
Anatomical Variations of the Sciatic Nerve Exit from the Pelvis and Its Relationship with the Piriformis Muscle: A Cadaveric Study


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
2.2. Dissection Technique
2.3. Ethical and Bioethical Principles
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brooks, J.B.B.; Silva, C.A.C.; Soares, S.A.; Kai, M.R.; Cabral, R.H.; Fragoso, Y.D. Anatomical variations of the sciatic nerve in a group of Brazilian cadavers. Rev. Dor 2011, 12, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Karmakar, M.K.; Reina, M.A.; Sivakumar, R.K.; Areeruk, P.; Pakpirom, J.; Sala-Blanch, X. Ultrasound-guided subparaneural popliteal sciatic nerve block: There is more to it than meets the eyes. Reg. Anesth. Pain Med. 2021, 46, 268–275. [Google Scholar] [CrossRef]
- Singh, H.; Gargya, A.; Lin, T.; Gulati, A. Sciatic, Femoral, and Lateral Femoral Cutaneous Nerve Ultrasound-Guided Percutaneous Peripheral Nerve Stimulation. Pain Med. 2020, 21 (Suppl. 1), S47–S50. [Google Scholar] [CrossRef] [PubMed]
- San-Emeterio-Iglesias, R.; Minaya-Muñoz, F.; Romero-Morales, C.; De-la-Cruz-Torres, B. Correct Sciatic Nerve Management to Apply Ultrasound-Guided Percutaneous Neuromodulation in Patients with Chronic Low Back Pain: A Pilot Study. Neuromodulation 2021, 24, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Selame, L.A.; McFadden, K.; Duggan, N.M.; Goldsmith, A.J.; Shokoohi, H. Ultrasound-Guided Transgluteal Sciatic Nerve Block for Gluteal Procedural Analgesia. J. Emerg. Med. 2021, 60, 512–516. [Google Scholar] [CrossRef]
- Wessig, C.; Koltzenburg, M.; Reiners, K.; Solymosi, L.; Bendszus, M. Muscle magnetic resonance imaging of denervation and reinnervation: Correlation with electrophysiology and histology. Exp. Neurol. 2004, 185, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Filler, A.G.; Maravilla, K.R.; Tsuruda, J.S. MR neurography and muscle MR imaging for image diagnosis of disorders affecting the peripheral nerves and musculature. Neurol. Clin. 2004, 22, 643–682. [Google Scholar] [CrossRef]
- Sulak, O.; Sakalli, B.; Ozguner, G.; Kastamoni, Y. Anatomical relation between sciatic nerve and piriformis muscle and its bifurcation level during fetal period in human. Surg. Radiol. Anat. 2014, 36, 265–272. [Google Scholar] [CrossRef]
- Calvo Delfino, M.; Frydman, J.; Pfund, G. Variación Anatómica en la Formación y Emergencia del Nervio Ciático: Reporte de Caso. Available online: http://www.revista-anatomia.com.ar/archivos-parciales/2017-1-revista-argentina-de-anatomia-online-a.pdf (accessed on 10 August 2022).
- Di Giovanna, E.L.; Schiowitz, S.; Dowling, D.J. An Osteopathic Approach to Diagnosis and Treatment, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Chaitow, L. Soft Tissue Manipulation: A Practitioner’s Guide to the Diagnosis and Treatment of Soft-Tissue Dysfunction and Reflex Activity; Healing Arts Press: Rochester, VT, USA, 1988; p. 1. [Google Scholar]
- Testut, L. Tomo Primero: Osteologίa, Artrologίa, Miologίa, Tratado de Anatomίa Humana, 6th ed.; Editorial Salvat: Barcelona, Spain, 1984; Volume 252. [Google Scholar]
- Beaton, L.E.; Anson, B.J. The relation of the sciatic nerve and its subdivisions to the piriformis muscle. Anat. Rec. 1937, 70, 1–5. [Google Scholar] [CrossRef]
- Beaton, L.E. The sciatic nerve and piriform muscle: Their interrelationa possible cause of coccgodynia. J. Bone Jt. Surg. Am. 1938, 20, 686–688. [Google Scholar]
- Pooja, R.; Sunita, K. A cadaveric study of normal and variant levels of division of sciatic nerve and coupled anomalies with clinical application in surgical interventions. Int. J. Anat. Res. 2015, 3, 1230–1236. [Google Scholar]
- Güleç, G.G.; Kurt Oktay, K.N.; Aktaş, İ.; Yılmaz, B. Visualizing Anatomic Variants of the Sciatic Nerve Using Diagnostic Ultrasound During Piriformis Muscle Injection: An Example of 4 Cases. J. Chiropr. Med. 2022, 21, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Berihu, B.A.; Debeb, Y.G. Anatomical variation in bifurcation and trifurcations of sciatic nerve and its clinical implications: In selected university in Ethiopia. BMC Res. Notes 2015, 8, 633. [Google Scholar] [CrossRef] [Green Version]
- Monte de Oca, F. Prospective Cross-Sectional Study of Frequency of Anatomical Variations in the Exit of the Sciatic Nerve in Relation to the Piriformis Muscle; Institute of Human Anatomy, Autonomous University of Santo Domingo: Salt Lake City, UT, USA, 2018; Volume 1, p. 1. [Google Scholar]
- Budhiraja, V.; Rastogi, R.; Jain, S.K.; Sharma, N.; Garg, R.; Nafees, H. Variations in the relationship of the sciatic nerve to the piriformis muscle: A cadaveric study in North India. Argent. J. Clin. Anat. 2016, 8, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Atoni, A.D.; Oyinbo, C.A.; Francis, D.A.U.; Tabowei, U.L. Anatomic Variation of the Sciatic Nerve: A Study on the Prevalence, and Bifurcation Loci in Relation to the Piriformis and Popliteal Fossa. Acta Med. Acad. 2022, 51, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Natsis, K.; Totlis, T.; Konstantinidis, G.A.; Paraskevas, G.; Piagkou, M.; Koebke, J. Anatomical variations between the sciatic nerve and the piriformis muscle: A contribution to surgical anatomy in piriformis syndrome. Surg. Radiol. Anat. 2014, 36, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Ogeng’o, J.A.; El-Busaidy, H.; Mwika, P.M.; Khanbhai, M.M.; Munguti, J. Variant anatomy of sciatic nerve in a black Kenyan population. Folia Morphol. 2011, 70, 175–179. [Google Scholar]
- Barbosa, A.B.M.; Santos, P.V.D.; Targino, V.A.; Silva, N.D.A.; Silva, Y.C.D.M.; Gomes, F.B.; Assis, T.D.O. Sciatic nerve and its variations: Is it possible to associate them with piriformis syndrome? Arq. Neuro-Psiquiatr. 2019, 77, 646–653. [Google Scholar] [CrossRef]
- Poutoglidou, F.; Piagkou, M.; Totlis, T.; Tzika, M.; Natsis, K. Sciatic Nerve Variants and the Piriformis Muscle: A Systematic Review and Meta-Analysis. Cureus 2020, 12, e11531. [Google Scholar] [CrossRef]
- Montemurro, N.; Ortenzi, V.; Naccarato, G.A.; Perrini, P. Angioleiomyoma of the knee: An uncommon cause of leg pain. A systematic review of the literature. Interdiscip. Neurosurg. 2020, 22, 100877. [Google Scholar] [CrossRef]
- Mishra, R.; Narayanan, M.K.; Umana, G.E.; Montemurro, N.; Chaurasia, B.; Deora, H. Virtual Reality in Neurosurgery: Beyond Neurosurgical Planning. Int. J. Environ. Res. Public Health 2022, 19, 1719. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, K.; Khan, S.I.; Zaman, N.; Montemurro, N.; Ahmed, N.; Chaurasia, B. Fusion versus nonfusion treatment for recurrent lumbar disc herniation. J. Craniovertebr. Junction Spine 2021, 12, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Snow, P.W.; Dimante, D.; Sinisi, M.; Loureiro, R.C.V. Virtual Reality combined with Robotic facilitated movements for pain management and sensory stimulation of the upper limb following a Brachial Plexus injury: A case study. In Proceedings of the 2022 International Conference on Rehabilitation Robotics (ICORR), Rotterdam, The Netherlands, 25–29 July 2022; Volume 22, pp. 1–6. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number | (%) |
|---|---|---|
| Overall anatomical bodies | 20 | 100 |
| Sciatic nerve studied | 40 | 100 |
| Sex | ||
| Male | 10 | 50 |
| Female | 10 | 50 |
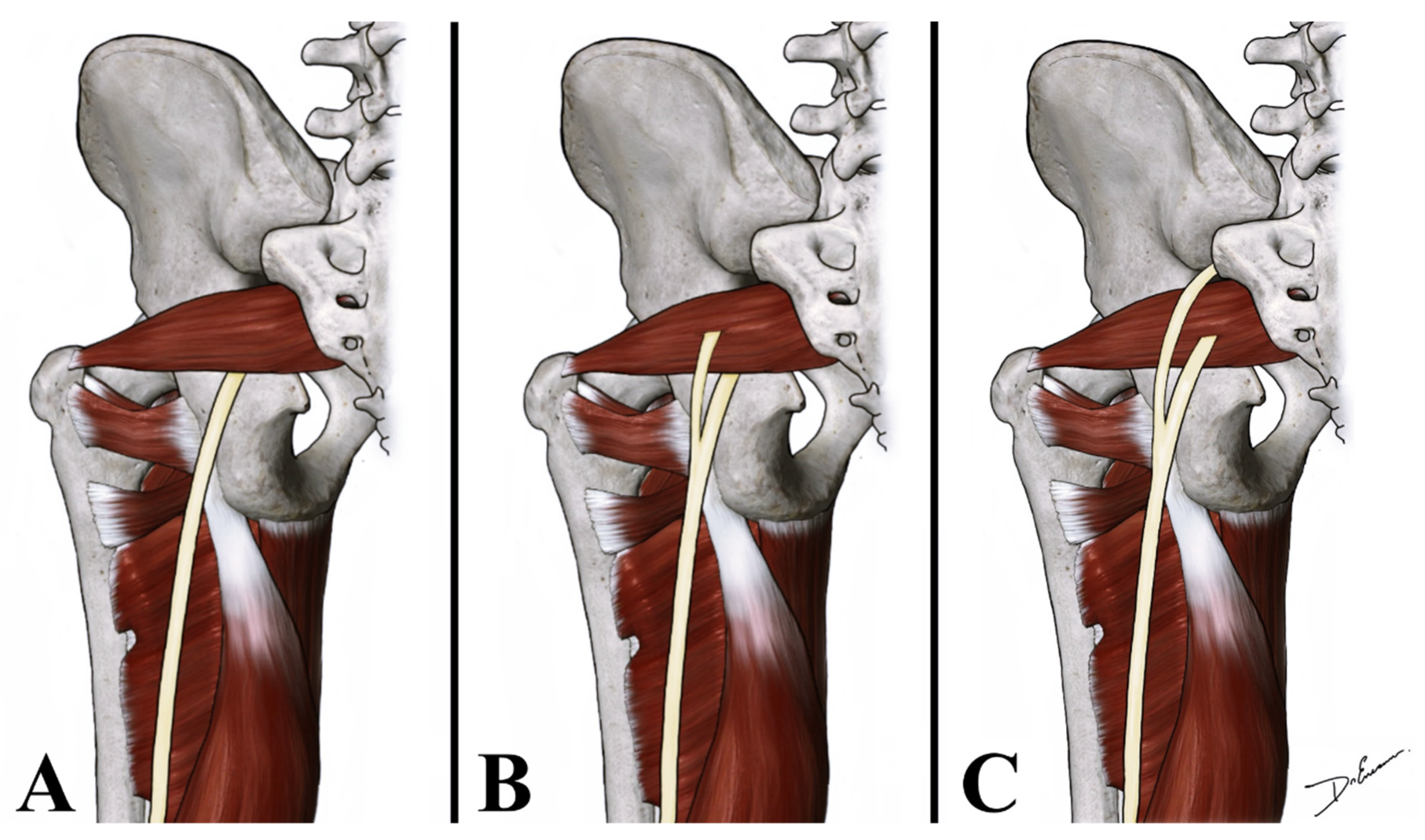
| Anatomical variations of the SN exit from the pelvis | ||
| Inferior to the PM | 37 | 92.5 |
| Between the fascicles of the PM and inferior to the PM | 2 | 5 |
| Between the fascicles of the PM and superior to the PM | 1 | 2.5 |
| Anatomical variations of the SN exit from the pelvis among sex | ||
| Male | 1/20 | 5 |
| Female | 2/20 | 10 |
| Anatomical variation of the SN according to the side of the body | ||
| Unilateral | 3/3 | 100 |
| Bilateral | 0/3 | 0 |
| Side of anatomical variation of the SN | ||
| Right | 1/20 | 5 |
| Left | 2/20 | 10 |
| Region of division of the SN into tibial nerve and the common peroneal trunk | ||
| Gluteal region | 14 | 35 |
| Middle third of the thigh | 4 | 10 |
| Proximal part of the popliteal fossa | 22 | 55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reynoso, J.P.; De Jesus Encarnacion, M.; Nurmukhametov, R.; Melchenko, D.; Efe, I.E.; Goncharov, E.; Taveras, A.A.; Ramirez Pena, I.J.; Montemurro, N. Anatomical Variations of the Sciatic Nerve Exit from the Pelvis and Its Relationship with the Piriformis Muscle: A Cadaveric Study. Neurol. Int. 2022, 14, 894-902. https://doi.org/10.3390/neurolint14040072
Reynoso JP, De Jesus Encarnacion M, Nurmukhametov R, Melchenko D, Efe IE, Goncharov E, Taveras AA, Ramirez Pena IJ, Montemurro N. Anatomical Variations of the Sciatic Nerve Exit from the Pelvis and Its Relationship with the Piriformis Muscle: A Cadaveric Study. Neurology International. 2022; 14(4):894-902. https://doi.org/10.3390/neurolint14040072
Chicago/Turabian StyleReynoso, Juan Pablo, Manuel De Jesus Encarnacion, Renat Nurmukhametov, Dmitry Melchenko, Ibrahim E. Efe, Evgeniy Goncharov, Angel Alfonso Taveras, Issael Jesus Ramirez Pena, and Nicola Montemurro. 2022. "Anatomical Variations of the Sciatic Nerve Exit from the Pelvis and Its Relationship with the Piriformis Muscle: A Cadaveric Study" Neurology International 14, no. 4: 894-902. https://doi.org/10.3390/neurolint14040072