


The Clinical Utility of Leukoaraiosis as a Prognostic Indicator in Ischemic Stroke Patients
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results
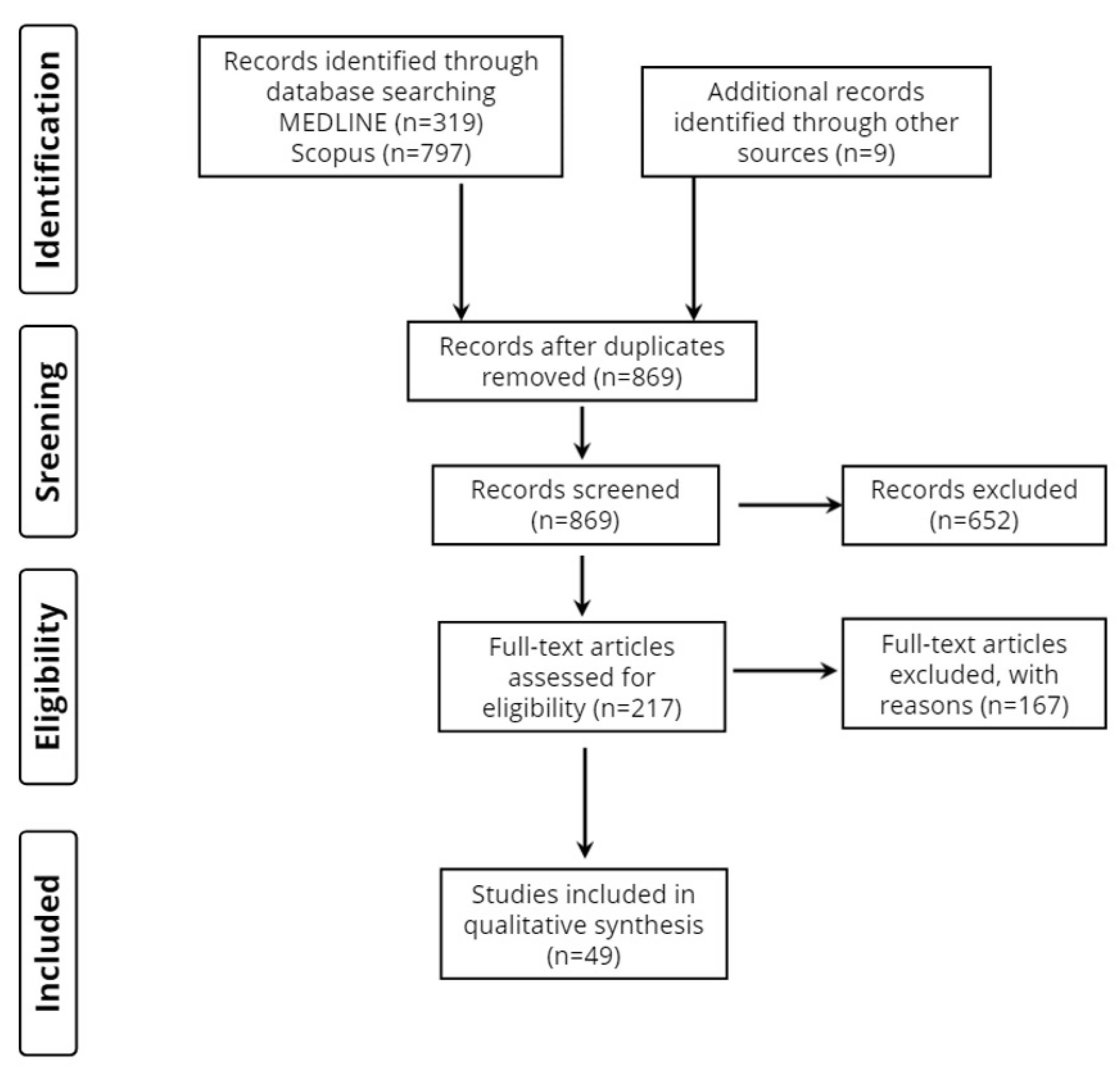
3.1. Database Searches
3.2. Study Characteristics
3.3. Time of Clinical Outcome
3.4. Method of Leukoaraiosis Neuroimaging Assessment
3.5. Study Design

{kind=link}
| 1st Author, (Year) | Type of Stroke, Study Design, Participants (n) | Demographics: Age (Years), Gender (M/F), Education (Years or Level), Marital/Occupational Status, Income, BMI | Cerebrovascular Risk Factors (n) | Medication (n) | Previous Stroke (n) | Follow up Time | Leukoaraiosis/ WMH Assessment | Time of MRI | Scale of Stroke Severity and Prognosis/Clinical Outcome | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Hemorrhagic transformation | ||||||||||
| Wei, (2017) [41] | Cardioembolic stroke due to atrial fibrillation or rheumatic heart disease, Longitudinal, 251 | 68.49 ± 12.43, 99M/152F | Hypertension (n = 105), Diabetes mellitus (n = 27), Hyperlipidemia (n = 3), Alcohol (n = 43), Smoking (n = 44) | Anticoagulants (n = 26), Antiplatelets (n = 32), Statins (n = 12), | 51 | Until discharge | Fazekas score, Van Swieten scale and ARWMC scale | Within 5 days after admission | NIHSS and GCS score on admission | Higher median NIHSS score, lower median GCS score, larger infarct areas, lower levels of serum total cholesterol or low-density lipoprotein on admission, periventricular and frontal moderate to severe LA are associated with higher HT risk. |
| Wang, (2022) [42] | Acute Cerebellar Infarction, Longitudinal, 190 | 61.84 ± 12.16, 141M/49F | Hypertension (n = 149), Diabetes mellitus (n = 77), Atrial Fibrillation (n = 20), Alcohol (n = 49), Smoking (n = 58) | Single Antiplatelet (n = 68), Dual Antiplatelets (n = 95), Anticoagulants (n = 5), Both Antiplatelets and Anticoagulants (n = 22) | 58 | 14 days | Fazekas score | Cranial CT or MRI within 72 h of symptom onset and again whenever HT was suspected or within 14 days after stroke onset | n/a | Atrial fibrillation, infarct diameter and WMH are independent risk factors for HT. |
| Early neurological deterioration or improvement (within 1st week) | ||||||||||
| Feng, (2014) [43] | Small subcortical infarcts (<1.5 cm in diameter) Longitudinal, 435 | 71.1 ± 8.89, 219M/216F | Hypertension (n = 356), Diabetes (n = 118), Dyslipidemia (n = 218), Coronary Artery Disease (n = 69), Smoking (n = 87) | n/a | n/a | 1 week | ARWMC scale | n/a | NIHSS on admission and every day for a week | Age, diabetes mellitus, HbA1c and TC levels, baseline NIHSS score and LA severity are independently associated with END after small subcortical infarction. |
| Jeong, (2015) [44] | Single Small Subcortical Infarction, Longitudinal, 587 | 65 ± 12, 347M/240F BMI 25.0 ± 3.7 in END and 24.0 ± 3.3 in no END group | Hypertension (n = 412), Diabetes mellitus (n = 193), Hyperlipidemia (n = 147), Smoking (n = 248), Relevant artery stenosis (0% to 50% narrowing) (n = 159), branch atheromatous lesions (n = 220) | n/a | 113 | 3 weeks | Fazekas score | Within 24 h of admission | NIHSS on admission and at least once a day during hospitalization, mRS at 3 months | END is associated with large vessel pathologies, but not previous lacunar infarction, CMBs or WMHs. |
| Nannoni, (2015) [45] | Subcortical stroke, Longitudinal, 94 | 67.5 ± 11.7, 68M/26F | Hypertension (n = 76), Diabetes mellitus (n = 22), Hypercholesterolaemia (n = 32), Coronary Artery Disease (n = 7), Smoking (n = 66) | n/a | 22 | 72 h | Van Swieten Scale and Fazekas score | Baseline CT scan on admission. Progressors had CT or MRI performed within 24 h from the onset of worsening. Non-progressors had CT or MRI performed before discharge | NIHSS on admission, every 6–8 h during hospitalization, and at discharge. | Combined vascular risk factors, infarct size and severe LA are independently associated with END |
| Nam, (2016) [46] | Isolated pontine infarction, Longitudinal, 82 | 71, 51M/31F | Hypertension (n = 59), Diabetes mellitus (n = 39), Hyperlipidemia (n = 39), Smoking (n = 37) | Mono antiplatelet drug (n = 48), Dual antiplatelet drug (n = 31), Anticoagulant (n = 0), Both (n = 2), None (n = 1) | 13 | 72 h | Fazekas score | Within 24 h from admission | NIHSS on admission and after 72 h from admission | Severe periventricular and subcortical WMHa are associated with END in patients with isolated pontine infarction. |
| Chen, (2017) [47] | AIS (with NIHSS < 12), Longitudinal, 687 | 59.6 ± 12.7, 496M/191F | Hypertension (n = 476), Diabetes mellitus (n = 162), Coronary Artery Disease (n = 34), Smoking (n = 243) | Mono-antiplatelet treatment (n = 391), Dual-antiplatelet treatment (n = 245), Anticoagulation treatment (n = 54), Statins (n = 48) | 111 | 72 h after admission | Fazekas score | During the initial 24 h after admission | NIHSS | END was not associated with SVD markers |
| Nam, (2017) [48] | AIS, Longitudinal, 325 | 69, 202M/123F | Hypertension (n = 232), Diabetes mellitus (n = 99), Hyperlipidemia (n = 100), Atrial Fibrillation (n = 89), Smoking (n = 104) | Mono-antiplatelet (n = 155) Dual-antiplatelet (n = 138) Anticoagulation (n = 10) Both 14 None 8 | 4 days | Fazekas score | Within 24 h of admission | NIHSS on admission, at 72 h and 7 days, mRS at 3 months | END is associated with severe LA, distal hyperintense vessel sign, advanced age, history of atrial fibrillation and NIHSS on admission. | |
| Μarek, (2018) [49] | AIS, Longitudinal, 77 | 50–93, 44M/33F | n/a | n/a | n/a | n/a | van Swieten scale | Upon admission | NIHSS on admission | Extent of LA is not correlated with NIHSS scale upon admission. |
| Etherton, (2019) [50] | AIS, Longitudinal, 42 | 70.2 ± 9.2, 24M/18F | Atrial fibrillation (n = 16), Myocardial infarction (n = 7), Diabetes mellitus (n = 9), Hyperlipidemia (n = 23), Hypertension (n = 29), Smoking (n = 26) | n/a | 7 | 5 days | WML volumetry | Within 12 h and at day 3–5 post stroke | NIHSS on admission and at day 3–5 post stroke | Periventricular WMHs and preserved normal appearing white-matter microstructural integrity are associated with early neurological improvement. |
| Nam, (2021) [51] | AIS (cryptogenic stroke patients with active cancer), Longitudinal, 179 | 67 ± 10, 108M/71F | Hypertension (n = 77), Diabetes mellitus (n = 55), Dyslipidemia (n = 76), Smoking (n = 61) | n/a | n/a | 3 months | Fazekas score | n/a | NIHSS at baseline and 72 h, mRS at 3 months | No association between END and CMBs or WMHs was observed. In contrast, SBI were associated with END |
| Early Stroke Outcome (<1 month) | ||||||||||
| Kang, (2013) [52] | AIS, Longitudinal, 408 | 64.7 ± 10.0, 238M/170F, 8.5 ± 5.0 | Hypertension (n = 204), Diabetes mellitus (n = 112), Heart disease (n = 33), Hypercholesterolemia (n = 229) | n/a | 34 | 2 weeks, 1 year for 284 patients | Fazekas score | At admission | NIHSS, mRS, BI on admission, at 2 weeks and at 1 year, MMSE at the 2 weeks and 1 year. | Severe periventricular WMHs, but not deep WMHs, are associated with worse outcome both at 2 weeks and at 1 year after stroke. |
| Huang, (2014) [53] | Acute cerebral infarction, Longitudinal, 279 | 73.11 ± 10.32, 191M/88F | n/a | n/a | n/a | 14 days or until discharge | Fazekas score | Before or within 5 days after admission | NIHSS on days 1, 7 and 14 after admission and on the day of discharge, mRS on the day of discharge | WMH grade ≥2 is associated with high probability of self-care incapability upon discharge |
| Toscano, (2015) [54] | Any type (205 with ischemic stroke), Longitudinal, 254 | 73 ± 11.6, 138M/116F, years of education: 0–4 (n = 23), 5–7 (n = 115), 8–12 (n = 72), 13+ (n = 44) | Coronary Artery Disease (n = 217) | n/a | 14 days | Fazekas score | Within 7 days from stroke onset | NIHSS on admission, Water swallow test upon admission and after 14 days | Age, NIHSS ≥ 12 upon admission and LA degree are associated with early post-stroke dysphagia | |
| Zhang, (2017) [55] | AIS (with NIHSS score ≤ 5), Longitudinal, 217, 147 females | 70M/147F, None-to-mild leukoaraiosis group vs. moderate leukoaraiosis group: illiterate (30% vs. 31%), primary school (26.7% vs. 29%), middle school or higher (43.3% vs. 40%) | Hypertension (n = 156), Diabetes mellitus (n = 111), Dyslipidemia (n = 53), Coronary artery disease (n = 13), Smoking (n = 90) | Antiplatelets (n = 210), Oral anticoagulants (n = 4), Statins (n = 217), Antiglycemics (n = 53), Antihypertensives (n = 95) | n/a | 30 days | Fazekas score | Within 48 h after admission | NIHSS and MMSE at baseline and at 30 days. | Severe LA is associated with poor early functional recovery. |
| Fandler, (2017) [56] | Recent small subcortical infarct, Longitudinal, 332 | 67.7 ± 11.9, 214M/118F | Hypertension (n = 282), Diabetes mellitus (n = 93), Hyperlipidemia (n = 197), Smoking (n = 97) | n/a | 73 | 1 day (range, 0–9) | Fazekas score | n/a | NIHSS on admission Gugging Swallowing Screen | NIHSS on admission, pontine infarcts and severe baseline WMHs are independent risk factors of early post-stroke dysphagia |
| Ko, (2017) [57] | Acute Unilateral Corona Radiata Infarction with or without contralateral CBT Involvement, Longitudinal, 81, 29 females | 64.6 ± 11.5, 344M/115F | Hypertension (n = 43), Diabetes mellitus (n = 19) | n/a | n/a | Until discharge | Fazekas score | n/a | NIHSS at baseline, bedside swallowing test, videofluoroscopic swallowing study | Contralateral CBT involvement predicts post-stroke dysphagia. |
| Shang, (2020) [58] | AIS (patients with MCA stroke), Longitudinal, 459 | n/a | Hypertension (n = 245), Diabetes mellitus (n = 109), Hypercholesteremia (n = 121), Smoking (n = 149) | Antiplatelet drugs (n = 176) Anticoagulants (n = 8) Statins (n = 153) | 81 | At discharge | Fazekas score | Two groups: ≤14-day and ≥15-day | NIHSS on admission, mRS at discharge | LA combined with fluid attenuated inversion recovery vascular hyperintensity are associated with unfavorable early clinical outcomes |
| Li, (2020) [59] | Any type (98 with ischemic stroke), Longitudinal, 130 | 57.87 ± 14.22, 83M/47F, no education (n = 5), some education (n = 124), never married (n = 7), currently married (n = 111), formerly married (n = 12), high income (n = 30), low income (n = 100) | Hypertension (n = 120), Diabetes mellitus (n = 45), Dyslipidemia (n = 109), Alcohol (n = 54) | n/a | n/a | 12 months (only the one-month endpoint was used for analysis) | WML volumetry | Within 10 days of symptom onset | mRS, NIHSS, MBI | WMH volume is positively correlated to poor 1-month post-stroke outcome |
| Kim, (2014) [60] | AIS, Longitudinal, 225 | 67.6 ± 13.7, 123M/102F | Hypertension (n = 141), Diabetes mellitus (n = 64), Dyslipidemia (n = 87), Ischemic Heart Disease (n = 19), Atrial Fibrillation (n = 53) | Anticoagulants (n = 4), Antiplatelets(n = 48), Statins (n = 12) | 44 | 6 months | Semiquantitative Scheltens visual rating system [61] | Within 24 h of admission | NIHSS on admission, mRS at discharge and at 6 months | Poor functional outcome upon discharge and at 6 months is positively associated with advanced age, presence of CMB and WMH scores. |
| Short-term stroke outcome (1–3 months) | ||||||||||
| Onteddu, (2015) [62] | AIS (with NIHSS ≤ 5), Longitudinal, 185 | 69, 119M/66F | Hypertension (n = 138), Dyslipidemia (n = 110), Diabetes (n = 63), Atrial fibrillation (n = 36), Coronary artery disease (n = 51), Congestive heart failure (n = 21), Peripheral vascular disease (n = 13), Smoking (n = 56) | Antiplatelets (n = 100), Oral anticoagulants (n = 15), Statins (n = 85), Antiglycemics (n = 46), Antihypertensives (n = 125) | 37 | 90 days | van Swieten scale, Fazekas score | n/a | NIHSS at baseline, discharge, and 90 days, mRS at 90 days | Compared to chronological age, LA is a more sensitive predictor of short term neurological deficit after minor ischemic stroke. |
| Helenius, (2017) [63] | Acute small subcortical infarct, Longitudinal, 80 | 67, 43M/37F | Hypertension (n = 57), Dyslipidemia (n = 49), Diabetes mellitus (n = 27), Atrial fibrillation (n = 5), Coronary Artery Disease (n = 18), Peripheral artery disease (n = 8), Smoking (n = 19), Alcohol (n = 9) | Statins (n = 42), Antihypertensives (n = 52), Antiglycemics (n = 23), Antiplatelets (n = 48), Oral anticoagulant (n = 4) | 20 | 90 days | Fazekas score | Between 24 and 168 h since symptom onset | NIHSS at presentation, mRS at presentation and at 90 days. | Greater WMH burden was independently associated with SSI infarct volume and a worse 90-day functional outcome. |
| Ryu, (2017) [64] | AIS (large artery atherosclerosis, small vessel occlusion, or cardioembolism) Longitudinal, 5035 | 66.3 ± 12.8, 3000M/2032F, BMI per WMH quantiles: Q1 = 23.9, Q2 = 23.9, Q3 = 23.8,Q4 = 23.4, Q5 = 23.3 | Hypertension (n = 3250), Hyperlipidemia (n = 1587), Diabetes mellitus (n = 1363), Smoking (n = 1951), Coronary Artery Disease (n = 425), Atrial Fibrillation (n = 989) | Statins (n = 558), Antiplatelets (n = 1049) | n/a | 3 months | WML volumetry | n/a | NIHSS on admission, mRS pre-stroke, at discharge and at 3 months. | Higher WMH volumes are associated with poor short-term prognosis mainly in large artery atherosclerosis stroke |
| Giralt- Steinhauer, (2018) [65] | TIA or AIS, Longitudinal, 313 | 200M/113F | Hypertension (n = 232), Hyperlipidemia (n = 180), Diabetes mellitus (n = 124), Coronary Artery Disease (n = 37), Atrial Fibrillation (n = 76), Peripheral artery disease (n = 36) | n/a | 27 | 3 months | WML volumetry | Median 7 days | NIHSS on admission, mRS at 3 months | Brainstem WMHs are independent predictors of poor outcome after AIS/TIA. |
| Jeong, (2018) [66] | AIS (with cryptogenic stroke), Longitudinal, 235 | 63 (IQR, 54–69), 159M/76F | Hypertension (n = 178), Hyperlipidemia (n = 13), Diabetes mellitus (n = 72), Smoking (n = 118) Cerebral artery atherosclerosis: intracranial (n = 61), extracranial (n = 23), combined (n = 46) | n/a | n/a | A median of 7.7 years (6.7–9.0) | Fazekas score | Within 3 days after admission | NIHSS at baseline, mRS at 3 months | Severe WMHs are associated with poor short-term functional outcome in young and old CS patients. Younger CS patients with severe WMHs had higher death rates |
| Zerna, (2018) [67] | High risk TIA or AIS (NHISS ≤ 3), Longitudinal, 412 | 69, 248M/164F | Hypertension (n = 225), Congestive heart failure (n = 3), Atrial fibrillation (n = 28), Diabetes mellitus (n = 57), Smoking (n = 63), Intracranial occlusion/stenosis (n = 64) | Aspirin (n = 134), Plavix (n = 24), Aggrenox (n = 4), Warfarin (n = 17) | n/a | 90 days | Fazekas score, WML volumetry | n/a | NIHSS on admission, mRS at 90 days | WML burden was associated with short-term outcomes in TIA and minor stroke patients who had good prestroke function in the presence of intracranial stenosis/occlusion. |
| Schirmer, (2018) [68] | AIS, Longitudinal, 453 | 66.6 ± 14.7, 165M/288F | Hypertension (n = 311) | n/a | n/a | 3–6 months | WML volumetry | Within 48 h of admission | mRS at 90 days | Significant direct association between WMH volume and early stroke outcome was not established. |
| Appleton, (2020) [69] | Any type (3342 with ischemic stroke), Longitudinal, 4011 | 70.3, 2297M/1714F | Hypertension (n = 2607), Diabetes mellitus (n = 699), Atrial Fibrillation (n = 762), Ischemic Heart Disease (n = 669), Peripheral Arterial Disease (n = 117), Smoking (n = 945), Hyperlipidemia (n = 1098), Alcohol (n = 294) | n/a | 1138 | 90 days | LA was assessed separately in anterior and posterior brain regions defined as 0 = no lucency, 1 = lucency restricted to region adjoining ventricles, or 2 = lucency covering entire region from lateral ventricle to cortex | At baseline, usually before randomization | NIHSS at baseline, mRS at day 90 | Severe LA, severe cerebral atrophy and old lacunar infarcts/lacunes score are associated with unfavorable functional outcome at day 90 in lacunar and non-lacunar stroke, with a stronger effect in lacunar stroke. |
| Griessenauer, (2020) [70] | AIS, Large vessel occlusion (LVO) and non-LVO Longitudinal, 1285 | 69 (58–78), 497M/788F BMI ≥ 30 (n = 755) | Hypertension (n = 1264), Diabetes mellitus (n = 621), Dyslipidemia (n = 1148), Smoking (n = 954), Alcohol (n = 552), Peripheral vascular disease (n = 161), Coronary artery disease (n = 477), Atrial fibrillation (n = 355), Carotid stenosis (n = 607), Intracranial atherosclerotic stenosis (n = 483), Anemia (n = 243), Sleep apnea (n = 170), COPD (n = 188) | n/a | 503 | 90 days | WML volumetry | At the time of the stroke admission | NIHSS at presentation, mRS at 90 days | Increasing WMH volume from 0 to 4 mL is correlated with an unfavorable outcome among LVO and non-LVO patients |
| Ryu, (2020) [71] | AIS, Longitudinal, 477 | 66 ± 14, 294M/183F | Hypertension (n = 359), Diabetes mellitus (n = 182), Hyperlipidemia (n = 143), Smoking (n = 221), Coronary Artery Disease (n = 75) | n/a | 99 | 3 months | WML volumetry | Within 7 days of stroke onset | NIHSS on admission, mRS at 3 months | WMHs, lacunes and CMBs are independently associated with mRS scores at 3 months. |
| Coutureau, (2021) [72] | AIS, Longitudinal,
| Dataset 1: 67.5 ± 14.1, 221M/127F, Baccalaureate or higher educational status (n = 106) Dataset 2: 64.8 ± 12.6, 82M/55F, Baccalaureate or higher educational status (n = 51) | n/a | n/a | n/a | 3 months for dataset 1 and 6 months for dataset 2 | Fazekas score | 24 and 72 h after stroke onset | NIHSS at baseline, mRS at 3 months for dataset 1 and mRS at 6 months for dataset 2 | Total SVD score was associated with poor early recovery post-stroke, but did not provide significant improvement of prediction models compared to age and baseline NIHSS |
| Farag, (2021) [73] | AIS, Longitudinal, 460 | 282M/178F | Hypertension (n = 319), Diabetes mellitus (n = 243), Smoking (n = 186), Ischemic Heart Disease (n = 109) | Antiplatelets (n = 243), Statins (n = 54) | 174 | 3 months | Group A (absent leukoaraiosis) and group B (present leukoaraiosis). | A few days post-admission | NIHSS at baseline, mRS at discharge and at 3 months | LA degree is not associated with stroke severity on admission, but with worse clinical outcome at 3 months follow up. |
| Bu, (2021) [61] | AIS, Longitudinal, 259 | 69 ± 12, 139M/120F | n/a | n/a | 42 | 90 days | Fazekas score | Within 9 h of symptom onset | ΝIHSS at baseline, mRS at 90 days | WMHs were not associated with short-term stroke outcome. |
| Sakuta, (2021) [74] | Non-cardiogenic AIS (NIHSS score < 4), Longitudinal, 240 | 66 (57–76), 187M/53F BMI (median): 23.7 | Hypertension (n = 165), Diabetes mellitus (n = 74), Dyslipidemia (n = 126), Ischemic Heart Disease (n = 20), Peripheral arterial disease (n = 6), Chronic kidney disease (n = 33), Malignant neoplasms (n = 17) | Single antiplatelet agent (n = 150), Dual antiplatelet agent (n = 90) | 43 | 90 days | Fazekas score | On admission | NIHSS on admission, mRS at day 90 | deep WMH is not an independent risk factor for poor short-term functional outcome |
| Chen, (2021) [75] | AIS (with NIHSS ≤ 3), Longitudinal, 388 | 66.54 ± 11.15, 111M/277F | Hypertension (n = 324), Coronary artery disease (n = 51), Atrial fibrillation (n = 52), Diabetes mellitus (n = 142), Hyperlipidemia (n = 162), Stroke (n = 61), Smoking 73, Alcohol (n = 56), Carotid atherosclerosis (n = 259) | n/a | n/a | 90 days | Fazekas score | Within 7 days of stroke onset | NIHSS on admission, mRS at 90 days | Among SVD neuroimaging markers, only Fazekas score was associated with poor short-term outcome in minor ischemic stroke. |
| Song, (2021) [76] | TIA, TSI or AIS with symptomatic carotid artery stenosis (CAS), Longitudinal, 158 | 134M/24F, BMI: TIA/TSI = 23.6 3.9, Mild = 23.8 ± 4.0, Moderate to severe = 23.4 ± 2.7 | Hypertension (n = 123), Diabetes mellitus (n = 59), Hyperlipidemia (n = 78), Ischemic Heart Disease (n = 37), Peripheral arterial disease (n = 13), Smoking (n = 53), Congestive Heart Failure (n = 22), Atrial Fibrillation (n = 10) | Antiplatelets (n = 93), Anticoagulants (n = 10), Statins (n = 82) | 45 | 90 days | WML volumetry and Fazekas scale | Within 48 h from the symptom onset | NIHSS at baseline, mRS at day 90 | Larger WMH volume, but not brain-blood flow dynamics or carotid plaque characteristics, is associated with moderate to severe stroke and poor short-term prognosis in symptomatic CAS patients. |
| Long-term stroke outcome (3–12 months) | ||||||||||
| Reid, (2012) [77] | Any type (468 with ischemic stroke), Longitudinal, 538 | 74 (61–80), 286M/252F | Atrial Fibrillation (n = 78) | n/a | 148 | 6 months | Score previously described by Reid et al. [74] | n/a | mRS | LA score was the only independent radiological predictor of both excellent and devastating outcomes. |
| Liu, (2017) [78] | AIS; patients with branch atheromatous disease (BAD), Longitudinal, 176 | 121M/55F | Hypertension (n = 132), Diabetes mellitus (n = 63), Dyslipidemia (n = 101), Ischemic Heart Disease (n = 14), Smoking (n = 78), Alcohol (n = 67) | n/a | n/a | 6 months | Fazekas score | Within 5 days of admission | NIHSS, mRS at 6 months | WMHs were associated with 6-month functional outcome only in the paramedian pontine and not the lenticulostriate atherosclerotic cerebral infarction group |
| Wardlaw, (2017) [79] | AIS (with NIHSS ≤ 7), Longitudinal, 190 | 65.3 ± 11.3, 112M/78F | Hypertension (n = 142), Smoking (n = 73), Hyperlipidemia (n = 116), Diabetes mellitus (n = 21) | n/a | n/a | 1 year | Fazekas score | At presentation and at 1 year after stroke | NIHSS on admission, mRS at 1 year | WMH may regress after minor stroke. Blood pressure reduction might accentuate WMH growth |
| Auriat, (2019) [39] | Any type, Cross-sectional, 30 | 65.68 ± 8.16, 21M/7F, 14.47 ± 3.23 | n/a | n/a | Last diagnosed stroke at least 6 months before participation in the study | WML volumetry | n/a | The upper-extremity motor portion of the Fugl-Meyer assessment (FM) to index impairment of the hemiparetic arm and Wolf Motor Function Test to assess motor function of the upper extremity. | deep WMH volume correlated with motor function and impairment. Periventricular WMH volume is associated with non-memory impairment | |
| Hicks, (2018) [80] | Any type (with upper extremity hemiparesis), Longitudinal, 28 | 63.2 ± 11.5 | n/a | n/a | n/a | post-stroke interval more than 10 months | WML volumetry | Pre-treatment | Hemiparetic arm function was measured using the Motor Activity Log and Wolf Motor Function Test | WMH predicts 10-month stroke-related upper extremity motor impairment. |
| Wright, (2018) [40] | AIS, Cross-sectional, 42 | 56.1 ± 15.0 | n/a | n/a | n/a | >3 months | CHS rating scale | 1 to 4 weeks from stroke onset | WAB object naming score and WAB word fluency score | >3-monhts post-stroke naming outcome is associated with LA severity |
| Lee, (2020) [81] | AIS, Longitudinal, 137 | 68.7 ± 14.0 69M/68F | Diabetes mellitus (26.2%), Hypertension (71.4%), Smoking (9.5%). | n/a | n/a | 6 months | Fazekas score | n/a | NIHSS on admission, Clinical Dysphagia Scale at baseline | WMH burden is associated with 6-month post-stroke dysphagia |
| Chronic stroke outcome (>1 year) | ||||||||||
| Baik, (2017) [82] | AIS (with large artery atherosclerosis), Longitudinal, 538 | 65.7 ± 10.3, 305M/233F | Hypertension (n = 416), Hyperlipidemia (n = 68), Diabetes mellitus (n = 221), Smoking (n = 268) | Antithrombotics (n = 40), Statins (n = 24) | n/a | Median of 7.7 years (interquartile range, 5.6–9.7) | Fazekas score | n/a | NIHSS at baseline, mRS at 3 months | WMH severity is associated with increased all-cause and cardiovascular mortality. |
| Jeon, (2017) [83] | AIS, Longitudinal, 1138 | 73.3 ± 9.9, 156M/982F | Hypertension (n = 192), Diabetes mellitus (n = 90), Coronary heart disease (n = 3), Dyslipidemia (n = 79), Smoking (n = 49) | n/a | 63 | 3 years | Fazekas score | At the time of admission | 3-year mortality | SVD, especially, WMH, and renal dysfunction are associated with increased 3-year mortality post-stroke |
| Hert, (2020) [84] | Atrial fibrillation stroke (treated with anticoagulation), Longitudinal, 320 | 78.2 ± 9.2, 170M/150F | Hypertension (n = 241), Diabetes mellitus (n = 62), Hypercholesterolemia (n = 122), Smoking (n = 81), Alcohol (n = 78) | Vitamin K Antagonists (n = 61), Vitamin K Antagonists/Antiplatelet (n = 15), Direct Oral Anticoagulants (n = 216), Direct Oral Anticoagulants/antiplatelet (n = 18), Antiplatelet (n = 5) | n/a | Median follow-up time of 754 days | ARWMC score | n/a | NIHSS at baseline, mRS at 3, 6, 12, and 24 months | WMHs and CMBs were related to increased risk of ischemic stroke, intracranial hemorrhage, death and disability 2 years post stroke. |
| Rehabilitation outcome | ||||||||||
| Senda, (2016) [85] | AIS, Longitudinal, 520 | 72.8 ± 8.4, 317M/203F | Hypertension (n = 325), Diabetes mellitus (n = 147), Hyperlipidemia (n = 183), Smoking (n = 204), History of Heart Disease (n = 105) | n/a | 131 | From admission to discharge from a convalescent rehabilitation hospital | Fazekas score | n/a | FIM scores on admission and at discharge | Periventricular WMHs are associated with poor FIM motor scores, whereas deep WMHs are related to poor FIM cognitive scores at discharge from rehabilitation. |
| Khan, (2019) [86] | AIS, Longitudinal, 109 | 66.6 ± 12.4, 65M/44F | Hypertension (n = 84), Diabetes mellitus (n = 43), Atrial Fibrillation (n = 22) | n/a | n/a | From admission to discharge from acute inpatient rehabilitation | Fazekas score | n/a | NIHSS at baseline, Functional Independence Measure (FIM) motor and cognitive score | LA severity is an independent predictor of cognitive, but not motor FIM score, after rehabilitation for AIS. |
| Dai, (2022) [87] | Any type (172 with ischemic stroke), Longitudinal, 210 | 67.3, 142M/68F, BMI: no/mild WHMs = 24.5, moderate/severe WMHs = 26.2 | Hypertension (n = 128), Diabetes mellitus (n = 43), Dyslipidemia (n = 98), Smoking (n = 121), Alcohol (n = 49) | n/a | n/a | Until discharge from the neurorehabilitation ward | Fazekas score | NM | NIHSS on admission, mRS, Postural Assessment Scale for Stroke and modified Fugl–Meyer Gait Assessment on day 30 ± 3 post-stroke and at discharge from the rehabilitation ward | LA severity is independently associated with poor gait and balance recovery and increased risk of falls post-AIS. |
3.6. Stroke Patient Groups and Demographic Profile
3.7. Reference Groups
3.8. Time of MRI Execution
3.9. Scales of Stroke Severity and Prognosis/Clinical Outcome
4. Discussion
4.1. Hemorrhagic Transformation
4.2. Early Neurological Deterioration
4.3. Early Stroke Outcome (<1 Month)
4.4. Short-Term Stroke Outcome (<3 Months)
4.5. Longterm Stroke Outcome (<1 Year)
4.6. Chronic Stroke (>1 Year) Outcome
4.7. Rehabilitation Outcome
4.8. Current Guidelines
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef]
- Grefkes, C.; Fink, G.R. Recovery from stroke: Current concepts and future perspectives. Neurol. Res. Pract. 2020, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- United Nations DoEaSA Population Division. World Population Prospects, The 2006 Revision, Highlights; United Nations: New York, NY, USA, 2007. [Google Scholar]
- Kokkotis, C.; Giarmatzis, G.; Giannakou, E.; Moustakidis, S.; Tsatalas, T.; Tsiptsios, D.; Vadikolias, K.; Aggelousis, N. An Explainable Machine Learning Pipeline for Stroke Prediction on Imbalanced Data. Diagnostics 2022, 12, 2392. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Winstein, C. Can Neurological Biomarkers of Brain Impairment Be Used to Predict Poststroke Motor Recovery? A Systematic Review. Neurorehabil. Neural Repair. 2017, 31, 3–24. [Google Scholar] [CrossRef] [Green Version]
- Stinear, C.M. Prediction of motor recovery after stroke: Advances in biomarkers. Lancet Neurol. 2017, 16, 826–836. [Google Scholar] [CrossRef]
- Quinn, T.J.; Singh, S.; Lees, K.R.; Bath, P.M.; Myint, P.K.; Collaborators, V. Validating and comparing stroke prognosis scales. Neurology 2017, 89, 997–1002. [Google Scholar] [CrossRef] [Green Version]
- Saposnik, G.; Guzik, A.K.; Reeves, M.; Ovbiagele, B.; Johnston, S.C. Stroke Prognostication using Age and NIH Stroke Scale: SPAN-100. Neurology 2013, 80, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Karatzetzou, S.; Tsiptsios, D.; Terzoudi, A.; Aggeloussis, N.; Vadikolias, K. Transcranial magnetic stimulation implementation on stroke prognosis. Neurol. Sci. 2022, 43, 873–888. [Google Scholar] [CrossRef]
- Gkantzios, A.; Tsiptsios, D.; Karatzetzou, S.; Kitmeridou, S.; Karapepera, V.; Giannakou, E.; Vlotinou, P.; Aggelousis, N.; Vadikolias, K. Stroke and Emerging Blood Biomarkers: A Clinical Prospective. Neurol. Int. 2022, 14, 784–803. [Google Scholar] [CrossRef]
- Christidi, F.; Tsiptsios, D.; Fotiadou, A.; Kitmeridou, S.; Karatzetzou, S.; Tsamakis, K.; Sousanidou, A.; Psatha, E.A.; Karavasilis, E.; Seimenis, I.; et al. Diffusion Tensor Imaging as a Prognostic Tool for Recovery in Acute and Hyperacute Stroke. Neurol. Int. 2022, 14, 841–874. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, M. Leukoaraiosis. Pract. Neurol. 2008, 8, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Hachinski, V.C.; Potter, P.; Merskey, H. Leuko-araiosis. Arch. Neurol. 1987, 44, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. AJR Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef] [Green Version]
- De Leeuw, F.E.; de Groot, J.C.; Achten, E.; Oudkerk, M.; Ramos, L.M.; Heijboer, R.; Hofman, A.; Jolles, J.; van Gijn, J.; Breteler, M.M. Prevalence of cerebral white matter lesions in elderly people: A population based magnetic resonance imaging study. The Rotterdam Scan Study. J. Neurol. Neurosurg. Psychiatry 2001, 70, 9–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, W.; Sachdev, P.S.; Li, J.J.; Chen, X.; Anstey, K.J. White matter hyperintensities in the forties: Their prevalence and topography in an epidemiological sample aged 44-48. Hum. Brain Mapp. 2009, 30, 1155–1167. [Google Scholar] [CrossRef]
- Debette, S.; Markus, H.S. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: Systematic review and meta-analysis. BMJ 2010, 341, c3666. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, R.O.; Beck, C.J.; Burnett, D.L.; Weaver, L.K.; Victoroff, J.; Bigler, E.D. Prevalence of white matter hyperintensities in a young healthy population. J. Neuroimaging 2006, 16, 243–251. [Google Scholar] [CrossRef]
- Marek, M.; Horyniecki, M.; Fraczek, M.; Kluczewska, E. Leukoaraiosis—New concepts and modern imaging. Pol. J. Radiol. 2018, 83, e76–e81. [Google Scholar] [CrossRef]
- Del Bene, A.; Ciolli, L.; Borgheresi, L.; Poggesi, A.; Inzitari, D.; Pantoni, L. Is type 2 diabetes related to leukoaraiosis? an updated review. Acta Neurol. Scand. 2015, 132, 147–155. [Google Scholar] [CrossRef]
- Lin, Q.; Huang, W.Q.; Ma, Q.L.; Lu, C.X.; Tong, S.J.; Ye, J.H.; Lin, H.N.; Gu, L.; Yi, K.H.; Cai, L.L.; et al. Incidence and risk factors of leukoaraiosis from 4683 hospitalized patients: A cross-sectional study. Medicine 2017, 96, e7682. [Google Scholar] [CrossRef] [PubMed]
- Helenius, J.; Tatlisumak, T. Treatment of leukoaraiosis: A futuristic view. Curr. Drug Targets 2007, 8, 839–845. [Google Scholar] [CrossRef]
- Van Dijk, E.J.; Prins, N.D.; Vrooman, H.A.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M. Progression of cerebral small vessel disease in relation to risk factors and cognitive consequences: Rotterdam Scan study. Stroke 2008, 39, 2712–2719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Wang, D.; Lan, L.; Fan, Y. Multiple Factors Involved in the Pathogenesis of White Matter Lesions. Biomed. Res. Int. 2017, 2017, 9372050. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Hui, L.; Li, Y.; Chen, X.; Liu, R.; Ma, J. Pathogenesis and research progress in leukoaraiosis. Front. Hum. Neurosci. 2022, 16, 902731. [Google Scholar] [CrossRef]
- Wang, S.; Yuan, J.; Guo, X.; Peng, P.; Gu, H.; Niu, S.; Fregni, F.; Chen, A.C.; Hu, W. Neurochemical correlates of cognitive dysfunction in patients with leukoaraiosis: A proton magnetic resonance spectroscopy study. Neurol. Res. 2012, 34, 989–997. [Google Scholar] [CrossRef]
- Baezner, H.; Blahak, C.; Poggesi, A.; Pantoni, L.; Inzitari, D.; Chabriat, H.; Erkinjuntti, T.; Fazekas, F.; Ferro, J.M.; Langhorne, P.; et al. Association of gait and balance disorders with age-related white matter changes: The LADIS study. Neurology 2008, 70, 935–942. [Google Scholar] [CrossRef]
- Poggesi, A.; Pracucci, G.; Chabriat, H.; Erkinjuntti, T.; Fazekas, F.; Verdelho, A.; Hennerici, M.; Langhorne, P.; O’Brien, J.; Scheltens, P.; et al. Urinary complaints in nondisabled elderly people with age-related white matter changes: The Leukoaraiosis And DISability (LADIS) Study. J. Am. Geriatr. Soc. 2008, 56, 1638–1643. [Google Scholar] [CrossRef]
- Kloppenborg, R.P.; Nederkoorn, P.J.; Geerlings, M.I.; van den Berg, E. Presence and progression of white matter hyperintensities and cognition: A meta-analysis. Neurology 2014, 82, 2127–2138. [Google Scholar] [CrossRef] [Green Version]
- Verdelho, A.; Madureira, S.; Moleiro, C.; Ferro, J.M.; Santos, C.O.; Erkinjuntti, T.; Pantoni, L.; Fazekas, F.; Visser, M.; Waldemar, G.; et al. White matter changes and diabetes predict cognitive decline in the elderly: The LADIS study. Neurology 2010, 75, 160–167. [Google Scholar] [CrossRef]
- Alber, J.; Alladi, S.; Bae, H.J.; Barton, D.A.; Beckett, L.A.; Bell, J.M.; Berman, S.E.; Biessels, G.J.; Black, S.E.; Bos, I.; et al. White matter hyperintensities in vascular contributions to cognitive impairment and dementia (VCID): Knowledge gaps and opportunities. Alzheimers Dement. 2019, 5, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Prins, N.D.; Scheltens, P. White matter hyperintensities, cognitive impairment and dementia: An update. Nat. Rev. Neurol. 2015, 11, 157–165. [Google Scholar] [CrossRef]
- Firbank, M.J.; Teodorczuk, A.; van der Flier, W.M.; Gouw, A.A.; Wallin, A.; Erkinjuntti, T.; Inzitari, D.; Wahlund, L.O.; Pantoni, L.; Poggesi, A.; et al. Relationship between progression of brain white matter changes and late-life depression: 3-year results from the LADIS study. Br. J. Psychiatry 2012, 201, 40–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group, L.S. 2001–2011: A decade of the LADIS (Leukoaraiosis And DISability) Study: What have we learned about white matter changes and small-vessel disease? Cerebrovasc. Dis. 2011, 32, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Scheltens, P.; Erkinjunti, T.; Leys, D.; Wahlund, L.O.; Inzitari, D.; del Ser, T.; Pasquier, F.; Barkhof, F.; Mantyla, R.; Bowler, J.; et al. White matter changes on CT and MRI: An overview of visual rating scales. European Task Force on Age-Related White Matter Changes. Eur. Neurol. 1998, 39, 80–89. [Google Scholar] [CrossRef]
- Saba, L.; Raz, E.; Bassareo, P.P.; di Martino, M.; de Cecco, C.N.; Mercuro, G.; Grassi, R.; Suri, J.S.; Piga, M. Is there an association between cerebral microbleeds and leukoaraiosis? J. Stroke Cerebrovasc. Dis. 2015, 24, 284–289. [Google Scholar] [CrossRef]
- Puy, L.; Pasi, M.; Rodrigues, M.; van Veluw, S.J.; Tsivgoulis, G.; Shoamanesh, A.; Cordonnier, C. Cerebral microbleeds: From depiction to interpretation. J. Neurol. Neurosurg. Psychiatry 2021, 92, 598–607. [Google Scholar] [CrossRef]
- Auriat, A.M.; Ferris, J.K.; Peters, S.; Ramirez, J.; Black, S.E.; Jacova, C.; Boyd, L.A. The Impact of Covert Lacunar Infarcts and White Matter Hyperintensities on Cognitive and Motor Outcomes After Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 381–388. [Google Scholar] [CrossRef]
- Wright, A.; Tippett, D.; Saxena, S.; Sebastian, R.; Breining, B.; Faria, A.; Hillis, A.E. Leukoaraiosis is independently associated with naming outcome in poststroke aphasia. Neurology 2018, 91, e526–e532. [Google Scholar] [CrossRef]
- Wei, C.C.; Zhang, S.T.; Wang, Y.H.; Liu, J.F.; Li, J.; Yuan, R.Z.; Tan, G.; Zhang, S.H.; Liu, M. Association between leukoaraiosis and hemorrhagic transformation after cardioembolic stroke due to atrial fibrillation and/or rheumatic heart disease. J. Neurol. Sci. 2017, 378, 94–99. [Google Scholar] [CrossRef]
- Wang, L.; Liu, L.; Zhao, Y.; Gao, D.; Yang, Y.; Chu, M.; Teng, J. Analysis of Factors Associated with Hemorrhagic Transformation in Acute Cerebellar Infarction. J. Stroke Cerebrovasc. Dis. 2022, 31, 106538. [Google Scholar] [CrossRef]
- Feng, C.; Tan, Y.; Wu, Y.F.; Xu, Y.; Hua, T.; Huang, J.; Liu, X.Y. Leukoaraiosis correlates with the neurologic deterioration after small subcortical infarction. J. Stroke Cerebrovasc. Dis. 2014, 23, 1513–1518. [Google Scholar] [CrossRef]
- Jeong, H.G.; Kim, B.J.; Yang, M.H.; Han, M.K.; Bae, H.J. Neuroimaging markers for early neurologic deterioration in single small subcortical infarction. Stroke 2015, 46, 687–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nannoni, S.; Del Bene, A.; Palumbo, V.; Petrone, L.; Sottile, F.; Pracucci, G.; Inzitari, D. Predictors of progression in patients presenting with minor subcortical stroke. Acta Neurol. Scand. 2015, 132, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.W.; Lim, J.S.; Kang, D.W.; Lee, Y.S.; Han, M.K.; Kwon, H.M. Severe White Matter Hyperintensity Is Associated with Early Neurological Deterioration in Patients with Isolated Pontine Infarction. Eur. Neurol. 2016, 76, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Li, W.; Sun, W.; Xiao, L.; Dai, Q.; Cao, Y.; Han, Y.; Zhu, W.; Xu, G.; Liu, X. Correlation study between small vessel disease and early neurological deterioration in patients with mild/moderate acute ischemic stroke. Int. J. Neurosci. 2017, 127, 579–585. [Google Scholar] [CrossRef]
- Nam, K.W.; Kwon, H.M.; Park, S.W.; Lim, J.S.; Han, M.K.; Lee, Y.S. Distal hyperintense vessel sign is associated with neurological deterioration in acute ischaemic stroke. Eur. J. Neurol. 2017, 24, 617–623. [Google Scholar] [CrossRef]
- Marek, M.; Horyniecki, M.; Karpe, J.; Adamczyk-Sowa, M.; Walecki, J.; Kluczewska, E. Relationship between stroke severity, extensity of leukoaraiosis, and brain atrophy in patients with ischaemic stroke. Pol. J. Radiol. 2019, 84, e80–e85. [Google Scholar] [CrossRef]
- Etherton, M.R.; Wu, O.; Giese, A.K.; Lauer, A.; Boulouis, G.; Mills, B.; Cloonan, L.; Donahue, K.L.; Copen, W.; Schaefer, P.; et al. White Matter Integrity and Early Outcomes After Acute Ischemic Stroke. Transl. Stroke Res. 2019, 10, 630–638. [Google Scholar] [CrossRef]
- Nam, K.W.; Kwon, H.M.; Lee, Y.S.; Kim, J.M.; Ko, S.B. Effects of cerebral small vessel disease on the outcomes in cryptogenic stroke with active cancer. Sci. Rep. 2021, 11, 17510. [Google Scholar] [CrossRef]
- Kang, H.J.; Stewart, R.; Park, M.S.; Bae, K.Y.; Kim, S.W.; Kim, J.M.; Shin, I.S.; Cho, K.H.; Yoon, J.S. White matter hyperintensities and functional outcomes at 2 weeks and 1 year after stroke. Cerebrovasc. Dis. 2013, 35, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Xia, Z.X.; Wei, W.; Gao, G.R.; Gong, J.J.; Li, Y.; Zhang, W.W. The impact of leucoaraiosis on neurological function recovery in elderly patients with acute cerebral infarction: Clinical study involving 279 Chinese patients. J. Int. Med. Res. 2014, 42, 857–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toscano, M.; Cecconi, E.; Capiluppi, E.; Vigano, A.; Bertora, P.; Campiglio, L.; Mariani, C.; Petolicchio, B.; Sasso D’Elia, T.; Verzina, A.; et al. Neuroanatomical, Clinical and Cognitive Correlates of Post-Stroke Dysphagia. Eur. Neurol. 2015, 74, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Ren, W.; Shao, B.; Xu, H.; Cheng, J.; Wang, Q.; Gu, Y.; Zhu, B.; He, J. Leukoaraiosis is Associated with Worse Short-Term Functional and Cognitive Recovery after Minor Stroke. Neurol. Med. Chir. 2017, 57, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Fandler, S.; Gattringer, T.; Eppinger, S.; Doppelhofer, K.; Pinter, D.; Niederkorn, K.; Enzinger, C.; Wardlaw, J.M.; Fazekas, F. Frequency and Predictors of Dysphagia in Patients With Recent Small Subcortical Infarcts. Stroke 2017, 48, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Ko, E.J.; Choi, K.H.; Kwon, S.U. The Relationship Between Leukoaraiosis Involving Contralateral Corticobulbar Tract and Dysphagia in Patients with Acute Unilateral Corona Radiata Infarction with Corticobulbar Tract Involvement. Dysphagia 2019, 34, 654–664. [Google Scholar] [CrossRef]
- Shang, W.J.; Shu, L.M.; Zhou, X.; Liao, H.Q.; Chen, X.H.; Hong, H.; Chen, H.B. Association of FLAIR vascular hyperintensity and acute MCA stroke outcome changes with the severity of leukoaraiosis. Neurol. Sci. 2020, 41, 3209–3218. [Google Scholar] [CrossRef]
- Li, J.; Ogbole, G.; Aribisala, B.; Affini, M.; Yaria, J.; Kehinde, I.; Rahman, M.; Adekunle, F.; Banjo, R.; Faniyan, M.; et al. Association between white matter hyperintensities and stroke in a West African patient population: Evidence from the Stroke Investigative Research and Educational Network study. Neuroimage 2020, 215, 116789. [Google Scholar] [CrossRef]
- Kim, T.W.; Lee, S.J.; Koo, J.; Choi, H.S.; Park, J.W.; Lee, K.S.; Kim, J.S. Cerebral microbleeds and functional outcomes after ischemic stroke. Can. J. Neurol. Sci. 2014, 41, 577–582. [Google Scholar] [CrossRef] [Green Version]
- Bu, N.; Khlif, M.S.; Lemmens, R.; Wouters, A.; Fiebach, J.B.; Chamorro, A.; Ringelstein, E.B.; Norrving, B.; Laage, R.; Grond, M.; et al. Imaging Markers of Brain Frailty and Outcome in Patients With Acute Ischemic Stroke. Stroke 2021, 52, 1004–1011. [Google Scholar] [CrossRef]
- Onteddu, S.R.; Goddeau, R.P., Jr.; Minaeian, A.; Henninger, N. Clinical impact of leukoaraiosis burden and chronological age on neurological deficit recovery and 90-day outcome after minor ischemic stroke. J. Neurol. Sci. 2015, 359, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Helenius, J.; Mayasi, Y.; Henninger, N. White matter hyperintensity lesion burden is associated with the infarct volume and 90-day outcome in small subcortical infarcts. Acta Neurol. Scand. 2017, 135, 585–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, W.S.; Woo, S.H.; Schellingerhout, D.; Jang, M.U.; Park, K.J.; Hong, K.S.; Jeong, S.W.; Na, J.Y.; Cho, K.H.; Kim, J.T.; et al. Stroke outcomes are worse with larger leukoaraiosis volumes. Brain 2017, 140, 158–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giralt-Steinhauer, E.; Medrano, S.; Soriano-Tarraga, C.; Mola-Caminal, M.; Rasal, R.; Cuadrado-Godia, E.; Rodriguez-Campello, A.; Ois, A.; Capellades, J.; Jimenez-Conde, J.; et al. Brainstem leukoaraiosis independently predicts poor outcome after ischemic stroke. Eur. J. Neurol. 2018, 25, 1086–1092. [Google Scholar] [CrossRef]
- Jeong, S.H.; Ahn, S.S.; Baik, M.; Kim, K.H.; Yoo, J.; Kim, K.; Lee, H.S.; Ha, J.; Kim, Y.D.; Heo, J.H.; et al. Impact of white matter hyperintensities on the prognosis of cryptogenic stroke patients. PLoS ONE 2018, 13, e0196014. [Google Scholar] [CrossRef] [Green Version]
- Zerna, C.; Yu, A.Y.X.; Modi, J.; Patel, S.K.; Coulter, J.I.; Smith, E.E.; Coutts, S.B. Association of White Matter Hyperintensities With Short-Term Outcomes in Patients With Minor Cerebrovascular Events. Stroke 2018, 49, 919–923. [Google Scholar] [CrossRef]
- Schirmer, M.D.; Etherton Md Ph, D.M.; Dalca Ph, D.A.; Giese Md, A.K.; Cloonan, M.L.; Wu Ph, D.O.; Golland Ph, D.P.; Rost Md Mph Faan, N.S. Effective Reserve: A Latent Variable to Improve Outcome Prediction in Stroke. J. Stroke Cerebrovasc. Dis. 2019, 28, 63–69. [Google Scholar] [CrossRef]
- Appleton, J.P.; Woodhouse, L.J.; Adami, A.; Becker, J.L.; Berge, E.; Cala, L.A.; Casado, A.M.; Caso, V.; Christensen, H.K.; Dineen, R.A.; et al. Imaging markers of small vessel disease and brain frailty, and outcomes in acute stroke. Neurology 2020, 94, e439–e452. [Google Scholar] [CrossRef] [Green Version]
- Griessenauer, C.J.; McPherson, D.; Berger, A.; Cuiper, P.; Sofoluke, N.; Adams, M.D.; Kunaprayoon, S.; Zand, R.; Li, J.; Abedi, V.; et al. Effects of White Matter Hyperintensities on 90-Day Functional Outcome after Large Vessel and Non-Large Vessel Stroke. Cerebrovasc. Dis. 2020, 49, 419–426. [Google Scholar] [CrossRef]
- Ryu, W.S.; Jeong, S.W.; Kim, D.E. Total small vessel disease burden and functional outcome in patients with ischemic stroke. PLoS ONE 2020, 15, e0242319. [Google Scholar] [CrossRef]
- Coutureau, J.; Asselineau, J.; Perez, P.; Kuchcinski, G.; Sagnier, S.; Renou, P.; Munsch, F.; Lopes, R.; Henon, H.; Bordet, R.; et al. Cerebral Small Vessel Disease MRI Features Do Not Improve the Prediction of Stroke Outcome. Neurology 2021, 96, e527–e537. [Google Scholar] [CrossRef] [PubMed]
- Farag, S.; Kenawy, F.F.; Shokri, H.M.; Zakaria, M.; Aref, H.; Fahmi, N.; Khayat, N.; Shalash, A.; Nahas, N.E. The Clinical Characteristics of Patients with Pre-Existing Leukoaraiosis Compared to Those Without Leukoaraiosis in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105956. [Google Scholar] [CrossRef] [PubMed]
- Sakuta, K.; Yaguchi, H.; Nakada, R.; Sato, T.; Kitagawa, T.; Takatsu, H.; Miyagawa, S.; Komatsu, T.; Sakai, K.; Mitsumura, H.; et al. Cerebral Microbleeds Load and Long-Term Outcomes in Minor Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105973. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, L.; Jiang, J.; Gao, Y.; Zhang, R.; Zhao, X.; Shen, T.; Dai, Q.; Li, J. Association of neuroimaging markers of cerebral small vessel disease with short-term outcomes in patients with minor cerebrovascular events. BMC Neurol. 2021, 21, 21. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Kim, K.H.; Jeon, P.; Kim, Y.W.; Kim, D.I.; Park, Y.J.; Park, M.S.; Chung, J.W.; Seo, W.K.; Bang, O.Y.; et al. White matter hyperintensity determines ischemic stroke severity in symptomatic carotid artery stenosis. Neurol. Sci. 2021, 42, 3367–3374. [Google Scholar] [CrossRef] [PubMed]
- Reid, J.M.; Dai, D.; Christian, C.; Reidy, Y.; Counsell, C.; Gubitz, G.J.; Phillips, S.J. Developing predictive models of excellent and devastating outcome after stroke. Age Ageing 2012, 41, 560–564. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Fan, Y.T.; Liu, Y.M.; Wang, T.; Feng, H.L.; Liu, G.Z.; Mei, B. A retrospective study of branch atheromatous disease: Analyses of risk factors and prognosis. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2017, 37, 93–99. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Chappell, F.M.; Valdes Hernandez, M.D.C.; Makin, S.D.J.; Staals, J.; Shuler, K.; Thrippleton, M.J.; Armitage, P.A.; Munoz-Maniega, S.; Heye, A.K.; et al. White matter hyperintensity reduction and outcomes after minor stroke. Neurology 2017, 89, 1003–1010. [Google Scholar] [CrossRef] [Green Version]
- Hicks, J.M.; Taub, E.; Womble, B.; Barghi, A.; Rickards, T.; Mark, V.W.; Uswatte, G. Relation of white matter hyperintensities and motor deficits in chronic stroke. Restor. Neurol. Neurosci. 2018, 36, 349–357. [Google Scholar] [CrossRef]
- Lee, W.H.; Lim, M.H.; Seo, H.G.; Seong, M.Y.; Oh, B.M.; Kim, S. Development of a Novel Prognostic Model to Predict 6-Month Swallowing Recovery After Ischemic Stroke. Stroke 2020, 51, 440–448. [Google Scholar] [CrossRef]
- Baik, M.; Kim, K.; Yoo, J.; Kim, H.C.; Jeong, S.H.; Kim, K.H.; Park, H.J.; Kim, Y.D.; Heo, J.H.; Nam, H.S. Differential impact of white matter hyperintensities on long-term outcomes.s in ischemic stroke patients with large artery atherosclerosis. PLoS ONE 2017, 12, e0189611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, J.W.; Jeong, H.S.; Choi, D.E.; Ham, Y.R.; Na, K.R.; Lee, K.W.; Shin, J.W.; Kim, J. Prognostic Relationships between Microbleed, Lacunar Infarction, White Matter Lesion, and Renal Dysfunction in Acute Ischemic Stroke Survivors. J. Stroke Cerebrovasc. Dis. 2017, 26, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Hert, L.; Polymeris, A.A.; Schaedelin, S.; Lieb, J.; Seiffge, D.J.; Traenka, C.; Fladt, J.; Thilemann, S.; Gensicke, H.; De Marchis, G.M.; et al. Small vessel disease is associated with an unfavourable outcome in stroke patients on oral anticoagulation. Eur. Stroke J. 2020, 5, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Senda, J.; Ito, K.; Kotake, T.; Kanamori, M.; Kishimoto, H.; Kadono, I.; Suzuki, Y.; Katsuno, M.; Nishida, Y.; Ishiguro, N.; et al. Association of Leukoaraiosis With Convalescent Rehabilitation Outcome in Patients With Ischemic Stroke. Stroke 2016, 47, 160–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, M.; Heiser, H.; Bernicchi, N.; Packard, L.; Parker, J.L.; Edwardson, M.A.; Silver, B.; Elisevich, K.V.; Henninger, N. Leukoaraiosis Predicts Short-term Cognitive But not Motor Recovery in Ischemic Stroke Patients During Rehabilitation. J. Stroke Cerebrovasc. Dis. 2019, 28, 1597–1603. [Google Scholar] [CrossRef]
- Dai, S.; Piscicelli, C.; Lemaire, C.; Christiaens, A.; Schotten, M.T.; Hommel, M.; Krainik, A.; Detante, O.; Perennou, D. Recovery of balance and gait after stroke is deteriorated by confluent white matter hyperintensities: Cohort study. Ann. Phys. Rehabil. Med. 2022, 65, 101488. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Debette, S.; Jokinen, H.; De Leeuw, F.E.; Pantoni, L.; Chabriat, H.; Staals, J.; Doubal, F.; Rudilosso, S.; Eppinger, S.; et al. ESO Guideline on covert cerebral small vessel disease. Eur. Stroke J. 2021, 6, CXI–CLXII. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christidi, F.; Tsiptsios, D.; Sousanidou, A.; Karamanidis, S.; Kitmeridou, S.; Karatzetzou, S.; Aitsidou, S.; Tsamakis, K.; Psatha, E.A.; Karavasilis, E.; et al. The Clinical Utility of Leukoaraiosis as a Prognostic Indicator in Ischemic Stroke Patients. Neurol. Int. 2022, 14, 952-980. https://doi.org/10.3390/neurolint14040076
Christidi F, Tsiptsios D, Sousanidou A, Karamanidis S, Kitmeridou S, Karatzetzou S, Aitsidou S, Tsamakis K, Psatha EA, Karavasilis E, et al. The Clinical Utility of Leukoaraiosis as a Prognostic Indicator in Ischemic Stroke Patients. Neurology International. 2022; 14(4):952-980. https://doi.org/10.3390/neurolint14040076
Chicago/Turabian StyleChristidi, Foteini, Dimitrios Tsiptsios, Anastasia Sousanidou, Stefanos Karamanidis, Sofia Kitmeridou, Stella Karatzetzou, Souzana Aitsidou, Konstantinos Tsamakis, Evlampia A. Psatha, Efstratios Karavasilis, and et al. 2022. "The Clinical Utility of Leukoaraiosis as a Prognostic Indicator in Ischemic Stroke Patients" Neurology International 14, no. 4: 952-980. https://doi.org/10.3390/neurolint14040076