
The Evolution and Recent Trends in Acoustic Targeting of Encapsulated Drugs to Solid Tumors: Strategies beyond Sonoporation
Abstract
:1. Introduction
2. Drug Encapsulation and Nanomedicine
2.1. Nanomedicine beyond the EPR Effect
2.2. Improving Delivery by Drug Uncaging
3. Drug Transport in Tumor Tissue
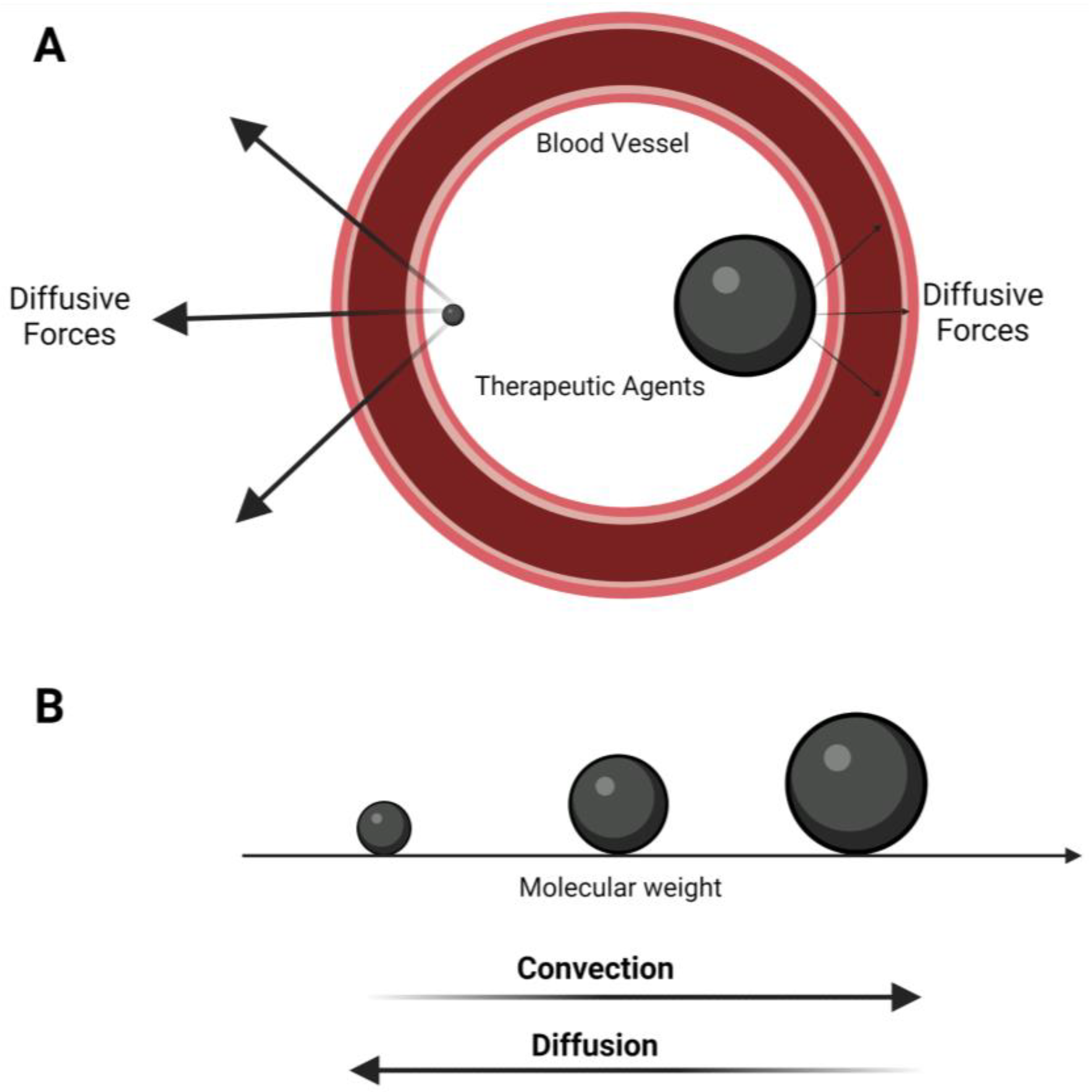
3.1. Convection and Diffusion
3.2. Small Molecule Chemotherapy Delivery
3.3. Drug Encapsulation: Advantages and Challenges with Nanoparticle Drug Delivery
4. Ultrasound and Its Contrast Agents
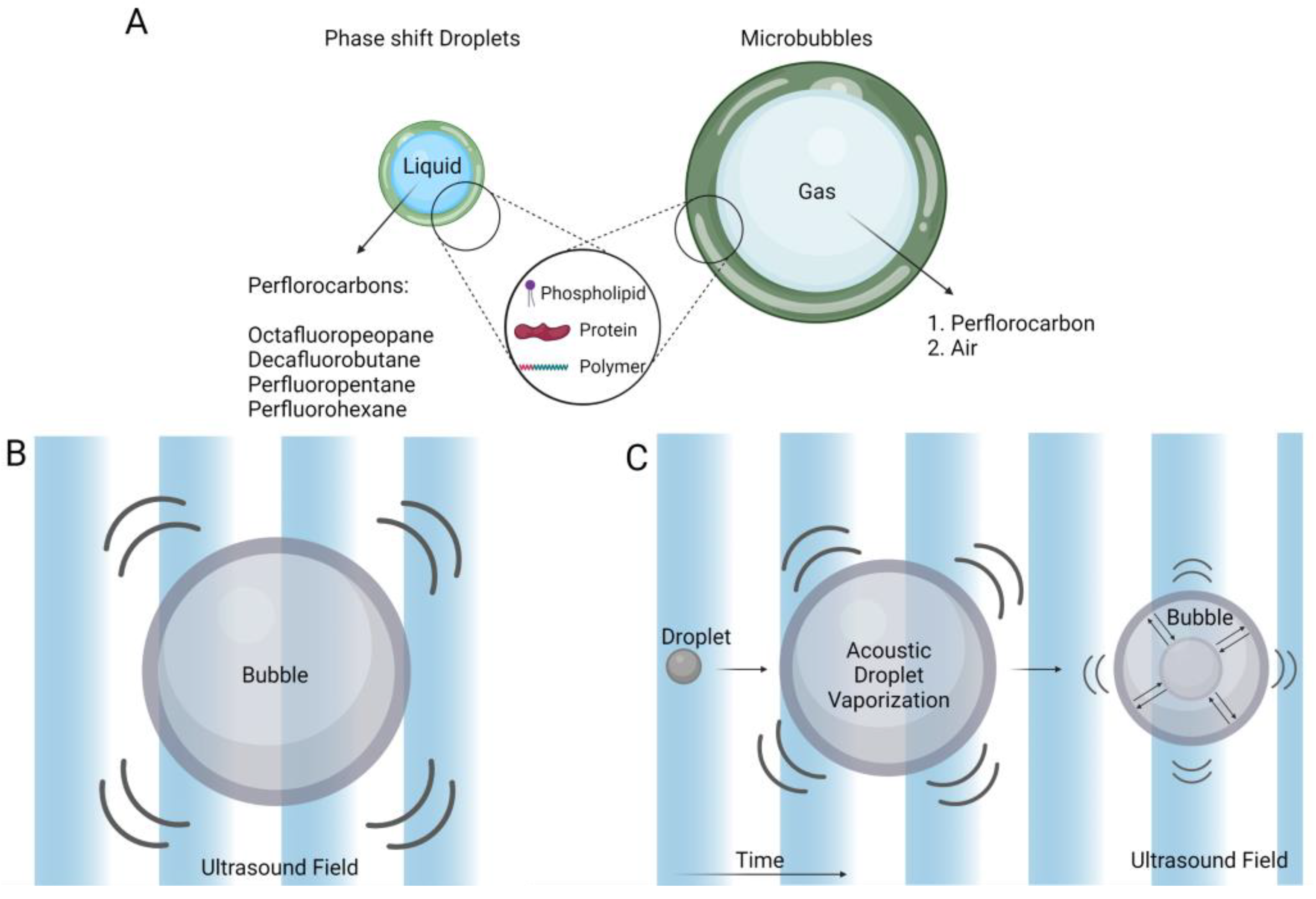
Microbubbles and Phase-Shift Contrast Agents
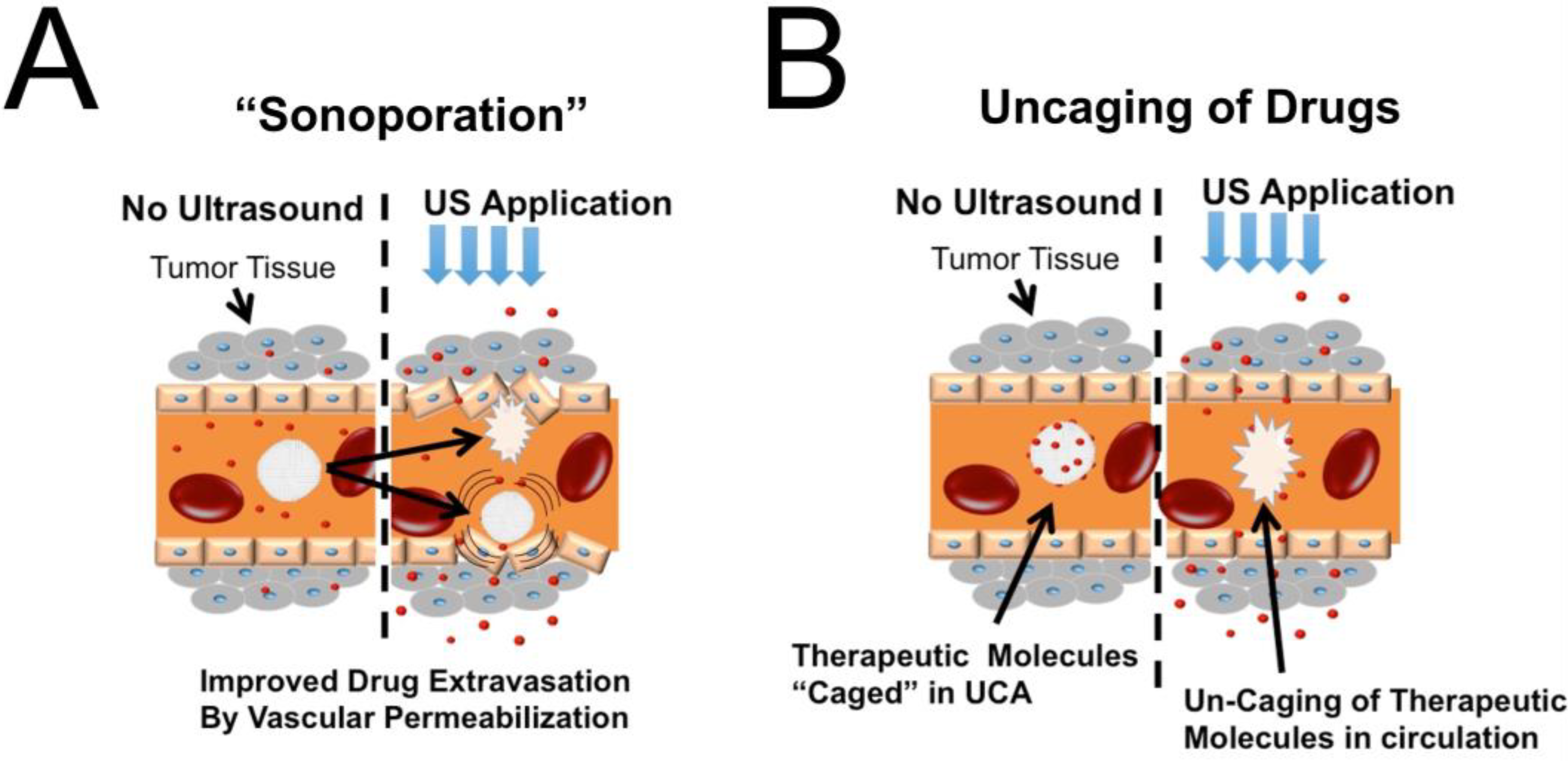
5. Ultrasound-Mediated Drug Delivery
Materials for Ultrasonic Drug Uncaging
6. Emerging Areas with Ultrasonic Drug Uncaging
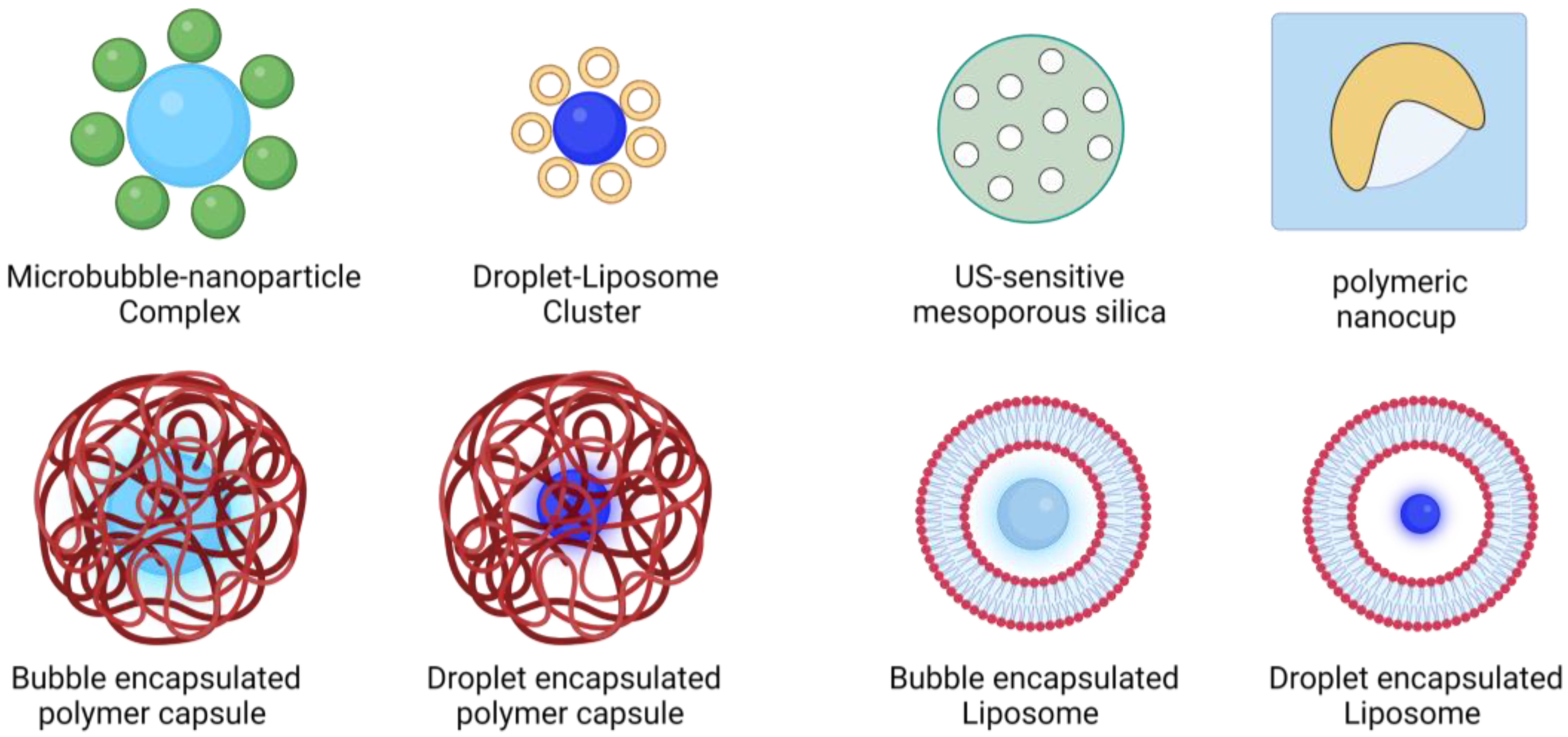
6.1. Incorporating Cavitation Nuclei in Drug-Delivery Vehicles
6.2. Microbubble-Nested Drug Carriers
6.3. Droplet-Nested Drug Carriers
6.4. Nesting Cavitation Nuclei in Solid Drug Carriers
7. Materials for Ultrasound-Sensitive Drug Carriers
7.1. Lipids
7.2. Polymers
8. The Role of Ultrasound Parameters in Drug Vehicle Design
9. Acoustic Radiation Forces in Drug Delivery
10. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Parascandola, J. The Theoretical Basis of Paul Ehrlich’s Chemotherapy. J. Hist. Med. Allied Sci. 1981, 36, 19–43. [Google Scholar] [CrossRef] [PubMed]
- Thorburn, A.L. Paul Ehrlich: Pioneer of Chemotherapy and Cure by Arsenic (1854–1915). Br. J. Vener. Dis. 1983, 59, 404. [Google Scholar] [CrossRef] [PubMed]
- Strebhardt, K.; Ullrich, A. Paul Ehrlich’s Magic Bullet Concept: 100 Years of Progress. Nat. Rev. Cancer 2008, 8, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Groner, B.; Schumacher, U.; Superti-Furga, G.; Busslinger, M.; Kralovics, R.; Zielinski, C.; Penninger, J.M.; Kerjaschki, D.; Stingl, G.; et al. Paul Ehrlich (1854–1915) and His Contributions to the Foundation and Birth of Translational Medicine. J. Innate Immun. 2016, 8, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Ellis, H. Paul Ehrlich: Nobel Laureate and Father of Modern Chemotherapy. Br. J. Hosp. Med. 2015, 76, 483. [Google Scholar] [CrossRef]
- Podczeck, F.; Jones, B.E. Pharmaceutical Capsules; Pharmaceutical Press: London, UK; Chicago, IL, USA, 2004; ISBN 0-85369-568-7. [Google Scholar]
- Park, H.; Otte, A.; Park, K. Evolution of Drug Delivery Systems: From 1950 to 2020 and Beyond. J. Control. Release 2022, 342, 53–65. [Google Scholar] [CrossRef]
- Abu-Thabit, N.Y.; Makhlouf, A.S.H. Historical Development of Drug Delivery Systems: From Conventional Macroscale to Controlled, Targeted, and Responsive Nanoscale Systems. In Stimuli Responsive Polymeric Nanocarriers for Drug Delivery Applications; Woodhead Publishing: Sawston, UK, 2018; Volume 1. [Google Scholar]
- Matsumura, Y.; Maeda, H. A New Concept for Macromolecular Therapeutics in Cancer Chemotherapy: Mechanism of Tumoritropic Accumulation of Proteins and the Antitumor Agent Smancs. Cancer Res. 1986, 46, 6387–6392. [Google Scholar]
- Iyer, A.K.; Khaled, G.; Fang, J.; Maeda, H. Exploiting the Enhanced Permeability and Retention Effect for Tumor Targeting. Drug Discov. Today 2006, 11, 812–818. [Google Scholar] [CrossRef]
- Prabhakar, U.; Maeda, H.; Jain, R.K.; Sevick-Muraca, E.M.; Zamboni, W.; Farokhzad, O.C.; Barry, S.T.; Gabizon, A.; Grodzinski, P.; Blakey, D.C. Challenges and Key Considerations of the Enhanced Permeability and Retention Effect for Nanomedicine Drug Delivery in Oncology. Cancer Res. 2013, 73, 2412–2417. [Google Scholar] [CrossRef] [Green Version]
- Greish, K. Enhanced Permeability and Retention Effect for Selective Targeting of Anticancer Nanomedicine: Are We There Yet? Drug Discov. Today Technol. 2012, 9, e161–e166. [Google Scholar] [CrossRef]
- Huynh, E.; Zheng, G. Cancer Nanomedicine: Addressing the Dark Side of the Enhanced Permeability and Retention Effect. Nanomedicine 2015, 10, 1993–1995. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Mochida, A.; Choyke, P.L.; Kobayashi, H. Nanodrug Delivery: Is the Enhanced Permeability and Retention Effect Sufficient for Curing Cancer? Bioconjugate Chem. 2016, 27, 2225–2238. [Google Scholar] [CrossRef] [PubMed]
- Sriraman, S.K.; Aryasomayajula, B.; Torchilin, V.P. Barriers to Drug Delivery in Solid Tumors. Tissue Barriers 2014, 2, e29528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco, E.; Shen, H.; Ferrari, M. Principles of Nanoparticle Design for Overcoming Biological Barriers to Drug Delivery. Nat. Biotechnol. 2015, 33, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Dewhirst, M.W.; Secomb, T.W. Transport of Drugs from Blood Vessels to Tumour Tissue. Nat. Rev. Cancer 2017, 17, 738–750. [Google Scholar] [CrossRef]
- Kim, S.M.; Faix, P.H.; Schnitzer, J.E. Overcoming Key Biological Barriers to Cancer Drug Delivery and Efficacy. J. Control. Release 2017, 267, 15–30. [Google Scholar] [CrossRef]
- Couvreur, P. Nanoparticles in Drug Delivery: Past, Present and Future. Adv. Drug Deliv. Rev. 2013, 65, 21–23. [Google Scholar] [CrossRef]
- De Jong, W.H.; Borm, P.J.A. Drug Delivery and Nanoparticles:Applications and Hazards. Int. J. Nanomed. 2008, 3, 133–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, R.H.; Shegokar, R.; Keck, C.M. 20 Years of Lipid Nanoparticles (SLN and NLC): Present State of Development and Industrial Applications. Curr. Drug Discov. Technol. 2011, 8, 207–227. [Google Scholar] [CrossRef]
- Hou, X.; Zaks, T.; Langer, R.; Dong, Y. Lipid Nanoparticles for MRNA Delivery. Nat. Rev. Mater. 2021, 6, 1078–1094. [Google Scholar] [CrossRef]
- Wilson, B.; Geetha, K.M. Lipid Nanoparticles in the Development of MRNA Vaccines for COVID-19. J. Drug Deliv. Sci. Technol. 2022, 74, 103553. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Li, J.; Zhao, Q.; Pan, T.; Zhong, H.; Wang, W. Advanced and Innovative Nano-Systems for Anticancer Targeted Drug Delivery. Pharmaceutics 2021, 13, 1151. [Google Scholar] [CrossRef] [PubMed]
- Trucillo, P. Drug Carriers: Classification, Administration, Release Profiles, and Industrial Approach. Processes 2021, 9, 470. [Google Scholar] [CrossRef]
- Shi, J.; Kantoff, P.W.; Wooster, R.; Farokhzad, O.C. Cancer Nanomedicine: Progress, Challenges and Opportunities. Nat. Rev. Cancer 2017, 17, 20–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nehoff, H.; Parayath, N.N.; Domanovitch, L.; Taurin, S.; Greish, K. Nanomedicine for Drug Targeting: Strategies beyond the Enhanced Permeability and Retention Effect. Int. J. Nanomed. 2014, 9, 2539–2555. [Google Scholar] [CrossRef] [Green Version]
- Moradi Kashkooli, F.; Soltani, M.; Souri, M. Controlled Anti-Cancer Drug Release through Advanced Nano-Drug Delivery Systems: Static and Dynamic Targeting Strategies. J. Control. Release 2020, 327, 316–349. [Google Scholar] [CrossRef]
- Srinivasarao, M.; Low, P.S. Ligand-Targeted Drug Delivery. Chem. Rev. 2017, 117, 12133–12164. [Google Scholar] [CrossRef]
- Ojha, T.; Pathak, V.; Shi, Y.; Hennink, W.E.; Moonen, C.T.W.; Storm, G.; Kiessling, F.; Lammers, T. Pharmacological and Physical Vessel Modulation Strategies to Improve EPR-Mediated Drug Targeting to Tumors. Adv. Drug Deliv. Rev. 2017, 119, 44–60. [Google Scholar] [CrossRef] [Green Version]
- Bayat Mokhtari, R.; Homayouni, T.S.; Baluch, N.; Morgatskaya, E.; Kumar, S.; Das, B.; Yeger, H. Combination Therapy in Combating Cancer. Oncotarget 2017, 8, 38022–38043. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Torchilin, V.P. Stimulus-Responsive Nanopreparations for Tumor Targeting. Integr. Biol. 2013, 5, 96–107. [Google Scholar] [CrossRef]
- Danhier, F.; Feron, O.; Préat, V. To Exploit the Tumor Microenvironment: Passive and Active Tumor Targeting of Nanocarriers for Anti-Cancer Drug Delivery. J. Control. Release 2010, 148, 135–146. [Google Scholar] [CrossRef]
- Li, R.; Xie, Y. Nanodrug Delivery Systems for Targeting the Endogenous Tumor Microenvironment and Simultaneously Overcoming Multidrug Resistance Properties. J. Control. Release 2017, 251, 49–67. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.; Gu, L.; Ren, W.; Liu, Y. Stimuli-Responsive Polymers for Anti-Cancer Drug Delivery. Mater. Sci. Eng. C 2014, 45, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Mi, P. Stimuli-Responsive Nanocarriers for Drug Delivery, Tumor Imaging, Therapy and Theranostics. Theranostics 2020, 10, 4557–4588. [Google Scholar] [CrossRef] [PubMed]
- Kauscher, U.; Holme, M.N.; Björnmalm, M.; Stevens, M.M. Physical Stimuli-Responsive Vesicles in Drug Delivery: Beyond Liposomes and Polymersomes. Adv. Drug Deliv. Rev. 2019, 138, 259–275. [Google Scholar] [CrossRef]
- Regenold, M.; Bannigan, P.; Evans, J.C.; Waspe, A.; Temple, M.J.; Allen, C. Turning down the Heat: The Case for Mild Hyperthermia and Thermosensitive Liposomes. Nanomed. Nanotechnol. Biol. Med. 2022, 40, 102484. [Google Scholar] [CrossRef]
- Dai, Y.; Su, J.; Wu, K.; Ma, W.; Wang, B.; Li, M.; Sun, P.; Shen, Q.; Wang, Q.; Fan, Q. Multifunctional Thermosensitive Liposomes Based on Natural Phase-Change Material: Near-Infrared Light-Triggered Drug Release and Multimodal Imaging-Guided Cancer Combination Therapy. ACS Appl. Mater. Interfaces 2019, 11, 10540–10553. [Google Scholar] [CrossRef]
- Amin, M.; Lammers, T.; ten Hagen, T.L.M. Temperature-Sensitive Polymers to Promote Heat-Triggered Drug Release from Liposomes: Towards Bypassing EPR. Adv. Drug Deliv. Rev. 2022, 189, 114503. [Google Scholar] [CrossRef]
- Nardecchia, S.; Sánchez-Moreno, P.; de Vicente, J.; Marchal, J.A.; Boulaiz, H. Clinical Trials of Thermosensitive Nanomaterials: An Overview. Nanomaterials 2019, 9, 191. [Google Scholar] [CrossRef] [Green Version]
- Dou, Y.; Hynynen, K.; Allen, C. To Heat or Not to Heat: Challenges with Clinical Translation of Thermosensitive Liposomes. J. Control. Release 2017, 249, 63–73. [Google Scholar] [CrossRef]
- Lyon, P.C.; Gray, M.D.; Mannaris, C.; Folkes, L.K.; Stratford, M.; Campo, L.; Chung, D.Y.F.; Scott, S.; Anderson, M.; Goldin, R.; et al. Safety and Feasibility of Ultrasound-Triggered Targeted Drug Delivery of Doxorubicin from Thermosensitive Liposomes in Liver Tumours (TARDOX): A Single-Centre, Open-Label, Phase 1 Trial. Lancet Oncol. 2018, 19, 1027–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lammers, T.; Kiessling, F.; Hennink, W.E.; Storm, G. Nanotheranostics and Image-Guided Drug Delivery: Current Concepts and Future Directions. Mol. Pharm. 2010, 7, 1899–1912. [Google Scholar] [CrossRef] [PubMed]
- Andresen, T.L.; Jensen, S.S.; Jørgensen, K. Advanced Strategies in Liposomal Cancer Therapy: Problems and Prospects of Active and Tumor Specific Drug Release. Prog. Lipid Res. 2005, 44, 68–97. [Google Scholar] [CrossRef] [PubMed]
- Halford, S.; Yip, D.; Karapetis, C.S.; Strickland, A.H.; Steger, A.; Khawaja, H.T.; Harper, P.G. A Phase II Study Evaluating the Tolerability and Efficacy of CAELYX (Liposomal Doxorubicin, Doxil) in the Treatment of Unresectable Pancreatic Carcinoma. Ann. Oncol. 2001, 12, 1399–1402. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Gotoh, M.; Muro, K.; Yamada, Y.; Shirao, K.; Shimada, Y.; Okuwa, M.; Matsumoto, S.; Miyata, Y.; Ohkura, H.; et al. Phase I and Pharmacokinetic Study of MCC-465, a Doxorubicin (DXR) Encapsulated in PEG Immunoliposome, in Patients with Metastatic Stomach Cancer. Ann. Oncol. 2004, 15, 517–525. [Google Scholar] [CrossRef]
- Harrington, K.J.; Lewanski, C.R.; Northcote, A.D.; Whittaker, J.; Wellbank, H.; Vile, R.G.; Peters, A.M.; Stewart, J.S. Phase I–II Study of Pegylated Liposomal Cisplatin (SPI-077) in Patients with Inoperable Head and Neck Cancer. Ann. Oncol. 2001, 12, 493–496. [Google Scholar] [CrossRef]
- Gabizon, A.A. Pegylated Liposomal Doxorubicin: Metamorphosis of an Old Drug into a New Form of Chemotherapy. Cancer Investig. 2001, 19, 424–436. [Google Scholar] [CrossRef]
- Charrois, G.J.R.; Allen, T.M. Multiple Injections of Pegylated Liposomal Doxorubicin: Pharmacokinetics and Therapeutic Activity. J. Pharmacol. Exp. Ther. 2003, 306, 1058–1067. [Google Scholar] [CrossRef] [Green Version]
- Mura, S.; Nicolas, J.; Couvreur, P. Stimuli-Responsive Nanocarriers for Drug Delivery. Nat. Mater. 2013, 12, 991–1003. [Google Scholar] [CrossRef]
- Mirvakili, S.M.; Langer, R. Wireless On-Demand Drug Delivery. Nat. Electron. 2021, 4, 464–477. [Google Scholar] [CrossRef]
- Torchilin, V.P. Multifunctional, Stimuli-Sensitive Nanoparticulate Systems for Drug Delivery. Nat. Rev. Drug Discov. 2014, 13, 813–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, S.H.; Wientjes, M.G.; Lu, D.; Au, J.L.S. Drug Delivery and Transport to Solid Tumors. Pharm. Res. 2003, 20, 1337–1350. [Google Scholar] [CrossRef] [PubMed]
- Rapp, B.E. Chapter 9—Fluids. In Microfluidics: Modelling, Mechanics and Mathematics; Rapp, B.E., Ed.; Elsevier: Oxford, UK, 2017; pp. 243–263. ISBN 978-1-4557-3141-1. [Google Scholar]
- Prichard, R.; Gibson, M.; Joseph, C.; Strasser, W. Chapter 13—A Review of Fluid Flow in and around the Brain, Modeling, and Abnormalities. In Multiscale Biomechanical Modeling of the Brain; Prabhu, R., Horstemeyer, M., Eds.; Academic Press: Cambridge, MA, USA, 2022; pp. 209–238. ISBN 978-0-12-818144-7. [Google Scholar]
- Swabb, E.A.; Wei, J.; Gullino, P.M. Diffusion and Convection in Normal and Neoplastic Tissues. Cancer Res. 1974, 34, 2814–2822. [Google Scholar]
- Wientjes, M.G.; Yeung, B.Z.; Lu, Z.; Wientjes, M.G.; Au, J.L.S. Predicting Diffusive Transport of Cationic Liposomes in 3-Dimensional Tumor Spheroids. J. Control. Release 2014, 192, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attama, A.A.; Momoh, M.A.; Builders, P.F. Chapter 5—Lipid Nanoparticulate Drug Delivery Systems: A Revolution in Dosage Form Design and Development. In Recent Advances in Novel Drug Carrier Systems; Ali Demir Sezer, Ed.; IntechOpen: Rijeka, Croatia, 2012. [Google Scholar]
- Baxter, L.T.; Jain, R.K. Transport of Fluid and Macromolecules in Tumors. I. Role of Interstitial Pressure and Convection. Microvasc. Res. 1989, 37, 77–104. [Google Scholar] [CrossRef] [PubMed]
- Khawar, I.A.; Kim, J.H.; Kuh, H.-J. Improving Drug Delivery to Solid Tumors: Priming the Tumor Microenvironment. J. Control. Release 2015, 201, 78–89. [Google Scholar] [CrossRef]
- Munson, J.; Shieh, A. Interstitial Fluid Flow in Cancer: Implications for Disease Progression and Treatment. Cancer Manag. Res. 2014, 6, 317–328. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Chen, X.; Cao, J.; Gao, H. Overcoming the Biological Barriers in the Tumor Microenvironment for Improving Drug Delivery and Efficacy. J. Mater. Chem. B 2020, 8, 6765–6781. [Google Scholar] [CrossRef]
- Stine, C.A.; Munson, J.M. Convection-Enhanced Delivery: Connection to and Impact of Interstitial Fluid Flow. Front. Oncol. 2019, 9, 966. [Google Scholar] [CrossRef] [Green Version]
- Carmeliet, P.; Jain, R.K. Principles and Mechanisms of Vessel Normalization for Cancer and Other Angiogenic Diseases. Nat. Rev. Drug Discov. 2011, 10, 417–427. [Google Scholar] [CrossRef]
- Chowdhury, S.M.; Abou-Elkacem, L.; Lee, T.; Dahl, J.; Lutz, A.M. Ultrasound and Microbubble Mediated Therapeutic Delivery: Underlying Mechanisms and Future Outlook. J. Control. Release 2020, 326, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, R. Theory for Acoustic Streaming in Soft Porous Matter and Its Applications to Ultrasound-Enhanced Convective Delivery. J. Ther. Ultrasound 2018, 6, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J. Acoustic Streaming and Its Applications. Fluids 2018, 3, 108. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, J.; Magin, R.; Yatvin, M.; Zaharko, D. Liposomes and Local Hyperthermia: Selective Delivery of Methotrexate to Heated Tumors. Science 1979, 204, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Yatvin, M.; Weinstein, J.; Dennis, W.; Blumenthal, R. Design of Liposomes for Enhanced Local Release of Drugs by Hyperthermia. Science 1978, 202, 1290–1293. [Google Scholar] [CrossRef]
- Manzoor, A.A.; Lindner, L.H.; Landon, C.D.; Park, J.-Y.; Simnick, A.J.; Dreher, M.R.; Das, S.; Hanna, G.; Park, W.; Chilkoti, A.; et al. Overcoming Limitations in Nanoparticle Drug Delivery: Triggered, Intravascular Release to Improve Drug Penetration into Tumors. Cancer Res. 2012, 72, 5566–5575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ten Hagen, T.L.M.; Dreher, M.R.; Zalba, S.; Seynhaeve, A.L.B.; Amin, M.; Li, L.; Haemmerich, D. Drug Transport Kinetics of Intravascular Triggered Drug Delivery Systems. Commun. Biol. 2021, 4, 920. [Google Scholar] [CrossRef]
- Borys, N.; Dewhirst, M.W. Drug Development of Lyso-Thermosensitive Liposomal Doxorubicin: Combining Hyperthermia and Thermosensitive Drug Delivery. Adv. Drug Deliv. Rev. 2021, 178, 113985. [Google Scholar] [CrossRef]
- Sirsi, S.R.; Borden, M.A. State-of-the-Art Materials for Ultrasound-Triggered Drug Delivery. Adv. Drug Deliv. Rev. 2014, 72, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Frinking, P.; Segers, T.; Luan, Y.; Tranquart, F. Three Decades of Ultrasound Contrast Agents: A Review of the Past, Present and Future Improvements. Ultrasound Med. Biol. 2020, 46, 892–908. [Google Scholar] [CrossRef] [Green Version]
- Lea-Banks, H.; O’Reilly, M.A.; Hynynen, K. Ultrasound-Responsive Droplets for Therapy: A Review. J. Control. Release 2019, 293, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Wells, P.N.T. Ultrasound Imaging. Phys. Med. Biol. 2006, 51, R83. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.A. Medical Ultrasound Imaging. Prog. Biophys. Mol. Biol. 2007, 93, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Wells, P.N.T.; Liang, H.-D. Medical Ultrasound: Imaging of Soft Tissue Strain and Elasticity. J. R. Soc. Interface 2011, 8, 1521–1549. [Google Scholar] [CrossRef] [Green Version]
- Shung, K.K. Diagnostic Ultrasound: Imaging and Blood Flow Measurements; CRC Press: Boca Raton, FL, USA, 2015; ISBN 1-4665-8265-0. [Google Scholar]
- Borden, M.A.; Dayton, P.A.; Slagle, C.; Walmer, R.W. Chapter 35—Ultrasound Contrast Agents. In Molecular Imaging, 2nd ed.; Ross, B.D., Gambhir, S.S., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 639–653. ISBN 978-0-12-816386-3. [Google Scholar]
- Wang, Y.; Cong, H.; Wang, S.; Yu, B.; Shen, Y. Development and Application of Ultrasound Contrast Agents in Biomedicine. J. Mater. Chem. B 2021, 9, 7633–7661. [Google Scholar] [CrossRef]
- Paefgen, V.; Doleschel, D.; Kiessling, F. Evolution of Contrast Agents for Ultrasound Imaging and Ultrasound-Mediated Drug Delivery. Front. Pharmacol. 2015, 6, 197. [Google Scholar] [CrossRef] [Green Version]
- Gramiak, R.; Shah, P.M. Echocardiography of the Aortic Root. Investig. Radiol. 1968, 3, 356–366. [Google Scholar] [CrossRef]
- Bouakaz, A.; Zeghimi, A.; Doinikov, A.A. Sonoporation: Concept and Mechanisms. Adv. Exp. Med. Biol. 2016, 880, 175–189. [Google Scholar] [CrossRef]
- Liang, H.-D.; Tang, J.; Halliwell, M. Sonoporation, Drug Delivery, and Gene Therapy. Proc. Inst. Mech. Eng. H 2010, 224, 343–361. [Google Scholar] [CrossRef]
- Tsutsui, J.M.; Xie, F.; Porter, R.T. The Use of Microbubbles to Target Drug Delivery. Cardiovasc. Ultrasound 2004, 2, 23. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, K.; Pollard, R.; Borden, M. Ultrasound Microbubble Contrast Agents: Fundamentals and Application to Gene and Drug Delivery. Annu. Rev. Biomed. Eng. 2007, 9, 415–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, C.-H.; Ho, Y.-J.; Lin, C.-W.; Wu, N.; Chiang, P.-H.; Yeh, C.-K. State-of-the-Art of Ultrasound-Triggered Drug Delivery from Ultrasound-Responsive Drug Carriers. Expert Opin. Drug Deliv. 2022, 19, 997–1009. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.-J.; Huang, C.-C.; Fan, C.-H.; Liu, H.-L.; Yeh, C.-K. Ultrasonic Technologies in Imaging and Drug Delivery. Cell. Mol. Life Sci. 2021, 78, 6119–6141. [Google Scholar] [CrossRef] [PubMed]
- Entzian, K.; Aigner, A. Drug Delivery by Ultrasound-Responsive Nanocarriers for Cancer Treatment. Pharmaceutics 2021, 13, 1135. [Google Scholar] [CrossRef]
- Skyba, D.M.; Price, R.J.; Linka, A.Z.; Skalak, T.C.; Kaul, S. Direct in Vivo Visualization of Intravascular Destruction of Microbubbles by Ultrasound and Its Local Effects on Tissue. Circulation 1998, 98, 290–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sirsi, S.R.; Borden, M.A. Microbubble Compositions, Properties and Biomedical Applications. Bubble Sci. Eng. Technol. 2009, 1, 3–17. [Google Scholar] [CrossRef] [Green Version]
- Blomley, M.J.; Cooke, J.C.; Unger, E.C.; Monaghan, M.J.; Cosgrove, D.O. Microbubble Contrast Agents: A New Era in Ultrasound. BMJ 2001, 322, 1222–1225. [Google Scholar] [CrossRef]
- Leighton, T.G.; Apfel, R.E. The Acoustic Bubble. J. Acoust. Soc. Am. 1994, 96, 2616. [Google Scholar] [CrossRef]
- Sboros, V. Response of Contrast Agents to Ultrasound. Adv. Drug Deliv. Rev. 2008, 60, 1117–1136. [Google Scholar] [CrossRef]
- Cosgrove, D. Ultrasound Contrast Agents: An Overview. Eur. J. Radiol. 2006, 60, 324–330. [Google Scholar] [CrossRef]
- Keller, M.W.; Glasheen, W.; Kaul, S. Albunex: A Safe and Effective Commercially Produced Agent for Myocardial Contrast Echocardiography. J. Am. Soc. Echocardiogr. 1989, 2, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-Y.; Chen, C.C.; Tung, Y.-S.; Olumolade, O.O.; Konofagou, E.E. Effects of the Microbubble Shell Physicochemical Properties on Ultrasound-Mediated Drug Delivery to the Brain. J. Control. Release 2015, 212, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheeran, P.S.; Dayton, P.A. Phase-Change Contrast Agents for Imaging and Therapy. Curr. Pharm. Des. 2012, 18, 2152–2165. [Google Scholar] [CrossRef] [PubMed]
- Mountford, P.A.; Smith, W.S.; Borden, M.A. Fluorocarbon Nanodrops as Acoustic Temperature Probes. Langmuir 2015, 31, 10656–10663. [Google Scholar] [CrossRef]
- Mountford, P.A.; Thomas, A.N.; Borden, M.A. Thermal Activation of Superheated Lipid-Coated Perfluorocarbon Drops. Langmuir 2015, 31, 4627–4634. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, P.S.; Luois, S.; Dayton, P.A.; Matsunaga, T.O. Formulation and Acoustic Studies of a New Phase-Shift Agent for Diagnostic and Therapeutic Ultrasound. Langmuir 2011, 27, 10412–10420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seda, R.; Li, D.S.; Fowlkes, J.B.; Bull, J.L. Characterization of Bioeffects on Endothelial Cells under Acoustic Droplet Vaporization. Ultrasound Med. Biol. 2015, 41, 3241–3252. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.-T.; Lin, Y.-C.; Yeh, C.-K. Mechanical Bioeffects of Acoustic Droplet Vaporization in Vessel-Mimicking Phantoms. Ultrason. Sonochem. 2014, 21, 1866–1874. [Google Scholar] [CrossRef]
- Fix, S.M.; Novell, A.; Yun, Y.; Dayton, P.A.; Arena, C.B. An Evaluation of the Sonoporation Potential of Low-Boiling Point Phase-Change Ultrasound Contrast Agents in Vitro. J. Ther. Ultrasound 2017, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Loskutova, K.; Grishenkov, D.; Ghorbani, M. Review on Acoustic Droplet Vaporization in Ultrasound Diagnostics and Therapeutics. BioMed Res. Int. 2019, 2019, 9480193. [Google Scholar] [CrossRef]
- Kooiman, K.; Roovers, S.; Langeveld, S.A.G.; Kleven, R.T.; Dewitte, H.; O’Reilly, M.A.; Escoffre, J.-M.; Bouakaz, A.; Verweij, M.D.; Hynynen, K.; et al. Ultrasound-Responsive Cavitation Nuclei for Therapy and Drug Delivery. Ultrasound Med. Biol. 2020, 46, 1296–1325. [Google Scholar] [CrossRef] [Green Version]
- Lammertink, B.H.A.; Bos, C.; Deckers, R.; Storm, G.; Moonen, C.T.W.; Escoffre, J.-M. Sonochemotherapy: From Bench to Bedside. Front. Pharmacol. 2015, 6, 138. [Google Scholar] [CrossRef] [Green Version]
- Rich, J.; Tian, Z.; Huang, T.J. Sonoporation: Past, Present, and Future. Adv. Mater. Technol. 2022, 7, 2100885. [Google Scholar] [CrossRef] [PubMed]
- Lentacker, I.; De Cock, I.; Deckers, R.; De Smedt, S.C.; Moonen, C.T.W. Understanding Ultrasound Induced Sonoporation: Definitions and Underlying Mechanisms. Adv. Drug Deliv. Rev. 2014, 72, 49–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, P.; Han, T.; Yu, A.C.H.; Xu, L. Mechanistic Understanding the Bioeffects of Ultrasound-Driven Microbubbles to Enhance Macromolecule Delivery. J. Control. Release 2018, 272, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Helfield, B.; Chen, X.; Watkins, S.C.; Villanueva, F.S. Biophysical Insight into Mechanisms of Sonoporation. Proc. Natl. Acad. Sci. USA 2016, 113, 9983–9988. [Google Scholar] [CrossRef] [Green Version]
- O’Reilly, M.A.; Hynynen, K. Ultrasound Enhanced Drug Delivery to the Brain and Central Nervous System. Int. J. Hyperth. 2012, 28, 386–396. [Google Scholar] [CrossRef] [Green Version]
- Dasgupta, A.; Liu, M.; Ojha, T.; Storm, G.; Kiessling, F.; Lammers, T. Ultrasound-Mediated Drug Delivery to the Brain: Principles, Progress and Prospects. Drug Discov. Today Technol. 2016, 20, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Mainprize, T.; Lipsman, N.; Huang, Y.; Meng, Y.; Bethune, A.; Ironside, S.; Heyn, C.; Alkins, R.; Trudeau, M.; Sahgal, A.; et al. Blood-Brain Barrier Opening in Primary Brain Tumors with Non-Invasive MR-Guided Focused Ultrasound: A Clinical Safety and Feasibility Study. Sci. Rep. 2019, 9, 321. [Google Scholar] [CrossRef] [Green Version]
- Abrahao, A.; Meng, Y.; Llinas, M.; Huang, Y.; Hamani, C.; Mainprize, T.; Aubert, I.; Heyn, C.; Black, S.E.; Hynynen, K.; et al. First-in-Human Trial of Blood–Brain Barrier Opening in Amyotrophic Lateral Sclerosis Using MR-Guided Focused Ultrasound. Nat. Commun. 2019, 10, 4373. [Google Scholar] [CrossRef] [Green Version]
- Meng, Y.; Pople, C.B.; Lea-Banks, H.; Abrahao, A.; Davidson, B.; Suppiah, S.; Vecchio, L.M.; Samuel, N.; Mahmud, F.; Hynynen, K.; et al. Safety and Efficacy of Focused Ultrasound Induced Blood-Brain Barrier Opening, an Integrative Review of Animal and Human Studies. J. Control. Release 2019, 309, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Krut, Z.; Gazit, D.; Gazit, Z.; Pelled, G. Applications of Ultrasound-Mediated Gene Delivery in Regenerative Medicine. Bioengineering 2022, 9, 190. [Google Scholar] [CrossRef]
- Duan, X.; Zhou, Q.; Wan, J.M.F.; Yu, A.C.H. Sonoporation Generates Downstream Cellular Impact after Membrane Resealing. Sci. Rep. 2021, 11, 5161. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, Z.I.; Tu, T.-W.; Sundby, M.; Qureshi, F.; Lewis, B.K.; Jikaria, N.; Burks, S.R.; Frank, J.A. MRI and Histological Evaluation of Pulsed Focused Ultrasound and Microbubbles Treatment Effects in the Brain. Theranostics 2018, 8, 4837–4855. [Google Scholar] [CrossRef] [PubMed]
- Jung, O.; Thomas, A.; Burks, S.R.; Dustin, M.L.; Frank, J.A.; Ferrer, M.; Stride, E. Neuroinflammation Associated with Ultrasound-Mediated Permeabilization of the Blood-Brain Barrier. Trends Neurosci. 2022, 45, 459–470. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, K.; Barzegar-Fallah, A.; Banstola, A.; Rizwan, S.B.; Reynolds, J.N.J. Ultrasound-Mediated Blood-Brain Barrier Disruption for Drug Delivery: A Systematic Review of Protocols, Efficacy, and Safety Outcomes from Preclinical and Clinical Studies. Pharmaceutics 2022, 14, 833. [Google Scholar] [CrossRef] [PubMed]
- Przystupski, D.; Ussowicz, M. Landscape of Cellular Bioeffects Triggered by Ultrasound-Induced Sonoporation. Int. J. Mol. Sci. 2022, 23, 11222. [Google Scholar] [CrossRef]
- Furusawa, Y.; Hassan, M.A.; Zhao, Q.-L.; Ogawa, R.; Tabuchi, Y.; Kondo, T. Effects of Therapeutic Ultrasound on the Nucleus and Genomic DNA. Ultrason. Sonochem. 2014, 21, 2061–2068. [Google Scholar] [CrossRef]
- Yang, Y.; Li, Q.; Guo, X.; Tu, J.; Zhang, D. Mechanisms Underlying Sonoporation: Interaction between Microbubbles and Cells. Ultrason. Sonochem. 2020, 67, 105096. [Google Scholar] [CrossRef]
- Izadifar, Z.; Babyn, P.; Chapman, D. Mechanical and Biological Effects of Ultrasound: A Review of Present Knowledge. Ultrasound Med. Biol. 2017, 43, 1085–1104. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.K. Normalization of Tumor Vasculature: An Emerging Concept in Antiangiogenic Therapy. Science 2005, 307, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Mo, S.; Coussios, C.-C.; Seymour, L.; Carlisle, R. Ultrasound-Enhanced Drug Delivery for Cancer. Expert Opin. Drug Deliv. 2012, 9, 1525–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, A.; Hynynen, K. Drug Delivery across the Blood-Brain Barrier Using Focused Ultrasound. Expert Opin. Drug Deliv. 2014, 11, 711–721. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.C.; Sheeran, P.S.; Wu, S.-Y.; Olumolade, O.O.; Dayton, P.A.; Konofagou, E.E. Targeted Drug Delivery with Focused Ultrasound-Induced Blood-Brain Barrier Opening Using Acoustically-Activated Nanodroplets. J. Control. Release 2013, 172, 795–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omata, D.; Unga, J.; Suzuki, R.; Maruyama, K. Lipid-Based Microbubbles and Ultrasound for Therapeutic Application. Adv. Drug Deliv. Rev. 2020, 154–155, 236–244. [Google Scholar] [CrossRef]
- Al-Jawadi, S.; Thakur, S.S. Ultrasound-Responsive Lipid Microbubbles for Drug Delivery: A Review of Preparation Techniques to Optimise Formulation Size, Stability and Drug Loading. Int. J. Pharm. 2020, 585, 119559. [Google Scholar] [CrossRef]
- Tinkov, S.; Winter, G.; Coester, C.; Bekeredjian, R. New Doxorubicin-Loaded Phospholipid Microbubbles for Targeted Tumor Therapy: Part I—Formulation Development and in-Vitro Characterization. J. Control. Release 2010, 143, 143–150. [Google Scholar] [CrossRef]
- Fokong, S.; Theek, B.; Wu, Z.; Koczera, P.; Appold, L.; Jorge, S.; Resch-Genger, U.; van Zandvoort, M.; Storm, G.; Kiessling, F.; et al. Image-Guided, Targeted and Triggered Drug Delivery to Tumors Using Polymer-Based Microbubbles. J. Control. Release 2012, 163, 75–81. [Google Scholar] [CrossRef]
- El-Sherif, D.M.; Wheatley, M.A. Development of a Novel Method for Synthesis of a Polymeric Ultrasound Contrast Agent. J. Biomed. Mater. Res. Part A 2003, 66A, 347–355. [Google Scholar] [CrossRef]
- Cochran, M.C.; Eisenbrey, J.; Ouma, R.O.; Soulen, M.; Wheatley, M.A. Doxorubicin and Paclitaxel Loaded Microbubbles for Ultrasound Triggered Drug Delivery. Int. J. Pharm. 2011, 414, 161–170. [Google Scholar] [CrossRef] [Green Version]
- Koczera, P.; Appold, L.; Shi, Y.; Liu, M.; Dasgupta, A.; Pathak, V.; Ojha, T.; Fokong, S.; Wu, Z.; van Zandvoort, M.; et al. PBCA-Based Polymeric Microbubbles for Molecular Imaging and Drug Delivery. J. Control. Release 2017, 259, 128–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Dasgupta, A.; Koczera, P.; Schipper, S.; Rommel, D.; Shi, Y.; Kiessling, F.; Lammers, T. Drug Loading in Poly(Butyl Cyanoacrylate)-Based Polymeric Microbubbles. Mol. Pharm. 2020, 17, 2840–2848. [Google Scholar] [CrossRef] [PubMed]
- Barmin, R.A.; Dasgupta, A.; Bastard, C.; De Laporte, L.; Rütten, S.; Weiler, M.; Kiessling, F.; Lammers, T.; Pallares, R.M. Engineering the Acoustic Response and Drug Loading Capacity of PBCA-Based Polymeric Microbubbles with Surfactants. Mol. Pharm. 2022, 19, 3256–3266. [Google Scholar] [CrossRef] [PubMed]
- Honari, A.; Kapilavaih, P.S.; Akter, N.; Sirsi, S.R. Remote Loading of Gas Bubbles into Polylactic Acid Microcapsules Creates Acoustically Active Janus Particles. ACS Appl. Polym. Mater. 2022, 4, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Seekell, R.P.; Cole, A.R.; Lamothe, J.R.; Lock, A.T.; van den Bosch, S.; Tang, X.; Kheir, J.N.; Polizzotti, B.D. Interfacial Nanoprecipitation toward Stable and Responsive Microbubbles and Their Use as a Resuscitative Fluid. Angew. Chem. Int. Ed. 2018, 57, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Chapla, R.; Huynh, K.T.; Schutt, C.E. Microbubble-Nanoparticle Complexes for Ultrasound-Enhanced Cargo Delivery. Pharmaceutics 2022, 14, 2396. [Google Scholar] [CrossRef]
- Kheirolomoom, A.; Dayton, P.A.; Lum, A.F.H.; Little, E.; Paoli, E.E.; Zheng, H.; Ferrara, K.W. Acoustically-Active Microbubbles Conjugated to Liposomes: Characterization of a Proposed Drug Delivery Vehicle. J. Control. Release 2007, 118, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Lentacker, I.; De Smedt, S.C.; Demeester, J.; Van Marck, V.; Bracke, M.; Sanders, N.N. Lipoplex-Loaded Microbubbles for Gene Delivery: A Trojan Horse Controlled by Ultrasound. Adv. Funct. Mater. 2007, 17, 1910–1916. [Google Scholar] [CrossRef] [Green Version]
- Klibanov, A.L.; Shevchenko, T.I.; Raju, B.I.; Seip, R.; Chin, C.T. Ultrasound-Triggered Release of Materials Entrapped in Microbubble–Liposome Constructs: A Tool for Targeted Drug Delivery. J. Control. Release 2010, 148, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Geers, B.; Lentacker, I.; Sanders, N.N.; Demeester, J.; Meairs, S.; De Smedt, S.C. Self-Assembled Liposome-Loaded Microbubbles: The Missing Link for Safe and Efficient Ultrasound Triggered Drug-Delivery. J. Control. Release 2011, 152, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Vandenbroucke, R.E.; Lentacker, I.; Demeester, J.; De Smedt, S.C.; Sanders, N.N. Ultrasound Assisted SiRNA Delivery Using PEG-SiPlex Loaded Microbubbles. J. Control. Release 2008, 126, 265–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, Y.I.; Kwon, Y.-S.; Cho, H.-S.; Heo, S.-H.; Park, K.S.; Park, S.G.; Lee, S.-H.; Hwang, S.I.; Kim, Y.I.; Jae, H.J.; et al. Ultrasound-Mediated Gene and Drug Delivery Using a Microbubble-Liposome Particle System. Theranostics 2014, 4, 1133–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, F.; Li, L.; Deng, Z.; Jin, Q.; Chen, J.; Yang, W.; Yeh, C.-K.; Wu, J.; Shandas, R.; Liu, X.; et al. Paclitaxel-Liposome-Microbubble Complexes as Ultrasound-Triggered Therapeutic Drug Delivery Carriers. J. Control. Release 2013, 166, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Nesbitt, H.; Logan, K.; Burnett, K.; White, B.; Jack, I.G.; Taylor, M.A.; Love, M.; Callan, B.; McHale, A.P.; et al. An Ultrasound Responsive Microbubble-Liposome Conjugate for Targeted Irinotecan-Oxaliplatin Treatment of Pancreatic Cancer. Eur. J. Pharm. Biopharm. 2020, 157, 233–240. [Google Scholar] [CrossRef]
- Huang, F.-Y.; Lei, J.; Sun, Y.; Yan, F.; Chen, B.; Zhang, L.; Lu, Z.; Cao, R.; Lin, Y.-Y.; Wang, C.-C.; et al. Induction of Enhanced Immunogenic Cell Death through Ultrasound-Controlled Release of Doxorubicin by Liposome-Microbubble Complexes. Oncoimmunology 2018, 7, e1446720. [Google Scholar] [CrossRef]
- Burke, C.W.; Alexander, E., 4th; Timbie, K.; Kilbanov, A.L.; Price, R.J. Ultrasound-Activated Agents Comprised of 5FU-Bearing Nanoparticles Bonded to Microbubbles Inhibit Solid Tumor Growth and Improve Survival. Mol. Ther. 2014, 22, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Rapoport, N.; Gao, Z.; Kennedy, A. Multifunctional Nanoparticles for Combining Ultrasonic Tumor Imaging and Targeted Chemotherapy. J. Natl. Cancer Inst. 2007, 99, 1095–1106. [Google Scholar] [CrossRef]
- Rapoport, N. Drug-Loaded Perfluorocarbon Nanodroplets for Ultrasound-Mediated Drug Delivery. Adv. Exp. Med. Biol. 2016, 880, 221–241. [Google Scholar] [CrossRef]
- Rapoport, N. Phase-Shift, Stimuli-Responsive Perfluorocarbon Nanodroplets for Drug Delivery to Cancer: Phase-Shift Perfluorocarbon Nanoemulsions. WIREs Nanomed. Nanobiotechnol. 2012, 4, 492–510. [Google Scholar] [CrossRef] [Green Version]
- Ji, G.; Yang, J.; Chen, J. Preparation of Novel Curcumin-Loaded Multifunctional Nanodroplets for Combining Ultrasonic Development and Targeted Chemotherapy. Int. J. Pharm. 2014, 466, 314–320. [Google Scholar] [CrossRef]
- Zhang, W.; Shi, Y.; Abd Shukor, S.; Vijayakumaran, A.; Vlatakis, S.; Wright, M.; Thanou, M. Phase-Shift Nanodroplets as an Emerging Sonoresponsive Nanomaterial for Imaging and Drug Delivery Applications. Nanoscale 2022, 14, 2943–2965. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Xu, N.; Liu, Y.; Ling, G.; Yu, J.; Zhang, P. Functional Ultrasound-Triggered Phase-Shift Perfluorocarbon Nanodroplets for Cancer Therapy. Ultrasound Med. Biol. 2021, 47, 2064–2079. [Google Scholar] [CrossRef]
- Dong, W.; Wu, P.; Zhou, D.; Huang, J.; Qin, M.; Yang, X.; Wan, M.; Zong, Y. Ultrasound-Mediated Gene Therapy of Hepatocellular Carcinoma Using Pre-MicroRNA Plasmid-Loaded Nanodroplets. Ultrasound Med. Biol. 2020, 46, 90–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Y.; Chen, Y.; Yu, T.; Guo, Y.; Liu, F.; Yao, Y.; Li, P.; Wang, D.; Wang, Z.; Chen, Y.; et al. Drug Release from Phase-Changeable Nanodroplets Triggered by Low-Intensity Focused Ultrasound. Theranostics 2018, 8, 1327–1339. [Google Scholar] [CrossRef]
- Honari, A.; Merillat, D.A.; Bellary, A.; Ghaderi, M.; Sirsi, S.R. Improving Release of Liposome-Encapsulated Drugs with Focused Ultrasound and Vaporizable Droplet-Liposome Nanoclusters. Pharmaceutics 2021, 13, 609. [Google Scholar] [CrossRef] [PubMed]
- Airan, R. Neuromodulation with Nanoparticles. Science 2017, 357, 465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Airan, R.D.; Meyer, R.A.; Ellens, N.P.K.; Rhodes, K.R.; Farahani, K.; Pomper, M.G.; Kadam, S.D.; Green, J.J. Noninvasive Targeted Transcranial Neuromodulation via Focused Ultrasound Gated Drug Release from Nanoemulsions. Nano Lett. 2017, 17, 652–659. [Google Scholar] [CrossRef]
- Lea-Banks, H.; O’Reilly, M.A.; Hamani, C.; Hynynen, K. Localized Anesthesia of a Specific Brain Region Using Ultrasound-Responsive Barbiturate Nanodroplets. Theranostics 2020, 10, 2849–2858. [Google Scholar] [CrossRef]
- Lea-Banks, H.; Hynynen, K. Sub-Millimetre Precision of Drug Delivery in the Brain from Ultrasound-Triggered Nanodroplets. J. Control. Release 2021, 338, 731–741. [Google Scholar] [CrossRef]
- Ozdas, M.S.; Shah, A.S.; Johnson, P.M.; Patel, N.; Marks, M.; Yasar, T.B.; Stalder, U.; Bigler, L.; von der Behrens, W.; Sirsi, S.R.; et al. Non-Invasive Molecularly-Specific Millimeter-Resolution Manipulation of Brain Circuits by Ultrasound-Mediated Aggregation and Uncaging of Drug Carriers. Nat. Commun. 2020, 11, 4929. [Google Scholar] [CrossRef]
- Gorick, C.M.; Mathew, A.S.; Garrison, W.J.; Thim, E.A.; Fisher, D.G.; Copeland, C.A.; Song, J.; Klibanov, A.L.; Miller, G.W.; Price, R.J. Sonoselective Transfection of Cerebral Vasculature without Blood–Brain Barrier Disruption. Proc. Natl. Acad. Sci. USA 2020, 117, 5644–5654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wrenn, S.; Dicker, S.; Small, E.; Mleczko, M. Controlling Cavitation for Controlled Release. In Proceedings of the 2009 IEEE International Ultrasonics Symposium, Rome, Italy, 20–23 September 2009; pp. 104–107. [Google Scholar]
- Wallace, N.; Dicker, S.; Lewin, P.; Wrenn, S.P. Influence of Nesting Shell Size on Brightness Longevity and Resistance to Ultrasound-Induced Dissolution during Enhanced B-Mode Contrast Imaging. Ultrasonics 2014, 54, 2099–2108. [Google Scholar] [CrossRef] [PubMed]
- Cimorelli, M.; Angel, B.; Fafarman, A.; Kohut, A.; Andrien, B.; Barrett, K.; Wrenn, S. Introducing a Nested Phase Change Agent with an Acoustic Response That Depends on Electric Field: A Candidate for Myocardial Perfusion Imaging and Drug Delivery. Appl. Acoust. 2018, 138, 9–17. [Google Scholar] [CrossRef]
- Wallace, N.; Wrenn, S.P. Ultrasound Triggered Drug Delivery with Liposomal Nested Microbubbles. Ultrasonics 2015, 63, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Ibsen, S.; Benchimol, M.; Simberg, D.; Schutt, C.; Steiner, J.; Esener, S. A Novel Nested Liposome Drug Delivery Vehicle Capable of Ultrasound Triggered Release of Its Payload. J. Control. Release 2011, 155, 358–366. [Google Scholar] [CrossRef] [Green Version]
- Batchelor, D.V.B.; Abou-Saleh, R.H.; Coletta, P.L.; McLaughlan, J.R.; Peyman, S.A.; Evans, S.D. Nested Nanobubbles for Ultrasound-Triggered Drug Release. ACS Appl. Mater. Interfaces 2020, 12, 29085–29093. [Google Scholar] [CrossRef]
- Javadi, M.; Pitt, W.G.; Belnap, D.M.; Tsosie, N.H.; Hartley, J.M. Encapsulating Nanoemulsions Inside ELiposomes for Ultrasonic Drug Delivery. Langmuir 2012, 28, 14720–14729. [Google Scholar] [CrossRef]
- de Matos, M.B.C.; Deckers, R.; van Elburg, B.; Lajoinie, G.; de Miranda, B.S.; Versluis, M.; Schiffelers, R.; Kok, R.J. Ultrasound-Sensitive Liposomes for Triggered Macromolecular Drug Delivery: Formulation and In Vitro Characterization. Front. Pharmacol. 2019, 10, 1463. [Google Scholar] [CrossRef]
- Hayward, A.T.J. The Role of Stabilized Gas Nuclei in Hydrodynamic Cavitation Inception. J. Phys. D Appl. Phys. 1970, 3, 574. [Google Scholar] [CrossRef]
- Thomas, R.G.; Jonnalagadda, U.S.; Kwan, J.J. Biomedical Applications for Gas-Stabilizing Solid Cavitation Agents. Langmuir 2019, 35, 10106–10115. [Google Scholar] [CrossRef]
- Manzano, M.; Vallet-Regí, M. Ultrasound Responsive Mesoporous Silica Nanoparticles for Biomedical Applications. Chem. Commun. 2019, 55, 2731–2740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, F.-C.; Xie, Y.; Deng, T.; Zink, J.I. Magnetism, Ultrasound, and Light-Stimulated Mesoporous Silica Nanocarriers for Theranostics and Beyond. J. Am. Chem. Soc. 2021, 143, 6025–6036. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Matsuda, H.; Zhou, H.; Honma, I. Ultrasound-Triggered Smart Drug Release from a Poly(Dimethylsiloxane)—Mesoporous Silica Composite. Adv. Mater. 2006, 18, 3083–3088. [Google Scholar] [CrossRef]
- Paris, J.L.; de la Torre, P.; Victoria Cabañas, M.; Manzano, M.; Grau, M.; Flores, A.I.; Vallet-Regí, M. Vectorization of Ultrasound-Responsive Nanoparticles in Placental Mesenchymal Stem Cells for Cancer Therapy. Nanoscale 2017, 9, 5528–5537. [Google Scholar] [CrossRef] [Green Version]
- Kwan, J.J.; Myers, R.; Coviello, C.M.; Graham, S.M.; Shah, A.R.; Stride, E.; Carlisle, R.C.; Coussios, C.C. Ultrasound-Propelled Nanocups for Drug Delivery. Small 2015, 11, 5305–5314. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Gupta, I.; Jonnalagadda, U.S.; Kwan, J.J. Complementary Effects of Porosigen and Stabilizer on the Structure of Hollow Porous Poly(Lactic-Co-Glycolic Acid) Microparticles. ACS Appl. Polym. Mater. 2020, 2, 3696–3703. [Google Scholar] [CrossRef]
- Sabuncu, S.; Yildirim, A. Gas-Stabilizing Nanoparticles for Ultrasound Imaging and Therapy of Cancer. Nano Converg. 2021, 8, 39. [Google Scholar] [CrossRef]
- Li, J.; Wang, X.; Zhang, T.; Wang, C.; Huang, Z.; Luo, X.; Deng, Y. A Review on Phospholipids and Their Main Applications in Drug Delivery Systems. Asian J. Pharm. Sci. 2015, 10, 81–98. [Google Scholar] [CrossRef]
- Singh, R.P.; Gangadharappa, H.V.; Mruthunjaya, K. Phospholipids: Unique Carriers for Drug Delivery Systems. J. Drug Deliv. Sci. Technol. 2017, 39, 166–179. [Google Scholar] [CrossRef]
- Ferrara, K.W.; Borden, M.A.; Zhang, H. Lipid-Shelled Vehicles: Engineering for Ultrasound Molecular Imaging and Drug Delivery. Acc. Chem. Res. 2009, 42, 881–892. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Peng, C.; Nguyen, T.; Sun, T.; Porter, T.; McDannold, N.; Kheir, J.N.; Polizzotti, B.D. Engineering Caged Microbubbles for Controlled Acoustic Cavitation and Pressure Sensing. ACS Mater. Lett. 2021, 3, 978–987. [Google Scholar] [CrossRef]
- Prajapati, S.K.; Jain, A.; Jain, A.; Jain, S. Biodegradable Polymers and Constructs: A Novel Approach in Drug Delivery. Eur. Polym. J. 2019, 120, 109191. [Google Scholar] [CrossRef]
- Urbánek, T.; Jäger, E.; Jäger, A.; Hrubý, M. Selectively Biodegradable Polyesters: Nature-Inspired Construction Materials for Future Biomedical Applications. Polymers 2019, 11, 1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, P.; Cornel, E.J.; Du, J. Ultrasound-Responsive Polymer-Based Drug Delivery Systems. Drug Deliv. Transl. Res. 2021, 11, 1323–1339. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Jung, K.; Li, A.; Liu, J.; Boyer, C. Recent Advances in Stimuli-Responsive Polymer Systems for Remotely Controlled Drug Release. Prog. Polym. Sci. 2019, 99, 101164. [Google Scholar] [CrossRef]
- Rudakovskaya, P.G.; Barmin, R.A.; Kuzmin, P.S.; Fedotkina, E.P.; Sencha, A.N.; Gorin, D.A. Microbubbles Stabilized by Protein Shell: From Pioneering Ultrasound Contrast Agents to Advanced Theranostic Systems. Pharmaceutics 2022, 14, 1236. [Google Scholar] [CrossRef]
- Hernot, S.; Klibanov, A.L. Microbubbles in Ultrasound-Triggered Drug and Gene Delivery. Adv. Drug Deliv. Rev. 2008, 60, 1153–1166. [Google Scholar] [CrossRef] [Green Version]
- Tharkar, P.; Varanasi, R.; Wong, W.S.F.; Jin, C.T.; Chrzanowski, W. Nano-Enhanced Drug Delivery and Therapeutic Ultrasound for Cancer Treatment and Beyond. Front. Bioeng. Biotechnol. 2019, 7, 324. [Google Scholar] [CrossRef] [Green Version]
- Kooiman, K.; Vos, H.J.; Versluis, M.; de Jong, N. Acoustic Behavior of Microbubbles and Implications for Drug Delivery. Adv. Drug Deliv. Rev. 2014, 72, 28–48. [Google Scholar] [CrossRef]
- Shakya, G.; Fajrial, A.K.; Ding, X.; Borden, M.A. Effect of Thermal History and Hydrocarbon Core Size on Perfluorocarbon Endoskeletal Droplet Vaporization. Langmuir 2022, 38, 2634–2641. [Google Scholar] [CrossRef]
- Wallace, N.; Dicker, S.; Lewin, P.; Wrenn, S.P. Inertial Cavitation Threshold of Nested Microbubbles. Ultrasonics 2015, 58, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Dayton, P.; Klibanov, A.; Brandenburger, G.; Ferrara, K. Acoustic Radiation Force in Vivo: A Mechanism to Assist Targeting of Microbubbles. Ultrasound Med. Biol. 1999, 25, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Borden, M.; Bloch, S.H.; Kruse, D.; Ferrara, K.W.; Dayton, P.A. Radiation-Force Assisted Targeting Facilitates Ultrasonic Molecular Imaging. Mol. Imaging 2004, 3, 135–148. [Google Scholar] [CrossRef]
- Ciancia, S.; Cafarelli, A.; Zahoranova, A.; Menciassi, A.; Ricotti, L. Pulsatile Drug Delivery System Triggered by Acoustic Radiation Force. Front. Bioeng. Biotechnol. 2020, 8, 317. [Google Scholar] [CrossRef] [PubMed]
- Lum, A.F.H.; Borden, M.A.; Dayton, P.A.; Kruse, D.E.; Simon, S.I.; Ferrara, K.W. Ultrasound Radiation Force Enables Targeted Deposition of Model Drug Carriers Loaded on Microbubbles. J. Control. Release 2006, 111, 128–134. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Rakshit, M.; Das, P.; Gupta, I.; Das, D.; Pramanik, M.; Ng, K.W.; Kwan, J. Ultrasonic Implantation and Imaging of Sound-Sensitive Theranostic Agents for the Treatment of Arterial Inflammation. ACS Appl. Mater. Interfaces 2021, 13, 24422–24430. [Google Scholar] [CrossRef]
- De Cock, I.; Lajoinie, G.; Versluis, M.; De Smedt, S.C.; Lentacker, I. Sonoprinting and the Importance of Microbubble Loading for the Ultrasound Mediated Cellular Delivery of Nanoparticles. Biomaterials 2016, 83, 294–307. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | Materials | Pro | Con | |
|---|---|---|---|---|
| UCA nested particles | Nested UCA Shell Material | Phospholipid (DSPC, DPPC) | 1. High drug-loading capacity 2. Long circulation time 3. Suitable for encapsulating both hydrophobic and hydrophilic agents | 1. Typically micro-size range 2. Limited ultrasound sensitivity |
| No shell | ||||
| Encapsulation material | Polymer (PLGA, PLA, PBCA) | |||
| Phospholipid (DSPC, DPPC, DMPC) | ||||
| UCA-Particle complex | UCA | Phospholipid (DSPC, DPPC) | 1. Improved ultrasound sensitivity 2. Improved drug release | Limited circulation time compared to polymers |
| Drug carrier | Phospholipid (various PCs) | |||
| Polymer (PLA, PLGA, PEG) | ||||
| Miscellaneous material (metallic particles, proteins, etc.) | ||||
| Coned shape particles | Air-entrapped polymer (PLA, PLGA) | 1. Biocompatible 2. Long circulation time 3. Biodegradability | 1. Large size 2. Limited ultrasound sensitivity | |
| Mesoporous particles | Air-entrapped silica | 1. Long circulation time 2. Biocompatible | Limited ultrasound sensitivity | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Honari, A.; Sirsi, S.R. The Evolution and Recent Trends in Acoustic Targeting of Encapsulated Drugs to Solid Tumors: Strategies beyond Sonoporation. Pharmaceutics 2023, 15, 1705. https://doi.org/10.3390/pharmaceutics15061705
Honari A, Sirsi SR. The Evolution and Recent Trends in Acoustic Targeting of Encapsulated Drugs to Solid Tumors: Strategies beyond Sonoporation. Pharmaceutics. 2023; 15(6):1705. https://doi.org/10.3390/pharmaceutics15061705
Chicago/Turabian StyleHonari, Arvin, and Shashank R. Sirsi. 2023. "The Evolution and Recent Trends in Acoustic Targeting of Encapsulated Drugs to Solid Tumors: Strategies beyond Sonoporation" Pharmaceutics 15, no. 6: 1705. https://doi.org/10.3390/pharmaceutics15061705