
The Effect of Adjunctive Use of Hyaluronic Acid on Prevalence of Porphyromonas gingivalis in Subgingival Biofilm in Patients with Chronic Periodontitis: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Development and Registration
2.2. Review Question
2.3. Eligibility Criteria
2.4. Search Strategy and Data Sources
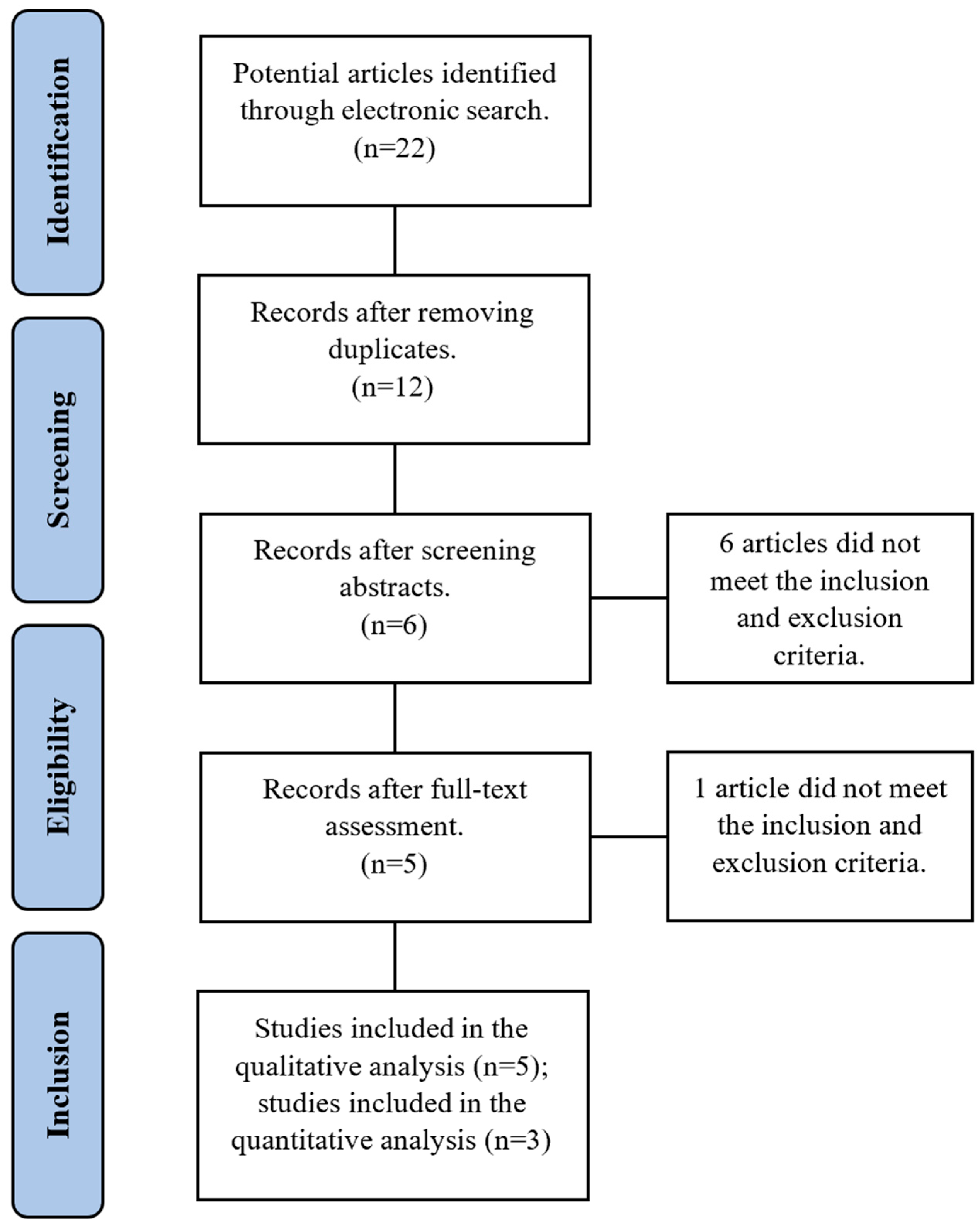
2.5. Study Selection
2.6. Risk of Bias Assessment
2.7. Data Synthesis
3. Results
3.1. Study Selection and Description
3.1.1. Engström et al., 2001 [37]
3.1.2. Xu et al., 2004 [38]
3.1.3. Eick et al., 2013 [39]
3.1.4. Nguyen et al., 2021 [40]
3.1.5. Vajawat et al., 2022 [41]
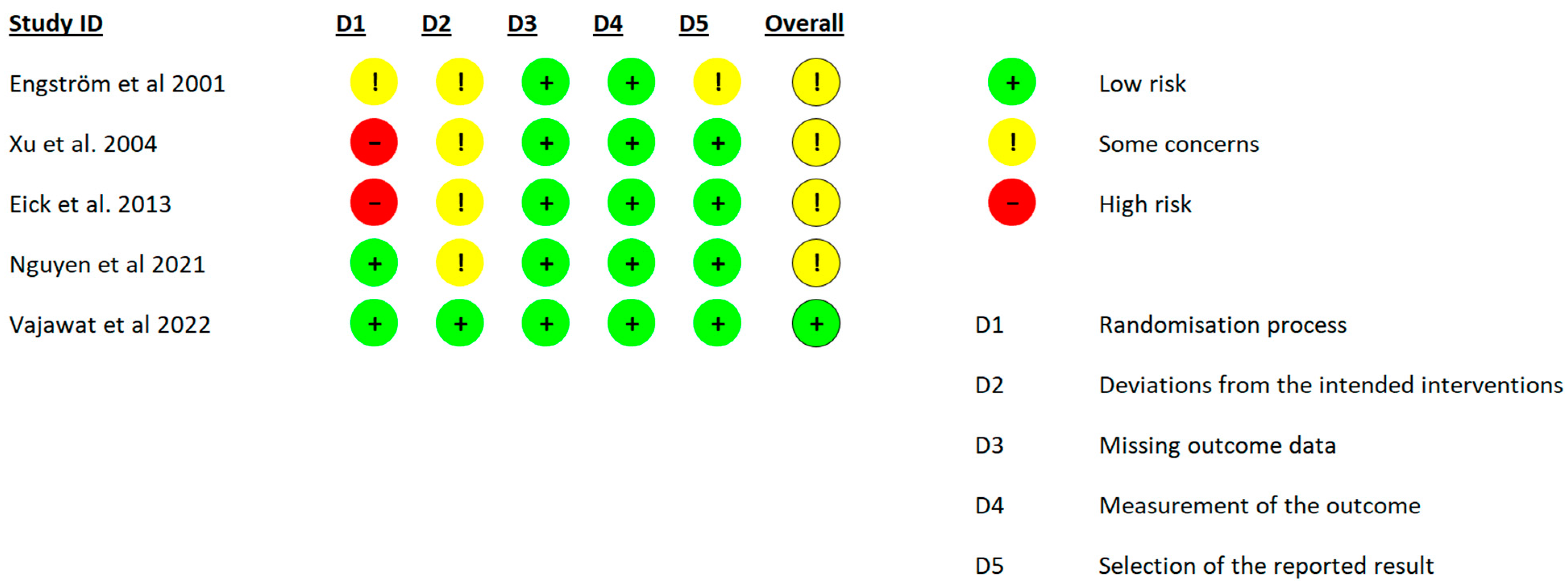
3.2. Risk of Bias
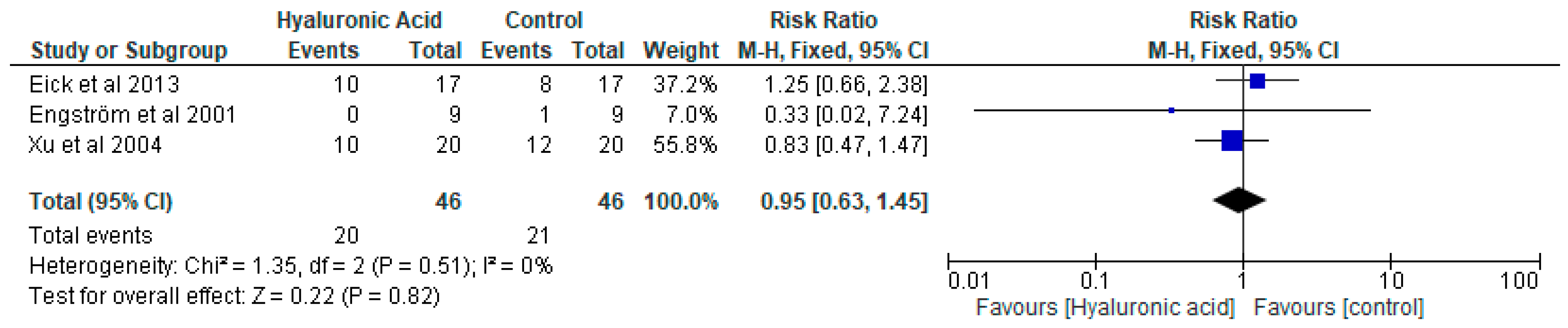
3.3. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Curtis, M.A.; Diaz, P.I.; Van Dyke, T.E. The role of the microbiota in periodontal disease. Periodontol. 2020 2020, 83, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Rosier, B.T.; De Jager, M.; Zaura, E.; Krom, B.P. Historical and contemporary hypotheses on the development of oral diseases: Are we there yet? Front. Cell. Infect. Microbiol. 2014, 4, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kornman, K.S. Mapping the pathogenesis of periodontitis: A new look. J. Periodontol. 2008, 79, 1560–1568. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Darveau, R.P.; Curtis, M.A. The keystone-pathogen hypothesis. Nat. Rev. Microbiol. 2012, 10, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Liang, S.; Payne, M.A.; Hashim, A.; Jotwani, R.; Eskan, M.A.; McIntosh, M.L.; Alsam, A.; Kirkwood, K.L.; Lambris, J.D.; et al. Low-abundance biofilm species orchestrates inflammatory periodontal disease through the commensal microbiota and complement. Cell Host Microbe 2011, 10, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Frias-Lopez, J.; Duran-Pinedo, A. Effect of periodontal pathogens on the metatranscriptome of a healthy multispecies biofilm model. J. Bacteriol. 2012, 194, 2082–2095. [Google Scholar] [CrossRef] [Green Version]
- How, K.Y.; Song, K.P.; Chan, K.G. Porphyromonas gingivalis: An Overview of Periodontopathic Pathogen below the Gum Line. Front. Microbiol. 2016, 7, 53. [Google Scholar] [CrossRef] [Green Version]
- Laine, M.L.; Appelmelk, B.J.; van Winkelhoff, A.J. Prevalence and distribution of six capsular serotypes of Porphyromonas gingivalis in periodontitis patients. J. Dent. Res. 1997, 76, 1840–1844. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S1–S8. [Google Scholar] [CrossRef]
- Herrera, D.; Matesanz, P.; Bascones-Martinez, A.; Sanz, M. Local and systemic antimicrobial therapy in periodontics. J. Evid. Based Dent. Pract. 2012, 12, 50–60. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; Participants, E.F.P.W.; Methodological, C. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Brody, H.; Lin, G.H.; Range, H.; Kuraji, R.; Ye, C.; Kamarajan, P.; Radaic, A.; Gao, L.; Kapila, Y. Probiotics, including nisin-based probiotics, improve clinical and microbial outcomes relevant to oral and systemic diseases. Periodontol. 2000 2020, 82, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Balazs, E.A.; Laurent, T.C.; Jeanloz, R.W. Nomenclature of hyaluronic acid. Biochem. J. 1986, 235, 903. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Vet. Sci. 2019, 6, 192. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Li, L.; Wang, Z.; Li, P.; Feng, F.; Zheng, X. High molecular weight hyaluronic acid regulates P. gingivalis-induced inflammation and migration in human gingival fibroblasts via MAPK and NF-κB signaling pathway. Arch. Oral Biol. 2019, 98, 75–80. [Google Scholar] [CrossRef]
- Takahashi, K.; Goomer, R.S.; Harwood, F.; Kubo, T.; Hirasawa, Y.; Amiel, D. The effects of hyaluronan on matrix metalloproteinase-3 (MMP-3), interleukin-1beta(IL-1beta), and tissue inhibitor of metalloproteinase-1 (TIMP-1) gene expression during the development of osteoarthritis. Osteoarthr. Cartil. 1999, 7, 182–190. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.T.; Lin, Y.T.; Chiang, B.L.; Lin, Y.H.; Hou, S.M. High molecular weight hyaluronic acid down-regulates the gene expression of osteoarthritis-associated cytokines and enzymes in fibroblast-like synoviocytes from patients with early osteoarthritis. Osteoarthr. Cartil. 2006, 14, 1237–1247. [Google Scholar] [CrossRef] [Green Version]
- Gotoh, S.; Onaya, J.; Abe, M.; Miyazaki, K.; Hamai, A.; Horie, K.; Tokuyasu, K. Effects of the molecular weight of hyaluronic acid and its action mechanisms on experimental joint pain in rats. Ann. Rheum. Dis. 1993, 52, 817–822. [Google Scholar] [CrossRef]
- Hashizume, M.; Koike, N.; Yoshida, H.; Suzuki, M.; Mihara, M. High molecular weight hyaluronic acid relieved joint pain and prevented the progression of cartilage degeneration in a rabbit osteoarthritis model after onset of arthritis. Mod. Rheumatol. 2010, 20, 432–438. [Google Scholar] [CrossRef]
- Sasaki, T.; Watanabe, C. Stimulation of osteoinduction in bone wound healing by high-molecular hyaluronic acid. Bone 1995, 16, 9–15. [Google Scholar] [CrossRef]
- Ardizzoni, A.; Neglia, R.G.; Baschieri, M.C.; Cermelli, C.; Caratozzolo, M.; Righi, E.; Palmieri, B.; Blasi, E. Influence of hyaluronic acid on bacterial and fungal species, including clinically relevant opportunistic pathogens. J. Mater. Sci. Mater. Med. 2011, 22, 2329–2338. [Google Scholar] [CrossRef] [Green Version]
- Romano, C.L.; De Vecchi, E.; Bortolin, M.; Morelli, I.; Drago, L. Hyaluronic Acid and Its Composites as a Local Antimicrobial/Antiadhesive Barrier. J. Bone Jt. Infect. 2017, 2, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Cankaya, Z.T.; Gurbuz, S.; Bakirarar, B.; Kurtis, B. Evaluation of the Effect of Hyaluronic Acid Application on the Vascularization of Free Gingival Graft for Both Donor and Recipient Sites with Laser Doppler Flowmetry: A Randomized, Examiner-Blinded, Controlled Clinical Trial. Int. J. Periodontics Restor. Dent. 2020, 40, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Mamajiwala, A.S.; Sethi, K.S.; Raut, C.P.; Karde, P.A.; Mamajiwala, B.S. Clinical and radiographic evaluation of 0.8% hyaluronic acid as an adjunct to open flap debridement in the treatment of periodontal intrabony defects: Randomized controlled clinical trial. Clin. Oral Investig. 2021, 25, 5257–5271. [Google Scholar] [CrossRef] [PubMed]
- Matheus, H.R.; Ervolino, E.; Gusman, D.J.R.; Alves, B.E.S.; Fiorin, L.G.; Pereira, P.A.; de Almeida, J.M. Association of hyaluronic acid with a deproteinized bovine graft improves bone repair and increases bone formation in critical-size bone defects. J. Periodontol. 2020, 92, 1646–1658. [Google Scholar] [CrossRef] [PubMed]
- Shirakata, Y.; Imafuji, T.; Nakamura, T.; Kawakami, Y.; Shinohara, Y.; Noguchi, K.; Pilloni, A.; Sculean, A. Periodontal wound healing/regeneration of two-wall intrabony defects following reconstructive surgery with cross-linked hyaluronic acid-gel with or without a collagen matrix: A preclinical study in dogs. Quintessence Int. 2021, 52, 308–316. [Google Scholar] [CrossRef]
- Shirakata, Y.; Nakamura, T.; Kawakami, Y.; Imafuji, T.; Shinohara, Y.; Noguchi, K.; Sculean, A. Healing of buccal gingival recessions following treatment with coronally advanced flap alone or combined with a cross-linked hyaluronic acid gel. An experimental study in dogs. J. Clin. Periodontol. 2021, 48, 570–580. [Google Scholar] [CrossRef]
- Pirnazar, P.; Wolinsky, L.; Nachnani, S.; Haake, S.; Pilloni, A.; Bernard, G.W. Bacteriostatic effects of hyaluronic acid. J. Periodontol. 1999, 70, 370–374. [Google Scholar] [CrossRef]
- Binshabaib, M.; Aabed, K.; Alotaibi, F.; Alwaqid, M.; Alfraidy, A.; Alharthi, S. Antimicrobial efficacy of 0.8% Hyaluronic Acid and 0.2% Chlorhexidine against Porphyromonas gingivalis strains: An in-vitro study. Pak. J. Med. Sci. 2020, 36, 111–114. [Google Scholar] [CrossRef] [Green Version]
- Alharbi, M.S.; Alshehri, F.A.; Alobaidi, A.S.; Alrowis, R.; Alshibani, N.; Niazy, A.A. High molecular weight hyaluronic acid reduces the growth and biofilm formation of the oral pathogen Porphyromonas gingivalis. Saudi Dent. J. 2023, 35, 141–146. [Google Scholar] [CrossRef]
- Alharbi, M.S.; Alshehri, F.A. High Molecular Weight Hyaluronic Acid Reduces the Expression of Virulence Genes fimA, mfa1, hagA, rgpA, and kgp in the Oral Pathogen Porphyromonas gingivalis. Pharmaceutics 2022, 14, 1628. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Periodontology Task Force Report on the Update to the 1999 Classification of Periodontal Diseases and Conditions. J. Periodontol. 2015, 86, 835–838. [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Yu, K.F. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998, 280, 1690–1691. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Engstrom, P.E.; Shi, X.Q.; Tronje, G.; Larsson, A.; Welander, U.; Frithiof, L.; Engstrom, G.N. The effect of hyaluronan on bone and soft tissue and immune response in wound healing. J. Periodontol. 2001, 72, 1192–1200. [Google Scholar] [CrossRef]
- Xu, Y.; Hofling, K.; Fimmers, R.; Frentzen, M.; Jervoe-Storm, P.M. Clinical and microbiological effects of topical subgingival application of hyaluronic acid gel adjunctive to scaling and root planing in the treatment of chronic periodontitis. J. Periodontol. 2004, 75, 1114–1118. [Google Scholar] [CrossRef]
- Eick, S.; Renatus, A.; Heinicke, M.; Pfister, W.; Stratul, S.I.; Jentsch, H. Hyaluronic Acid as an adjunct after scaling and root planing: A prospective randomized clinical trial. J. Periodontol. 2013, 84, 941–949. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.T.; Ho, H.T.; Huynh, N.C.; Dien, V.H.; Vo, T.L. Hyaluronic acid 0.2% application enhanced periodontitis treatment in non-surgical phase. J. Stomatol. 2021, 74, 76–83. [Google Scholar] [CrossRef]
- Vajawat, M.; Rao, D.P.C.; Kumar, G.S.V.; Rajeshwari, K.G.; Hareesha, M.S. Local delivery of hyaluronic acid as an adjunct to scaling and root planing in the treatment of chronic periodontitis in smokers and non-smokers: A clinical and microbiological study. J. Indian Soc. Periodontol. 2022, 26, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Eliezer, M.; Imber, J.C.; Sculean, A.; Pandis, N.; Teich, S. Hyaluronic acid as adjunctive to non-surgical and surgical periodontal therapy: A systematic review and meta-analysis. Clin. Oral. Investig. 2019, 23, 3423–3435. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S. Microbial dysbiosis: The root cause of periodontal disease. J. Periodontol. 2021, 92, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S. Microbiomics: Were we all wrong before? Periodontol. 2000 2021, 85, 8–11. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Subjects | Design | HA Application | Sampling and Quantification Techniques | Results |
|---|---|---|---|---|---|
| Engström et al., 2001 [37] | Nine participants (4 males and 5 females) Diagnosis: chronic periodontitis | Randomized, controlled In each participant: one tooth as test and another as control, same jaw, at least two teeth in between | Professional subgingival application 3 times at 1-week interval 0.85 mL containing 1.4% HA | Sampling: sterile paper point Identification: Presence or absence by Brucella-blood agar culture and UV-light fluorescence identification | Test: Presence of P.g in 1 subject (of 9) at three months. Absence in 9 (of 9) at all other time intervals. Control: presence in 1 (of 9) at three months. Absence in 9 (of 9) at all other time intervals. |
| Xu et al., 2004 [38] | 20 participants (11 males 9 females) Diagnosis: chronic periodontitis | Split-mouth, non-randomized | Weekly professional subgingival application (baseline to 6 weeks, total 7 applications) 1 mL 0.2% hyaluronic acid gel | Sampling: sterile paper points Identification: Positive or negative using PCR and reverse hybridization | Prevalence of P.g: Test: BL = 65%, 6W = 60%, 12W = 50% Control: BL = 65%, 6W = 50%, 12W = 60% |
| Eick et al., 2013 [39] | 34 participants (14 males and 20 females) Diagnosis: moderate or severe periodontitis | Randomized, controlled, non-masked | 1-Professional subgingival application immediately after SRP: 0.8% gel (1800 kDa) 2-Twice/day at home application for 14 days: 0.2% 1000 kDa) | Sampling: Paper strips at the deepest site at premolar and molar areas Identification: PCR positive or negative | Prevalence of P.g: Test: BL = 59%, 3M = 59%, 6M = 59% Control: BL = 47%, 3M = 53%, 6M = 76% |
| Nguyen et al., 2021 [40] | 28 participants (6 males and 22 females) Diagnosis: moderate or severe periodontitis | Randomized, controlled, double-blinded, split-mouth | Professional subgingival application of 1 mL 02% HA gel at baseline, 1 week, 2 weeks, and 3 weeks. | Sampling: paper point at the deepest pocket Identification: bacterial load as log10 copies per mL by Real-time PCR | Quantity of P.g: Test: BL = 4.09 ± 2.82, 6W = 2.00 ± 2.66 Control: BL = 3.96 ± 3.18, 6W = 2.77 ± 2.53 |
| Vajawat et al., 2022 [41] | 11 smokers 11 non-smokers (22 subjects, 44 sites) Diagnosis: chronic periodontitis | Randomized, controlled, double-blinded, split-mouth | Professional weekly application of a gel containing high-molecular-weight sodium hyaluronate | Sampling: sub-gingival plaque collection using a Gracy’s curette Identification: colony forming units counting on agar plates | p-value of test vs. control: Smokers: BL = 0.173, 1M = 0.007 Non-smokers: BL = 0.964, 1M = 0.038 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshehri, F.A.; Alharbi, M.S. The Effect of Adjunctive Use of Hyaluronic Acid on Prevalence of Porphyromonas gingivalis in Subgingival Biofilm in Patients with Chronic Periodontitis: A Systematic Review. Pharmaceutics 2023, 15, 1883. https://doi.org/10.3390/pharmaceutics15071883
Alshehri FA, Alharbi MS. The Effect of Adjunctive Use of Hyaluronic Acid on Prevalence of Porphyromonas gingivalis in Subgingival Biofilm in Patients with Chronic Periodontitis: A Systematic Review. Pharmaceutics. 2023; 15(7):1883. https://doi.org/10.3390/pharmaceutics15071883
Chicago/Turabian StyleAlshehri, Fahad A., and Meshal S. Alharbi. 2023. "The Effect of Adjunctive Use of Hyaluronic Acid on Prevalence of Porphyromonas gingivalis in Subgingival Biofilm in Patients with Chronic Periodontitis: A Systematic Review" Pharmaceutics 15, no. 7: 1883. https://doi.org/10.3390/pharmaceutics15071883