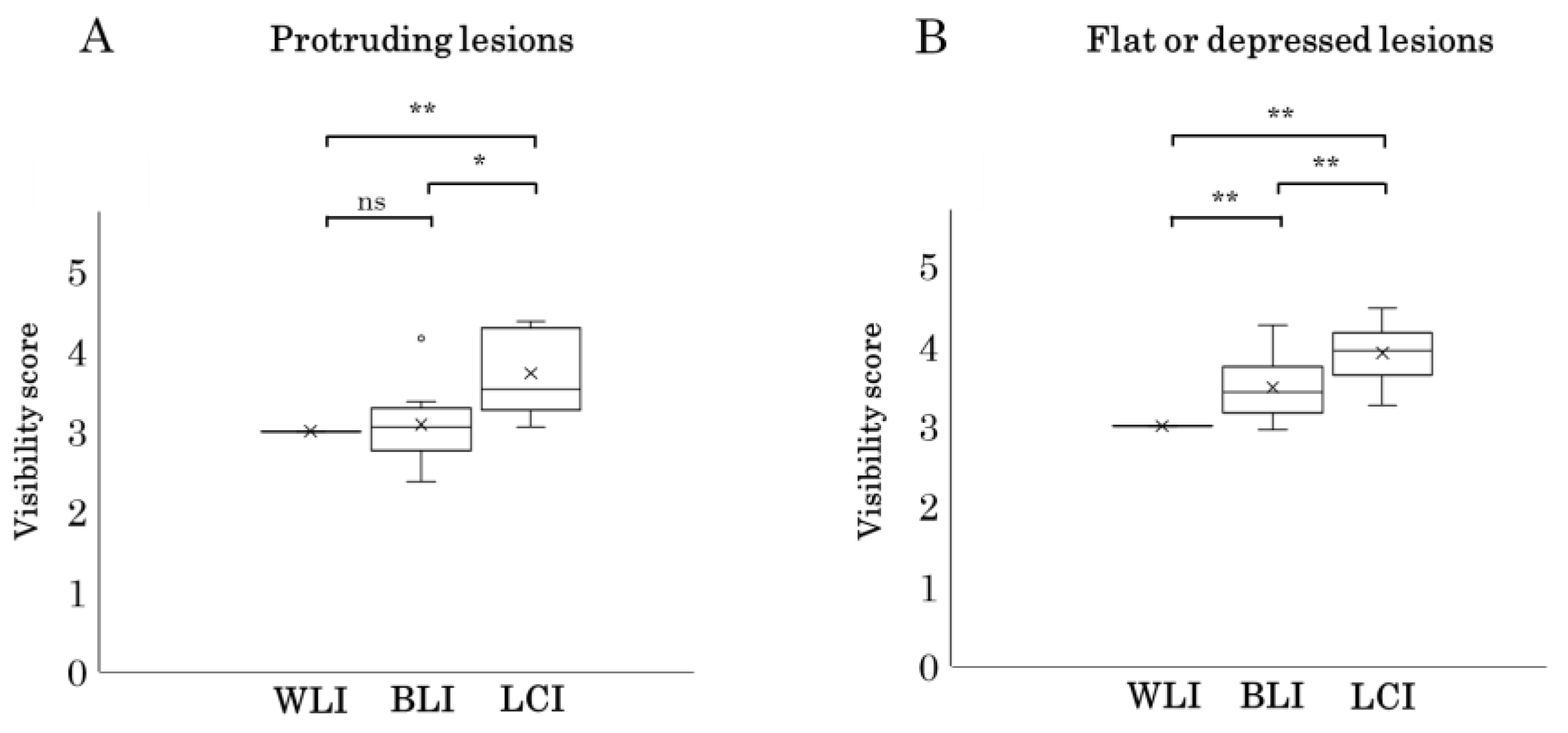
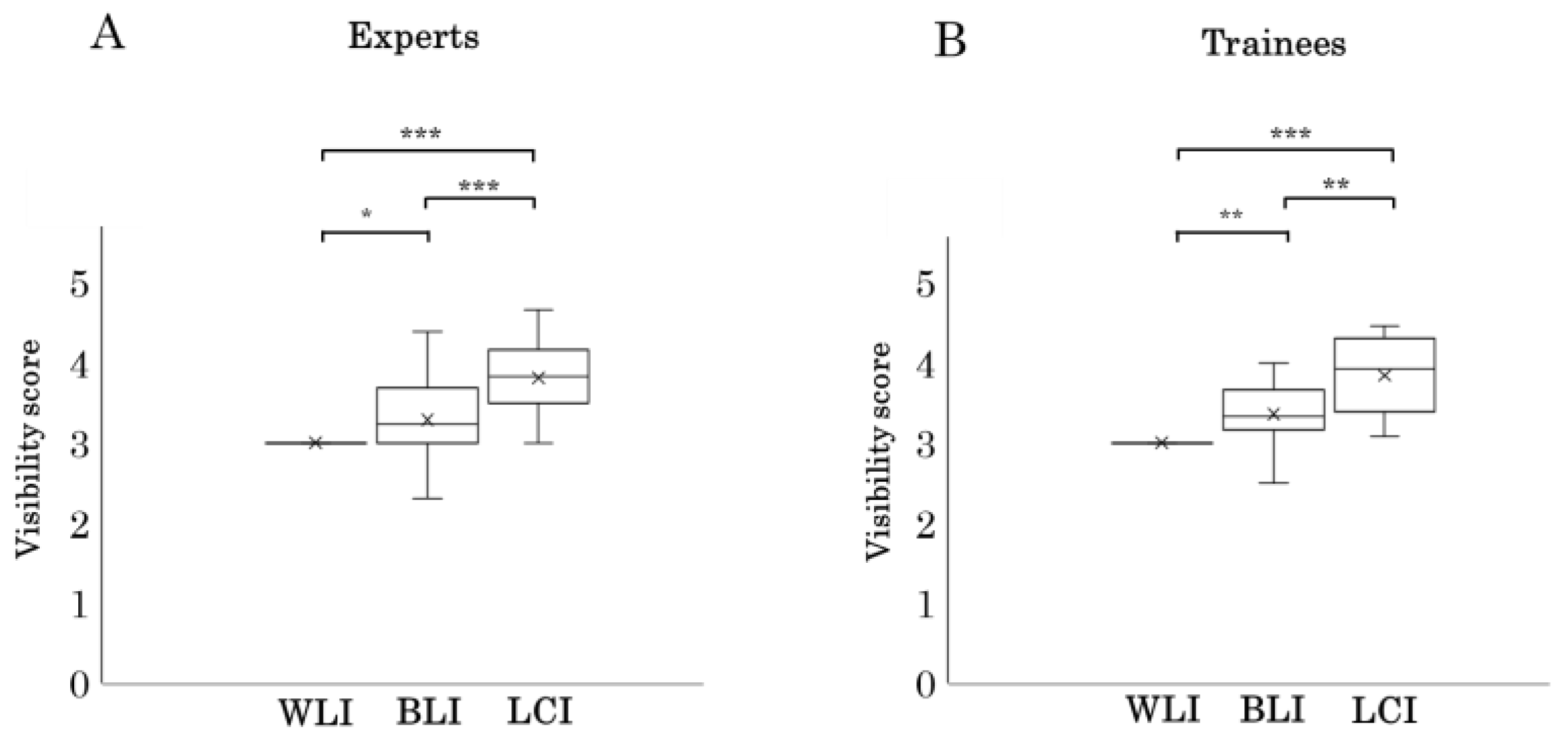
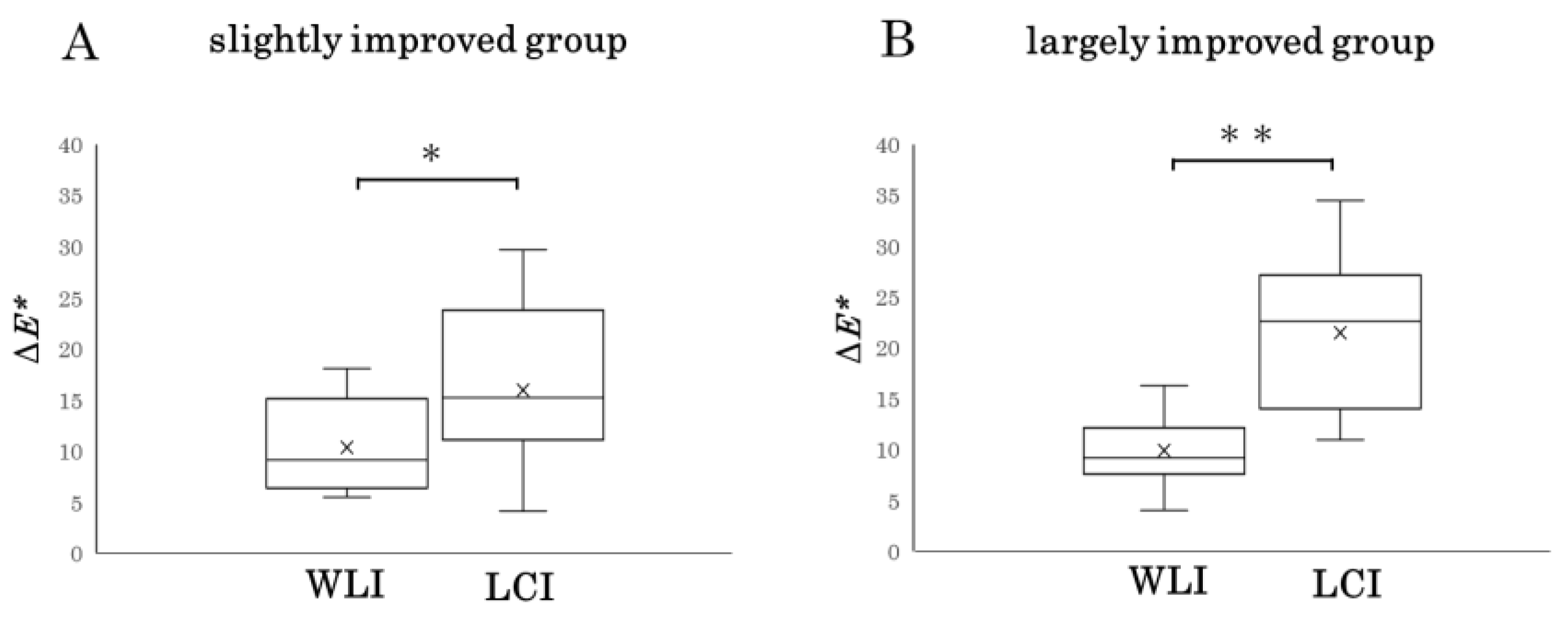
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pohl, H.; Sirovich, B.; Welch, H.G. Esophageal adenocarcinoma incidence: Are we reaching the peak? Cancer Epidemiol. Biomark. Prev. 2010, 19, 1468–1470. [Google Scholar] [CrossRef]
- Matsuno, K.; Ishihara, R.; Ohmori, M.; Iwagami, H.; Shichijyo, S.; Maekawa, A.; Kanesaka, T.; Yamamoto, S.; Takeuchi, Y.; Higashino, K.; et al. Time trends in the incidence of esophageal adenocarcinoma, gastric adenocarcinoma, and superficial esophagogastric junction adenocarcinoma. J. Gastroenterol. 2019, 54, 784–791. [Google Scholar] [CrossRef]
- Koike, T.; Saito, M.; Ohara, Y.; Hatta, W.; Masamune, A. Current status of surveillance for Barrett’s esophagus in Japan and the West. DEN Open 2022, 13, e94. [Google Scholar] [CrossRef]
- Hur, C.; Miller, M.; Kong, C.Y.; Dowling, E.C.; Nattinger, K.J.; Dunn, M.; Feuer, E.J. Trends in esophageal adenocarcinoma incidence and mortality. Cancer 2013, 119, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, R.; Goda, K.; Oyama, T. Endoscopic diagnosis and treatment of esophageal adenocarcinoma: Introduction of Japan Esophageal Society classification of Barrett’s esophagus. J. Gastroenterol. 2019, 54, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Probst, A.; Aust, D.; Märkl, B.; Anthuber, M.; Messmann, H. Early esophageal cancer in Europe: Endoscopic treatment by endoscopic submucosal dissection. Endoscopy 2015, 47, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Thosani, N.; Abu Dayyeh, B.K.; Sharma, P.; Aslanian, H.R.; Enestvedt, B.K.; Komanduri, S.; Manfredi, M.; Navaneethan, U.; Maple, J.T.; Pannala, R.; et al. ASGE Technology Committee systematic review and meta-analysis assessing the ASGE Preservation and incorporation of valuable endoscopic innovations thresholds for adopting realtime imaging-assisted endoscopic targeted biopsy during endoscopic surveillance of Barrett’s esophagus. Gastrointest. Endosc. 2016, 83, 684–698. [Google Scholar]
- Shinozaki, S.; Osawa, H.; Hayashi, Y.; Lefor, A.K.; Yamamoto, H. Linked Color Imaging for the Detection of Early Gastrointestinal Neoplasms. Ther. Adv. Gastroenterol. 2019, 12, 1756284819885246. [Google Scholar] [CrossRef] [PubMed]
- Osawa, H.; Miura, Y.; Takezawa, T.; Ino, Y.; Khurelbaatar, T.; Sagara, Y.; Lefor, A.K.; Yamamoto, H. Linked Color Imaging and Blue Laser Imaging for Upper Gastrointestinal Screening. Clin. Endosc. 2018, 51, 513–526. [Google Scholar] [CrossRef] [PubMed]
- Yoshifuku, Y.; Sanomura, Y.; Oka, S.; Kurihara, M.; Mizumoto, T.; Miwata, T.; Urabe, Y.; Hiyama, T.; Tanaka, S.; Chayama, K. Evaluation of the visibility of early gastric cancer using linked color imaging and blue laser imaging. BMC Gastroenterol. 2017, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Kanzaki, H.; Takenaka, R.; Kawahara, Y.; Kawai, D.; Obayashi, Y.; Baba, Y.; Sakae, H.; Gotoda, T.; Kono, Y.; Miura, K.; et al. Linked color imaging (LCI), a novel image-enhanced endoscopy technology, emphasizes the color of early gastric cancer. Endosc. Int. Open 2017, 5, E1005–E1013. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Miura, Y.; Osawa, H.; Takezawa, T.; Ino, Y.; Okada, M.; Khurelbaatar, T.; Lefor, A.K.; Yamamoto, H. Linked color imaging can enhance recognition of early gastric cancer by high color contrast to surrounding gastric intestinal metaplasia. J. Gastroenterol. 2019, 54, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Paggi, S.; Mogavero, G.; Amato, A.; Rondonotti, E.; Andrealli, A.; Imperiali, G.; Lenoci, N.; Mandelli, G.; Terreni, N.; Conforti, F.S.; et al. Linked color imaging reduces the miss rate of neoplastic lesions in the right colon: A randomized tandem colonoscopy study. Endoscopy 2018, 50, 396–402. [Google Scholar] [PubMed]
- Okimoto, K.; Maruoka, D.; Matsumura, T.; Tokunaga, M.; Kaneko, T.; Oura, H.; Akizue, N.; Ohta, Y.; Saito, K.; Arai, M.; et al. Linked color imaging can improve the visibility of superficial non-ampullary duodenal epithelial tumors. Sci. Rep. 2020, 10, 20667. [Google Scholar] [CrossRef] [PubMed]
- Takeda, T.; Asaoka, D.; Abe, D.; Suzuki, M.; Nakagawa, Y.; Sasaki, H.; Inami, Y.; Ikemura, M.; Utsunomiya, H.; Oki, S.; et al. Linked color imaging improves visibility of reflux esophagitis. BMC Gastroenterol. 2020, 20, 356. [Google Scholar] [CrossRef] [PubMed]
- Abe, Y.; Sasaki, Y.; Yagi, M.; Mizumoto, N.; Onozato, Y.; Kon, T.; Shoji, M.; Sakuta, K.; Sakai, T.; Umehara, M.; et al. Linked color imaging improves the diagnostic accuracy of eosinophilic esophagitis. DEN Open 2022, 3, e146. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Kawada, K.; Dohi, O.; Kitamura, S.; Koike, T.; Hori, S.; Kanzaki, H.; Murao, T.; Yagi, N.; Sasaki, F.; et al. Linked Color Imaging Focused on Neoplasm Detection in the Upper Gastrointestinal Tract: A Randomized Trial. Ann. Intern. Med. 2021, 174, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Haruma, K.; Kato, M.; Kawada, K.; Murao, T.; Ono, S.; Suehiro, M.; Hori, S.; Sasaki, F.; Koike, T.; Kitamura, S.; et al. Diagnostic ability of linked color imaging in ultraslim endoscopy to identify neoplastic lesions in upper gastrointestinal tract. Endosc. Int. Open 2022, 10, E88–E95. [Google Scholar] [CrossRef]
- Saito, M.; Koike, T.; Ohara, Y.; Nakagawa, K.; Kanno, T.; Jin, X.; Hatta, W.; Uno, K.; Asano, N.; Imatani, A.; et al. Linked-color imaging may help improve the visibility of superficial Barrett’s esophageal adenocarcinoma by increasing the color difference. Intern. Med. 2021, 60, 3351–3358. [Google Scholar] [CrossRef]
- Tokunaga, M.; Matsumura, T.; Ishikawa, K.; Kaneko, T.; Oura, H.; Ishikawa, T.; Nagashima, A.; Shiratori, W.; Okimoto, K.; Akizue, N.; et al. The efficacy of linked color imaging in the endoscopic diagnosis of Barrett’s esophagus and esophageal adenocarcinoma. Gastroenterol. Res. Pract. 2020, 2020, 9604345. [Google Scholar] [CrossRef]
- de Groof, A.J.; Fockens, K.N.; Struyvenberg, M.R.; Pouw, R.E.; Weusten, B.L.; Schoon, E.J.; Mostafavi, N.; Bisschops, R.; Curvers, W.L.; Bergman, J.J. Blue-light imaging and linked-color imaging improve visualization of Barrett’s neoplasia by nonexpert endoscopists. Gastrointest. Endosc. 2020, 91, 1050–1057. [Google Scholar] [CrossRef]
- Takeda, T.; Nagahara, A.; Ishizuka, K.; Okubo, S.; Haga, K.; Suzuki, M.; Nakajima, A.; Komori, H.; Akazawa, Y.; Izumi, K.; et al. Improved visibility of Barrett’s esophagus with linked color imaging: Inter- and intra-rater reliability and quantitative analysis. Digestion 2018, 97, 183–194. [Google Scholar] [CrossRef]
- Japan Esophageal Society. Japanese Classification of Esophageal Cancer, 11th Edition: Part I. Esophagus 2017, 14, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Japan Esophageal Society. Japanese Classification of Esophageal Cancer, 11th Edition: Part II and III. Esophagus 2017, 14, 37–65. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely-available easy-to-use software “EZR” (Easy R) for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Ogata, Y.; Hatta, W.; Koike, T.; Takahashi, S.; Matsuhashi, T.; Oikawa, T.; Iwai, W.; Asonuma, S.; Okata, H.; Ohyauchi, M.; et al. Blue light imaging and linked color imaging as a screening mode for esophageal squamous cell carcinoma in high-risk patients: Multicenter randomized trial. Dig. Endosc. 2023, 35, 835–844. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | ||
|---|---|---|---|
| Total lesions (n = 21) | |||
| Color | Reddish | 18 | (85.7%) |
| Similar color to the surroundings or discolored | 3 | (14.3%) | |
| Form | Protruding | 9 | |
| Type 0—I | 3 | (14.3%) | |
| Type 0—IIa | 5 | (23.8%) | |
| Type 0—IIa + IIc | 1 | (4.8%) | |
| Flat or depressed | 12 | ||
| Type 0—IIb | 2 | (9.5%) | |
| Type 0—IIc | 10 | (47.6%) | |
| Barrett’s mucosa | SSBE | 17 | (80.9%) |
| LSBE | 4 | (19.1%) | |
| Circumferential location | 0–3 o’clock direction | 17 | (80.9%) |
| Other direction | 4 | (19.1%) | |
| The diameter of the lesions | mm, median (IQR) | 14 (11) |
| Color of the BA Lesion | Reddish (n = 18) | Discolored (n = 3) |
|---|---|---|
| WLI | - | - |
| BLI | - | 2 * |
| LCI | 18 | 2 * |
| SSBE or LSBE | SSBE (n = 17) | LSBE (n = 4) |
| WLI | - | - |
| BLI | 1 * | 1 |
| LCI | 17 * | 3 |
| Circumference of the BA Lesion | 0–3 O’Clock (n = 17) | Other (n = 4) |
| WLI | - | - |
| BLI | 1 * | 1 |
| LCI | 17 * | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, M.; Koike, T.; Ohara, Y.; Ogata, Y.; Kanno, T.; Jin, X.; Hatta, W.; Uno, K.; Asano, N.; Imatani, A.; et al. Linked Color Imaging of Barrett’s Esophageal Adenocarcinoma: Effects on Visibility. Gastroenterol. Insights 2024, 15, 145-155. https://doi.org/10.3390/gastroent15010010
Saito M, Koike T, Ohara Y, Ogata Y, Kanno T, Jin X, Hatta W, Uno K, Asano N, Imatani A, et al. Linked Color Imaging of Barrett’s Esophageal Adenocarcinoma: Effects on Visibility. Gastroenterology Insights. 2024; 15(1):145-155. https://doi.org/10.3390/gastroent15010010
Chicago/Turabian StyleSaito, Masahiro, Tomoyuki Koike, Yuki Ohara, Yohei Ogata, Takeshi Kanno, Xiaoyi Jin, Waku Hatta, Kaname Uno, Naoki Asano, Akira Imatani, and et al. 2024. "Linked Color Imaging of Barrett’s Esophageal Adenocarcinoma: Effects on Visibility" Gastroenterology Insights 15, no. 1: 145-155. https://doi.org/10.3390/gastroent15010010