1. Introduction
In vitro drug release tests (IVRTs) are one of the most important tools for drug development and the evaluation of semisolid dosage forms’ performance. The development of the drug release test as an analytical method poses a significant challenge for analysts. The new version of the ICH (International Council for Harmonisation) guidelines were adopted on 14 December 2023; ICH Q14 on analytical procedure development (Step 5) and the ICH Q2(R2) on the validation of analytical procedures (Step 5) are particularly relevant to our study. Together, the new ICH Q14 and the revised ICH Q2(R2) documents outline the proposed analytical development procedure and its validation for the analytical life cycle management approach. “The goal of development is to obtain an analytical procedure fit for its intended purpose: to measure an attribute or attributes of the analyzed material with the needed specificity/selectivity, accuracy and/or precision over the reportable range” [
1]. In the new ICH Q14 analytical procedure development guidelines, two types of approaches are discussed: minimal (traditional) and enhanced. The result of the traditional trial-and-error approach is that the quality of the product is ensured by final product testing, which is confirmed by one-time validation. In contrast, the enhanced approach integrates elements of Quality by Design (QbD) and describes a science- and risk assessment-based analytical development procedure to ensure that the product fit for its intended use. The three stages of the analytical procedure life cycle are procedure design, procedure performance qualification, and continued procedure performance verification. The first stage of the analytical procedure life cycle includes knowledge gathering, establishing the ATP, understanding the effects of various process parameters on procedure performance, optimizing them, and defining the initial control strategy. An important element of the improved approach is the ATP, which outlines the intended purpose of the method development. It summarizes the expected performance characteristics, including the allowable error for the measurement, along with associated performance criteria for the analytical procedure. The ATP is independent of any specific analytical procedure; therefore, after defining the ATP, the analyst should choose the analytical technique(s) [
1,
2,
3,
4].
The Static Vertical Franz-type diffusion cell, USP Apparatus II with immersion cell, and USP Apparatus IV with semisolid adapter (SSA) are well-known apparatuses for in vitro performance testing of semisolid drug products, as described in USP Chapter 1724 [
5]. However, the flow-through diffusion cell (FTDC) is not included in this chapter. Bronaugh and Stewart developed and described the flow-through diffusion cell apparatus in 1985 for percutaneous absorption studies [
6]. In terms of application, the flow-through diffusion cell is not as widespread as the static Franz cell. This can be explained by various studies that aimed to compare static and flow-through diffusion cells, revealing similar absorption profiles and quantitative values for the different activities in both types of cells [
6,
7,
8]. One advantage of using a flow-through diffusion cell is its ability to model the dynamics of blood flow, and maintaining sink conditions is more easily achieved [
7,
8]. Although, a drawback of the measurement is the challenge of ensuring the leak-free assembly of the device and preventing air being trapped between the membrane and the medium [
7].
This study focuses on defining the ATP for practical use and facilitating the selection of IVRT technology for topical hydrogels and creams containing diclofenac sodium (which are used as model products). This involves implementing the ICH Q14 draft guidelines [
1] and USP (United States Pharmacopeia) Chapter 1220 [
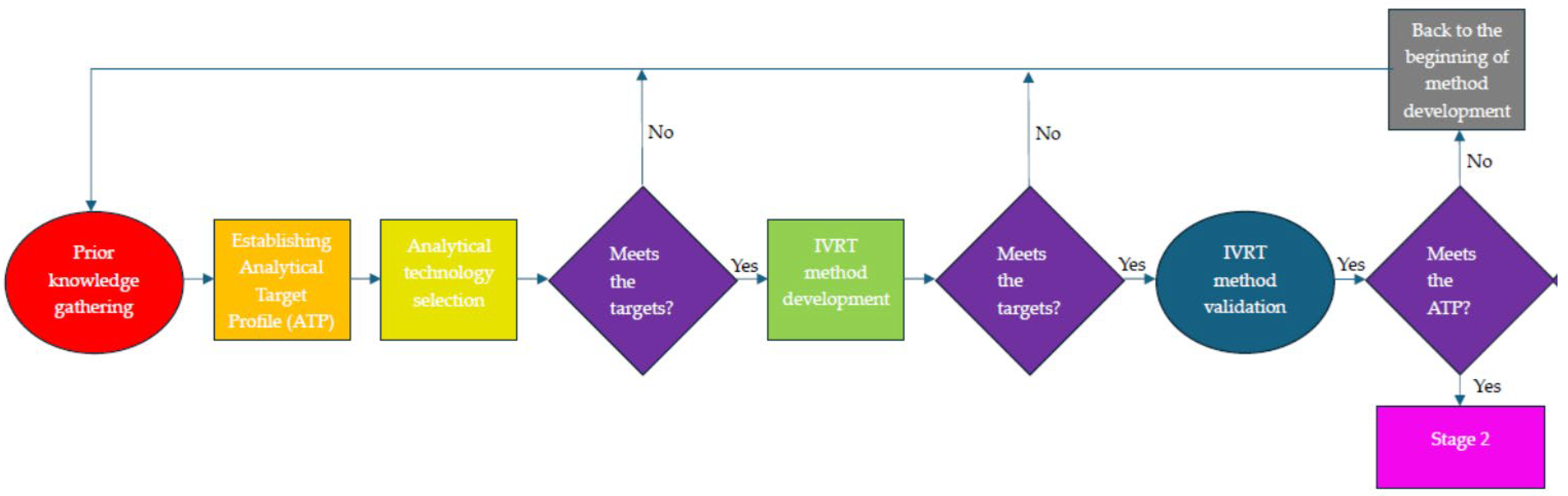
3]. In this article, we aim to compare four IVRT apparatuses (USP Apparatus II with immersion cell, USP Apparatus IV with semisolid adapter, static vertical diffusion cell, and a new, in-house-developed flow-through diffusion cell) with the assistance of the ATP, and to select a proper IVRT apparatus and method for further measurements using a minimum set of investigations. After selecting the considered apparatus for IVRT, the analytical method development phase can begin, followed by validation of the method (
Figure 1). However, this is not within the scope of this article.
4. Discussion
The planning of in vitro drug release studies and the selection of the appropriate apparatus and method are crucial for characterizing pharmaceutical formulations. The study of drug release from a topical semisolid formulation serves as a clear indicator of the formulation’s performance. The developed IVRT method should be sufficiently robust, providing a well-reproducible measurement. Additionally, the developed IVRT method should be capable of detecting microstructural variations in the formulation.
Currently, several accepted apparatuses are available, including the Static Vertical Franz-type diffusion cell, USP Apparatus II with immersion cell, and USP Apparatus IV with semisolid adapter (SSA), which are official pharmacopeial apparatuses for performing IVRT measurements on semisolid formulations [
5]. In contrast, the flow-through diffusion cell (FTDC) is a new apparatus developed in our laboratory. Its arrangement is similar to the Static Vertical Diffusion cell (Hanson), meaning that it is positioned towards the upper part of the cell and separated from the receptor phase by a membrane. However, unlike the Franz cell, the donor cell is open at the top. Another notable difference lies in the arrangement of the receptor phase: beneath the membrane, the medium circulates in a spiral path within the receptor cell, maintaining contact with the membrane throughout the spiral movement. This medium is continuously flowing, differing from the static medium in the Franz cell between samplings. FTDC holds an advantage over the static cell in that it allows continuous sampling and, with the continuous exchange of the receptor phase, effectively models blood flow in the skin. Additionally, maintaining the “sink condition” is easier with FTDC.
In our present work, we compared two static and two flow-through apparatuses, incorporating both open- and closed-cell configurations. This approach covered the most prevalent pharmacopeial apparatuses, along with a potential new arrangement type. The microstructure of semisolid formulations can pose a considerable challenge for reproduction. Furthermore, the employed apparatuses exhibit several unfavorable characteristics that complicate the reproducibility or evaluation of the IVRT method. All four apparatuses presented utilize membranes, and both the type and fitting of the membranes in the applied cells pose a potential source of error. Our exploration of membrane types in our testing systems is detailed in a prior article [
10], and as such, we do not delve into it in the current publication.
Another significant drawback of the apparatuses used in studying the release of semisolid active ingredients pertains to the filling of the donor cell, which must accommodate the semisolid formulation. This process involves ensuring a leak-free assembly, achieving a perfect fit between the formulation, membrane, and receptor phase, and ensuring the absence of air bubbles. Moreover, it is paramount to take a note of distortions that may arise from the dead space within automatic samplers. Taking all these factors into account, developing a well-reproducible IVRT method for semisolid formulations proves challenging, as has been described in several instances in the international literature.
In the study by Liebenberg et al., it was found that the release rates of hydrocortisone, salicylic acid, ascorbic acid, and triclosan from creams and gels were slower when measured with the flow-through cells compared to measurements with the Franz cell and immersion cells [
17]. Tanja Ilić et al. came to the same results, finding total agreement between the results obtained with the Franz cell and immersion cells [
18]. Similarly, in our study, the investigations suggested that the IVRRs of a cream which contains diclofenac sodium (µg × cm
−2 × min
−0.5) were the lowest when measured with FTDC and USP IV (with SSA). Those measured by USP II (with immersion cell) and Franz cell were consistent, and they were 1.3 times higher than those measured with FTDC. The ranking of the IVRR (µg × cm
−2 × min
−0.5) for our creams was: USP IV, SSA ≈ FTDC < USP II, immersion cell ≈ Franz cell.
Sanghvi and Collins compared the cumulative release rates of an enhancer (immersion cell) and Franz cell measured with hydrocortisone 1% ointment. It was found that the cumulative release using a cellulose membrane was more than threefold higher with the enhancer cell (immersion cell) compared to that seen with the Franz cell [
19]. In contrast, in our study, concerning a cream which contains diclofenac sodium, the IVRR measured with USP II (immersion cell) and Franz cell was the same.
Bao et al. compared the reproducibility and discrimination ability of three apparatus types (USP Apparatus IV with semisolid adapters, USP Apparatus 2 with enhancer cells, and Franz diffusion cells) using ophthalmic ointment preparations The coefficient of variation (CV%) of the drug release rate indicated no significant differences among the three methods, and our results also confirmed this [
20].
In terms of the diclofenac sodium hydrogel, the IVRR (µg × cm
−2 × min
−0.5) measured by USP IV (with SSA) was the highest, while those measured by USP II (with immersion cell) and the Franz cell were the same. The rank order of diclofenac sodium’s IVRR (µg × cm
−2 × min
−0.5) from the hydrogel is: USP II, immersion cell ≈ Franz cell < FTDC <USP IV, SSA. Clowes et al., investigated the absorption of water and mannitol through human, pig, and rat epidermises measured with static diffusion cell and flow-through diffusion cell. Contrary to our results, their findings showed that flow-through diffusion cells and static diffusion cells were similar in their ability to measure the percutaneous absorption of water-soluble penetrants [
7]. M.J. Lucero et al. used Franz cells and enhancer cells to investigate the controlled drug release of theophylline from a three-dimensional gel structure. They concluded that the Enhancer Cell apparatus provided more reliable and reproducible results than the Franz diffusion cell due to better monitoring and control of different variables. We also concur with this observation [
21]. The rank of the IVRRs (µg × cm
−2 × min
−0.5) of our hydrogels was: USP II, immersion cell ≈ Franz cell < FTDC < USP IV, SSA. The present work aimed to establish an ATP for the IVRT quality control test for a diclofenac sodium cream and hydrogel based on the new ICHQ14 draft guidelines [
1] and USP Chapter 1220 [
3]. Following the definition of the ATP, which was informed by the In Vitro Release Test Studies for Topical Drug Products Submitted in ANDAs draft guidance [
13], draft guidelines on quality and equivalence of topical products [
14], and ICH Q2(R1) Validation of Analytical Procedures: Text and Methodology guidelines [
15], our next step was the initial selection of technology for the development of the IVRT method. We could choose from four different IVRT apparatuses (FTDC, USP II with immersion cell, USP IV with 0.4 mL SSA, and static vertical diffusion cell). The HPLC method used for measuring IVRT samples was determined based on its compatibility with the matrix components, avoiding interference.
Two very common semisolid topical forms were examined in our study: o/w cream and hydrogel. In both formulations, the active ingredient was present in a dissolved state. The components of the formulated ATP assist in the selection of an appropriate IVRT method for the specific formulation. Our findings clearly indicate that each drug form exhibits distinct precision characteristics among the four apparatuses, and even within the same device, the precision may vary between the two drug forms. In terms of the precision of both of the semisolid systems, the USP IV, SSA apparatus proved to be the most favorable, while the FTDC was the least favorable. For the latter apparatus, the precision of the cream system exceeded the limit specified in the ATP (
Table 5), making it unsuitable as a reproducible measurement method for creams. However, for the hydrogel form, the precision was significantly improved with this apparatus. This substantial difference is likely explained by the formation of a poorly reproducible formulation–membrane–receptor interface, which is dependent on the formulation type, especially for a donor phase which is in the open position at the top.
The appropriate selection of the duration of the IVRT method is important for several reasons. It is necessary to specify a test duration that is sufficiently long to adequately characterize the kinetics of drug diffusion, while also preventing degradation processes that could negatively impact the drug or the carrier system, leading to the potential misinterpretation of results. In accordance with the EMA draft guidelines, it is recommended that, at the last measurement point, a minimum of 70% of the drug should have diffused, and the ascending linear phase should include at least six measurement points. The 70% drug release was achieved in the hydrogel forms for all apparatuses, but in the cream forms, it notably fell short of this value. Interestingly, both the Franz cell and FTDC exhibited considerably higher values at the last measurement point compared to the other two cells, even though they had a smaller receptor volume. It is worth noting that, in the case of the FTDC, the sink conditions could not be met at the starting point and were only met during dynamic flow. A possible explanation for this phenomenon with these two cell types is the dynamics of receptor phase exchange. With the FTDC, the receptor medium continuously flows beneath the membrane, facilitating the renewal of the membrane–receptor phase interface. In the context of the Franz cell, although the cell remains static during sampling, a volume greater than the actual sample is exchanged in the cell’s receptor medium. This exchange occurs as part of the cleaning of the automatic sampling system’s tubing, leading to the renewal of the receptor surface under the membrane. This interface renewal may be exploited for more structured, slower drug release systems, achieving satisfactory results within a relatively shorter test duration.
The accuracy of the method is also a critical parameter, and, for this purpose, we specified a specification limit between 90–110% in our ATP table. Since FTDC was no longer suitable in terms of precision, we only performed this test for the remaining three apparatuses using drug-free blank formulations. All three apparatuses met the criterion, showing no deviation between the cream and hydrogel systems. However, regarding the Franz cell, we observed a more significant, but still within the limit, decrease. This decrease may be attributed to the systematic error of the mentioned apparatus or the back diffusion of the receptor medium towards the donor chamber during sampling.
The robustness regarding pH was evaluated on three apparatuses (USP II, IV, and Franz cell), while the flow rate was characterized by the flow rate within two apparatuses (USP IV, SSA, and FTDC). In terms of pH robustness, significant differences were clearly observed, particularly for the cream systems, with the USP IV, SSA apparatus showing a deviation beyond the limit. The cause of this is not currently identifiable from the measurement data and device types; further measurements are needed to clarify this in the future.
The flow rate robustness for FTDC in cream systems cannot be justified; presumably, for this apparatus type, since the sink condition cannot be ensured with the chosen medium in the initial state, the drug release rate depends on the flow rate. Meanwhile, in the system where the sink condition is fulfilled (USP IV, SSA), the flow rate is less influenced, and the chosen range of 2 to 4 mL/min is robust for the measurements.
As a final conclusion, the results of the preliminary IVRT experiments of the cream which contains diclofenac sodium showed that the release of the diclofenac sodium from the cream matrix was slow, as measured by all four IVRT apparatuses, and the Qfinal ≥ 70% criterion described in the ATP was not met. Therefore, the IVRT measurement should be at least 12 h long. Based on our results, the USP II with immersion cell apparatus will be the best choice to develop an analytical IVRT method for diclofenac sodium cream, and the USP II with immersion cell apparatus and/or USP IV with SSA is best for diclofenac sodium hydrogel.









{kind=link}
{kind=link}
{kind=link}