
Ranibizumab Port Delivery System in Neovascular Age-Related Macular Degeneration: Where Do We Stand? Overview of Pharmacokinetics, Clinical Results, and Future Directions

 , ,
, ,
Abstract
:1. Introduction
2. Methods
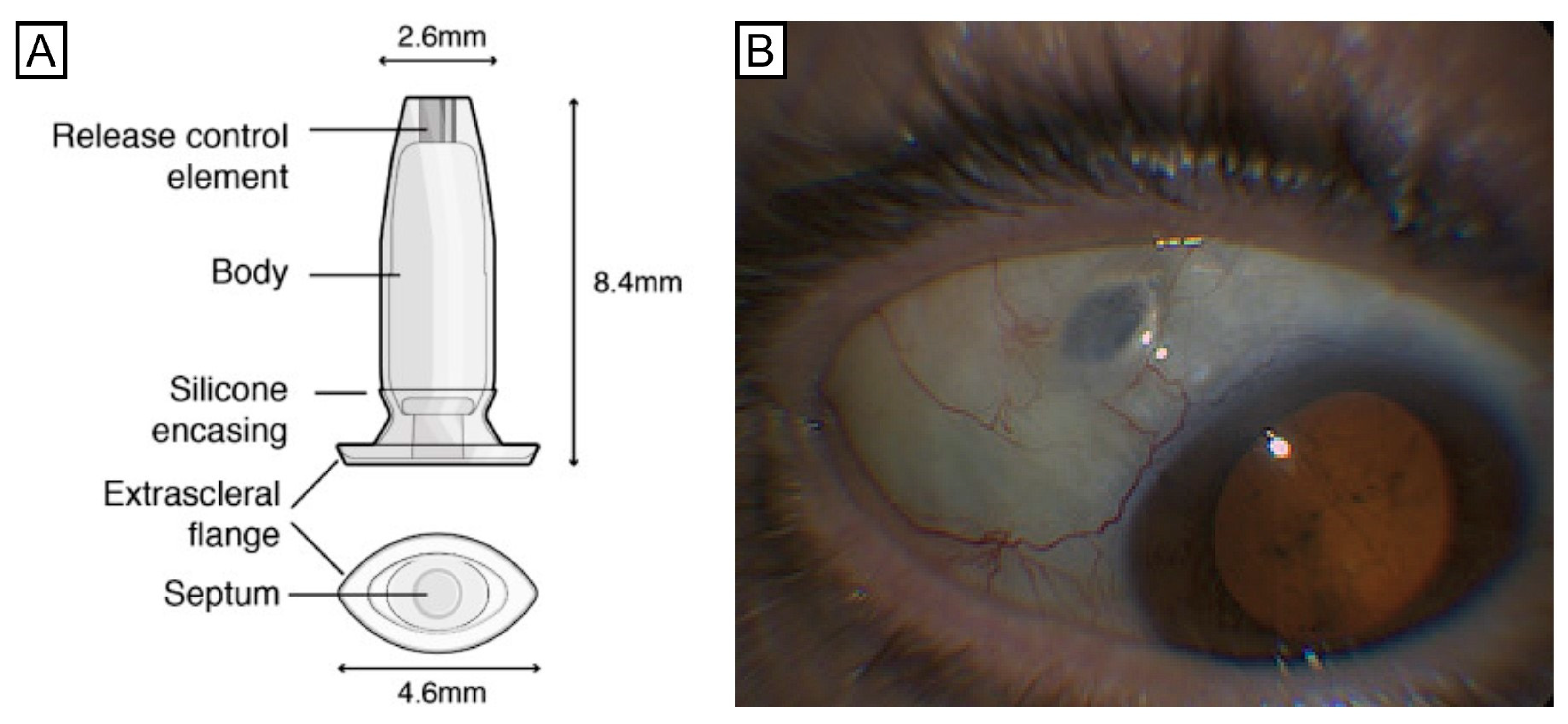
3. The Device
4. Surgical Technique
Refill–Exchange Technique
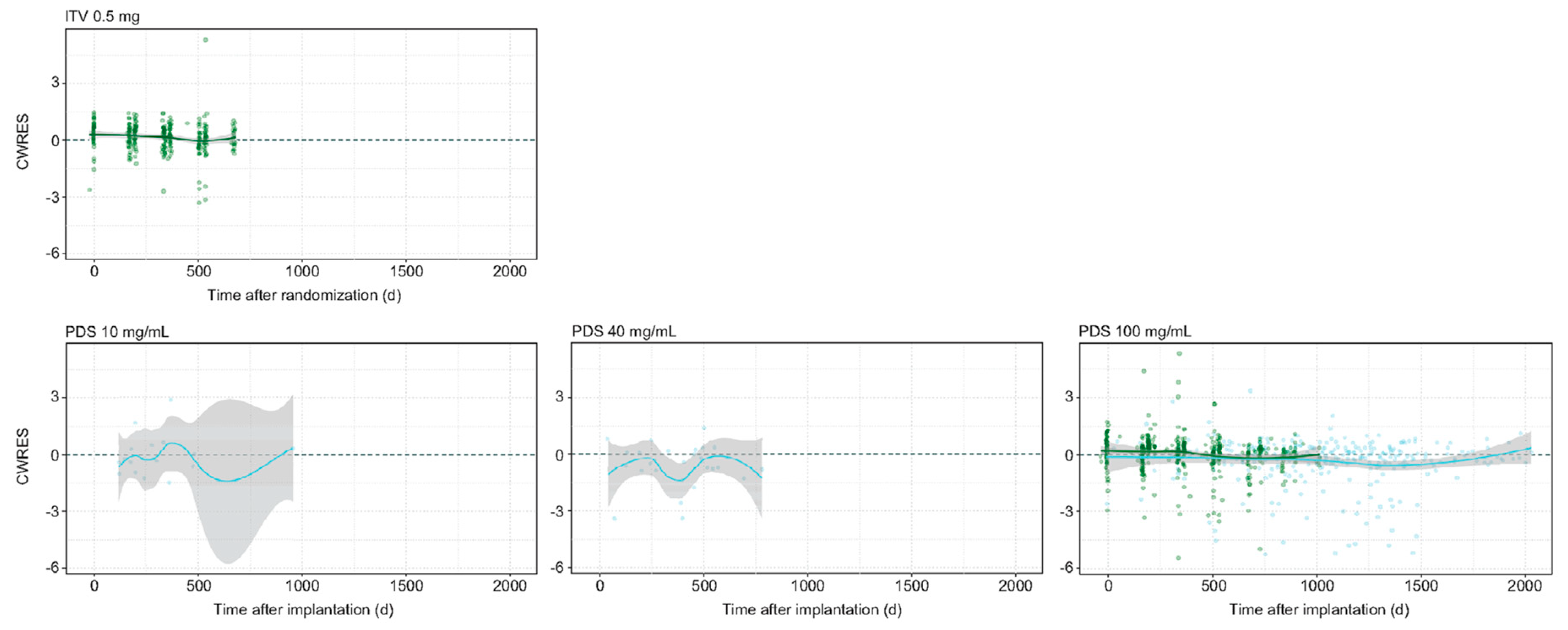
5. Pharmacokinetics
Biocompatibility
6. Clinical Results
6.1. The LADDER Trial
6.2. The ARCHWAY Trial
7. Adverse Events
8. Future Directions
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bourne, R.R.A.; Jonas, J.B.; Bron, A.M.; Cicinelli, M.V.; Das, A.; Flaxman, S.R.; Friedman, D.S.; Keeffe, J.E.; Kempen, J.H.; Leasher, J.; et al. Prevalence and causes of vision loss in high-income countries and in Eastern and Central Europe in 2015: Magnitude, temporal trends and projections. Br. J. Ophthalmol. 2018, 102, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Almony, A. Disease burden of neovascular age-related macular degeneration and diabetic macular edema. Am. J. Manag. Care 2023, 29, S75–S80. [Google Scholar] [CrossRef]
- Helotera, H.; Kaarniranta, K. A Linkage between Angiogenesis and Inflammation in Neovascular Age-Related Macular Degeneration. Cells 2022, 11, 3453. [Google Scholar] [CrossRef]
- Fauser, S.; Viebahn, U.; Muether, P.S. Intraocular and systemic inflammation-related cytokines during one year of ranibizumab treatment for neovascular age-related macular degeneration. Acta Ophthalmol. 2015, 93, 734–738. [Google Scholar] [CrossRef]
- Boyer, D.S.; Antoszyk, A.N.; Awh, C.C.; Bhisitkul, R.B.; Shapiro, H.; Acharya, N.R.; MARINA Study Group. Subgroup analysis of the MARINA study of ranibizumab in neovascular age-related macular degeneration. Ophthalmology 2007, 114, 246–252. [Google Scholar] [CrossRef]
- Brown, D.M.; Michels, M.; Kaiser, P.K.; Heier, J.S.; Sy, J.P.; Ianchulev, T. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Ophthalmology 2009, 116, 57–65.e5. [Google Scholar] [CrossRef]
- Busbee, B.G.; Ho, A.C.; Brown, D.M.; Heier, J.S.; Suñer, I.J.; Li, Z.; Rubio, R.G.; Lai, P.; HARBOR Study Group. Twelve-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology 2013, 120, 1046–1056. [Google Scholar] [CrossRef]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y.; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef]
- Comparison of Age-Related Macular Degeneration Treatments Trials (CATT) Research Group; Martin, D.F.; Maguire, M.G.; Fine, S.L.; Ying, G.S.; Jaffe, G.J.; Grunwald, J.E.; Toth, C.; Redford, M.; Ferris, F.L., 3rd. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: Two-year results. Ophthalmology 2012, 119, 1388–1398. [Google Scholar] [CrossRef]
- Souied, E.H.; Oubraham, H.; Mimoun, G.; Cohen, S.Y.; Quere, S.; Derveloy, A.; TWIN Study Group. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: The TWIN Study. Retina 2015, 35, 1743–1749. [Google Scholar] [CrossRef]
- Holz, F.G.; Tadayoni, R.; Beatty, S.; Berger, A.; Cereda, M.G.; Cortez, R.; Hoyng, C.B.; Hykin, P.; Staurenghi, G.; Heldner, S.; et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br. J. Ophthalmol. 2015, 99, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.Y.; Mimoun, G.; Oubraham, H.; Zourdani, A.; Malbrel, C.; Quere, S.; Schneider, V.; LUMIERE Study Group. Changes in visual acuity in patients with wet age-related macular degeneration treated with intravitreal ranibizumab in daily clinical practice: The LUMIERE study. Retina 2013, 33, 474–481. [Google Scholar] [CrossRef]
- Gohil, R.; Crosby-Nwaobi, R.; Forbes, A.; Burton, B.; Hykin, P.; Sivaprasad, S. Caregiver Burden in Patients Receiving Ranibizumab Therapy for Neovascular Age Related Macular Degeneration. PLoS ONE 2015, 10, e0129361. [Google Scholar] [CrossRef] [PubMed]
- Prenner, J.L.; Halperin, L.S.; Rycroft, C.; Hogue, S.; Williams Liu, Z.; Seibert, R. Disease Burden in the Treatment of Age-Related Macular Degeneration: Findings from a Time-and-Motion Study. Am. J. Ophthalmol. 2015, 160, 725–731.e1. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Marcus, D.M.; Awh, C.C.; Regillo, C.; Adamis, A.P.; Bantseev, V.; Chiang, Y.; Ehrlich, J.S.; Erickson, S.; Hanley, W.D.; et al. The Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration: Results from the Randomized Phase 2 Ladder Clinical Trial. Ophthalmology 2019, 126, 1141–1154. [Google Scholar] [CrossRef] [PubMed]
- Holekamp, N.M.; Campochiaro, P.A.; Chang, M.A.; Miller, D.; Pieramici, D.; Adamis, A.P.; Brittain, C.; Evans, E.; Kaufman, D.; Maass, K.F.; et al. Archway Randomized Phase 3 Trial of the Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2022, 129, 295–307. [Google Scholar] [CrossRef] [PubMed]
- Eichenbaum, D.A.; Ahmed, A.; Hiya, F. Ranibizumab port delivery system: A clinical perspective. BMJ Open Ophthalmol. 2022, 7, e001104. [Google Scholar] [CrossRef] [PubMed]
- Khanani, A.M.; Graff, J.M.; Marcus, D.M.; Wykoff, C.C.; Jhaveri, C.D.; Barteselli, G.; Malhotra, V.K.; Menezes, A.R.; Callaway, N.F. Refill-Exchange Procedure of the Port Delivery System with Ranibizumab: Overview and Clinical Trial Experience. Ophthalmic Surg. Lasers Imaging Retin. 2022, 53, 257–265. [Google Scholar] [CrossRef]
- Adamis, A.P.; de Juan, E., Jr. Development of the Port Delivery System with ranibizumab for neovascular age-related macular degeneration. Curr. Opin. Ophthalmol. 2022, 33, 131–136. [Google Scholar] [CrossRef]
- Pieramici, D.J.; Wieland, M.R.; Stewart, J.M.; Chang, R.T.; Gune, S.A.; Malhotra, V.K.; Barteselli, G.; Awh, C.C. Implant Insertion Procedure of the Port Delivery System With Ranibizumab: Overview and Clinical Pearls. Ophthalmic Surg. Lasers Imaging Retin. 2022, 53, 249–256. [Google Scholar] [CrossRef]
- Ericksen, C.J.; Christensen, C.A.; Berger, B.; Gune, S.; Nielsen, J.S. Implantation Site of a Port Delivery System with Ranibizumab: Anterior Segment Optical Coherence Tomography Evaluation. J. Vitreoretin. Dis. 2022, 6, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Timmons, K.; Heckmann, L.C.; Ren, Y.; Gunderson, I.; Makkouk, F.; Berger, B.B. Ranibizumab Injection (Susvimo) Implant Septum Dislodgement in a Patient with Neovascular Age-Related Macular Degeneration. JAMA Ophthalmol. 2022, 140, 832. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Lu, T.; Tuomi, L.; Jumbe, N.; Lu, J.; Eppler, S.; Kuebler, P.; Damico-Beyer, L.A.; Joshi, A. Pharmacokinetics of ranibizumab in patients with neovascular age-related macular degeneration: A population approach. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Ritschel, W.A. Handbook of Basic Pharmacokinetics; Drug Intelligence Publications: Hamilton, IL, USA, 1980. [Google Scholar]
- Yohe, S.; Maass, K.F.; Horvath, J.; Rea, J.; Barteselli, G.; Ranade, S.V. In-vitro characterization of ranibizumab release from the Port Delivery System. J. Control. Release 2022, 345, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Wykoff, C.C.; Campochiaro, P.A.; Pieramici, D.J.; Khanani, A.M.; Gune, S.; Maia, M.; Kagedal, M.; Ding, H.T.; Maass, K.F. Pharmacokinetics of the Port Delivery System with Ranibizumab in the Ladder Phase 2 Trial for Neovascular Age-Related Macular Degeneration. Ophthalmol. Ther. 2022, 11, 1705–1717. [Google Scholar] [CrossRef]
- Kagedal, M.; Alskar, O.; Petersson, K.; Hanze, E.; Maia, M.; Lu, T.; Vakhavkar, S.; Quartino, A.; Willis, J.R.; Jin, J.Y.; et al. Population Pharmacokinetics of Ranibizumab Delivered via the Port Delivery System Implanted in the Eye in Patients with Neovascular Age-Related Macular Degeneration. J. Clin. Pharmacol. 2023, 63, 1210–1220. [Google Scholar] [CrossRef]
- Ciulla, T.A.; Hussain, R.M.; Pollack, J.S.; Williams, D.F. Visual Acuity Outcomes and Anti-Vascular Endothelial Growth Factor Therapy Intensity in Neovascular Age-Related Macular Degeneration Patients: A Real-World Analysis of 49 485 Eyes. Ophthalmol. Retina 2020, 4, 19–30. [Google Scholar] [CrossRef]
- Kim, L.N.; Mehta, H.; Barthelmes, D.; Nguyen, V.; Gillies, M.C. Metaanalysis of Real-World Outcomes of Intravitreal Ranibizumab for the Treatment of Neovascular Age-Related Macular Degeneration. Retina 2016, 36, 1418–1431. [Google Scholar] [CrossRef]
- Le, K.N.; Gibiansky, L.; van Lookeren Campagne, M.; Good, J.; Davancaze, T.; Loyet, K.M.; Morimoto, A.; Strauss, E.C.; Jin, J.Y. Population Pharmacokinetics and Pharmacodynamics of Lampalizumab Administered Intravitreally to Patients with Geographic Atrophy. CPT Pharmacomet. Syst. Pharmacol. 2015, 4, 595–604. [Google Scholar] [CrossRef]
- Crowell, S.R.; Wang, K.; Famili, A.; Shatz, W.; Loyet, K.M.; Chang, V.; Liu, Y.; Prabhu, S.; Kamath, A.V.; Kelley, R.F. Influence of Charge, Hydrophobicity, and Size on Vitreous Pharmacokinetics of Large Molecules. Transl. Vis. Sci. Technol. 2019, 8, 1. [Google Scholar] [CrossRef]
- Zhang, Y.; Yao, Z.; Kaila, N.; Kuebler, P.; Visich, J.; Maia, M.; Tuomi, L.; Ehrlich, J.S.; Rubio, R.G.; Campochiaro, P.A. Pharmacokinetics of ranibizumab after intravitreal administration in patients with retinal vein occlusion or diabetic macular edema. Ophthalmology 2014, 121, 2237–2246. [Google Scholar] [CrossRef]
- Krohne, T.U.; Liu, Z.; Holz, F.G.; Meyer, C.H. Intraocular pharmacokinetics of ranibizumab following a single intravitreal injection in humans. Am. J. Ophthalmol. 2012, 154, 682–686.e2. [Google Scholar] [CrossRef]
- Bantseev, V.; Horvath, J.; Barteselli, G.; Ranade, S.; Maia, M.; Yadav, D.B.; Schuetz, C.; Shelton, A.; Booler, H.S. Nonclinical Toxicology and Biocompatibility Program Supporting Clinical Development and Registration of the Port Delivery System With Ranibizumab for Neovascular Age-Related Macular Degeneration. Toxicol. Pathol. 2021, 49, 663–672. [Google Scholar] [CrossRef]
- Genentech, I. Study of the Efficacy and Safety of the Ranibizumab Port Delivery System for Sustained Delivery of Ranibizumab in Patients with Subfoveal Neovascular Age-Related Macular Degeneration; ClinicalTrials. gov: NCT02510794. Available online: https://www.clinicaltrials.gov/study/NCT02510794?cond=NCT02510794&rank=1 (accessed on 20 January 2024).
- Khanani, A.M.; Callanan, D.; Dreyer, R.; Chen, S.; Howard, J.G.; Hopkins, J.J.; Lin, C.Y.; Lorenz-Candlin, M.; Makadia, S.; Patel, S.; et al. End-of-Study Results for the Ladder Phase 2 Trial of the Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration. Ophthalmol. Retina 2021, 5, 775–787. [Google Scholar] [CrossRef]
- Jaffe, G.J.; Cameron, B.; Kardatzke, D.; Ives, J.; Barteselli, G.; Gune, S. Prevalence and Progression of Macular Atrophy in Eyes with Neovascular Age-Related Macular Degeneration in the Phase 2 Ladder Trial of the Port Delivery System with Ranibizumab. Ophthalmol. Retina 2022, 6, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Roche, H. A Phase III Study to Evaluate the Port Delivery System with Ranibizumab Compared with Monthly Ranibizumab Injections in Participants with Wet Age-Related Macular Degeneration. ClinicalTrials. gov: NCT03677934. Available online: https://www.clinicaltrials.gov/study/NCT03677934?cond=NCT03677934&rank=1 (accessed on 20 January 2024).
- Regillo, C.; Berger, B.; Brooks, L.; Clark, W.L.; Mittra, R.; Wykoff, C.C.; Callaway, N.F.; DeGraaf, S.; Ding, H.T.; Fung, A.E.; et al. Archway Phase 3 Trial of the Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration 2-Year Results. Ophthalmology 2023, 130, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Awh, C.C.; Barteselli, G.; Makadia, S.; Chang, R.T.; Stewart, J.M.; Wieland, M.R.; Brassard, R.; Callaway, N.F.; Gune, S.; Heatherton, P.; et al. Management of Key Ocular Adverse Events in Patients Implanted with the Port Delivery System with Ranibizumab. Ophthalmol. Retina 2022, 6, 1028–1043. [Google Scholar] [CrossRef] [PubMed]
- Pieramici, D.J.; Heimann, F.; Brassard, R.; Barteselli, G.; Ranade, S. Virtual Reality Becomes a Reality for Ophthalmologic Surgical Clinical Trials. Transl. Vis. Sci. Technol. 2020, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Roche, H. This Study Will Evaluate the Efficacy, Safety, and Pharmacokinetics of the Port Delivery System with Ranibizumab in Participants with Diabetic Macular Edema Compared with Intravitreal Ranibizumab. ClinicalTrials. gov: NCT04108156. Available online: https://www.clinicaltrials.gov/study/NCT04108156?cond=NCT04108156&rank=1 (accessed on 20 January 2024).
- Roche, H. A Multicenter, Randomized Study in Participants with Diabetic Retinopathy without Center-Involved Diabetic Macular Edema to Evaluate the Efficacy, Safety, and Pharmacokinetics of Ranibizumab Delivered via the Port Delivery System Relative to the Comparator Arm. ClinicalTrials. gov: NCT04503551. Available online: https://www.clinicaltrials.gov/study/NCT04503551?cond=NCT04503551&rank=1 (accessed on 20 January 2024).
- Roche, H. A Study of the Efficacy, Safety, and Pharmacokinetics of a 36-Week Refill Regimen for the Port Delivery System with Ranibizumab in Patients with Neovascular Age-Related Macular Degeneration (Velodrome). ClinicalTrials. gov: NCT04657289. Available online: https://www.clinicaltrials.gov/study/NCT04657289?cond=NCT04657289&rank=1 (accessed on 20 January 2024).
- Roche, H. Extension Study for the Port Delivery System with Ranibizumab (Portal). ClinicalTrials. gov: NCT03683251. Available online: https://www.clinicaltrials.gov/study/NCT03683251?cond=NCT03683251&rank=1 (accessed on 20 January 2024).
- Genentech, I. A Study Assessing Corneal Endothelial Cells in Patients With Neovascular Age-related Macular Degeneration Treated with the Port Delivery System with Ranibizumab (PDS) (Belvedere). ClinicalTrials. gov: NCT04853251. Available online: https://www.clinicaltrials.gov/study/NCT04853251?cond=NCT04853251&rank=1 (accessed on 20 January 2024).
- Roche, H. A Real-World Study to Gain Clinical Insights into Roche ophthalmology Products. ClinicalTrials. gov: NCT05476926. Available online: https://www.clinicaltrials.gov/study/NCT05476926?cond=NCT05476926&rank=1 (accessed on 20 January 2024).
- Roche, H. A Study of the Effectiveness and Safety of a 36-Week Refill Regimen for the Port Delivery System with Ranibizumab vs Aflibercept Treat and Extend in Subjects with Neovascular Age-Related Macular Degeneration. ClinicalTrials. gov: NCT05126966. Available online: https://www.clinicaltrials.gov/study/NCT05126966?cond=NCT05126966&rank=1 (accessed on 20 January 2024).
- Roche, H. A Study of the Efficacy, Safety, and Pharmacokinetics of the Port Delivery System with Ranibizumab in Chinese Patients with Neovascular Age-Related Macular Degeneration. ClinicalTrials. gov: NCT05562947. Available online: https://www.clinicaltrials.gov/study/NCT05562947?cond=NCT05562947&rank=1 (accessed on 20 January 2024).



{kind=link}
{kind=link}
| Phase 2 LADDER Trial | Phase 3 ARCHWAY Trial | |
|---|---|---|
| Start/end | 2015/2019 | 2018/2021 |
| Participants | Overall, n = 220 PDS, n = 179
| 418 randomized and 415 treated PDS, n = 248 IVI, n = 167 |
| Intervention | PDS with RBZ (10, 40, or 100 mg/mL) | PDS with RBZ (100 mg/mL) refilled Q24W |
| Control group | Monthly IVI of 0.5 mg RBZ | Monthly IVIs of 0.5 mg RBZ |
| Follow-up period | 22 months | 36–40 weeks, then extended to 88–92 weeks |
| Primary findings | Median time to first refill
| Mean change in ETDRS from baseline
|
| Secondary findings | ||
| BCVA | Mean change in ETDRS from baseline
| Mean change in ETDRS from baseline to weeks 44 and 48
|
| OCT | Mean change in CFT from baseline
| Mean change in CFT from baseline at week 96
|
| Trial | Start/End | Sponsor | Current Status | Condition | Participants | Study Type |
|---|---|---|---|---|---|---|
| PAGODA | 2019/2024 | Hoffmann La-Roche a | Recruitment ended | DME | 634 (actual) | Interventional |
| PAVILION | 2020/2024 | Hoffmann La-Roche a | Recruitment ended | DME | 174 (actual) | Interventional |
| VELODROME | 2021/2026 | Hoffmann La-Roche a | Recruiting | nAMD | 442 (estimate) | Interventional |
| PORTAL | 2018/2026 | Hoffmann La-Roche a | Recruiting | nAMD | 1000 (estimate) | Interventional |
| BELVEDERE | 2021/2027 | Genentech, Inc. | Recruiting | nAMD | 185 (estimate) | Interventional |
| VOYAGER | 2022/2027 | Hoffmann La-Roche a | Recruiting | nAMD | 5000 (estimate) | Observational |
| DIAGRID | 2023/2026 | Hoffmann La-Roche a | Suspended | nAMD | 0 (actual) | Interventional |
| Chinese | 2024/2029 | Hoffmann La-Roche a | Not yet recruiting | nAMD | 68 (estimate) | Interventional |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlà, M.M.; Savastano, M.C.; Boselli, F.; Giannuzzi, F.; Rizzo, S. Ranibizumab Port Delivery System in Neovascular Age-Related Macular Degeneration: Where Do We Stand? Overview of Pharmacokinetics, Clinical Results, and Future Directions. Pharmaceutics 2024, 16, 314. https://doi.org/10.3390/pharmaceutics16030314
Carlà MM, Savastano MC, Boselli F, Giannuzzi F, Rizzo S. Ranibizumab Port Delivery System in Neovascular Age-Related Macular Degeneration: Where Do We Stand? Overview of Pharmacokinetics, Clinical Results, and Future Directions. Pharmaceutics. 2024; 16(3):314. https://doi.org/10.3390/pharmaceutics16030314
Chicago/Turabian StyleCarlà, Matteo Mario, Maria Cristina Savastano, Francesco Boselli, Federico Giannuzzi, and Stanislao Rizzo. 2024. "Ranibizumab Port Delivery System in Neovascular Age-Related Macular Degeneration: Where Do We Stand? Overview of Pharmacokinetics, Clinical Results, and Future Directions" Pharmaceutics 16, no. 3: 314. https://doi.org/10.3390/pharmaceutics16030314