
Hyaluronic Acid in Rheumatology

1
Medical Faculty, University of Zurich (UZH), CH-8006 Zurich, Switzerland
2
Arztpraxis Hottingen, CH-8032 Zurich, Switzerland
3
Medical Faculty, University of Jena, D-07743 Jena, Germany
*
Author to whom correspondence should be addressed.
Pharmaceutics 2023, 15(9), 2247; https://doi.org/10.3390/pharmaceutics15092247
Submission received: 15 July 2023
/
Revised: 25 August 2023
/
Accepted: 29 August 2023
/
Published: 30 August 2023
(This article belongs to the Special Issue Hyaluronic Acid for Medical Applications)
Abstract
:Hyaluronic acid (HA), also known as hyaluronan, is an anionic glycosaminoglycan widely distributed throughout various tissues of the human body. It stands out from other glycosaminoglycans as it lacks sulfation and can attain considerable size: the average human synovial HA molecule weighs about 7 million Dalton (Da), equivalent to roughly 20,000 disaccharide monomers; although some sources report a lower range of 3–4 million Da. In recent years, HA has garnered significant attention in the field of rheumatology due to its involvement in joint lubrication, cartilage maintenance, and modulation of inflammatory and/or immune responses. This review aims to provide a comprehensive overview of HA’s involvement in rheumatology, covering its physiology, pharmacology, therapeutic applications, and potential future directions for enhancing patient outcomes. Nevertheless, the use of HA therapy in rheumatology remains controversial with conflicting evidence regarding its efficacy and safety. In conclusion, HA represents a promising therapeutic option to improve joint function and alleviate inflammation and pain.
1. Introduction
Hyaluronic acid (HA) plays an important role in a wide range of medical physiological and pathological conditions: Notably, it finds application in dermatology, ophthalmology, cosmetic medicine, and rheumatology [1,2,3]. Its significance extends to wound healing, granulation, and cell migration [4]. However, the efficacy of HA in rheumatology remains a subject of controversy at times [5,6].
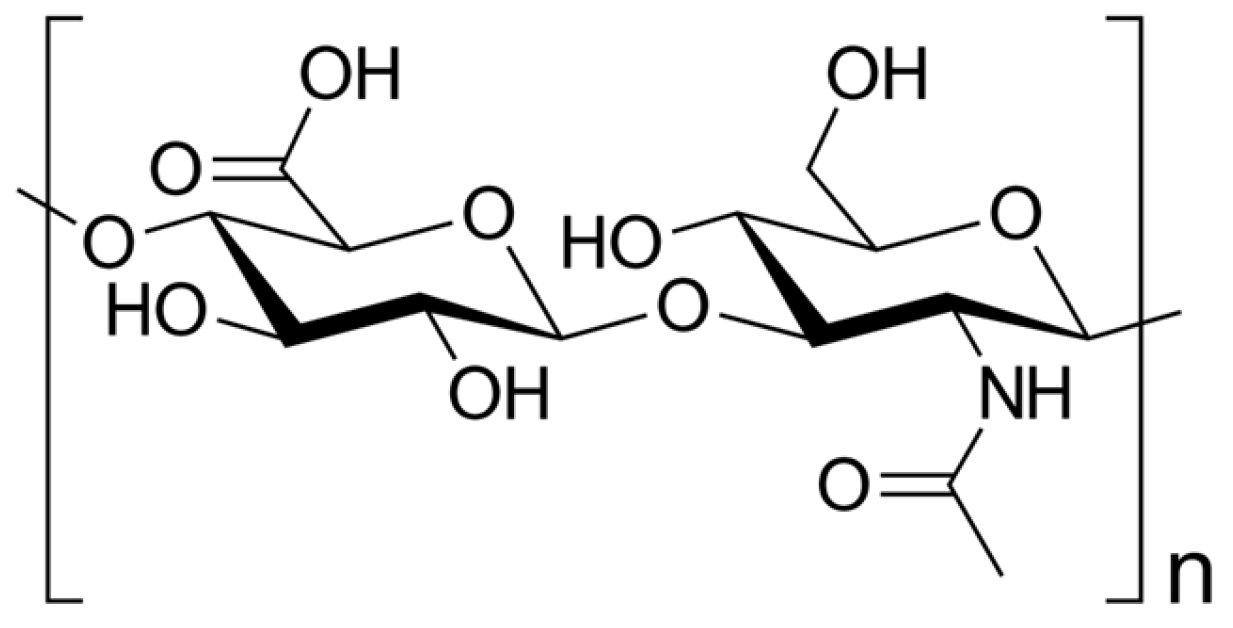
HA is as naturally occurring glycosaminoglycan composed of repeating disaccharide units consisting of glucuronic acids and N-acetylglucosamine (Figure 1), resulting in different molecular weights [7,8,9]. This structural variability imparts diverse functional implications in both physiological and pathological contexts [10]. HA is commercially produced through extraction from animal tissues, such as chicken combs, and from Streptococci bacteria [11].
Functionally, HA demonstrates remarkable water-binding capacity, rendering it an essential constituent of the extracellular matrix (ECM) [12]. Its elongated, unbranched chains create a gel-like network, imparting hydration and lubrication to crucial tissues like the skin, cartilage, and synovial fluid [13,14,15].
In the field of rheumatology, HA has garnered substantial attention, owing to its pivotal involvement in joint health and its relevance to diseases like osteoarthritis (OA) and rheumatoid arthritis (RA) [16,17].
OA is a degenerative joint disorder characterized by the gradual deterioration of articular cartilage, resulting in pain, stiffness, and diminished joint function [18]. There is no cure for OA, so doctors usually treat OA symptoms with a combination of therapies [18]. HA serves as a lubricant and shock absorber within the synovial fluid, facilitating smooth joint movements [19]. However, in OA, the concentration and quality of HA decrease, compromising its protective and viscoelastic properties due to heightened degradation and decreased synthesis. Consequently, this leads to impaired cartilage function and joint degeneration [20]. As a therapeutic approach, supplementation with exogenous HA has emerged to alleviate symptoms and enhance joint function in OA patients [21]. By restoring synovial fluid viscosity and promoting cartilage repair, HA aids in improving joint mobility and reducing pain [16].
On the other hand, RA is an autoimmune and inflammatory disease characterized by the immune system mistakenly attacking healthy cells, resulting in inflammation, particularly in the joints, leading to painful swelling [22]. RA can be effectively treated and managed with medication(s) and self-management strategies [22]. In RA, the level of HA in the synovial fluid is significantly diminished, causing reduced lubrication and increased inflammation and pain [23].
Numerous studies have explored the potential therapeutic benefits of exogenous HA supplementation in rheumatic diseases. Through intra-articular injections, HA has shown promise in improving joint mobility, reducing pain, and promoting cartilage repair by restoring synovial fluid viscosity [24].
Furthermore, HA has demonstrated immunomodulatory effects, including the suppression of pro-inflammatory cytokines and the promotion of anti-inflammatory cytokine production [25]. This suggests that HA may also hold promise in the treatment of immune-mediated rheumatic diseases [26].
Moreover, researchers have explored HA’s potential applications in drug delivery systems and tissue engineering due to its biocompatibility and biodegradability [27].
However, the use of HA therapy in rheumatology remains a topic of controversy, with conflicting evidence regarding its efficacy and safety [5,28].
In summary, HA represents a promising therapeutic option in the field of rheumatology due to its potential to enhance joint function and alleviate inflammation and pain [29]. Nevertheless, further investigation is required to fully elucidate its therapeutic potential in rheumatic diseases.
This review aims to provide a comprehensive overview of the structure, function, and rheumatological significance of HA. Additionally, it will discuss recent advancements in understanding HA’s role in joint health and the therapeutic potential of HA-based interventions. Furthermore, a critical analysis of the existing literature on HA in rheumatology will be presented.
2. Hyaluronic Acid: Structure, Function, and Biochemistry
HA plays a crucial role in diverse cellular and tissue processes, encompassing hydration, lubrication, tissue repair, regulation of inflammation, and cell signaling [14]. It is naturally synthesized by various cell types, predominantly fibroblasts, chondrocytes, and synoviocytes [30]. The biosynthesis of HA takes place in the plasma membrane through the coordinated activity of specific enzymes, including hyaluronan synthases [30].
2.1. Molecular Structure of Hyaluronic Acid
Hyaluronan synthases catalyze the addition of glucuronic acid and N-acetylglucosamine, leading to the formation of the repeating disaccharide units that constitute HA [31]. The molecular weight of HA displays highly variability, ranging from several hundred kilo Da to millions of kilo Da, exerting a direct impact on its functional properties [32]: Notably, higher-molecular-weight HA exhibits increased viscosity [33], thereby affecting its flow and lubrication capability, i.e., in joints [34]. As a result, high-molecular-weight HA provides superior lubrication and cushioning effects [35].
2.2. Biosynthesis and Degradation of Hyaluronic Acid
HA turnover in tissues is intricately regulated by a delicate balance between biosynthesis and degradation processes [36]. The degradation of HA primarily involves the action of enzymes known as hyaluronidases, which cleave HA into smaller fragments [37]. Hyaluronidase enzymes are categorized into several families, including HYAL1, HYAL2, and PH-20 [38], and they play a pivotal role in maintaining the appropriate concentration and size distribution of HA within tissues [39]. Furthermore, the degradation of HA can be modulated by reactive oxygen species, matrix metalloproteinases (MMPs), and other factors present in the extracellular environment [40].
2.3. Physiological Functions and Distribution in Tissues of Hyaluronic Acid
HA plays a critical role in tissue repair and remodeling processes within the human body [41]. It participates in various stages of wound healing, encompassing inflammation, cell migration, proliferation, and ECM remodeling [42]. As a scaffolding molecule, HA provides essential structural support and aids in cell migration during tissue repair [43] (Table 1).
During the inflammatory phase of wound healing, HA is involved in the recruitment and activation of immune cells, such as macrophages and neutrophils [51]. HA fragments generated during tissue injury can function as damage-associated molecular patterns and trigger immune responses [51]. Moreover, HA promotes the infiltration of immune cells into the wound site, facilitating the removal of debris and pathogens [52]. In the subsequent proliferative phase, HA contributes to cell migration and proliferation [53]. It forms a provisional matrix that guides cell movement and stimulates cell proliferation [53]. HA receptors, such as CD44 and RHAMM, mediate cell adhesion, migration, and signal transduction, enabling cells to migrate into the wound area and contribute to tissue repair [54]. Furthermore, HA plays a regulatory role in ECM remodeling during tissue repair [55]. It interacts with other components, such as fibronectin and collagen, promoting their assembly and organization [56]. HA also influences the activity of enzymes involved in ECM remodeling, such as MMPs and tissue inhibitors of MMPs, which are essential for matrix turnover and remodeling [57].
Beyond its involvement in tissue repair, HA also plays a role in tissue remodeling processes, such as embryonic development, organ morphogenesis, and angiogenesis [58]. HA provides a structural framework for cell migration and tissue organization during these processes [59]. It regulates cell behavior, including cell differentiation, proliferation, and survival, through interactions with specific receptors and signaling pathways [60].
Overall, HA exhibits a multifaceted role in tissue repair and remodeling, contributing to inflammation resolution, cell migration, proliferation, and ECM (re)organization [61]. Its involvement in these processes highlights its significance in wound healing, tissue regeneration, and developmental biology [62].
Regarding tissue distribution, HA is widely distributed throughout the body, with particularly high concentrations found in connective tissues, such as the skin, synovial fluid, and cartilage [63]. In the skin, HA resides in the ECM and contributes to tissue hydration, elasticity, and wound healing [64]. In the synovial fluid of joints, HA forms a viscous, gel-like substance that provides lubrication, shock absorption, and nutrient supply to the articular cartilage [65]. Additionally, HA is present in the vitreous humor of the eye, where it helps maintain the transparency and shape of the eyeball [66]. Moreover, HA is found in other tissues, including the umbilical cord, umbilical vessels, and embryonic tissues, where it plays crucial roles in development and tissue morphogenesis [67].
3. Pathophysiological Role of Hyaluronic Acid in Rheumatic Diseases
HA plays a crucial pathophysiological role in rheumatic diseases, especially concerning joint health and function [68]. In a healthy joint, HA’s viscoelastic properties facilitate smooth movement of the joint surfaces and shield the cartilage from excessive mechanical stress [69]. HA serves as a shock absorber, mitigating the impact on the joint and thereby reducing the risk of damage. However, in rheumatic conditions such as OA and RA, significant alterations occur in the HA metabolism and distribution within the joint [70].
3.1. Osteoarthritis
3.1.1. Role of Hyaluronic Acid in Joint Lubrication
In OA, there is a notable reduction in the concentration of HA within the synovial fluid, leading to diminished joint lubrication and compromised cartilage protection [69]. This decline in HA levels can be attributed to an imbalance between HA synthesis and degradation, with increased activity of hyaluronidases, the enzymes responsible for HA breakdown [71]. Consequently, the cartilage becomes vulnerable to wear and tear, resulting in pain, stiffness, and functional impairment [72]. Dysregulated HA metabolism, including increased synthesis and degradation, contributes to cartilage degradation, synovitis, and pain in OA [73]. The altered biomechanical properties of HA affect joint lubrication, chondrocyte activity, and inflammation, further exacerbating disease progression [74].
3.1.2. Protective Effects on Chondrocytes and Cartilage Matrix
HA serves as a fundamental component of the cartilage matrix, playing a crucial role in maintaining joint integrity. However, in OA, changes occur in the quantity, molecular weight, and distribution of HA, which can impact its functional properties [75]. The molecular weight of HA influences its retention time within the tissues [76]. Generally, higher-molecular-weight HA exhibits a longer half-life, meaning it remains in the joint or tissue for a more extended period before being broken down and cleared by the body [8]. This prolonged presence may result in longer-lasting effects [8]. On the other hand, lower-molecular-weight HA can more easily penetrate the ECM and reach target cells, while higher-molecular-weight HA may have more limited diffusion [8].
3.1.3. Modulation of Inflammation and Synovial Fluid Changes
Inflammation is a hallmark of rheumatic diseases [77], and HA plays a multifaceted role in this process [78]. Pathological conditions often lead to changes in the quantity and molecular weight of HA in synovial fluid, with implications for disease severity and progression [79]. During the inflammatory phase, HA actively participates in the recruitment and activation of immune cells, such as macrophages and neutrophils [79]. HA engages with specific cell surface receptors, such as CD44 [80], and the binding affinity of HA to these receptors can vary depending on its molecular weight [81]. Distinct fractions of HA, characterized by different molecular weights, can have specific effects on cell signaling, inflammation, and tissue repair processes [82].
3.2. Rheumatoid Arthritis
In RA, the inflammatory process significantly disrupts HA homeostasis [83]. Synovial inflammation induces the release of pro-inflammatory cytokines and enzymes that promote the degradation of HA, leading to a decrease in its concentration and alterations in its molecular weight distribution [84]. These changes in HA metabolism have profound effects on joint lubrication, exacerbate cartilage damage, and perpetuate the inflammatory cycle [85].
3.2.1. Altered Hyaluronic Acid Synthesis and Breakdown
In RA, alterations in HA synthesis and breakdown contribute to the pathogenesis of the disease [70]. Synovial fibroblasts, key players in RA pathophysiology, exhibit dysregulated HA synthesis, leading to increased production and accumulation of HA in the synovial fluid and tissues [86]. This abnormal HA synthesis is influenced by various factors, including pro-inflammatory cytokines and growth factors, which stimulate the expression of HA synthases [87]. Concurrently, increased HA degradation occurs due to upregulated expression and activity of hyaluronidases [88]. The imbalance between HA synthesis and degradation results in the accumulation of fragmented HA in the synovial fluid, exacerbating inflammation and joint damage [89]. Moreover, the presence of HA fragments in the synovium further amplifies the inflammatory response by activating immune cells and promoting the production of pro-inflammatory mediators [90]. The presence of HA fragments and their interaction with CD44 receptors contribute to the perpetuation of chronic inflammation and joint damage in RA [91].
3.2.2. Inflammatory Mediator Modulation
Moreover, the anti-inflammatory properties of HA, which typically involve the modulation of the inflammatory responses within the joints, are disturbed in RA [83]. The inhibitory action of HA on the production of pro-inflammatory cytokines, such as tumor necrosis factor-alpha and interleukin-1 beta, and the suppression of inflammatory enzymes, such as cyclooxygenase-2 and MMPs, become dysregulated [92]. During the subsequent proliferative phase, HA continues to play a role in cell migration and proliferation, forming a provisional matrix that guides cell movement and stimulates cell proliferation [93].
3.2.3. Effects on Synovial Hyperplasia and Pannus Formation
HA exerts significant effects on synovial hyperplasia and pannus formation in RA [93]. It plays a pivotal role in promoting synovial hyperplasia by stimulating the proliferation and migration of synovial fibroblasts [94]. Furthermore, it interacts with CD44 receptors on the surface of these fibroblasts, triggering intracellular signaling cascades that promote cell survival, proliferation, and ECM production [95]. Additionally, HA enhances the expression of various pro-inflammatory mediators, such as cytokines and chemokines, further driving synovial hyperplasia and inflammation [96]. Additionally, HA fragments, generated due to the increased breakdown of HA in RA, can stimulate the production of matrix-degrading enzymes, leading to cartilage and bone destruction [97].
4. Mechanisms of Action and Delivery Systems
HA has undergone extensive study to unravel its mechanisms of action and explore various delivery systems to enhance its therapeutic applications [29]. HA exerts its effects through multiple mechanisms, including its ability to bind to cell surface receptors, regulate cell signaling pathways, modulate inflammation, and provide structural support to tissues [98]. Moreover, HA serves as a viscoelastic agent, offering lubrication and shock absorption in joints, and contributing to tissue hydration and elasticity [99]. Overall, HA exhibits diverse mechanisms of action, and its therapeutic efficacy has been supported by clinical trials in various medical fields [100,101]. HA-based delivery systems have been developed to improve its delivery and enhance therapeutic outcomes [102]. As a relatively new polymer for constructing drug delivery systems, HA offers a promising platform for physically encapsulating or chemically conjugating various drugs [103]. With a favorable safety profile, HA-based therapies have shown promise as effective treatments for conditions such as OA, among others [104]. It is essential to note that the specific effects of HA, based on its molecular weight, can vary depending on the context, such as the route of administration (e.g., intra-articular injection, topical application) and the specific medical condition being targeted [105]. The selection of HA with a specific molecular weight for therapeutic use is often based on the desired therapeutic outcomes and the specific needs of the patient [106].
4.1. Safety Profile and Adverse Events
In terms of safety, HA-based therapies are generally well-tolerated [107]. It is crucial for healthcare professionals to conduct a thorough evaluation of patients for contraindications, carefully select suitable candidates for HA-based therapies, and adhere to proper injection techniques to minimize the risk of adverse events. Furthermore, patients should be informed about potential risks and benefits, and their consent should be obtained before initiating treatment.
While HA is considered safe, it is essential to be aware of potential local and systemic reactions, the risk of infection, hypersensitivity reactions, and long-term safety when using HA-based therapies [108]. HA derived from different sources and with varying molecular weights may differ in immunogenic potential [109]. Some studies have indicated that lower-molecular-weight HA might have a higher likelihood of inducing immune responses [110], although the clinical significance of this is still under investigation. Adherence to appropriate guidelines, proper patient selection, and adequate follow-up(s) are essential aspects to ensure the safe and effective use of HA in clinical practice.
4.1.1. Local and Systemic Reactions
Adverse events related to HA-based therapies are generally rare and mostly mild, often limited to local reactions at the injection site, such as pain or swelling [111]. Severe allergic reactions or systemic adverse events are extremely uncommon but can occur, underscoring the importance of proper patient selection and administration technique [112]. Overall, the safety profile of HA is considered favorable (Table 2).
4.1.2. Infections Risks
In terms of infection risk, the incidence of HA-related infections is low [108]. Adherence to proper aseptic techniques during the procedure and following guidelines can effectively minimize the risk of infection [113]. However, in rare cases, infection can occur, particularly when HA injections are performed in areas with compromised skin integrity or in the presence of preexisting infections [108].
4.1.3. Hypersensitivity Reactions
Hypersensitivity reactions to HA have been reported, albeit rarely [1]. These reactions can vary from mild local allergic reactions to more severe systemic manifestations [114]. Individuals with a history of known hypersensitivity to HA or other components of the formulation should be carefully evaluated and, if necessary, alternative treatment options should be considered.
4.1.4. Long-Term Safety
Long-term safety and follow-up studies play a crucial role in assessing the safety profile of HA-based therapies. Although HA has been utilized for several decades, ongoing research aims to evaluate its long-term effects and ensure its continued safety. Follow-up studies have consistently demonstrated the safety and efficacy of HA injections over extended periods, with low rates of serious adverse events reported [24] (Table 2).

{kind=link}
Table 2.
Safety and adverse events of hyaluronic acid (HA) in rheumatology.
| Study | Design | Participants | Findings | References |
|---|---|---|---|---|
| Petrella et al. (2008) | Systematic review | 24 randomized controlled trials | HA injections had a low incidence of adverse events, with most being mild and transient in nature. | [111] |
| Shen et al. (2018) | Meta-analysis | 84 randomized controlled trials | HA injections were generally well tolerated, with low rates of serious adverse events. | [115] |
| Najm et al. (2021) | Systematic review and meta-analysis | 15 randomized controlled trials | HA injections demonstrated a favourable safety profile, with rare reports of hypersensitivity reactions and infections. | [116] |
| Conrozier et al. (2021) | Review (Delphi method) | 24 statements | HA injections were associated with a low risk of adverse events, with most being localized and self-limiting. | [117] |
| Chevalier et al. (2020) | Systematic review and meta-analysis | 162 randomized controlled trials | HA injections were well tolerated, with a low incidence of serious adverse events and local reactions. | [118] |
Summary of selected studies that have examined the safety profile and adverse events associated with the use of HA in rheumatology. It is important to note that the incidence and nature of adverse events may vary across studies and patient populations. For a comprehensive understanding, it is recommended to refer to the full-text articles cited in the references.
4.2. Systemic Administration of Hyaluronic Acid
To optimize the delivery of HA-based therapeutics, various delivery systems have been developed. These systems encompass injectable gels, nanoparticles, liposomes, and hydrogels, which enable the controlled release and targeted delivery of HA to specific tissues or cells [119]. By utilizing these delivery systems, the bioavailability and retention of HA at the desired site can be enhanced, thereby improving its therapeutic efficacy [120].
4.2.1. Oral, Intravenous, and Intraarticular Routes
HA has been extensively studied for its potential therapeutic applications via different routes of administration, including oral, intra-articular, and intravenous routes [121]. Each route presents its own set of challenges and limitations.
The oral administration of HA aims to provide systemic benefits, targeting various tissues throughout the body [122]. However, the oral bioavailability of HA is generally low, due to its large molecular size and susceptibility to enzymatic degradation in the gastrointestinal tract [123]. Furthermore, the absorption of HA through the intestinal epithelium is limited [124]. These challenges have hindered the development of effective oral formulations of HA, and alternative routes of administration have been explored to overcome these limitations.
Intra-articular administration of HA has been widely used for the treatment of joint disorders such as OA [16]. This route allows for the direct delivery of HA into the affected joint, providing local therapeutic effects. Intra-articular injections of HA have shown clinical efficacy in reducing pain, improving joint function, and delaying disease progression [125] (Table 3). However, the limitations of this route include the need for repeated injections, potential injection-related complications, and the possibility of adverse reactions, although these are rare [16].
Intravenous administration of HA has been investigated for its potential systemic effects and applications. This route allows the rapid distribution of HA throughout the body, potentially targeting various tissues and organs. However, the challenges lie in achieving optimal bioavailability and targeting specific tissues, as HA may undergo rapid clearance from the bloodstream and may not reach the desired site of action in sufficient concentrations [130].
4.2.2. Delivery Systems
In summary, due to its unique physicochemical properties and therapeutic potential, HA has garnered considerable attention in terms of therapeutical use. However, the clinical utility of HA is hindered by its short half-life and poor bioavailability [131]. To overcome these limitations, various delivery systems have been developed to enhance the stability, sustained release, and targeted delivery of HA [29,104]. Different types of HA delivery systems have been explored, such as injectable hydrogels, including micro- and nanoparticles, liposomes, as well as coatings and scaffolds [132,133,134,135]. Furthermore, various formulation strategies and modes of action, such as crosslinking techniques, surface modification, encapsulation methods, or sustained release mechanisms, have been employed [136,137,138,139]. Moreover, hybrid delivery systems have been introduced, allowing for optimized HA delivery, and contributing to personalized treatment options [140,141].
4.3. Disease-Modifying Effects and Immunomodulation
HA appears to have the ability to modify the disease course and modulate the immune response in rheumatological conditions [142,143]. This is attributed to its interactions with receptors, impact on inflammatory mediators, and modulation of cellular responses [144] (see also Section 2 and Section 3 above: Physiological and pathophysiological role of HA). Understanding of HA’s therapeutic potential in rheumatologic disorders paves the way for the development of novel treatment strategies.
4.4. Challenges and Limitations
Despite the therapeutic potential of HA, its clinical application via different routes still faces certain limitations. These include the high cost of production and purification, potential immunogenicity, and allergic reactions, as well as the need for further optimization of delivery systems to enhance bioavailability, targeting, and sustained release [145]. Additionally, there is a need for standardized dosing regimens, well-designed clinical trials, and long-term safety data to establish the efficacy and safety profile of HA-based therapies.
In conclusion, while HA holds promise for therapeutic applications via oral, intra-articular, and intravenous routes, each route presents specific challenges and limitations. Further research is needed to overcome these limitations, optimize delivery systems, and establish the efficacy, safety, and long-term benefits of HA-based therapies.
5. Therapeutic Approaches
Understanding the pathophysiological role of HA in rheumatic diseases offers potential avenues for therapeutic interventions. Clinical trials have been conducted to evaluate the efficacy of HA-based therapies in various medical conditions. In the field of rheumatology, intra-articular injections of HA have shown beneficial effects in reducing pain, improving joint function, and delaying the progression of OA [46]. Clinical evidence supports the use of HA injections as a safe and effective treatment option for knee OA, with long-term benefits and a favorable safety profile [146].
Targeting HA-mediated pathways, including HA synthesis, degradation, and interactions with specific receptors, holds promise for developing disease-modifying therapies [147]. Additionally, emerging techniques like tissue engineering and nanotechnology present exciting opportunities for HA-based interventions [148].
5.1. Combination Therapies
HA has demonstrated potential for use in combination therapies and novel approaches to enhance its therapeutic effects in various medical conditions [149]. These approaches involve combinations of HA with corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), or platelet-rich plasma (PRP), which can provide synergistic benefits in managing inflammatory and degenerative conditions.
5.1.1. Hyaluronic Acid and Corticosteroids
5.1.2. Hyaluronic Acid and Nonsteroidal Anti-Inflammatory Drugs
Another combination strategy involves the use of HA in conjunction with NSAIDs. This approach aims to address both the inflammatory component and symptomatic relief in conditions such as OA [152]. Studies have shown that combining HA with NSAIDs can result in enhanced pain reduction and improved joint function compared to NSAIDs alone [153].
5.1.3. Hyaluronic Acid and Platelet-Rich Plasma
Furthermore, HA has been explored in combination with PRP, which contains growth factors and cytokines that promote tissue healing and regeneration [154]. The combination of HA and PRP has shown promising results in accelerating tissue repair, reducing pain, and improving functional outcomes in conditions such as tendinopathies and OA [155].
5.2. Novel Approaches, Emerging Strategies, and Future Directions
HA plays a key role in the pathophysiology of rheumatic diseases, exerting diverse effects on inflammation, joint destruction, and tissue homeostasis [156]. Advances in understanding HA metabolism and its interaction with immune and non-immune components have illuminated the complex mechanisms underlying rheumatic diseases. Leveraging this knowledge may lead to the development of innovative therapeutic strategies to improve patient outcomes and alleviate the burden associated with rheumatic diseases.
Novel approaches are also being explored to enhance the therapeutic potential of HA. These include the development of modified forms of HA with improved properties, such as crosslinked HA derivatives, which exhibit the prolonged residence time and sustained release of HA [157]. Additionally, nanotechnology-based delivery systems and combinations with other biomaterials are being investigated to improve HA’s bioavailability, targeting, and regenerative potential [158].
Emerging strategies for HA-based therapies involve tissue engineering approaches where HA is combined with cells and scaffolds to promote tissue regeneration [159]. This approach holds promise for the repair and regeneration of various tissues, including cartilage, skin, and bone [160].
By harnessing the synergistic effects of HA with other therapeutic agents, it is possible to enhance its regenerative, anti-inflammatory, and analgesic properties, opening up new avenues for personalized medicine and tissue engineering approaches [161,162,163]. Further research is warranted to elucidate the precise molecular mechanisms and evaluate the efficacy of targeted interventions in clinical settings with respect to long-term safety and cost-effectiveness of combination therapies involving HA.
6. Conclusions and Future Perspectives
In conclusion, HA has emerged as a valuable therapeutic agent in rheumatology due to its unique properties, including its lubricating, anti-inflammatory, and chondroprotective effects, making it an attractive option for the management of various rheumatic diseases, particularly OA. Intra-articular injections of HA have shown efficacy in reducing pain, improving joint function, and delaying disease progression. Moreover, HA’s role in tissue repair and remodeling, as well as its potential to modulate inflammation and protect chondrocytes and cartilage matrices, further highlight its therapeutic potential in rheumatology.
In clinical practice, intra-articular injections of exogenous HA have been widely used as a therapeutic approach for managing rheumatic diseases. These injections aim to restore depleted levels of HA in the joint, improve lubrication, reduce inflammation, and provide symptomatic relief. Numerous clinical studies have demonstrated the efficacy of HA injections in alleviating pain, enhancing joint function, and delaying the need for surgical interventions in patients with OA and RA.
Insurance coverage for medical procedures, including intra-articular HA injections, can vary widely depending on the country, specific insurance plan, and local regulations. This may be due to a lack of sufficient evidence. Health insurance systems often consider the effectiveness and cost-effectiveness of treatments before providing coverage. If there is limited scientific evidence or conflicting studies regarding the effectiveness of intra-articular HA injections for a specific condition, insurers may be hesitant to cover it. Intra-articular HA injections can be relatively expensive, especially considering the number of injections required for a full treatment course. If insurers deem the cost to outweigh the potential benefits, they may choose not to cover it. Additionally, in some cases, there may be alternative treatments available for the same condition that might have been proven to be more effective or cost-effective. Then, insurers may prioritize coverage for those alternatives, such as physical therapy, medications, or other interventions, over intra-articular HA injections.
Future perspectives on the use of HA in rheumatology are promising. Advancements in the development of delivery systems and formulations may improve the bioavailability and sustained release of HA, thereby optimizing its therapeutic effects. Combination therapies involving HA, such as its combination with corticosteroids, NSAIDs, or PRP, hold potential for enhanced therapeutic outcomes and improved patient management. Furthermore, the exploration of novel approaches, including tissue engineering and regenerative medicine strategies, may lead to the development of more targeted and personalized treatment options in rheumatic diseases.
Despite the progress made in understanding the role of HA in rheumatology, further research is needed to elucidate its mechanisms of action, optimize treatment protocols, and establish long-term safety and efficacy. Well-designed clinical trials, standardized dosing regimens, and comprehensive follow-up studies are necessary to gather robust evidence and guide clinical practice. Additionally, cost-effectiveness analyses and health–economic evaluations will contribute to the broader adoption and accessibility of HA-based therapies in rheumatology.
Overall, HA holds great promise as a therapeutic agent in rheumatology. With ongoing research and technological advancements, it is expected that HA-based treatments will continue to evolve, providing improved outcomes and enhancing the quality of life for patients with rheumatic diseases.
Author Contributions
Conceptualization, H.S.; formal analysis, H.S.; writing—original draft preparation, H.S.; writing—review and editing, C.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable due to the review design.
Informed Consent Statement
Not applicable due to the review design.
Data Availability Statement
No new data were created or analyzed in this review article. Data sharing is not applicable to this review.
Acknowledgments
Dedicated to Helmut Bräunlich, Professor emeritus and former head of the Department of Pharmacology at the Institute of Pharmacology and Toxicology of the University of Jena, Germany, our mentor and teacher.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Monfort, J.; Lisbona, M.P.; Gimenez-Arnau, A.; Iglesias, M.; Llorente-Onaindia, J.; Benito, P. Immunoallergic reaction following intraarticular injection of high molecular weight hyaluronic acid. Jt. Bone Spine 2013, 80, 551–552. [Google Scholar] [CrossRef] [PubMed]
- Roszkowska, A.M.; Inferrera, L.; Spinella, R.; Postorino, E.; Gargano, R.; Oliverio, G.W.; Aragona, P. Clinical Efficacy, Tolerability and Safety of a New Multiple-Action Eyedrop in Subjects with Moderate to Severe Dry Eye. J. Clin. Med. 2022, 11, 6975. [Google Scholar] [CrossRef] [PubMed]
- Borzabadi-Farahani, A.; Mosahebi, A.; Zargaran, D. A Scoping Review of Hyaluronidase Use in Managing the Complications of Aesthetic Interventions. Aesthetic Plast. Surg. 2022. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U. Medical use of hyaluronic acid—A 2023 perspective. CosmoDerma 2023, 3, 86. [Google Scholar] [CrossRef]
- Chen, L.H.; Xue, J.F.; Zheng, Z.Y.; Shuhaidi, M.; Thu, H.E.; Hussain, Z. Hyaluronic acid, an efficient biomacromolecule for treatment of inflammatory skin and joint diseases: A review of recent developments and critical appraisal of preclinical and clinical investigations. Int. J. Biol. Macromol. 2018, 116, 572–584. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.E. Towards reaching consensus on hyaluronic acid efficacy in knee osteoarthritis. Clin. Rheumatol. 2019, 38, 2881–2883. [Google Scholar] [CrossRef] [PubMed]
- Hyaluronic Acid. Available online: https://en.wikipedia.org/wiki/Hyaluronic_acid (accessed on 3 June 2023).
- Fraser, J.R.; Laurent, T.C.; Laurent, U.B. Hyaluronan: Its nature, distribution, functions and turnover. J. Intern. Med. 1997, 242, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Saari, H.; Konttinen, Y.T.; Friman, C.; Sorsa, T. Differential effects of reactive oxygen species on native synovial fluid and purified human umbilical cord hyaluronate. Inflammation 1993, 17, 403–415. [Google Scholar] [CrossRef]
- Bruyère, O.; Reginster, J.Y.; Honvo, G. Health economic evaluation of a high and low molecular weight hyaluronic acid formulation for the treatment of knee osteoarthritis. Post hoc analyses from a randomized clinical trial. Rheumatol. Ther. 2022, 9, 1119–1128. [Google Scholar] [CrossRef]
- Sze, J.; Brownlie, J.C.; Love, C.A. Biotechnological production of hyaluronic acid: A mini review. 3 Biotech 2016, 6, 67. [Google Scholar] [CrossRef]
- Ohnishi, T.; Novais, E.J.; Risbud, M. Alterations in ECM signature underscore multiple sub-phenotypes of intervertebral disc degeneration. Matrix Biol. Plus 2020, 21, 100036. [Google Scholar] [CrossRef] [PubMed]
- Galvez-Martin, P.; Soto-Fernandez, C.; Romero-Rueda, J.; Cabañas, J.; Torrent, A.; Castells, G.; Martinez-Puig, D. A Novel Hyaluronic Acid Matrix Ingredient with Regenerative, Anti-Aging and Antioxidant Capacity. Int. J. Mol. Sci. 2023, 24, 4774. [Google Scholar] [CrossRef] [PubMed]
- Matheson, A.R.; Sheehy, E.J.; Jay, G.D.; Scott, W.M.; O’Brien, F.J.; Schmidt, T.A. The role of synovial fluid constituents in the lubrication of collagen-glycosaminoglycan scaffolds for cartilage repair. J. Mech. Behav. Biomed. Mater. 2021, 118, 104445. [Google Scholar] [CrossRef] [PubMed]
- Mustonen, A.; Capra, J.; Rilla, K.; Lehenkari, P.; Oikari, S.; Kääriäinen, T.; Joukainen, A.; Kröger, H.; Paakkonen, T.; Matilainen, J.; et al. Characterization of hyaluronan-coated extracellular vesicles in synovial fluid of patients with osteoarthritis and rheumatoid arthritis. BMC Musculoskelet. Disord. 2021, 22, 247. [Google Scholar] [CrossRef] [PubMed]
- Householder, N.A.; Raghuram, A.; Agyare, K.; Thipaphay, S.; Zumwalt, M. A Review of Recent Innovations in Cartilage Regeneration Strategies for the Treatment of Primary Osteoarthritis of the Knee: Intra-articular Injections. Orthop. J. Sports Med. 2023, 11, 23259671231155950. [Google Scholar] [CrossRef] [PubMed]
- Marcolina, A.; Vu, K.; Chang Chien, G. Peripheral Joint Injections. Phys. Med. Rehabil. Clin. N. Am. 2022, 33, 267–306. [Google Scholar] [CrossRef] [PubMed]
- Osteoarthritis (OA) Arthritis CDC. Available online: https://www.cdc.gov/arthritis/basics/osteoarthritis.htm (accessed on 4 August 2023).
- Ferreira, N.D.R.; Sanz, C.K.; Raybolt, A.; Pereira, C.M.; DosSantos, M.F. Action of Hyaluronic Acid as a Damage-Associated Molecular Pattern Molecule and Its Function on the Treatment of Temporomandibular Disorders. Front. Pain Res. 2022, 3, 852249. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Yuan, Z.; Yang, H.; Zhong, H.; Peng, W.; Xie, R. Recent Advances in Understanding the Role of Cartilage Lubrication in Osteoarthritis. Molecules 2021, 26, 6122. [Google Scholar] [CrossRef]
- Costa, F.R.; Costa Marques, M.R.; Costa, V.C.; Santos, G.S.; Martins, R.A.; Santos, M.D.S.; Santana, M.H.A.; Nallakumarasamy, A.; Jeyaraman, M.; Lana, J.V.B.; et al. Intra-Articular Hyaluronic Acid in Osteoarthritis and Tendinopathies: Molecular and Clinical Approaches. Biomedicines 2023, 11, 1061. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Division of Population Health. Available online: https://www.cdc.gov/arthritis/basics/rheumatoid-arthritis.html (accessed on 4 August 2023).
- Ragan, C.; Meyer, K. The hyaluronic acid of synovial fluid in rheumatoid arthritis. J. Clin. Investig. 1949, 28, 56–59. [Google Scholar] [CrossRef]
- De Lucia, O.; Murgo, A.; Pregnolato, F.; Pontikaki, I.; De Souza, M.; Sinelli, A.; Cimaz, R.; Caporali, R. Hyaluronic Acid injections in the treatment of osteoarthritis secondary to primary inflammatory rheumatic diseases: A systematic review and qualitative synthesis. Adv. Ther. 2020, 37, 1347–1359. [Google Scholar] [CrossRef] [PubMed]
- Knopf-Marques, H.; Pravda, M.; Wolfova, L.; Velebny, V.; Schaaf, P.; Vrana, N.E.; Lavalle, P. Hyaluronic Acid and Its Derivatives in Coating and Delivery Systems: Applications in Tissue Engineering, Regenerative Medicine and Immunomodulation. Adv. Healthc. Mater. 2016, 5, 2841–2855. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.M.; Bedi, A.; Manjoo, A.; Niazi, F.; Shaw, P.; Mease, P. Anti-Inflammatory Effects of Intra-Articular Hyaluronic Acid: A Systematic Review. Cartilage 2019, 10, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Salathia, S.; Gigliobianco, M.; Casadidio, C.; Di Martino, P.; Censi, R. Hyaluronic Acid-Based Nanosystems for CD44 Mediated Anti-Inflammatory and Antinociceptive Activity. Int. J. Mol. Sci. 2023, 24, 7286. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.; Plaas, A.; Block, J.A. Intra-articular Hyaluronan Therapy for Symptomatic Knee Osteoarthritis. Rheum. Dis. Clin. N. Am. 2019, 45, 439–451. [Google Scholar] [CrossRef] [PubMed]
- Harrer, D.; Sanchez Armengol, E.; Friedl, J.D.; Jalil, A.; Jelkmann, M.; Leichner, C.; Laffleur, F. Is hyaluronic acid the perfect excipient for the pharmaceutical need? Int. J. Pharm. 2021, 15, 120589. [Google Scholar] [CrossRef] [PubMed]
- Pendyala, M.; Woods, P.S.; Brubaker, D.K.; Blaber, E.A.; Schmidt, T.A.; Chan, D.D. Endogenous production of hyaluronan, PRG4, and cytokines is sensitive to cyclic loading in synoviocytes. PLoS ONE 2022, 17, e0267921. [Google Scholar] [CrossRef]
- Atkins, E.D.; Sheehan, J.K. The molecular structure of hyaluronic acid. Biochem. J. 1971, 125, 92P. [Google Scholar] [CrossRef]
- Jabbari, F.; Babaeipour, V.; Saharkhiz, S. Comprehensive review on biosynthesis of hyaluronic acid with different molecular weights and its biomedical applications. Int. J. Biol. Macromol. 2023, 240, 124484. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Okamoto, A.; Nishinari, K. Viscoelasticity of hyaluronic acid with different molecular weights. Biorheology 1994, 31, 235–244. [Google Scholar] [CrossRef]
- Zhang, L.; Weifeng, L.; Yaxun, F.; Nir, K.; Yilin, W.; Klein, J. Effects of Hyaluronan Molecular Weight on the Lubrication of Cartilage-Emulating Boundary Layers. Biomacromolecules 2020, 21, 4345–4354. [Google Scholar] [CrossRef]
- Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Vet. Sci. 2019, 6, 192. [Google Scholar] [CrossRef] [PubMed]
- Tobisawa, Y.; Fujita, N.; Yamamoto, H.; Ohyama, C.; Irie, F.; Yamaguchi, Y.J. The cell surface hyaluronidase TMEM2 is essential for systemic hyaluronan catabolism and turnover. J. Biol. Chem. 2021, 297, 101281. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.T.; Kam, J.; Bloom, J.D. Hyaluronic Acid. Basics and Rheology. Clin. Plast. Surg. 2023, 50, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Csoka, A.B.; Frost, G.I.; Stern, R. The six hyaluronidase-like genes in the human and mouse genomes. Matrix Biol. 2001, 20, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Valcarcel, J.; García, M.; Varela, U.R.; Vázquez, J.A. Hyaluronic acid of tailored molecular weight by enzymatic and acid depolymerization. Int. J. Biol. Macromol. 2020, 145, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.; You, H.; Cai, J.; Zhang, Q.; Yan, S.; You, R. Physically crosslinked silk fibroin/hyaluronic acid scaffolds. Carbohydr. Polym. 2020, 239, 116232. [Google Scholar] [CrossRef]
- Casale, J.; Crane, J.S. Biochemistry, Glycosaminoglycans. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- De Francesco, F.; Saparov, A.; Riccio, M. Hyaluronic acid accelerates re-epithelialization and healing of acute cutaneous wounds. Eur. Rev. Med. Pharmacol. Sci. 2023, 7, 37–45. [Google Scholar] [CrossRef]
- Menezes, R.; Vincent, R.; Osorno, L.; Hu, P.; Arinzeh, T.L. Biomaterials and tissue engineering approaches using glycosaminoglycans for tissue repair: Lessons learned from the native extracellular matrix. Acta Biomater. 2023, 163, 210–227. [Google Scholar] [CrossRef]
- Henrotin, Y.; Raman, R.; Richette, P.; Bard, H.; Jerosch, J.; Conrozier, T.; Chevalier, X.; Migliore, A. Consensus statement on viscosupplementation with hyaluronic acid for the management of osteoarthritis. Semin. Arthritis Rheum. 2015, 45, 140–149. [Google Scholar] [CrossRef]
- Filardo, G.; Di Matteo, B.; Di Martino, A.; Merli, M.L.; Cenacchi, A.; Fornasari, P.; Marcacci, M.; Kon, E. Platelet-Rich Plasma Intra-articular Knee Injections Show No Superiority Versus Viscosupplementation: A Randomized Controlled Trial. Am. J. Sports Med. 2015, 43, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.D.; Manjoo, A.; Fierlinger, A.; Niazi, F.; Nicholls, M. The mechanism of action for hyaluronic acid treatment in the osteoarthritic knee: A systematic review. BMC Musculoskelet. Disord. 2015, 16, 321. [Google Scholar] [CrossRef] [PubMed]
- Daheshia, M.; Yao, J.Q. The interleukin 1beta pathway in the pathogenesis of osteoarthritis. J. Rheumatol. 2008, 35, 2306–2312. [Google Scholar] [CrossRef] [PubMed]
- Genasetti, A.; Vigetti, D.; Viola, M.; Karousou, E.; Moretto, P.; Rizzi, M.; Bartolini, B.; Clerici, M.; Pallotti, F.; De Luca, G.; et al. Hyaluronan and human endothelial cell behavior. Connect. Tissue Res. 2008, 49, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, E.; Roth, M.; Karakiulakis, G. Hyaluronic acid: A key molecule in skin aging. Dermatoendocrinol 2012, 4, 253–258. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, T.E.; Bannuru, R.R. Osteoarthritis: Is viscosupplementation really so unsafe for knee OA? Nat. Rev. Rheumatol. 2012, 8, 635–636. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Hoselton, S.A.; Dorsam, G.P.; Schuh, J.M. Hyaluronan fragments as mediators of inflammation in allergic pulmonary disease. Immunobiology 2015, 220, 575–588. [Google Scholar] [CrossRef]
- Johnson, P.; Arif, A.A.; Lee-Sayer, S.S.M.; Dong, Y. Hyaluronan and Its Interactions With Immune Cells in the Healthy and Inflamed Lung. Front. Immunol. 2018, 9, 2787. [Google Scholar] [CrossRef]
- Parnigoni, A.; Viola, M.; Karousou, E.; Rovera, S.; Giaroni, C.; Passi, A.; Vigetti, D. Hyaluronan in pathophysiology of vascular diseases: Specific roles in smooth muscle cells, endothelial cells, and macrophages. Am. J. Physiol. Cell Physiol. 2022, 323, C505–C519. [Google Scholar] [CrossRef]
- Naor, D. Interaction Between Hyaluronic Acid and Its Receptors (CD44, RHAMM) Regulates the Activity of Inflammation and Cancer. Front. Immunol. 2016, 8, 39. [Google Scholar] [CrossRef]
- Leng, Y.; Abdullah, A.; Wendt, M.; Calve, S. Hyaluronic acid, CD44 and RHAMM regulate myoblast behavior during embryogenesis. Matrix Biol. 2019, 78–79, 236–254. [Google Scholar] [CrossRef] [PubMed]
- Hackett, T.L.; Osei, E.T. Modeling Extracellular Matrix-Cell Interactions in Lung Repair and Chronic Disease. Cells 2021, 10, 2145. [Google Scholar] [CrossRef] [PubMed]
- Ambili, M.; Sudhakaran, P.R. Modulation of neutral matrix metalloproteinases of involuting rat mammary gland by different cations and glycosaminoglycans. J. Cell Biochem. 1999, 73, 218–226. [Google Scholar] [CrossRef]
- Yung, S.; Chan, T.M. Hyaluronan-regulator and initiator of peritoneal inflammation and remodeling. Int. J. Artif. Organs 2007, 30, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Lierova, A.; Kasparova, J.; Filipova, A.; Cizkova, J.; Pekarova, L.; Korecka, L.; Mannova, N.; Bilkova, Z.; Sinkorova, Z. Hyaluronic Acid: Known for Almost a Century, but Still in Vogue. Z. Pharm. 2022, 14, 838. [Google Scholar] [CrossRef] [PubMed]
- Amorim, S.; Reis, C.A.; Reis, R.L.; Pires, R.A. Extracellular Matrix Mimics Using Hyaluronan-Based Biomaterials. Trends Biotechnol. 2021, 39, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Reitinger, S.; Lepperdinger, G. Hyaluronan, a ready choice to fuel regeneration: A mini-review. Gerontology 2013, 59, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Knudson, C.B.; Toole, B.P. Hyaluronate-cell interactions during differentiation of chick embryo limb mesoderm. Dev. Biol. 1987, 124, 82–90. [Google Scholar] [CrossRef]
- Bastow, E.R.; Byers, S.; Golub, S.B.; Clarkin, C.E.; Pitsillides, A.A.; Fosang, A.J. Hyaluronan synthesis and degradation in cartilage and bone. Cell Mol. Life Sci. 2008, 65, 395–413. [Google Scholar] [CrossRef]
- Legouffe, R.; Jeanneton, O.; Gaudin, M.; Tomezyk, A.; Gerstenberg, A.; Dumas, M.; Heusèle, C.; Bonnel, D.; Stauber, J.; Schnebert, S. Hyaluronic acid detection and relative quantification by mass spectrometry imaging in human skin tissues. Anal. Bioanal. Chem. 2022, 414, 5781–5791. [Google Scholar] [CrossRef]
- Laurent, T.C.; Laurent, U.B.; Fraser, J.R. The structure and function of hyaluronan: An overview. Immunol. Cell Biol. 1996, 74, A1–A7. [Google Scholar] [CrossRef] [PubMed]
- Deguine, V.; Labat-Robert, J.; Ferrari, P.; Pouliquen, Y.; Menasche, M.; Robert, L. Aging of the vitreous body. Role of glycation and free radicals. Pathol. Biol. 1997, 45, 321–330. (In French) [Google Scholar] [PubMed]
- Klein, J.; Meyer, F.A. Tissue structure and macromolecular diffusion in umbilical cord. Immobilization of endogenous hyaluronic acid. Biochim. Biophys. Acta 1983, 755, 400–411. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Gastelum, N.S.; Nguyen, Q.T.; Schumacher, B.L.; Sah, R.L. Boundary lubrication of articular cartilage: Role of synovial fluid constituents. Arthritis Rheum. 2007, 56, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Mederake, M.; Trappe, D.; Jacob, C.; Hofmann, U.K.; Schüll, D.; Dalheimer, P.; Exner, L.; Walter, C. Influence of hyaluronic acid on intra-articular friction—A biomechanical study in whole animal joints. BMC Musculoskelet. Disord. 2022, 23, 927. [Google Scholar] [CrossRef] [PubMed]
- Kosinska, M.K.; Ludwig, T.E.; Liebisch, G.; Zhang, R.; Siebert, H.C.; Wilhelm, J.; Kaesser, U.; Dettmeyer, R.B.; Klein, H.; Ishaque, B.; et al. Articular Joint Lubricants during Osteoarthritis and Rheumatoid Arthritis Display Altered Levels and Molecular Species. PLoS ONE 2015, 10, e0125192. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Sai, S.; Marumo, K.; Tanaka, T.; Itano, N.; Kimata, K.; Fujii, K. Expression analysis of three isoforms of hyaluronan synthase and hyaluronidase in the synovium of knees in osteoarthritis and rheumatoid arthritis by quantitative real-time reverse transcriptase polymerase chain reaction. Arthritis Res. Ther. 2004, 6, R514–R520. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Nishida, Y.; Koike, H.; Ito, K.; Zhuo, L.; Nishida, K.; Kimata, K.; Ikuta, K.; Sakai, T.; Urakawa, H.; et al. Hyaluronan in articular cartilage: Analysis of hip osteoarthritis and osteonecrosis of femoral head. J. Orthop. Res. 2023, 41, 307–315. [Google Scholar] [CrossRef]
- Papaneophytou, C.; Alabajos-Cea, A.; Viosca-Herrero, E.; Calvis, C.; Costa, M.; Christodoulides, A.E.; Kroushovski, A.; Lapithis, A.; Lapithi, V.; Papayiannis, I.; et al. Associations between serum biomarkers of cartilage metabolism and serum hyaluronic acid, with risk factors, pain categories, and disease severity in knee osteoarthritis: A pilot study. BMC Musculoskelet. Disord. 2022, 23, 195. [Google Scholar] [CrossRef]
- Sun, Z.P.; Wu, S.P.; Liang, C.D.; Zhao, C.X.; Sun, B.Y. The synovial fluid neuropeptide PACAP may act as a protective factor during disease progression of primary knee osteoarthritis and is increased following hyaluronic acid injection. Innate Immun. 2019, 25, 255–264. [Google Scholar] [CrossRef]
- Sasaki, E.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Inoue, R.; Chiba, D.; Fujita, H.; Takahashi, I.; Umeda, T.; Nakaji, S.; et al. Serum hyaluronic acid concentration predicts the progression of joint space narrowing in normal knees and established knee osteoarthritis—A five-year prospective cohort study. Arthritis Res. Ther. 2015, 17, 283. [Google Scholar] [CrossRef] [PubMed]
- Ye, T.; Zhang, W.; Sun, M.; Yang, R.; Song, S.; Mao, Y.; Yao, J.; Yang, X.; Wang, S.; Pan, W. Study on intralymphatic-targeted hyaluronic acid-modified nanoliposome: Influence of formulation factors on the lymphatic targeting. Int. J. Pharm. 2014, 471, 245–257. [Google Scholar] [CrossRef]
- Berenbaum, F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthr. Cartil. 2013, 21, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Xu, K.; Liang, Y.; Du, P.; Wan, S.; Jiang, C. Effect of hyaluronic acid on cytokines and immune cells change in patients of knee osteoarthritis. BMC Musculoskelet. Disord. 2022, 23, 812. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.H.; Lu, P.W.; Lin, C.W.; Lu, E.W.; Yang, S.F. Different molecular weights of hyaluronan research in knee osteoarthritis: A state-of-the-art review. Matrix Biol. 2023, 117, 46–71. [Google Scholar] [CrossRef] [PubMed]
- Bayer, I.S. Hyaluronic Acid and Controlled Release: A Review. Molecules 2020, 25, 2649. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, M.; Kakehi, K. Analysis of the interaction between hyaluronan and hyaluronan-binding proteins by capillary affinity electrophoresis: Significance of hyaluronan molecular size on binding reaction. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2005, 816, 289–295. [Google Scholar] [CrossRef]
- Mizrahy, S.; Raz, S.R.; Hasgaard, M.; Liu, H.; Soffer-Tsur, N.; Cohen, K.; Dvash, R.; Landsman-Milo, D.; Bremer, M.G.; Moghimi, S.M.; et al. Hyaluronan-coated nanoparticles: The influence of the molecular weight on CD44-hyaluronan interactions and on the immune response. J. Control. Release 2011, 156, 231–238. [Google Scholar] [CrossRef]
- Guo, Y.; Wei, T.; Hu, N.; Zhou, X. Disrupted homeostasis of synovial hyaluronic acid and its associations with synovial mast cell proteases of rheumatoid arthritis patients and collagen-induced arthritis rats. Immunol. Res. 2021, 69, 584–593. [Google Scholar] [CrossRef]
- Goto, M.; Hosako, Y.; Katayama, M.; Yamada, T. Biochemical analysis of rheumatoid synovial fluid after serial intra-articular injection of high molecular weight sodium hyaluronate. Int. J. Clin. Pharmacol. Res. 1993, 13, 161–166. [Google Scholar]
- Poole, A.R.; Dieppe, P. Biological markers in rheumatoid arthritis. Semin. Arthritis Rheum. 1994, 23 (Suppl. S2), 17–31. [Google Scholar] [CrossRef] [PubMed]
- Chang, X.; Yamada, R.; Yamamoto, K. Inhibition of antithrombin by hyaluronic acid may be involved in the pathogenesis of rheumatoid arthritis. Arthritis Res. Ther. 2005, 7, R268–R273. [Google Scholar] [CrossRef] [PubMed]
- Butler, D.M.; Vitti, G.F.; Leizer, T.; Hamilton, J.A. Stimulation of the hyaluronic acid levels of human synovial fibroblasts by recombinant human tumor necrosis factor alpha, tumor necrosis factor beta (lymphotoxin), interleukin-1 alpha, and interleukin-1 beta. Arthritis Rheum. 1988, 31, 1281–1289. [Google Scholar] [CrossRef] [PubMed]
- Pásztói, M.; Nagy, G.; Géher, P.; Lakatos, T.; Tóth, K.; Wellinger, K.; Pócza, P.; György, B.; Holub, M.C.; Kittel, A.; et al. Gene expression and activity of cartilage degrading glycosidases in human rheumatoid arthritis and osteoarthritis synovial fibroblasts. Arthritis Res. Ther. 2009, 11, R68. [Google Scholar] [CrossRef]
- Wollheim, F.A. Predictors of joint damage in rheumatoid arthritis. APMIS 1996, 104, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Olsson, M.; Bremer, L.; Aulin, C.; Harris, H.E. Fragmented hyaluronan has no alarmin function assessed in arthritis synovial fibroblast and chondrocyte cultures. Innate Immun. 2018, 24, 131–141. [Google Scholar] [CrossRef]
- Fujii, K.; Tanaka, Y.; Hübscher, S.; Saito, K.; Ota, T.; Eto, S. Crosslinking of CD44 on rheumatoid synovial cells augment interleukin 6 production. Lab. Investig. 1999, 79, 1439–1446. [Google Scholar] [PubMed]
- Hashizume, M.; Mihara, M. High molecular weight hyaluronic acid inhibits IL-6-induced MMP production from human chondrocytes by up-regulating the ERK inhibitor, MKP-1. Biochem. Biophys. Res. Commun. 2010, 403, 184–189. [Google Scholar] [CrossRef]
- Brondello, J.M.; Djouad, F.; Jorgensen, C. Where to Stand with Stromal Cells and Chronic Synovitis in Rheumatoid Arthritis? Cells 2019, 8, 1257. [Google Scholar] [CrossRef]
- Shiozawa, S.; Yoshihara, R.; Kuroki, Y.; Fujita, T.; Shiozawa, K.; Imura, S. Pathogenic importance of fibronectin in the superficial region of articular cartilage as a local factor for the induction of pannus extension on rheumatoid articular cartilage. Ann. Rheum. Dis. 1992, 51, 869–873. [Google Scholar] [CrossRef]
- Al-Sharif, A.; Jamal, M.; Zhang, L.X.; Larson, K.; Schmidt, T.A.; Jay, G.D.; Elsaid, K.A. Lubricin/Proteoglycan 4 Binding to CD44 Receptor: A Mechanism of the Suppression of Proinflammatory Cytokine-Induced Synoviocyte Proliferation by Lubricin. Arthritis Rheumatol. 2015, 67, 1503–1513. [Google Scholar] [CrossRef] [PubMed]
- Campo, G.M.; Avenoso, A.; D’Ascola, A.; Prestipino, V.; Scuruchi, M.; Nastasi, G.; Calatroni, A.; Campo, S. The stimulation of adenosine 2A receptor reduces inflammatory response in mouse articular chondrocytes treated with hyaluronan oligosaccharides. Matrix Biol. 2012, 31, 338–351. [Google Scholar] [CrossRef] [PubMed]
- Saxne, T.; Heinegård, D. Synovial fluid analysis of two groups of proteoglycan epitopes distinguishes early and late cartilage lesions. Arthritis Rheum. 1992, 35, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Migliore, A.; Paoletta, M.; Moretti, A.; Liguori, S.; Iolascon, G. The perspectives of intra-articular therapy in the management of osteoarthritis. Expert. Opin. Drug Deliv. 2020, 17, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Giji, S.; Arumugam, M. Isolation and characterization of hyaluronic acid from marine organisms. Adv. Food Nutr. Res. 2014, 72, 61–77. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.W.; Chang, M.J.; Shin, C.Y.; Chang, C.B.; Kang, S.B. A randomized controlled trial for comparing efficacy and safety between intraarticular polynucleotide and hyaluronic acid for knee osteoarthritis treatment. Sci. Rep. 2023, 13, 9419. [Google Scholar] [CrossRef]
- Da Silva, T.Z.; de Oliveira, A.C.; Margonar, R.; Faeda, R.S.; Dos Santos, P.L.; Queiroz, T.P. Effectiveness of Hyaluronic Acid Injection for Interdental Papillae Recovery in Esthetic Areas: A Randomized Clinical Trial. Int. J. Periodontics Restor. Dent. 2023, 43, e73–e80. [Google Scholar] [CrossRef]
- Alam, M.M.; Han, H.S.; Sung, S.; Kang, J.H.; Sa, K.H.; Al Faruque, H.; Hong, J.; Nam, E.J.; Kim, I.S.; Park, J.H.; et al. Endogenous inspired biomineral-installed hyaluronan nanoparticles as pH-responsive carrier of methotrexate for rheumatoid arthritis. J. Control. Release 2017, 252, 62–72. [Google Scholar] [CrossRef]
- Jiao, Y.; Pang, X.; Zhai, G. Advances in Hyaluronic Acid-Based Drug Delivery Systems. Curr. Drug Targets 2016, 17, 720–730. [Google Scholar] [CrossRef]
- Yang, L.; Liu, Y.; Shou, X.; Ni, D.; Kong, T.; Zhao, Y. Bio-inspired lubricant drug delivery particles for the treatment of osteoarthritis. Nanoscale 2020, 12, 17093–17102. [Google Scholar] [CrossRef]
- Kotla, N.G.; Bonam, S.R.; Rasala, S.; Wankar, J.; Bohara, R.A.; Bayry, J.; Rochev, Y.; Pandit, A. Recent advances and prospects of hyaluronan as a multifunctional therapeutic system. J. Control. Release 2021, 10, 598–620. [Google Scholar] [CrossRef] [PubMed]
- Dovedytis, M.; Liu, Z.J.; Bartlett, S. Hyaluronic acid and its biomedical applications: A review. Eng. Regen. 2020, 1, 102–113. [Google Scholar] [CrossRef]
- Oo, W.M.; Hunter, D.J. Efficacy, Safety, and Accuracy of Intra-articular Therapies for Hand Osteoarthritis: Current Evidence. Drugs Aging 2023, 40, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Honvo, G.; Reginster, J.Y.; Rannou Geerink, A.; Rabenda, V.; McAlindon, T.; Charles, A.A.; Fuggle, N.; Cooper, C.; Curtis, E.; Arden, N.; et al. Safety of Intra-articular Hyaluronic Acid Injections in Osteoarthritis: Outcomes of a Systematic Review and Meta-Analysis. Drugs Aging 2019, 36, 101–127. [Google Scholar] [CrossRef] [PubMed]
- Snetkov, P.; Zakharova, K.; Morozkina, S.; Olekhnovich, R.; Uspenskaya, M. Hyaluronic Acid: The Influence of Molecular Weight on Structural, Physical, Physico-Chemical, and Degradable Properties of Biopolymer. Polymers 2020, 12, 1800. [Google Scholar] [CrossRef] [PubMed]
- Chistyakov, D.V.; Astakhova, A.A.; Azbukina, N.V.; Goriainov, S.V.; Chistyakov, V.V.; Sergeeva, M.G. High and Low Molecular Weight Hyaluronic Acid Differentially Influences Oxylipins Synthesis in Course of Neuroinflammation. Int. J. Mol. Sci. 2019, 20, 3894. [Google Scholar] [CrossRef] [PubMed]
- Petrella, R.J.; Cogliano, A.; Decaria, J. Combining two hyaluronic acids in osteoarthritis of the knee: A randomized, double-blind, placebo-controlled trial. Clin. Rheumatol. 2008, 27, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Hamburger, M.I.; Lakhanpal, S.; Mooar, P.A.; Oster, D. Intra-articular hyaluronans: A review of product-specific safety profiles. Semin. Arthritis Rheum. 2003, 32, 296–309. [Google Scholar] [CrossRef]
- Uson, J.; Rodriguez-García, S.C.; Castellanos-Moreira, R.; O’Neill, T.W.; Doherty, M.; Boesen, M.; Pandit, H.; Möller Parera, I.; Vardanyan, V.; Terslev, L.; et al. EULAR recommendations for intra-articular therapies. Ann. Rheum. Dis. 2021, 80, 1299–1305. [Google Scholar] [CrossRef]
- Burns, J.W.; Kraines, J.L.; Magilavy, D.B.; Murray, C.W.; Richards, S.M. Response to: Identification of an immunogenic candidate for the elicitation of severe acute inflammatory reactions (SAIRs) to hylan G-F 20. Osteoarthr. Cartil. 2005, 13, 1128–1129. [Google Scholar] [CrossRef]
- Shen, D.; Chen, M.; Chen, K.; Wang, T.; Lu, L.; Yang, X. Efficacy of hyaluronic acid after knee arthroscopy: A systematic review and meta-analysis. J. Rehabil. Med. 2018, 50, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Najm, A.; Alunno, A.; Gwinnutt, J.M.; Weill, C.; Berenbaum, F. Efficacy of intra-articular corticosteroid injections in knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Jt. Bone Spine 2021, 88, 105198. [Google Scholar] [CrossRef] [PubMed]
- Conrozier, T.; Raman, R.; Chevalier, X.; Henrotin, Y.; Monfort, J.; Diraçoglù, D.; Bard, H.; Baron, D.; Jerosch, J.; Richette, P.; et al. Viscosupplementation for the treatment of osteoarthritis. The contribution of EUROVISCO group. Ther. Adv. Musculoskelet. Dis. 2021, 28, 1759720X211018605. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, X.; Sheehan, B.; Whittington, C.; Pourrahmat, M.M.; Duarte, L.; Ngai, W.; de Campos, G.C. Efficacy and Safety of Hylan G-F 20 Versus Intra-Articular Corticosteroids in People with Knee Osteoarthritis: A Systematic Review and Network Meta-Analysis. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2020, 13, 1179544120967370. [Google Scholar] [CrossRef]
- Barry, F.; Chai, F.; Chijcheapaza-Flores, H.; Garcia-Fernandez, M.J.; Blanchemain, N.; Nicot, R.J. Systematic review of studies on drug-delivery systems for management of temporomandibular-joint osteoarthritis. Stomatol. Oral. Maxillofac. Surg. 2022, 123, e336–e341. [Google Scholar] [CrossRef]
- Zewail, M.; Nafee, N.; Helmy, M.W.; Boraie, N. Synergistic and receptor-mediated targeting of arthritic joints via intra-articular injectable smart hydrogels containing leflunomide-loaded lipid nanocarriers. Drug Deliv. Transl. Res. 2021, 11, 2496–2519. [Google Scholar] [CrossRef]
- Barron, M.C.; Rubin, B.R. Managing osteoarthritic knee pain. J. Am. Osteopath. Assoc. 2007, 107 (Suppl. S6), ES21–ES27. [Google Scholar]
- Oliviero, F.; Ramonda, R.; Hoxha, A.; Scanu, A.; Galozzi, P.; Favero, M.; Frallonardo, P.; Punzi, L. Effect of an oral preparation containing hyaluronic acid, chondroitin sulfate, hydrolyzed collagen type II and hydrolyzed keratin on synovial fluid features and clinical indices in knee osteoarthritis. A pilot study. Reumatismo 2020, 72, 125–130. [Google Scholar] [CrossRef]
- Mannino, F.; Irrera, N.; Pallio, G.; Bitto, A. Steady state plasma and tissue distribution of low molecular weight hyaluronic acid after oral administration in mice. Nat. Prod. Res. 2023, 20, 1–8. [Google Scholar] [CrossRef]
- Yagi, H.; Tomono, T.; Handa, Y.; Saito, N.; Ukawa, M.; Miyata, K.; Shigeno, K.; Sakuma, S. Performance of Cell-Penetrating Peptides Anchored to Polysaccharide Platforms Applied via Various Mucosal Routes as an Absorption Enhancer. Mol. Pharm. 2023, 20, 303–313. [Google Scholar] [CrossRef]
- Bowden, D.J.; Eustace, S.J.; Kavanagh, E.C. The value of injectable viscoelastic supplements for joints. Skelet. Radiol. 2023, 52, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.D.; Akermark, C.; Beaulieu, A.D.; Schnitzer, T. Efficacy and safety of a single intra-articular injection of non-animal stabilized hyaluronic acid (NASHA) in patients with osteoarthritis of the knee. Durolane International Study Group. Osteoarthr. Cartil. 2004, 12, 642–649. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Natov, N.S.; Obadan, I.E.; Price, L.L.; Schmid, C.H.; McAlindon, T.E. Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: A systematic review and meta-analysis. Arthritis Rheum. 2009, 61, 1704–1711. [Google Scholar] [CrossRef] [PubMed]
- Rutjes, A.W.; Jüni, P.; da Costa, B.R.; Trelle, S.; Nüesch, E.; Reichenbach, S. Viscosupplementation for osteoarthritis of the knee: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Schmid, C.H.; Kent, D.M.; Vaysbrot, E.E.; Wong, J.B.; McAlindon, T.E. Comparative effectiveness of pharmacologic interventions for knee osteoarthritis: A systematic review and network meta-analysis. Ann. Intern. Med. 2015, 162, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Frisbie, D.D.; McIlwraith, C.W.; Kawcak, C.E.; Werpy, N.M. Efficacy of intravenous administration of hyaluronan, sodium chondroitin sulfate, and N-acetyl-d-glucosamine for prevention or treatment of osteoarthritis in horses. Am. J. Vet. Res. 2016, 77, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.T.; Lee, J.; Kim, M.H.; Park, J.H.; Lee, J.Y.; Song, J.H.; Jung, M.; Jang, M.H.; Cho, H.J.; Yoon, I.S.; et al. Novel reverse electrodialysis-driven iontophoretic system for topical and transdermal delivery of poorly permeable therapeutic agents. Drug Deliv. 2017, 24, 1204–1215. [Google Scholar] [CrossRef]
- Ho, S.S.; Murphy, K.C.; Binder, B.Y.; Vissers, C.B.; Leach, J.K. Increased Survival and Function of Mesenchymal Stem Cell Spheroids Entrapped in Instructive Alginate Hydrogels. Stem Cells Transl. Med. 2016, 5, 773–781. [Google Scholar] [CrossRef]
- He, Z.; Wang, B.; Hu, C.; Zhao, J. An overview of hydrogel-based intra-articular drug delivery for the treatment of osteoarthritis. Colloids Surf. B Biointerfaces 2017, 154, 33–39. [Google Scholar] [CrossRef]
- Deligianni, D.D.; Katsala, N.D.; Koutsoukos, P.G.; Missirlis, Y.F. Effect of surface roughness of hydroxyapatite on human bone marrow cell adhesion, proliferation, differentiation and detachment strength. Biomaterials 2001, 22, 87–96. [Google Scholar] [CrossRef]
- Moutos, F.T.; Guilak, F. Composite scaffolds for cartilage tissue engineering. Biorheology 2008, 45, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Fang, F.; Kong, Y.; Greer, S.E.; Kuss, M.; Liu, B.; Xue, W.; Jiang, X.; Lovell, P.; Mohs, A.M.; et al. Dynamic hyaluronic acid hydrogel with covalent linked gelatin as an anti-oxidative bioink for cartilage tissue engineering. Biofabrication 2021, 14, 014107. [Google Scholar] [CrossRef] [PubMed]
- Lahner, M.; Duif, C.; Ficklscherer, A.; Kaps, C.; Kalwa, L.; Seidl, T. Arthroscopic fixation of cell free polymer-based cartilage implants with a bioinspired polymer surface on the hip joint: A cadaveric pilot study. BioMed Res. Int. 2014, 2014, 717912. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Chi, J.; Wang, Y.; Zhao, Y.; Luo, Y.; Wang, Y. Zn-MOF Encapsulated Antibacterial and Degradable Microneedles Array for Promoting Wound Healing. Adv. Healthc. Mater. 2021, 10, e2100056. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Jiang, Q.; Jin, Z.; Chen, D.; Xu, Q.; Chen, J.; Zeng, Y.; Chen, S.; He, Q. Two-Dimensional Mg2 Si Nanosheet-Enabled Sustained Hydrogen Generation for Improved Repair and Regeneration of Deeply Burned Skin. Adv. Healthc. Mater. 2023, 12, e2201705. [Google Scholar] [CrossRef] [PubMed]
- Ottonelli, I.; Bighinati, A.; Adani, E.; Loll, F.; Caraffi, R.; Vandelli, M.A.; Boury, F.; Tosi, G.; Duskey, J.T.; Marigo, V.; et al. Optimization of an Injectable Hydrogel Depot System for the Controlled Release of Retinal-Targeted Hybrid Nanoparticles. Pharmaceutics 2022, 15, 25. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.; Xing, H.; Sun, Y.; Feng, S.; Wang, S. Non-small cell lung cancer combination therapy: Hyaluronic acid modified, epidermal growth factor receptor targeted, pH sensitive lipid-polymer hybrid nanoparticles for the delivery of erlotinib plus bevacizumab. Biomed. Pharmacother. 2020, 125, 109861. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.Y.; Lin, N.Y.; Wen, C.H.; Lin, C.A.; Venkatesan, P.; Wijerathna, P.; Lin, C.Y.; Lai, P.S. Development of triamcinolone acetonide-hyaluronic acid conjugates with selective targeting and less osteoporosis effect for rheumatoid arthritis treatments. Int. J. Biol. Macromol. 2023, 15, 124047. [Google Scholar] [CrossRef]
- Kim, Y.S.; Guilak, F. Engineering Hyaluronic Acid for the Development of New Treatment Strategies for Osteoarthritis. Int. J. Mol. Sci. 2022, 23, 8662. [Google Scholar] [CrossRef]
- Goldberg, V.M.; Buckwalter, J.A. Hyaluronans in the treatment of osteoarthritis of the knee: Evidence for disease-modifying activity. Osteoarthr. Cartil. 2005, 13, 216–224. [Google Scholar] [CrossRef]
- Ferreira, F.G.; Azzoni, A.R.; Andrade Santana, M.H.; Petrides, D. Techno-Economic Analysis of a Hyaluronic Acid Production Process Utilizing Streptococcal Fermentation. Processes 2021, 9, 241. [Google Scholar] [CrossRef]
- Balazs, E.A.; Denlinger, J.L. Viscosupplementation: A new concept in the treatment of osteoarthritis. J. Rheumatol. Suppl. 1993, 39, 3–9. [Google Scholar]
- Kotla, N.G.; Mohd Isa, I.L.; Larrañaga, A.; Maddiboyina, B.; Swamy, S.K.; Sivaraman, G.; Vemula, P.K. Hyaluronic acid based bioconjugate systems, scaffolds, and their therapeutic potential. Adv. Healthc. Mater. 2023, 12, e2203104. [Google Scholar] [CrossRef]
- Burdick, J.A.; Prestwich, G.D. Hyaluronic acid hydrogels for biomedical applications. Adv. Mater. 2011, 23, H41–H56. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.-Z.; Wu, D.-Y.; Chang, Q.; Guo, Y.-D.; Wang, C.; Fan, W.-M. Intra-articular, single-shot co-injection of hyaluronic acid and corticosteroids in knee osteoarthritis: A randomized controlled trial. Exp. Ther. Med. 2018, 16, 1928–1934. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Campbell, J.; Robinson, V.; Gee, T.; Bourne, R.; Wells, G. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database Syst. Rev. 2006, 2, CD005328, Update in: Cochrane Database Syst Rev. 2015, 10, CD005328. [Google Scholar] [CrossRef]
- Smith, C.; Patel, R.; Vannabouathong, C.; Sales, B.; Rabinovich, A.; McCormack, R.; L Belzile, E.; Bhandari, M. Combined intra-articular injection of corticosteroid and hyaluronic acid reduces pain compared to hyaluronic acid alone in the treatment of knee osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1974–1983. [Google Scholar] [CrossRef]
- Miller, L.E.; Fredericson, M.; Altman, R.D. Hyaluronic Acid Injections or Oral Nonsteroidal Anti-inflammatory Drugs for Knee Osteoarthritis: Systematic Review and Meta-analysis of Randomized Trials. Orthop. J. Sports Med. 2020, 8, 2325967119897909. [Google Scholar] [CrossRef]
- Euppayo, T.; Punyapornwithaya, V.; Chomdej, S.; Ongchai, S.; Nganvongpanit, K. Effects of hyaluronic acid combined with anti-inflammatory drugs compared with hyaluronic acid alone, in clinical trials and experiments in osteoarthritis: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2017, 18, 387. [Google Scholar] [CrossRef]
- Lin, X.; Zhi, F.; Lan, Q.; Deng, W.; Hou, X.; Wan, Q. Comparing the efficacy of different intra-articular injections for knee osteoarthritis: A network analysis. Medicine 2022, 101, e29655. [Google Scholar] [CrossRef]
- Zhao, J.; Huang, H.; Liang, G.; Zeng, L.F.; Yang, W.; Liu, J. Effects and safety of the combination of platelet-rich plasma (PRP) and hyaluronic acid (HA) in the treatment of knee osteoarthritis: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2020, 21, 224. [Google Scholar] [CrossRef] [PubMed]
- Pereira, H.; Sousa, D.A.; Cunha, A.; Andrade, R.; Espregueira-Mendes, J.; Oliveira, J.M.; Reis, R.L. Hyaluronic Acid. Adv. Exp. Med. Biol. 2018, 1059, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Toropitsyn, E.; Pravda, M.; Rebenda, D.; Ščigalková, I.; Vrbka, M.; Velebný, V. A composite device for viscosupplementation treatment resistant to degradation by reactive oxygen species and hyaluronidase. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 2595–2611. [Google Scholar] [CrossRef] [PubMed]
- Arslan, E.; Sardan Ekiz, M.; Eren Cimenci, C.; Can, N.; Gemci, M.H.; Ozkan, H.; Guler, M.; Tekinay, A.B. Protective therapeutic effects of peptide nanofiber and hyaluronic acid hybrid membrane in in vivo osteoarthritis model. Acta Biomater. 2018, 73, 263–274. [Google Scholar] [CrossRef]
- Litwiniuk, M.; Krejner, A.; Speyrer, M.; Gauto, A.R.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration. Wounds 2016, 28, 78–88. [Google Scholar] [PubMed]
- Abatangelo, G.; Vindigni, V.; Avruscio, G.; Pandis, L.; Brun, P. Hyaluronic Acid: Redefining Its Role. Cells 2020, 21, 1743. [Google Scholar] [CrossRef]
- Grieco, M.; Ursini, O.; Palamà, I.E.; Gigli, G.; Moroni, L.; Cortese, B. HYDRHA: Hydrogels of hyaluronic acid. New biomedical approaches in cancer, neurodegenerative diseases, and tissue engineering. Mater. Today Bio 2022, 17, 100453. [Google Scholar] [CrossRef] [PubMed]
- Rui, K.; Tang, X.; Shen, Z.; Jiang, C.; Zhu, Q.; Liu, S.; Che, N.; Tian, J.; Ling, J.; Yang, Y. Exosome inspired photo-triggered gelation hydrogel composite on modulating immune pathogenesis for treating rheumatoid arthritis. J. Nanobiotechnol. 2023, 21, 111. [Google Scholar] [CrossRef]
- Xuan, H.; Tang, X.; Zhu, Y.; Ling, J.; Yang, Y. Freestanding Hyaluronic Acid/Silk-Based Self-healing Coating toward Tissue Repair with Antibacterial Surface. ACS Appl. Bio Mater. 2020, 3, 1628–1635. [Google Scholar] [CrossRef]
Figure 1.
Skeletal formula of hyaluronan—a polymer consisting of D-glucuronic acid and N-acetyl-D-glucosamine linked via alternating β-(1→4) and β-(1→3) glycosidic bonds [7].
Figure 1.
Skeletal formula of hyaluronan—a polymer consisting of D-glucuronic acid and N-acetyl-D-glucosamine linked via alternating β-(1→4) and β-(1→3) glycosidic bonds [7].

Table 1.
Physiological functions of hyaluronic acid (HA) in rheumatology.
| Function | Mechanisms | References |
|---|---|---|
| Lubrication of joints | HA provides lubrication and viscoelastic properties to synovial fluid, reducing friction between joint surfaces and enhancing joint mobility. | [44] |
| Chondroprotection | HA exhibits chondroprotective effects by promoting cartilage matrix synthesis, reducing matrix degradation, and inhibiting the activity of proteolytic enzymes | [45,46] |
| Anti-inflammatory activity | HA can modulate inflammation by reducing the expression of pro-inflammatory cytokines and enzymes, inhibiting leukocyte migration, and suppressing immune responses. | [47,48] |
| Tissue repair and remodeling | HA plays a role in tissue repair and remodeling processes by promoting cell migration, angiogenesis, and extracellular matrix remodeling | [44,49] |
| Viscoelasticity | HA contributes to the viscoelastic properties of connective tissues, maintaining tissue integrity, elasticity, and shock-absorbing capabilities. | [48,50] |
Selected studies on the physiological role of HA in rheumatology. This is not an exhaustive list, and further research and clinical trials have been conducted in this field. For more detailed information, it is recommended to refer to the referenced papers.
Table 3.
Intra-articular application of hyaluronic acid (HA) in osteoarthritis (OA) and its findings.
Table 3.
Intra-articular application of hyaluronic acid (HA) in osteoarthritis (OA) and its findings.
| Study | Design | Participants | Intervention | Findings | References |
|---|---|---|---|---|---|
| Altman et al. (2004) | Randomized, double-blind, placebo-controlled trial | 495 patients with knee OA | HA injections (3 weekly injections) vs. placebo | HA group showed significant improvement in pain and function compared to placebo | [126] |
| Bannuru et al. (2009) | Meta-analysis | 29 randomized controlled trials | HA injections vs. control interventions (placebo, saline, or NSAIDs) | HA injections were superior to control interventions in reducing pain and improving function in knee OA | [127] |
| Rutjes et al. (2012) | Systematic review and meta-analysis | 76 randomized controlled trials | HA injections vs. control interventions (placebo or no treatment) | HA injections provided significant pain relief and functional improvement compared to control interventions in knee OA | [128] |
| Filardo et al. (2015) | Randomized controlled trial | 160 patients with knee OA | HA injections vs. platelet-rich plasma (PRP) injections | HA and PRP injections showed similar efficacy in reducing pain and improving function in knee osteoarthritis | [45] |
| Bannuru et al. (2015) | Systematic review and meta-analysis | 137 randomized controlled trials | Various HA preparations vs. control interventions (placebo, saline, or corticosteroids) | HA injections were effective in reducing pain and improving function in knee OA with a favourable safety profile | [129] |
Selected clinical studies on the use of intraarticular HA injections in OA. This is not an exhaustive list, and further research and clinical trials have been conducted in this field. For more detailed information, it is recommended to refer to the referenced papers.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sprott, H.; Fleck, C. Hyaluronic Acid in Rheumatology. Pharmaceutics 2023, 15, 2247. https://doi.org/10.3390/pharmaceutics15092247
AMA Style
Sprott H, Fleck C. Hyaluronic Acid in Rheumatology. Pharmaceutics. 2023; 15(9):2247. https://doi.org/10.3390/pharmaceutics15092247
Chicago/Turabian StyleSprott, Haiko, and Christian Fleck. 2023. "Hyaluronic Acid in Rheumatology" Pharmaceutics 15, no. 9: 2247. https://doi.org/10.3390/pharmaceutics15092247
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.