
Elucidating the Role of Baseline Leukoaraiosis on Forecasting Clinical Outcome of Acute Ischemic Stroke Patients Undergoing Reperfusion Therapy
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results
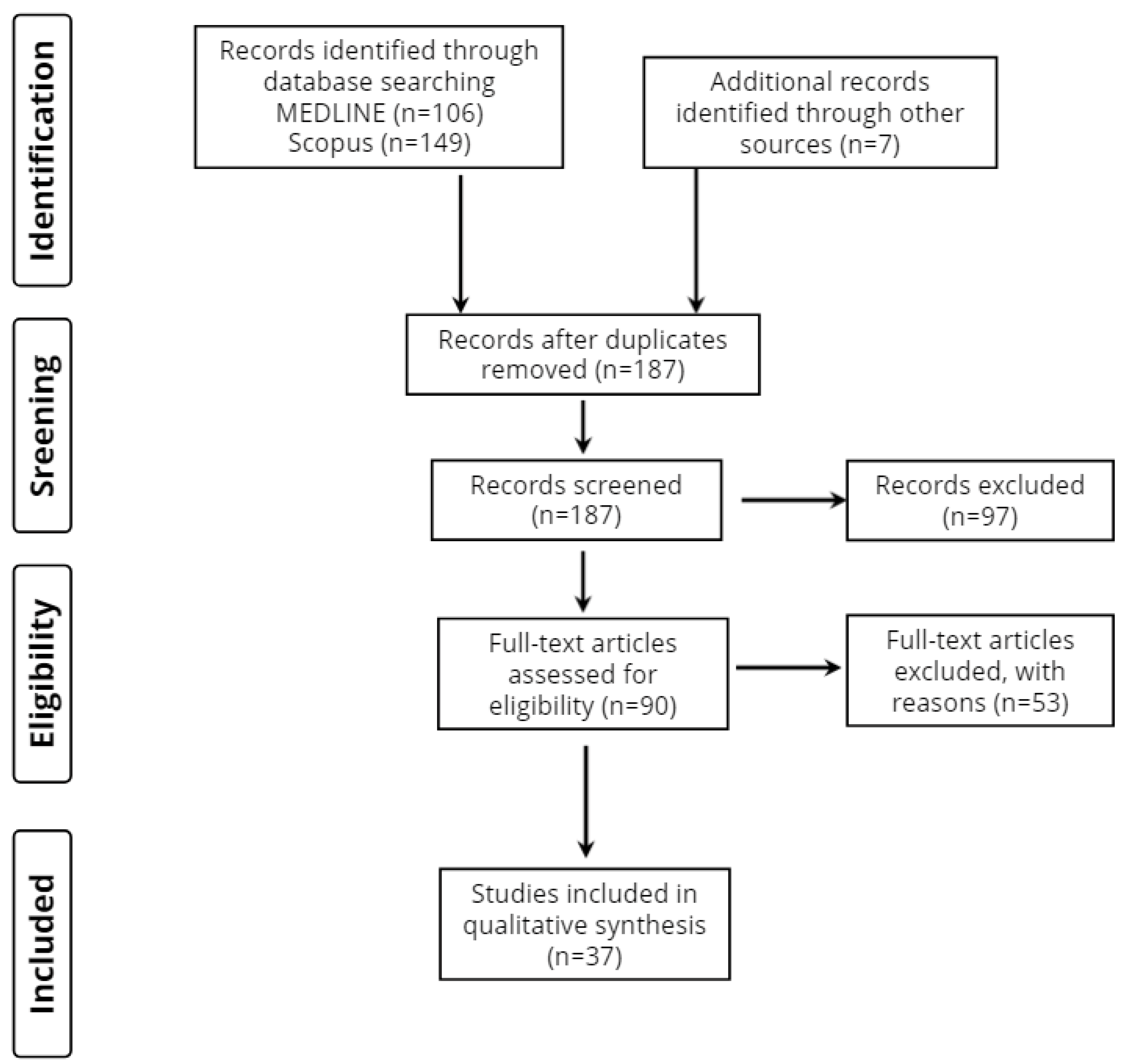
3.1. Database Searches
3.2. Study Characteristics
3.3. Method of LA Neuroimaging Assessment
3.4. Study Design
3.5. Stroke Patient Groups and Demographic Profile
3.6. Reference Groups
3.7. Scales of Stroke Severity and Prognosis/Clinical Outcome
4. Discussion
4.1. Endovascular Stroke Therapy
4.2. Intravenous Thrombolysis
4.3. Intravenous Thrombolysis and/or Endovascular Stroke Therapy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Donkor, S.E. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology and Quality of Life. Stroke Res. Treat. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Grefkes, C.; Fink, G.R. Recovery from stroke: Current concepts and future perspectives. Neurol. Res. Pract. 2020, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsivgoulis, G.; Kargiotis, O.; Alexandrov, A.V. Intravenous thrombolysis for acute ischemic stroke: A bridge between two centuries. Expert Rev. Neurother. 2017, 17, 819–837. [Google Scholar] [CrossRef]
- IST-3 Collaborative Group; Sandercock, P.; Wardlaw, J.M.; Lindley, R.I.; Dennis, M.; Cohen, G.; Murray, G.; Innes, K.; Venables, G.; Czlonkowska, A.; et al. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): A randomised controlled trial. Lancet 2012, 379, 2352–2363. [Google Scholar] [CrossRef] [Green Version]
- Wahlgren, N.; Ahmed, N.; Davalos, A.; Ford, G.A.; Grond, M.; Hacke, W.; Hennerici, M.G.; Kaste, M.; Kuelkens, S.; Larrue, V.; et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): An observational study. Lancet 2007, 369, 275–282. [Google Scholar] [CrossRef]
- Hacke, W.; Donnan, G.; Fieschi, C.; Kaste, M.; von Kummer, R.; Broderick, J.P.; Brott, T.; Frankel, M.; Grotta, J.C.; Haley, E.C.; et al. Association of outcome with early stroke treatment: Pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004, 9411, 768–774. [Google Scholar] [CrossRef]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; Román, L.S.; Serena, J.; Abilleira, S.; Ribo, M.; et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [Green Version]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Saver, J.L.; Goyal, M.; van der Lugt, A.; Menon, B.K.; Majoie, C.B.; Dippel, D.W.; Campbell, B.C.; Nogueira, R.G.; Demchuk, A.M.; Tomasello, A.; et al. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: A meta-analysis. JAMA 2016, 316, 1279–1288. [Google Scholar] [CrossRef]
- Nie, X.; Pu, Y.; Zhang, Z.; Liu, X.; Duan, W.; Liu, L. Futile recanalization after endovascular therapy in acute ischemic stroke. BioMed Res. Int. 2018, 2018, 5879548. [Google Scholar] [CrossRef] [Green Version]
- Machumpurath, B.; Davis, S.M.; Yan, B. Rapid neurological recovery after intravenous tissue plasminogen activator in stroke: Prognostic factors and outcome. Cerebrovasc. Dis. 2011, 31, 278–283. [Google Scholar] [CrossRef]
- Stinear, C.M.; Byblow, W.D.; Ackerley, S.J.; Barber, P.A.; Smith, M.C. Predicting Recovery Potential for Individual Stroke Patients Increases Rehabilitation Efficiency. Stroke 2017, 48, 1011–1019. [Google Scholar] [CrossRef]
- Gkantzios, A.; Tsiptsios, D.; Karatzetzou, S.; Kitmeridou, S.; Karapepera, V.; Giannakou, E.; Vlotinou, P.; Aggelousis, N.; Vadikolias, K. Stroke and Emerging Blood Biomarkers: A Clinical Prospective. Neurol. Int. 2022, 14, 65. [Google Scholar] [CrossRef]
- Karatzetzou, S.; Tsiptsios, D.; Terzoudi, A.; Aggeloussis, N.; Vadikolias, K. Transcranial magnetic stimulation implementation on stroke prognosis. Neurol. Sci. 2022, 43, 873–888. [Google Scholar] [CrossRef]
- Kokkotis, C.; Giarmatzis, G.; Giannakou, E.; Moustakidis, S.; Tsatalas, T.; Tsiptsios, D.; Vadikolias, K.; Aggelousis, N. An Explainable Machine Learning Pipeline for Stroke Prediction on Imbalanced Data. Diagnostics 2022, 12, 2392. [Google Scholar] [CrossRef]
- Hachinski, V.C.; Potter, P.; Merskey, H. Leuko-araiosis. Arch. Neurol. 1987, 44, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Vedala, K.; Nagabandi, A.K.; Looney, S.; Bruno, A. Factors associated with leukoaraiosis severity in acute stroke patients. J. Stroke Cerebrovasc. Dis. 2019, 28, 1897–1901. [Google Scholar] [CrossRef] [PubMed]
- Grueter, B.E.; Schulz, U.G. Age-related cerebral white matter disease (leukoaraiosis): A review. Postgrad. Med. J. 2012, 88, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Ay, H.; Arsava, E.M.; Rosand, J.; Furie, K.L.; Singhal, A.B.; Schaefer, P.W.; Wu, O.; Gonzalez, R.G.; Koroshetz, W.J.; Sorensen, A.G. Severity of leukoaraiosis and susceptibility to infarct growth in acute stroke. Stroke 2008, 39, 1409–1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawada, H.; Udaka, F.; Izumi, Y.; Nishinaka, K.; Kawakami, H.; Nakamura, S.; Kameyama, M. Cerebral white matter lesions are not associated with apoE genotype but with age and female sex in Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 2000, 68, 653–656. [Google Scholar] [CrossRef] [Green Version]
- de Leeuw, F.E.; de Groot, J.C.; Achten, E.; Oudkerk, M.; Ramos, L.M.; Heijboer, R.; Hofman, A.; Jolles, J.; van Gijn, J.; Breteler, M.M.B. Prevalence of cerebral white matter lesions in elderly people: A population based magnetic resonance imaging study. The Rotterdam scan study. J. Neurol. Neurosurg. Psychiatry 2001, 70, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Shi, Z.S.; Loh, Y.; Liebeskind, D.S.; Saver, J.L.; Gonzalez, N.R.; Tateshima, S.; Jahan, R.; Feng, L.; Vespa, P.M.; Starkman, S.; et al. Leukoaraiosis predicts parenchymal hematoma after mechanical thrombectomy in acute ischemic stroke. Stroke 2012, 43, 1806–1811. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Puri, A.S.; Khan, M.A.; Goddeau, R.P., Jr.; Henninger, N. Leukoaraiosis predicts a poor 90-day outcome after endovascular stroke therapy. AJNR Am. J. Neuroradiol. 2014, 35, 2070–2075. [Google Scholar] [CrossRef] [Green Version]
- Giurgiutiu, D.V.; Yoo, A.J.; Fitzpatrick, K.; Chaudhry, Z.; Leslie-Mazwi, T.; Schwamm, L.H.; Rost, N.S. Severity of leukoaraiosis, leptomeningeal collaterals, and clinical outcomes after intra-arterial therapy in patients with acute ischemic stroke. J. Neurointerv. Surg. 2015, 7, 326–330. [Google Scholar] [CrossRef]
- Gilberti, N.; Gamba, M.; Premi, E.; Costa, A.; Vergani, V.; Delrio, I.; Spezi, R.; Dikran, M.; Frigerio, M.; Gasparotti, R.; et al. Leukoaraiosis is a predictor of futile recanalization in acute ischemic stroke. J. Neurol. 2017, 264, 448–452. [Google Scholar] [CrossRef]
- Atchaneeyasakul, K.; Leslie-Mazwi, T.; Donahue, K.; Giese, A.K.; Rost, N.S. White Matter Hyperintensity Volume and Outcome of Mechanical Thrombectomy with Stentriever in Acute Ischemic Stroke. Stroke 2017, 48, 2892–2894. [Google Scholar] [CrossRef]
- Guo, Y.; Zi, W.; Wan, Y.; Zhang, S.; Sun, B.; Shang, X.; Li, S.; Bai, Y.; Li, Z.; Zheng, D.; et al. Leukoaraiosis severity and outcomes after mechanical thrombectomy with stent-retriever devices in acute ischemic stroke. J. Neurointerv. Surg. 2019, 11, 137–140. [Google Scholar] [CrossRef]
- Boulouis, G.; Bricout, N.; Benhassen, W.; Ferrigno, M.; Turc, G.; Bretzner, M. White matter hyperintensity burden in patients with ischemic stroke treated with thrombectomy. Neurology 2019, 93, e1498–e1506. [Google Scholar] [CrossRef]
- Liu, Y.; Gong, P.; Sun, H.; Zhang, S.; Zhou, J.; Zhang, Y. Leukoaraiosis is associated with poor outcomes after successful recanalization for large vessel occlusion stroke. Neurol. Sci. 2019, 40, 585–591. [Google Scholar] [CrossRef]
- Pedraza, M.I.; de Lera, M.; Bos, D.; Calleja, A.I.; Cortijo, E.; Gómez-Vicente, B.; Reyes, J.; Coco-Martín, M.B.; Calonge, T.; Agulla, J.; et al. Brain Atrophy and the Risk of Futile Endovascular Reperfusion in Acute Ischemic Stroke. Stroke 2020, 51, 1514–1521. [Google Scholar] [CrossRef]
- Mikati, A.G.; Mandelbaum, M.; Sapnar, S.; Puri, A.S.; Silver, B.; Goddeau, R.P., Jr.; Haussen, D.C.; Moonis, M.; Jun-O’Connell, A.H.; Henninger, N. Impact of Leukoaraiosis Severity on the Association of Time to Successful Reperfusion with 90-Day Functional Outcome after Large Vessel Occlusion Stroke. Transl. Stroke Res. 2020, 11, 39–49. [Google Scholar] [CrossRef]
- Guo, Y.; Zhang, S.; Li, M.; Sun, B.; Shang, X.; Li, S.; Bai, Y.; Li, Z.; Zi, W.; Liu, X. Leukoaraiosis and earlier neurological outcome after mechanical thrombectomy in acute ischemic stroke. J. Neuroradiol. 2020, 47, 428–432. [Google Scholar] [CrossRef]
- Mutzenbach, J.S.; Müller-Thies-Broussalis, E.; Killer-Oberpfalzer, M.; Griessenauer, C.J.; Hecker, C.; Moscote-Salazar, L.R.; Paradaiser, P.; Pikija, S. Severe Leukoaraiosis Is Associated with Poor Outcome after Successful Recanalization of M1 Middle Cerebral Artery Occlusion Strokes. Cerebrovasc. Dis. 2020, 49, 253–261. [Google Scholar] [CrossRef]
- Mechtouff, L.; Nighoghossian, N.; Amaz, C.; Buisson, M.; Berthezène, Y.; Derex, L.; Ong, E.; Eker, O.F.; Cho, T.-H. White matter burden does not influence the outcome of mechanical thrombectomy. J. Neurol. 2020, 267, 618–624. [Google Scholar] [CrossRef]
- Benson, J.; Seyedsaadat, S.M.; Mark, I.; Nasr, D.M.; Rabinstein, A.A.; Kallmes, D.F.; Brinjikji, W. Leukoaraiosis and acute ischemic stroke: 90-day clinical outcome following endovascular recanalization, with proposed “L-ASPECTS”. J. Neurointerv. Surg. 2021, 13, 384–389. [Google Scholar] [CrossRef]
- Kaginele, P.; Beer-Furlan, A.C.; Joshi, K.; Kadam, G.; Achanaril, A.; Levy, E.; Waqas, M.; Siddiqui, A.; Rai, H.; Snyder, K.; et al. Brain Atrophy and Leukoaraiosis Correlate with Futile Stroke Thrombectomy. J. Stroke Cerebrovasc. Dis. 2021, 30, 105871. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Hwang, Y.H.; Hong, J.M.; Choi, J.W.; Park, J.H.; Park, B.; Kang, D.-H.; Kim, Y.-W.; Hong, J.-H.; Yoo, J.; et al. Influence of cerebral microbleeds on mechanical thrombectomy outcomes. Sci. Rep. 2022, 12, 3637. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.H.; Zhuo, S.T.; Chen, Y.F.; Li, M.M.; Lin, Y.Y.; Yang, M.L.; Chen, Z.J. Factors influencing clinical outcomes of acute ischemic stroke treated with intravenous recombinant tissue plasminogen activator. Chin. Med. J. 2013, 126, 4685–4690. [Google Scholar]
- McAlpine, H.; Churilov, L.; Mitchell, P.; Dowling, R.; Teo, S.; Yan, B. Leukoaraiosis and early neurological recovery after intravenous thrombolysis. J. Stroke Cerebrovasc. Dis. 2014, 23, 2431–2436. [Google Scholar] [CrossRef] [PubMed]
- Willer, L.; Havsteen, I.; Ovesen, C.; Christensen, A.F.; Christensen, H. Computed Tomography--Verified Leukoaraiosis Is a Risk Factor for Post-thrombolytic Hemorrhage. J. Stroke Cerebrovasc. Dis. 2015, 24, 1126–1130. [Google Scholar] [CrossRef]
- IST-3 Collaborative Group. Association between brain imaging signs, early and late outcomes, and response to intravenous alteplase after acute ischaemic stroke in the third International Stroke Trial (IST-3): Secondary analysis of a randomised controlled trial. Lancet Neurol. 2015, 14, 485–496. [Google Scholar] [CrossRef] [Green Version]
- Nighoghossian, N.; Abbas, F.; Cho, T.H.; Geraldo, A.F.; Cottaz, V.; Janecek, E.; Mechtouff, L.; Bischoff, M.; El Khoury, C.; Schott, A.M.; et al. Impact of leukoaraiosis on parenchymal hemorrhage in elderly patients treated with thrombolysis. Neuroradiology 2016, 58, 961–967. [Google Scholar] [CrossRef]
- Arba, F.; Palumbo, V.; Boulanger, J.M.; Pracucci, G.; Inzitari, D.; Buchan, A.M.; Hill, M.D.; on behalf of CASES Investigators. Leukoaraiosis and lacunes are associated with poor clinical outcomes in ischemic stroke patients treated with intravenous thrombolysis. Int. J. Stroke 2016, 11, 62–67. [Google Scholar] [CrossRef]
- Zhong, G.; Yan, S.; Zhang, S.; Chen, Q.; Lai, Y.; Lou, M. Association between Leukoaraiosis and Poor Outcome is not due to Reperfusion Inefficiency after Intravenous Thrombolysis. Transl. Stroke Res. 2016, 7, 439–445. [Google Scholar] [CrossRef]
- Prats-Sanchez, L.; Martínez-Domeño, A.; Camps-Renom, P.; Delgado-Mederos, R.; Guisado-Alonso, D.; Marín, R.; Guisado-Alonso, D.; Marín, R.; Dorado, L.; Rudilosso, S.; et al. Risk factors are different for deep and lobar remote hemorrhages after intravenous thrombolysis. PLoS ONE 2017, 12, e0178284. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhang, M.; Chen, Y.; Gao, P.; Yun, W.; Zhou, X. The degree of leukoaraiosis predicts clinical outcomes and prognosis in patients with middle cerebral artery occlusion after intravenous thrombolysis. Brain Res. 2018, 1681, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Nagaraja, N.; Tasneem, N.; Shaban, A.; Dandapat, S.; Ahmed, U.; Policeni, B.; Olalde, H.; Shim, H.; Samaniego, E.A.; Pieper, C.; et al. Cerebral Microbleeds are an Independent Predictor of Hemorrhagic Transformation Following Intravenous Alteplase Administration in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.M.; Hung, C.L.; Su, H.C.; Lin, H.J.; Chen, C.H.; Lin, C.C.; Hu, H.-H.; Lin, S.-H.; Sung, P.-S. Leukoaraiosis and risk of intracranial hemorrhage and outcome after stroke thrombolysis. PLoS ONE 2018, 13, e0196505. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, M.; Bao, H.; Zhang, Z.; Mei, Y.; Yun, W.; Zhou, X. The efficacy of intravenous thrombolysis in acute ischemic stroke patients with white matter hyperintensity. Brain Behav. 2018, 8, e01149. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Yan, S.; Xu, M.; Zhong, G.; Liebeskind, D.S.; Lou, M. More extensive white matter hyperintensity is linked with higher risk of remote intracerebral hemorrhage after intravenous thrombolysis. Eur. J. Neurol. 2018, 25, 380-e15. [Google Scholar] [CrossRef]
- Delcourt, C.; Wang, X.; Zhou, Z.; Wardlaw, J.M.; Mair, G.; Robinson, T.G.; Chen, X.; Yoshimura, S.; Torii-Yoshimura, T.; Carcel, C.; et al. Brain imaging abnormalities and outcome after acute ischaemic stroke: The ENCHANTED trial. J. Neurol. Neurosurg. Psychiatry 2020, 91, 1290–1296. [Google Scholar] [CrossRef]
- Zivanovic, Z.; Ostojic, Z.; Rajic, S.; Vlahovic, D.; Mijajlovic, M.; Jovicevic, M. Outcome after intravenous thrombolysis in embolic stroke of undetermined source compared to cardioembolic stroke. Wien. Klin. Wochenschr. 2020, 132, 515–520. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, X.; Tian, C.; Wang, J. The relationship of leukoaraiosis, haemorrhagic transformation and prognosis at 3 months after intravenous thrombolysis in elderly patients aged ≥ 60 years with acute cerebral infarction. Neurol. Sci. 2020, 41, 3195–3200. [Google Scholar] [CrossRef]
- Qiu, F.; Chen, C.; Fan, Z.; Qiu, J.; Chen, Q.; Shao, B. White Matter Hypoperfusion Associated with Leukoaraiosis Predicts Intracranial Hemorrhage after Intravenous Thrombolysis. J. Stroke Cerebrovasc. Dis. 2021, 30, 105528. [Google Scholar] [CrossRef]
- Capuana, M.L.; Lorenzano, S.; Caselli, M.C.; Paciaroni, M.; Toni, D. Hemorrhagic risk after intravenous thrombolysis for ischemic stroke in patients with cerebral microbleeds and white matter disease. Neurol. Sci. 2021, 42, 1969–1976. [Google Scholar] [CrossRef]
- da Silva-Candal, A.; Pérez-Mato, M.; Rodríguez-Yáñez, M.; López-Dequidt, I.; Pumar, J.M.; Ávila-Gómez, P.; Sobrino, T.; Campos, F.; Castillo, J.; Hervella, P.; et al. The presence of leukoaraiosis enhances the association between sTWEAK and hemorrhagic transformation. Ann. Clin. Transl. Neurol. 2020, 7, 2103–2114. [Google Scholar] [CrossRef]
- Hervella, P.; Pérez-Mato, M.; Rodríguez-Yáñez, M.; López-Dequidt, I.; Pumar, J.M.; Sobrino, T.; Campos, F.; Castillo, J.; da Silva-Candal, A.; Iglesias-Rey, R. sTWEAK as Predictor of Stroke Recurrence in Ischemic Stroke Patients Treated with Reperfusion Therapies. Front. Neurol. 2021, 12, 652867. [Google Scholar] [CrossRef]
- Sudre, J.; Venditti, L.; Ancelet, C.; Chassin, O.; Sarov, M.; Smadja, D.; Chausson, N.; Lun, F.; Laine, O.; Duron, E.; et al. Reperfusion therapy for acute ischemic stroke in older people: An observational real-life study. J. Am. Geriatr. Soc. 2021, 69, 3167–3176. [Google Scholar] [CrossRef]


{kind=link}
| Authors, Year of Publication | Number of Participants/Age of Participants | Follow-Up Time | LA/WMH Assessment | Time of Neuroimaging | Time to Recanalization | Scale of Stroke Severity and Prognosis/Clinical Outcome | Main Results | |
|---|---|---|---|---|---|---|---|---|
| Endovascular stroke therapy | ||||||||
| Shi et al., 2012 [27] | 105/ 65.9 ± 18.9 | Until discharge | Fazekas scale | On admission and 3–12 h after MT | median of 5–5.8 h from symptom onset | NIHSS on admission, mRS at discharge | Patients with moderate or severe LA had worse clinical outcomes at discharge and higher rates of in-hospital mortality. Also, severity of LA was an independent predictor of hemorrhagic transformation and parenchymal hematoma |
| Zhang et al., 2014 [28] | 129/ 71 (58–80) | 90 days | Van Swieten scale | On admission and within 7 days | NA | NIHSS on admission, mRS scores at the time of presentation, discharge, and at 90 days | Severe LA was independently associated with a poor outcome at 90 days after endovascular stroke therapy. Moreover, among patients who were alive at discharge, those with severe LA had significantly less frequent improvement in the mRS score from discharge to 90 days |
| Giurgiutiu et al., 2015 [29] | 73/ 67.2 (SD 15.7) | 90 days | WMH Volumetry | Pre-intervention and within 24 h | within 6 h from symptom onset | NIHSS on admission, mRS at day 90 | Good collateral circulation grade in AIS patients undergoing IAT was independently associated with reduced LA volume, and higher LA volume decreased the odds of a good outcome, but LA did not appear to be a contraindication for acute intervention |
| Gilberti et al., 2017 [30] | 68/ 74 (IQR 66–79) | 90 days | van Swieten scale | On admission and within 24 h after MT | mean of 245.1 min from symptom onset | NIHSS at baseline, mRS at day 90 | The presence of moderate to severe LA was an independent predictor of futile recanalization |
| Atchaneeyasakul et al., 2017 [31] | 56/ 67.3 ± 14.2 | 90 days | WMH Volumetry | On admission and within 24 h after MT | within 6 h from symptom onset | mRS at discharge and at 90 days | Increasing WMH volume did not significantly affect the odds of 90-day good outcome, intracerebral hemorrhage, parenchymal hematoma, successful recanalization, or death after mechanical thrombectomy using stentrievers |
| Guo et al., 2019 [32] | 251/ 64.4 (SD 11.8) | 90 days | Van Swieten scale | Pre-intervention | mean of 361 min from symptom onset | NIHSS pre-treatment, mRS pre-treatment and at 90 days | Severe LA was a significant predictor of poor functional outcome at 90 days in acute stroke patients undergoing mechanical thrombectomy with stent-retriever devices. Additionally, the prevalence of futile recanalization and the mortality rate in patients with severe LA was higher than that in patients with absent-to-moderate LA, but the rate of symptomatic ICH was similar between the two groups |
| Boulouis et al., 2019 [33] | 496/68.1 ± 15.0 | 90 days | WMH Volumetry | Baseline MRI | within 5 h of symptom onset | NIHSS at baseline, mRS at 90 days | Patients exhibited increasingly worse outcomes with increasing WMH severity, but WMH volume was not associated with sICH rate, nor did it influence recanalization success. More than a quarter of patients in the highest WMH quartile experienced favorable 3-month outcomes, which suggests that MT should not be denied in patients with a high WMH burden |
| Liu et al., 2019 [34] | 97/ 70.0 ± 12.4 | 90 days | Fazekas scale | On admission and within 24 h after MT | mean of 338 min from symptom onset | NIHSS on admission, mRS at 3 months | Patients with moderate to severe LA had more than 3 times higher risk of having poor 90-day outcomes compared to patients with absent to mild LA, after successful recanalization. Also, patients with higher LA scores appeared to have an increased risk of any type of hemorrhage or symptomatic ICH, but the difference did not reach statistical significance |
| Pedraza et al., 2020 [35] | 295/ 71.29 ± 13.27 | 3 months | Fazekas scale | On admission | NA | NIHSS at baseline, mRS at baseline and at 3 months | Futile reperfusion (mRS score > 2 at 3 months) was associated with higher scores on the Fazekas scale |
| Mikati et al., 2020 [36] | 144/ 68 (57–81) | 90 days | van Swieten scale | On admission | within 24 h from symptom onset | NIHSS at the time of presentation, mRS at admission and at 90 days | Greater pre-existing LA was associated with poor 90-day functional outcome after successful reperfusion and LA impacted the association between the symptom onset-to-reperfusion time and 90-day mRS. Specifically, reperfusion had to occur at least 2 h earlier in subjects with moderate-to-severe LA than in those with absent-to-mild for similar 90-day functional outcomes |
| Guo et al., 2020 [37] | 273/ 64.4 (SD 11.9) | 90 days | van Swieten scale | On admission and within 24 h after MT | median of 360 min from symptom onset | NIHSS at baseline and after 24 h, mRS at 90 days | There was a significantly lower ENI rate (defined as a decrease of ≥4 points on the NIHSS, or an NIHSS score of zero 24 h after baseline assessment) and non-significantly higher END rate (defined as an increase of ≥4 points on the NIHSS 24 h after baseline) in patients with severe LA compared with patients with absent-to-moderate LA. However, when the analysis was restricted to patients without ICH, severe LA was a significant independent predictor of END |
| Mutzenbach et al., 2020 [38] | 209/ 75.0 (IQR 63.0–81.0) | 3 months | ARWMC scale | NA | mean of 247 min from symptom onset | NIHSS on admission, mRS at 3 months | Severe LA was associated with poor clinical outcomes at 3 months in acute stroke patients undergoing MT due to emergent M1 middle cerebral artery occlusion. Moreover, there were more hospital deaths in the severe LA group than in the absent to moderate LA group, but there were no associations between LA and the presence of ICH |
| Mechtouf et al., 2020 [39] | 293/ 67.12 (SD 16.23) | 90 days | Fazekas scale | On admission | mean of 233 min from symptom onset | NIHSS at baseline and at discharge, mRS at day 90 | Although WMH severity was moderately associated with a poor outcome, it was not an independent predictor in multivariate analysis. Also, WMHs severity did not influence the risk of parenchymal hemorrhage or the rate of futile recanalization |
| Benson et al., 2021 [40] | 174/ 68.0 ± 9.1 | 90 days | Fazekas scale | Pre-intervention | NA | NIHSS at baseline, mRS at day 90 | LA severity was associated with worse 90-day outcome, even after successful recanalization, and it was an independent risk factor for worse outcomes |
| Kaginele et al., 2021 [41] | 175/ 77.15 (SD 7.09) | 90 days | Fazekas scale | Pre-intervention | median of 300 min from symptom onset | NIHSS on admission, mRS at day 90 | Increasing brain atrophy and LA severity correlated with decreasing rates of 90-day good functional outcome, suggesting that a simplified, visual assessment of their degree on plain head CT was associated with futile recanalization in patients age > 65 years |
| Lee et al., 2022 [42] | 577/67 ± 13 | 3 months | CREDOS WMH visual rating scale | CT at baseline, MRI pretreatment | within 24 h of symptom onset | NIHSS at baseline, mRS at 3 months | Increased WMH burden was significantly associated with poorer functional outcomes |
| Intravenous Thrombolysis | ||||||||
| Huang et al., 2013 [43] | 101 | 90 days | Presence or absence of LA | On admission and 24 h after IVT and at clinical deterioration | within 4.5 h from symptom onset | NIHSS at baseline, mRS at day 90 | The good outcome group had fewer patients with LA and the absence of LA before thrombolysis was significantly associated with better functional outcome |
| McAlpine et al., 2014 [44] | 158/ 77 (IQR 68-84) | 3 months | Van Swieten scale | On admission | within 4.5 h from symptom onset | NIHSS at onset, and at 24 h after IVT, mRS at onset and at 3 months | There was no evidence of the association between the degree of LA and early neurological recovery after IVT |
| Willer et al., 2015 [45] | 311 | 36 h | Fazekas scale, ARWMC scale | On admission | within 4.5 h from symptom onset | NIHSS | LA doubles the risk of post-thrombolytic hemorrhagic transformation and symptomatic hemorrhage, but it was not an independent predictor of HT |
| The IST-3 collaborative group, 2015 [46] | 3017 | 6 months | Fazekas scale, van Swieten scale | Pre-intervention and within 24–48 h poststroke and at clinical deterioration within 7 days | within 6 h of symptom onset | NIHSS at baseline, OHS at 6 months | LA and severe atrophy predicted death, reduced chance of being independent, and diminished chance of a favorable outcome at 6 months |
| Nighoghossian et al., 2016 [47] | 180/ 81.3 (SD 4.6) | 3 months | Fazekas scale | On admission | mean time of 164.1 min from symptom onset | NIHSS at baseline, mRS at 3 months | In elderly patients treated with intravenous thrombolysis, severe LA was associated with HT and after adjusting for NIHSS and infarct volume it remained the only independent predictor of parenchymal hemorrhage |
| Arba et al., 2016 [48] | 820/ 71.3 ± 13.2 | 90 days | Van Swieten scale | On admission | within 3 h from symptom onset | NIHSS at baseline, mRS at day 90 | In patients younger than 80 years of age, severe SVD (comprising the presence and severity of LA and lacunes on baseline computer tomography scan) consistently reduced the chances to have either excellent or good neurological outcomes. The global burden of SVD was significantly associated with symptomatic hemorrhagic transformation in the whole cohort study, with a fivefold increase of risk in patients with severe SVD |
| Zhong et al., 2016 [49] | 79/ 69.99 ± 11.76 | 3 months | Fazekas scale | On admission and at 24 h after IVT | within 6 h of symptom onset | NIHSS at baseline, mRS at 3 months | Severe LA was associated with infarct growth and it was also an independent predictor of poor 3 months functional outcome after adjusting for reperfusion and baseline severity of stroke, but the burden of LA did not correlate with reperfusion inefficiency after IVT |
| Prats-Sanchez et al., 2017 [50] | 934/ 73.9 ± 12.6 | 14 days | Fazekas scale | On admission and within 36 h after IVT | mean of 144 min | NIHSS on admission | Lobar, but not deep, remote parenchymal hemorrhage were associated with the presence of severe LA |
| Liu et al., 2018 [51] | 97/ 66.6 ± 9.1 | 90 days | Fazekas scale | NA | within 4.5 h from symptom onset | Baseline NIHSS, FMS at baseline and at 90 days | Moderate to severe LA was an independent predictor of 90-day poor functional outcome and the patients in this group had a higher rate of hemorrhagic transformation and recurrent stroke. Interestingly, the percentage of the mild LA group was higher in early neurological recovery than that of the no LA or the moderate to severe LA group |
| Nagaraja et al., 2018 [52] | 366/ 67 ± 15 | 36 h | Fazekas scale | On admission and at 24 h | NA | NIHSS on admission | The presence of FLAIR LA in the deep or periventricular white matter was not associated with HT |
| Yang et al., 2018 [53] | 614/ 67.4 ± 12.6 | 3 months | modified Van Swieten scale, ARWMC scale | Pre-intervention and within 24–36 h after IVT | within 4.5 h from symptom onset | NIHSS at baseline, mRS at 3 months | There was no significant difference in the risk of symptomatic ICH between patients with and without severe LA, regardless of having used different LA rating scales. However, severe LA was independently associated with poor functional outcomes at 3 months |
| Liu et al., 2018 [54] | 113/ 67.5 ± 10.9 | 90 days | Fazekas scale | On admission | within 4.5 h from symptom onset | NIHSS on admission and 24 h later, FMS at admission and at day 90 | Deep WMH patients undergoing IVT had a higher risk of END (defined as an increase of ≥1 point on the motor NIHSS score or ≥2 points on the total NIHSS score 72 h after admission) and HT than deep WMH patients without IVT. Also, periventricular hyperintensities were an independent risk factor for stroke recurrence in AIS patients |
| Chen et al., 2018 [55] | 503/ 67.12 ± 12.76 | 3 months | WMH Volumetry | On admission and within 24 h after IVT | within 6 h from symptom onset | NIHSS on admission, mRS at 3 months | Patients with remote ICH had significantly larger WMH volumes, both periventricular and deep, than those without. WMH volume was also associated with local parenchymal hemorrhage, even after adjusting for admission NIHSS score and atrial fibrillation history. Lastly, WMH volume was associated with a 3-month poor functional outcome after adjusting for the variables of age, admission NIHSS score, and onset-to-needle time |
| Delcourt et al., 2020 [56] | 2916/ 67 ± 13 | 90 days | Van Swieten scale, Fazekas scale | On admission and at follow-up | within 4.5 h from symptoms onset | NIHSS at baseline, 24 h, and at day 7, mRS at 90 days | Severe LA reduced the chance of good functional outcomes, predicted any ICH and was associated with 90-day mortality |
| Zivanovic et al., 2020 [57] | 175 | 3 months | Presence or absence | On admission and within 24–48 h after IVT | mean of 155.6 min | NIHSS on admission, mRS at discharge and at 3 months | Independent predictors of a 3-month favorable outcome were ESUS, the absence of LA on CT, and the absence of diabetes |
| Zhang et al., 2020 [58] | 125/ 73.2 ± 8.2 | 3 months | Modified van Swieten scale | Pre-intervention and at 24 h after IVT and at clinical deterioration | within 4.5 h from symptoms onset | NIHSS on admission, mRS at 3 months | Severe LA was evidently associated with HT and with poor functional prognosis 3 months after IVT in elderly patients |
| Qiu et al., 2021 [59] | 175/ 67.0 ± 11.6 | 90 days | Fazekas scale | On admission and at 24 h after IVT | mean of 187 min from symptom onset | NIHSS on admission and at discharge, mRS at day 90 | White matter hypoperfusion, reflecting the severity of LA, was independently associated with ICH after intravenous thrombolysis, but it did not increase the risk of poor prognosis |
| Capuana et al., 2021 [60] | 434/ 68.3 ± 13.5 | 3 months | Fazekas scale | On admission or within 24 h after IVT | mean of 180 min from symptom onset | NIHSS at baseline, mRS at 3 months | Higher Fazekas scale score was significantly associated with more severe ICH and with poor functional outcome at 90 days, but it was not an independent predictor of symptomatic ICH, mortality, or functional outcome in adjusted analyses |
| Intravenous thrombolysis and/or endovascular stroke therapy | ||||||||
| 1. | da Silva-Candal et al., 2020 [61] | 875 (710 IVT, 87 EST, 78 both)/72.3 ± 12.2 | 3 months | Fazekas scale | MRI or CT study at admission and between 4th–7th day | Within 6 h from symptom onset | NIHSS at admission, every 6 h during the first day, and every 24 h during hospitalization, mRs at discharge, and at 3 months | The presence and grade of LA had a significant impact on symptomatic HT and LA degree was independently associated with poor functional outcome |
| 2. | Hervella et al., 2021 [62] | 875 (710 IVT, 87 EST, 78 both) | 25 ± 13 months | Fazekas scale | CT was performed in all patients and MRI in selected patients at admission. Follow-up CT scan after reperfusion therapy was performed in all patients at 24 h, and CT at 48 h or at any time if neurological deterioration was detected; and between the 4th and 7th day | Within 4.5 h from symptom onset | NIHSS at admission, every 6 h during the first day, and every 24 h during hospitalization, mRs at discharge, and at 3 months | Greater severity of LA was independently associated with higher probability of stroke recurrence |
| 3. | Sudre et al., 2021 [63] | 1000 (199 IVT, 278 EST, 523 both) | 3 months | Fazekas scale | NM | NM | NIHSS at admission, mRS at 3 months | The absence of severe Fazekas grade 3 periventricular white matter lesions was significantly associated with good outcome at 3 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karatzetzou, S.; Tsiptsios, D.; Sousanidou, A.; Christidi, F.; Psatha, E.A.; Chatzaki, M.; Kitmeridou, S.; Giannakou, E.; Karavasilis, E.; Kokkotis, C.; et al. Elucidating the Role of Baseline Leukoaraiosis on Forecasting Clinical Outcome of Acute Ischemic Stroke Patients Undergoing Reperfusion Therapy. Neurol. Int. 2022, 14, 923-942. https://doi.org/10.3390/neurolint14040074
Karatzetzou S, Tsiptsios D, Sousanidou A, Christidi F, Psatha EA, Chatzaki M, Kitmeridou S, Giannakou E, Karavasilis E, Kokkotis C, et al. Elucidating the Role of Baseline Leukoaraiosis on Forecasting Clinical Outcome of Acute Ischemic Stroke Patients Undergoing Reperfusion Therapy. Neurology International. 2022; 14(4):923-942. https://doi.org/10.3390/neurolint14040074
Chicago/Turabian StyleKaratzetzou, Stella, Dimitrios Tsiptsios, Anastasia Sousanidou, Foteini Christidi, Evlampia A. Psatha, Marilena Chatzaki, Sofia Kitmeridou, Erasmia Giannakou, Efstratios Karavasilis, Christos Kokkotis, and et al. 2022. "Elucidating the Role of Baseline Leukoaraiosis on Forecasting Clinical Outcome of Acute Ischemic Stroke Patients Undergoing Reperfusion Therapy" Neurology International 14, no. 4: 923-942. https://doi.org/10.3390/neurolint14040074