
Persistent 18F-FDG Brain PET Fronto-Temporal Hypometabolism and Cognitive Symptoms Two Years after SARS-CoV-2 Infection: A Case Report
 ,
,
Abstract
:1. Introduction
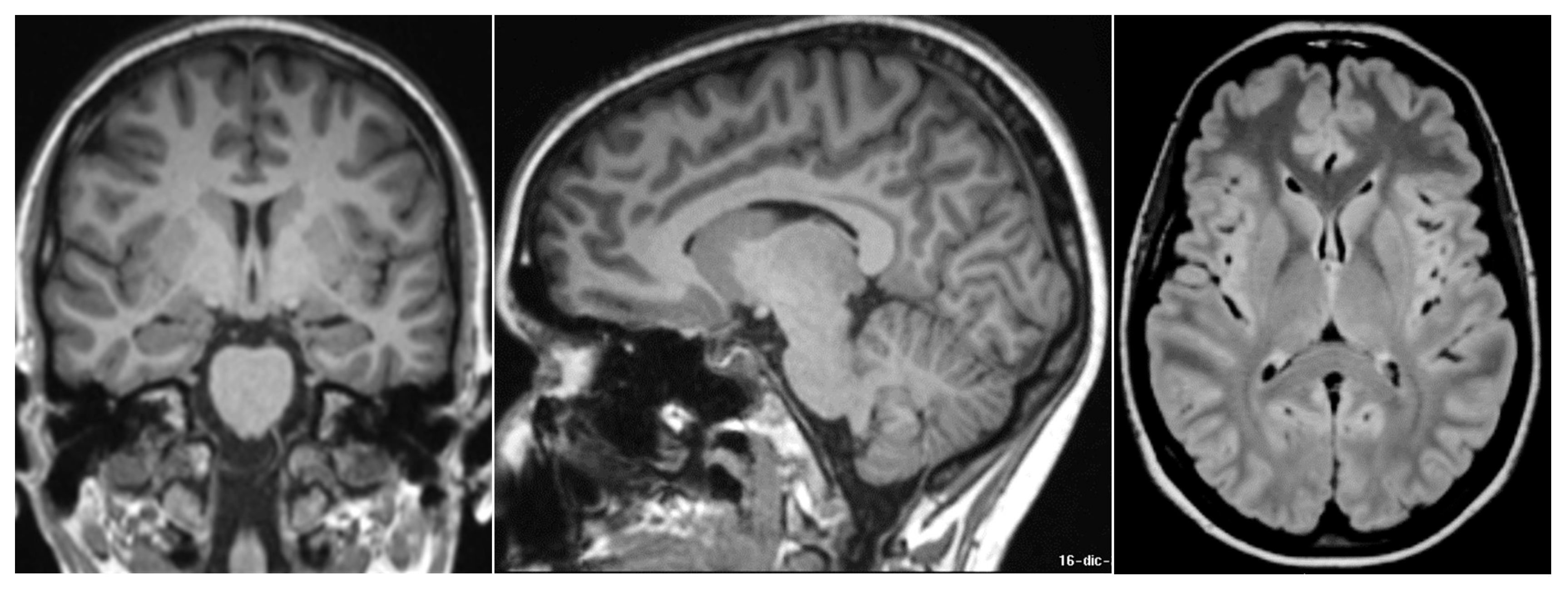
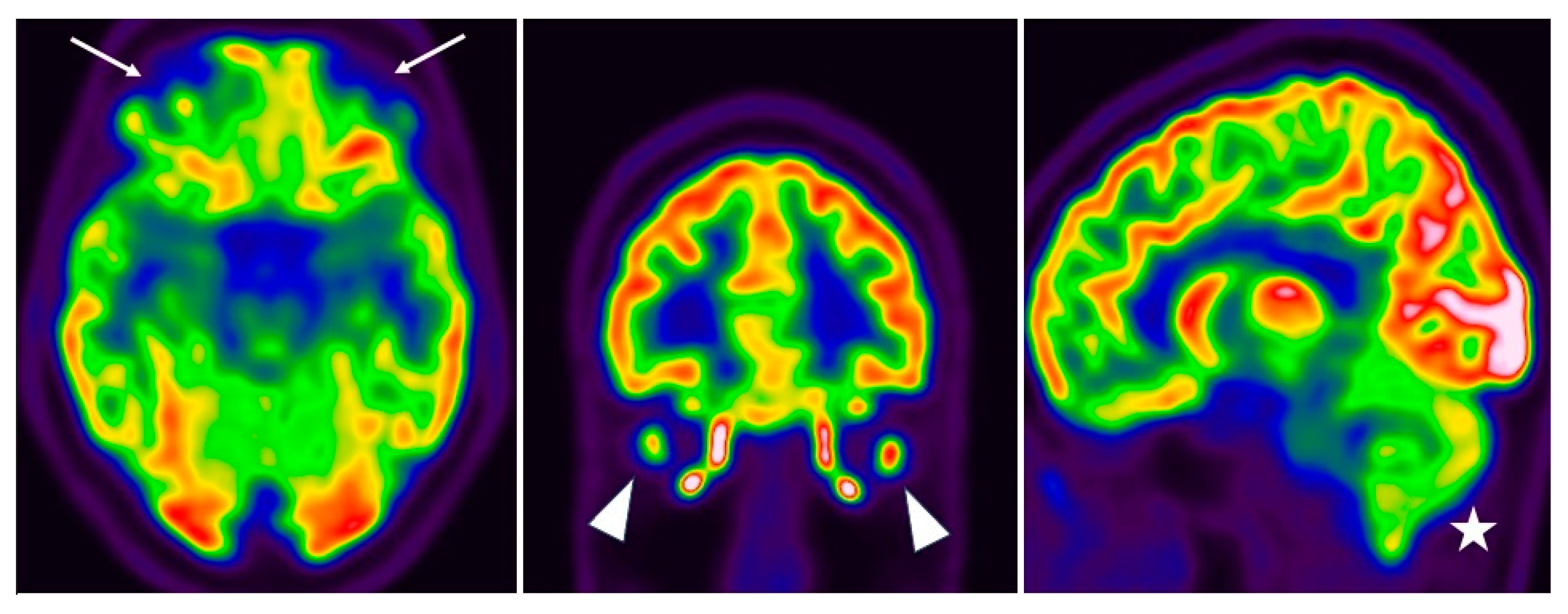
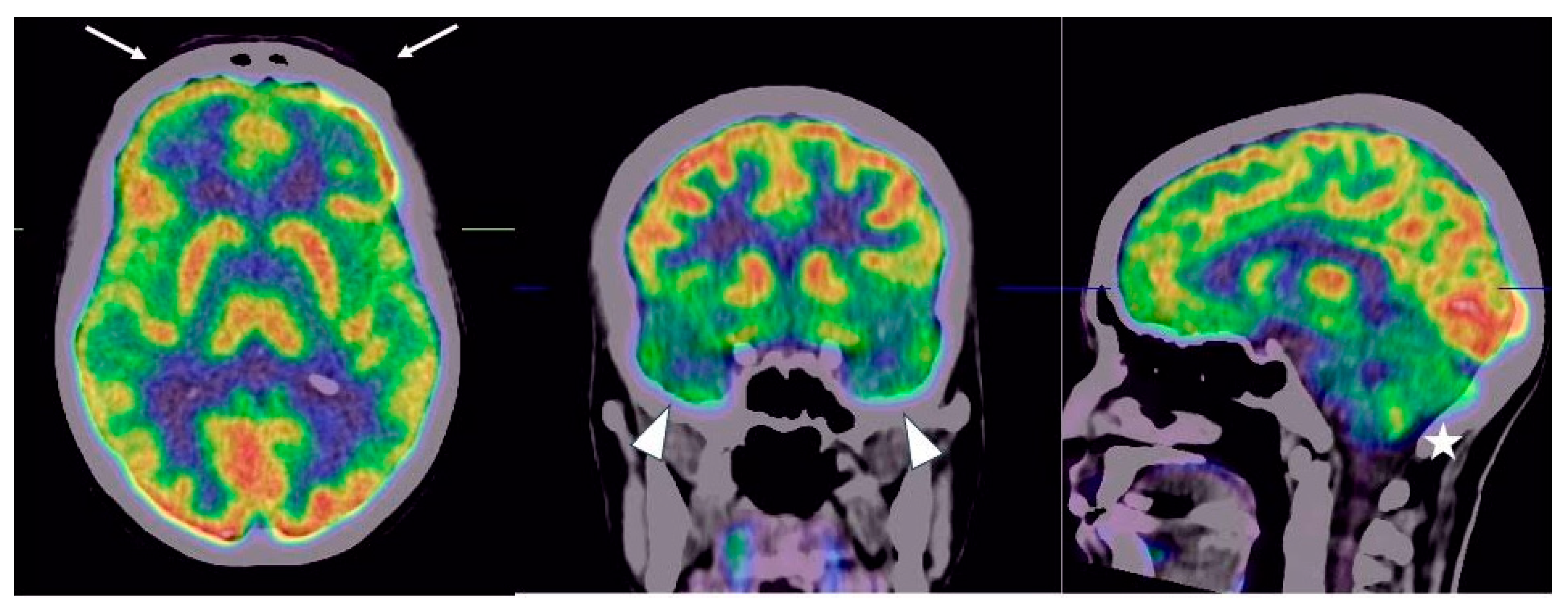
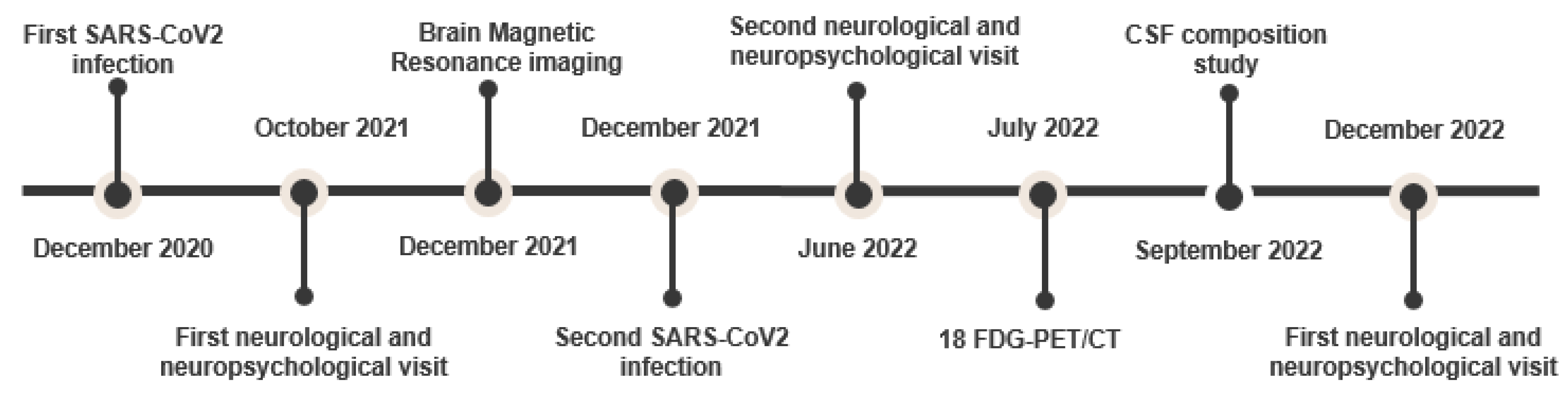
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Stefanou, M.-I.; Palaiodimou, L.; Bakola, E.; Smyrnis, N.; Papadopoulou, M.; Paraskevas, G.P.; Rizos, E.; Boutati, E.; Grigoriadis, N.; Krogias, C.; et al. Neurological manifestations of long-COVID syndrome: A narrative review. Ther. Adv. Chronic Dis. 2022, 13, 204062232210768. [Google Scholar] [CrossRef]
- Nehme, M.; Braillard, O.; Alcoba, G.; Perone, S.A.; Courvoisier, D.; Chappuis, F.; Guessous, I. COVID-19 Symptoms: Longitudinal Evolution and Persistence in Outpatient Settings. Ann. Intern. Med. 2021, 174, 723–725. [Google Scholar] [CrossRef]
- Global Burden of Disease Long COVID Collaborators; Hanson, S.W.; Abbafati, C.; Aerts, J.G.; Al-Aly, Z.; Ashbaugh, C.; Ballouz, T.; Blyuss, O.; Bobkova, P.; Bonsel, G.; et al. Estimated Global Proportions of Individuals With Persistent Fatigue, Cognitive, and Respiratory Symptom Clusters Following Symptomatic COVID-19 in 2020 and 2021. JAMA 2022, 328, 1604–1615. [Google Scholar] [CrossRef]
- Monje, M.; Iwasaki, A. The neurobiology of long COVID. Neuron 2022, 110, 3484–3496. [Google Scholar] [CrossRef]
- Lechner-Scott, J.; Levy, M.; Hawkes, C.; Yeh, A.; Giovannoni, G. Long COVID or post COVID-19 syndrome. Mult. Scler. Relat. Disord. 2021, 55, 103268. [Google Scholar] [CrossRef]
- Ceban, F.; Ling, S.; Lui, L.M.; Lee, Y.; Gill, H.; Teopiz, K.M.; Rodrigues, N.B.; Subramaniapillai, M.; Di Vincenzo, J.D.; Cao, B.; et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis. Brain, Behav. Immun. 2022, 101, 93–135. [Google Scholar] [CrossRef]
- Crivelli, L.; Palmer, K.; Calandri, I.; Guekht, A.; Beghi, E.; Carroll, W.; Frontera, J.; García-Azorín, D.; Westenberg, E.; Winkler, A.S.; et al. Changes in cognitive functioning after COVID-19: A systematic review and meta-analysis. Alzheimer’s Dement. 2022, 18, 1047–1066. [Google Scholar] [CrossRef]
- Rudroff, T.; Workman, C.D.; Ponto, L.L.B. 18F-FDG-PET Imaging for Post-COVID-19 Brain and Skeletal Muscle Alterations. Viruses 2021, 13, 2283. [Google Scholar] [CrossRef]
- Tavares-Júnior, J.W.; de Souza, A.C.; Borges, J.W.; Oliveira, D.N.; Siqueira-Neto, J.I.; Sobreira-Neto, M.A.; Braga-Neto, P. COVID-19 associated cognitive impairment: A systematic review. Cortex 2022, 152, 77–97. [Google Scholar] [CrossRef]
- Tana, C.; Bentivegna, E.; Cho, S.-J.; Harriott, A.M.; García-Azorín, D.; Labastida-Ramirez, A.; Ornello, R.; Raffaelli, B.; Beltrán, E.R.; Ruscheweyh, R.; et al. Long COVID headache. J. Headache Pain 2022, 23, 93. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Jackson, C. The Chalder Fatigue Scale (CFQ 11). Occup. Med. 2014, 65, 86. [Google Scholar] [CrossRef] [Green Version]
- Brickenkamp, R.; Zilmer, E. The d2 Test of Attention; Hogrefe and Huber Publishers: Seattle, WA, USA, 1998. [Google Scholar] [CrossRef]
- Rey, A. L ‘examen clinique en psychologie. In Clinical Tests in Psychology; Presses Universitaires de France: Paris, France, 1964. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s Dement. 2018, 14, 535–562. [Google Scholar] [CrossRef]
- Janelidze, S.; Stomrud, E.; Palmqvist, S.; Zetterberg, H.; van Westen, D.; Jeromin, A.; Song, L.; Hanlon, D.; Hehir, C.A.T.; Baker, D.; et al. Plasma β-amyloid in Alzheimer’s disease and vascular disease. Sci. Rep. 2016, 6, 26801. [Google Scholar] [CrossRef] [Green Version]
- Lewczuk, P.; Mroczko, B.; Fagan, A.; Kornhuber, J. Biomarkers of Alzheimer’s disease and mild cognitive impairment: A current perspective. Adv. Med. Sci. 2015, 60, 76–82. [Google Scholar] [CrossRef]
- Graus, F.; Vogrig, A.; Muñiz-Castrillo, S.; Antoine, J.-C.G.; Desestret, V.; Dubey, D.; Giometto, B.; Irani, S.R.; Joubert, B.; Leypoldt, F.; et al. Updated Diagnostic Criteria for Paraneoplastic Neurologic Syndromes. Neurol. Neuroimmunol. Neuroinflammation 2021, 8, e1014. [Google Scholar] [CrossRef]
- Sirkis, D.W.; Bonham, L.W.; Johnson, T.P.; La Joie, R.; Yokoyama, J.S. Dissecting the clinical heterogeneity of early-onset Alzheimer’s disease. Mol. Psychiatry 2022, 27, 2674–2688. [Google Scholar] [CrossRef]
- Knopman, D.S.; Amieva, H.; Petersen, R.C.; Chételat, G.; Holtzman, D.M.; Hyman, B.T.; Nixon, R.A.; Jones, D.T. Alzheimer disease. Nat. Rev. Dis. Prim. 2021, 7, 115–140. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. J. Alzheimers Assoc. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Crockett, D.J.; Hadjistavropoulos, T.; Hurwitz, T. Primacy and recency effects in the assessment of memory using the Rey Auditory Verbal Learning Test. Arch. Clin. Neuropsychol. 1992, 7, 97–107. [Google Scholar] [PubMed]
- Waugh, N.C.; Norman, D.A. Primary memory. Psychol. Rev. 1965, 72, 89–104. [Google Scholar] [CrossRef]
- Consonni, M.; Rossi, S.; Cerami, C.; Marcone, A.; Iannaccone, S.; Cappa, S.F.; Perani, D. Executive dysfunction affects word list recall performance: Evidence from amyotrophic lateral sclerosis and other neurodegenerative diseases. J. Neuropsychol. 2015, 11, 74–90. [Google Scholar] [CrossRef]
- Cian, V.; De Laurenzis, A.; Siri, C.; Gusmeroli, A.; Canesi, M. Cognitive and Neuropsychiatric Features of COVID-19 Patients After Hospital Dismission: An Italian Sample. Front. Psychol. 2022, 13, 908363. [Google Scholar] [CrossRef]
- Hugon, J. Long-COVID: Cognitive deficits (brain fog) and brain lesions in non–hospitalized patients. Presse Médicale 2022, 51, 104090. [Google Scholar] [CrossRef]
- Hugon, J.; Msika, E.-F.; Queneau, M.; Farid, K.; Paquet, C. Long COVID: Cognitive complaints (brain fog) and dysfunction of the cingulate cortex. J. Neurol. 2021, 269, 44–46. [Google Scholar] [CrossRef]
- Yu, A.T.; Absar, N.M. Long-term Neuropsychiatric Complications and 18F-FDG-PET Hypometabolism in the Brain From Prolonged Infection of COVID-19. Alzheimer Dis. Assoc. Disord. 2021, 36, 173–175. [Google Scholar] [CrossRef]
- Guedj, E.; Campion, J.Y.; Dudouet, P.; Kaphan, E.; Bregeon, F.; Tissot-Dupont, H.; Guis, S.; Barthelemy, F.; Habert, P.; Ceccaldi, M.; et al. 18F-FDG brain PET hypometabolism in patients with long COVID. Eur. J. Nucl. Med. 2021, 48, 2823–2833. [Google Scholar] [CrossRef]
- Morand, A.; Campion, J.-Y.; Lepine, A.; Bosdure, E.; Luciani, L.; Cammilleri, S.; Chabrol, B.; Guedj, E. Similar patterns of [18F]-FDG brain PET hypometabolism in paediatric and adult patients with long COVID: A paediatric case series. Eur. J. Nucl. Med. 2021, 49, 913–920. [Google Scholar] [CrossRef]
- Toniolo, S.; Di Lorenzo, F.; Scarioni, M.; Frederiksen, K.S.; Nobili, F. Is the Frontal Lobe the Primary Target of SARS-CoV-2? J. Alzheimer’s Dis. 2021, 81, 75–81. [Google Scholar] [CrossRef]
- Herholz, K.; Salmon, E.; Perani, D.; Baron, J.-C.; Holthoff, V.; Frölich, L.; Schönknecht, P.; Ito, K.; Mielke, R.; Kalbe, E. Discrimination between Alzheimer Dementia and Controls by Automated Analysis of Multicenter FDG PET. Neuroimage 2002, 17, 302–316. [Google Scholar] [CrossRef] [Green Version]
- Dressing, A.; Bormann, T.; Blazhenets, G.; Schroeter, N.; Walter, L.I.; Thurow, J.; August, D.; Hilger, H.; Stete, K.; Gerstacker, K.; et al. Neuropsychologic Profiles and Cerebral Glucose Metabolism in Neurocognitive Long COVID Syndrome. J. Nucl. Med. 2021, 63, 1058–1063. [Google Scholar] [CrossRef]
- Blazhenets, G.; Schroeter, N.; Bormann, T.; Thurow, J.; Wagner, D.; Frings, L.; Weiller, C.; Meyer, P.T.; Dressing, A.; A Hosp, J. Slow but evident recovery from neocortical dysfunction and cognitive impairment in a series of chronic COVID-19 patients. J. Nucl. Med. 2021, 62, 910–915. [Google Scholar] [CrossRef]
- Ferrucci, R.; Cuffaro, L.; Capozza, A.; Rosci, C.; Maiorana, N.; Groppo, E.; Reitano, M.R.; Poletti, B.; Ticozzi, N.; Tagliabue, L.; et al. Brain positron emission tomography (PET) and cognitive abnormalities one year after COVID-19. J. Neurol. 2023, 270, 1823–1834. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Task | Visit 1 | Visit 2 | Visit 3 |
|---|---|---|---|
| MoCA | 28/30 | 26/30 | 28/30 |
| Digit Span forward | 6/9 | 6/9 | 5/9 |
| Digit Span backward | 5/9 | 5/9 | 5/9 |
| Rey auditory verbal learning test (AVLT): Immediate total recall | 43/75 | 40/75 * | 37/75 * |
| Rey auditory verbal learning test (AVLT): Delayed total recall | 11/15 | 8/15 * | 5/15 * |
| Rey auditory verbal learning test (AVLT): Delayed recognition | 14/15 | 10/15 | 10/15 |
| D2 Sustained-Attention Test: speed | 130 * | 133 * | 119 * |
| D2 Sustained-Attention Test: error rate (%) | 5.2 | 3.07 | 3.3 |
| D2 Sustained-Attention Test: performance | 126 | 126 | 114 |
| Modified Five Point Test: unique designs | 34 | 55.8 | -- |
| Modified Five Point Test: strategy score | 40 | 67.5 | -- |
| Modified Five Point Test: percentage of perseverations | 2.94 | 2.5 | |
| Phonemic Fluency | 36 | 37 | |
| Chalder Fatigue Scale (CFS-11) | 8/11 * | -- | 1/11 |
| Hospital Anxiety and Depression scale (HADS): Anxiety | -- | 3/21 | 4/21 |
| Hospital Anxiety and Depression scale (HADS): Depression | -- | 2/21 | 4/21 |
| Parameters | Results |
|---|---|
| Appearance | Clear |
| Protein | 321 mg/L |
| Leukocytes | 0.7 Lc/μL |
| Albumin | 205 mg/L |
| Oligoclonal bands | 0 |
| Tau protein (normal reference < 452 ng/L) | 201 ng/L |
| P Tau protein (normal reference < 61 ng/L) | 33 ng/L |
| Aß42 (normal reference > 630 ng/L) | 1730 ng/L |
| Aß40 | 8239 |
| Ratio Aß42/40 (ref. > 0.1) | 0.21 |
| Anti-NMDAR, IgG | Negative |
| Anti-CASPR2, IgG | Negative |
| Anti-LGI1, IgG | Negative |
| Anti-DPPX | Negative |
| Anti-AMPA-R | Negative |
| Anti-IgLON5R | Negative |
| Anti-mGluR5 | Negative |
| Anti-GlyR | Negative |
| Negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, S.; Prodi, E.; Morese, R.; Paone, G.; Ruberto, T.; Sacco, L. Persistent 18F-FDG Brain PET Fronto-Temporal Hypometabolism and Cognitive Symptoms Two Years after SARS-CoV-2 Infection: A Case Report. Neurol. Int. 2023, 15, 908-916. https://doi.org/10.3390/neurolint15030058
Rossi S, Prodi E, Morese R, Paone G, Ruberto T, Sacco L. Persistent 18F-FDG Brain PET Fronto-Temporal Hypometabolism and Cognitive Symptoms Two Years after SARS-CoV-2 Infection: A Case Report. Neurology International. 2023; 15(3):908-916. https://doi.org/10.3390/neurolint15030058
Chicago/Turabian StyleRossi, Stefania, Elena Prodi, Rosalba Morese, Gaetano Paone, Teresa Ruberto, and Leonardo Sacco. 2023. "Persistent 18F-FDG Brain PET Fronto-Temporal Hypometabolism and Cognitive Symptoms Two Years after SARS-CoV-2 Infection: A Case Report" Neurology International 15, no. 3: 908-916. https://doi.org/10.3390/neurolint15030058