

Targeted Microbubbles for Drug, Gene, and Cell Delivery in Therapy and Immunotherapy


Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Contrast Agent | Manufacturer | Indications | Shell | Gas | Concentration (MBs/mL) | Size (Diameter) | Half-Life (min) | Volume Dose (μL/kg) a | Mechanical Properties | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| Optison | GE Healthcare | LVO/EBD | Protein: HSA ψ0 = −9.5 to −25.3 mV | C3F8 | 5–8 × 108 | 3.0–4.5 μm (max. 32 μm) 95% < 10 μm | 0.5 ± 0.3 | 6 | f = 2–4 MHz χ = 0.9 N/m | [39,40,41,42,43] |
| Definity | Lantheus | LVO/EBD, breast, liver, vascular. | Phospholipid: DPPC, DPPA, DPPE-mPEG5000 ψ0 = −1.1 to −4.2 mV | C3F8 | 1.2 × 1010 | 1.1–3.3 (max. 20 μm) 98% < 10 μm | 2.0 ± 0.3 | 10 | f = 2–6 MHz χ = 0.5–2.5 N/m | [40,42,43,44,45,46] |
| SonoVue | Bracco | LVO/EBD, breast, liver, vascular, urinary tract. | Phospholipid: DSPC, DPPG, PA ψ0 = −28.3 mV | SF6 | 1.5–2.5 × 108 | 1.5–2.5 (max. 20 μm) 99% < 10 μm | 1.04 ± 0.15 | 25 | f = 1.5–2 MHz χ = 0.2–0.3 N/m | [40,44,47,48,49] |
| Sonazoid | GE Healthcare | Myocardial perfusion, liver, breast. | Phospholipid: H-EPS ψ0 = −76 to −82 mV | C4F10 | 1.2 × 109 | 1.0–5.0 (max. 10 μm) 99.9% < 7 μm | 2.6 ± 0.2 | 15 | f = 4–6 MHz χ = 0.6 N/m | [50,51,52] |
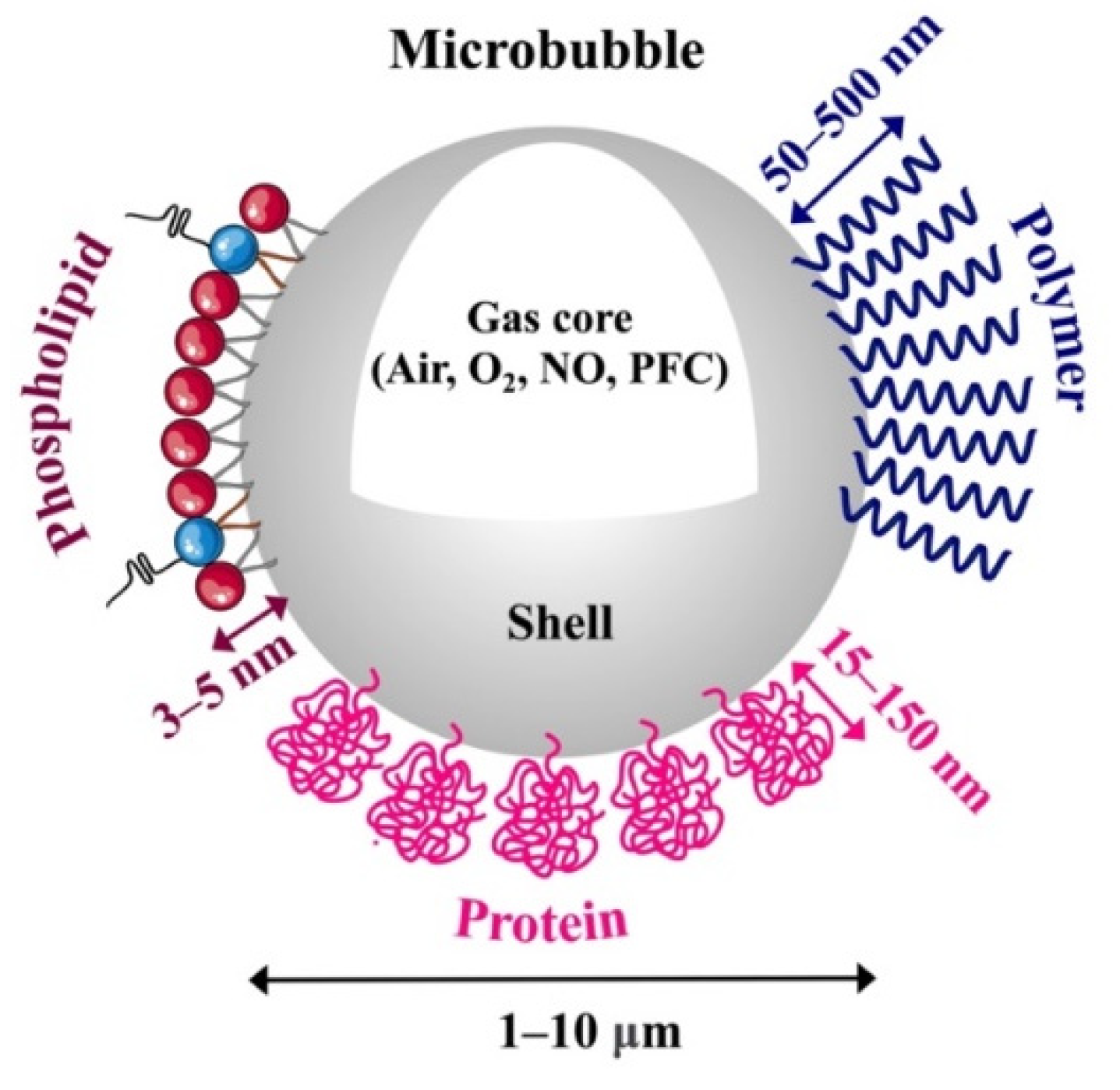
2. Microbubble Formulations
2.1. Shell Composition
2.1.1. Phospholipid-Coated Microbubbles
2.1.2. Protein-Coated Microbubbles
2.1.3. Polymer-Coated Microbubbles
2.2. Gas Composition
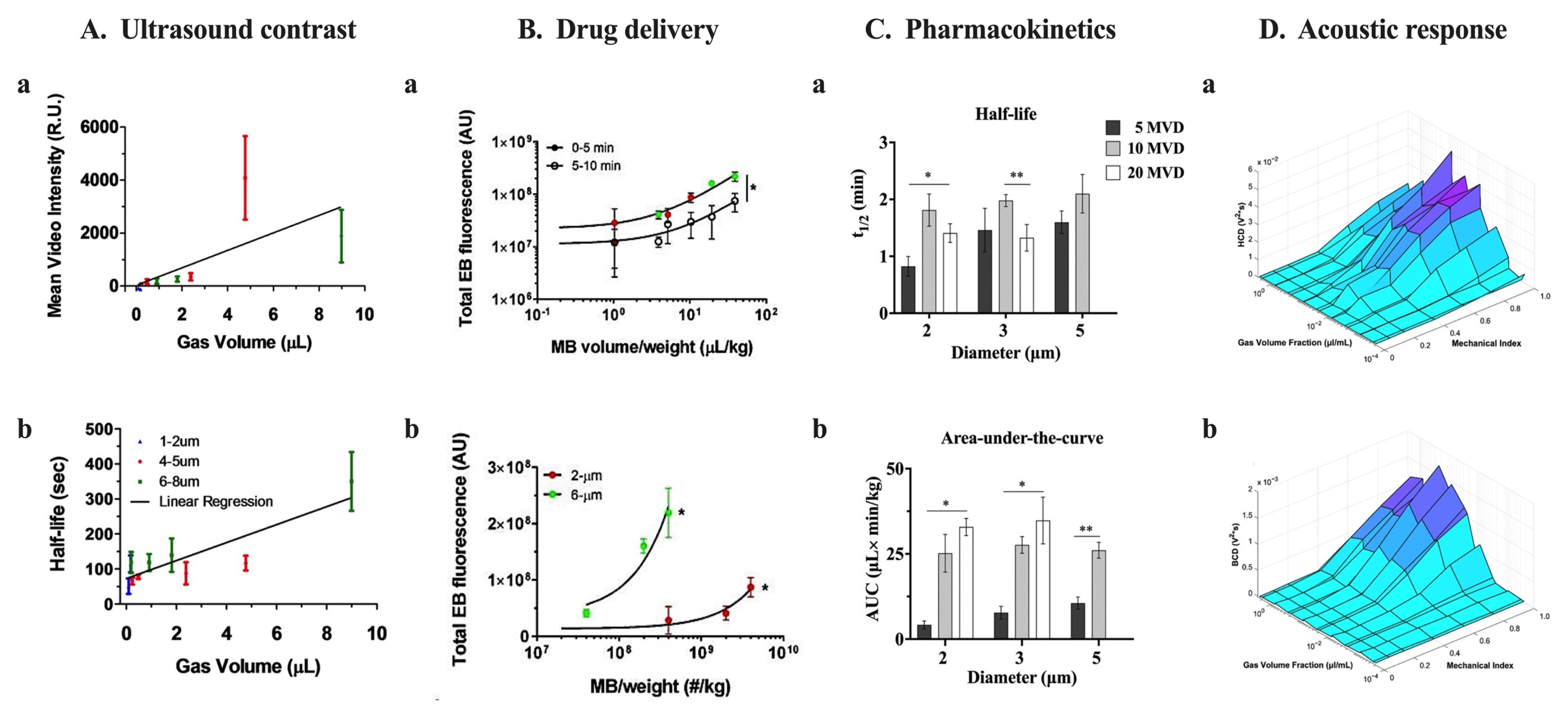
2.3. Size and Microbubble Volume Dose
2.4. Methods to Control Microbubble Size Distributions
2.4.1. Differential Centrifugation
2.4.2. Microfluidic Devices
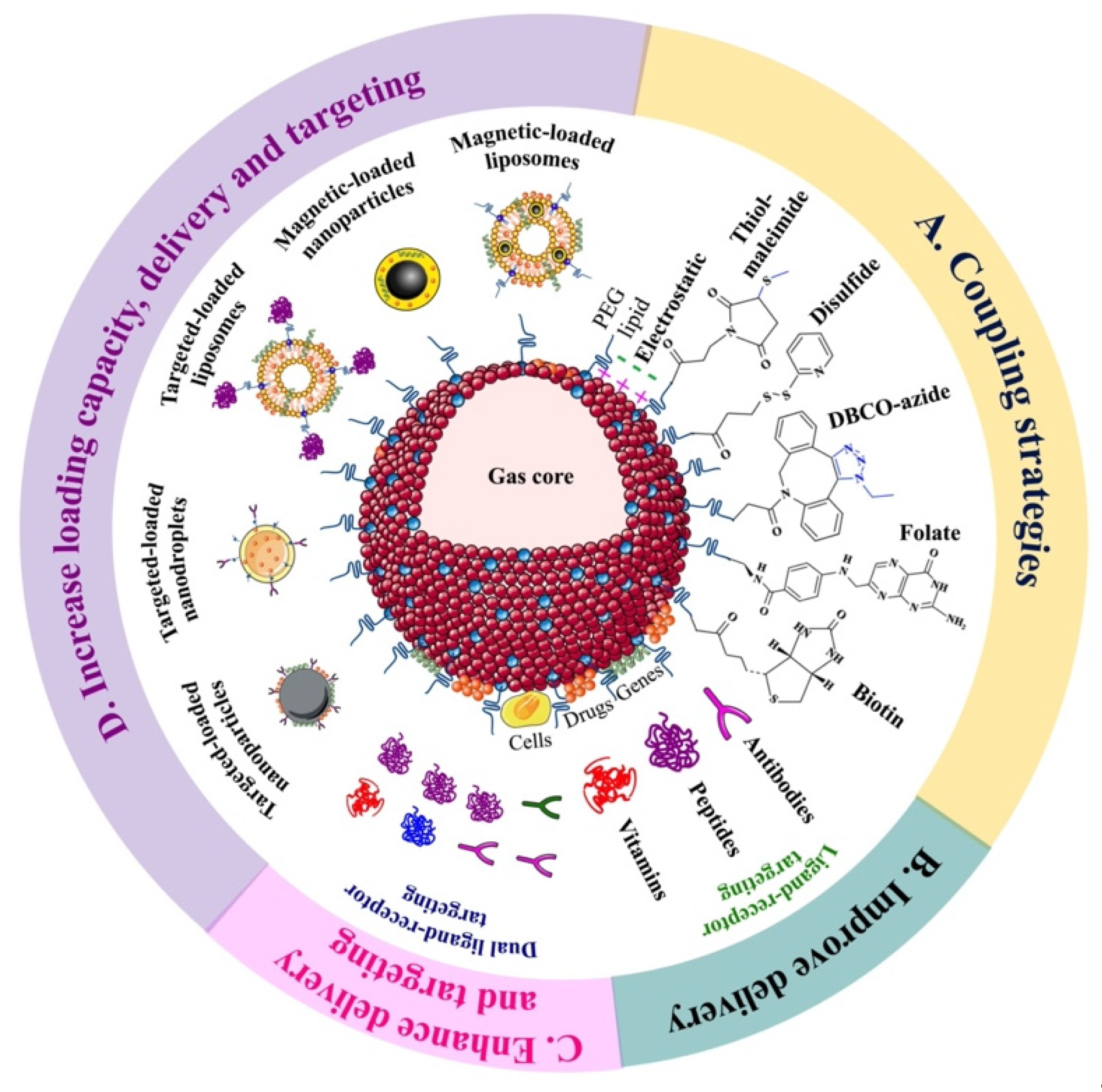
3. Targeted Microbubbles for Therapeutic Applications
3.1. Microbubbles Targeted with a Therapeutic Ligand
3.2. Drug or Gene Loaded-MBs Targeted with a Ligand
3.3. Drug-, Gene- or Cell-Loaded MBs Targeted with Two Different Ligands
3.4. MBs Conjugated with Magnetically or Molecularly Targeted Loaded Carriers
4. Targeted Microbubbles for Immunotherapy Applications
4.1. Monoclonal Antibody Immunotherapy
4.2. Immune Checkpoint Inhibitor Therapy
4.3. Adoptive Cell Immunotherapy
4.4. Cytokine Immunotherapy
4.5. Vaccine Immunotherapy
5. Challenges of tMBs in Therapy and Immunotherapy
6. Future Directions
- The design and characterization of tMB formulations to achieve high payload capacity, stable drug loading, homogenous and reproducible size distributions and colloidal stability, and strong echogenicity and ultrasound responsiveness.
- The understanding of tMB pharmacokinetics with the goal of extending circulation time and improving biodistribution, and determination of minimum effective dose and maximum tolerated dose for a given drug and US scheme.
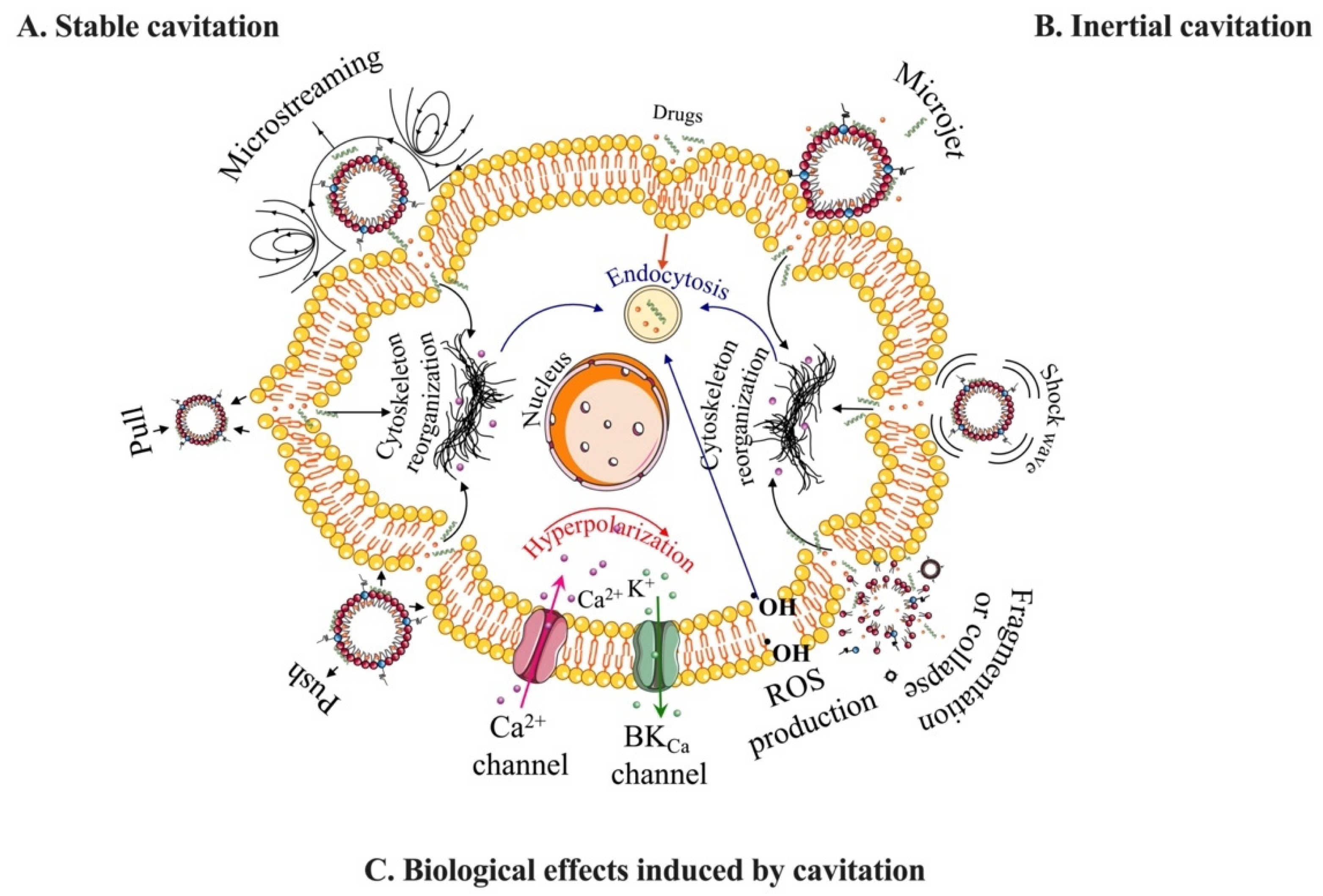
- The evaluation of tMB interactions with cells and tissues, their correlation to short- and long-term bioeffects in vivo, and molecular description of biological mechanisms induced by tMB cavitation.
- The optimization of US protocols with consideration of tMB pharmacokinetics and bioeffects to ensure treatment safety and efficacy.
- The establishment of drug, microbubble, and ultrasound dose metrics to compare therapeutic index between tMB formulations.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Epstein, P.S.; Plesset, M.S. On the Stability of Gas Bubbles in Liquid-Gas Solutions. J. Chem. Phys. 1950, 18, 1505–1509. [Google Scholar] [CrossRef]
- Segers, T.; Lohse, D.; Versluis, M.; Frinking, P. Universal Equations for the Coalescence Probability and Long-Term Size Stability of Phospholipid-Coated Monodisperse Microbubbles Formed by Flow Focusing. Langmuir 2017, 33, 10329–10339. [Google Scholar] [CrossRef]
- Sirsi, S.R.; Borden, M.A. Microbubble Compositions, Properties and Biomedical Applications. Bubble Sci. Eng. Technol. 2009, 1, 3–17. [Google Scholar] [CrossRef]
- Borden, M.A.; Song, K.-H. Reverse Engineering the Ultrasound Contrast Agent. Adv. Colloid Interface Sci. 2018, 262, 39–49. [Google Scholar] [CrossRef]
- Frinking, P.; Segers, T.; Luan, Y.; Tranquart, F. Three Decades of Ultrasound Contrast Agents: A Review of the Past, Present and Future Improvements. Ultrasound Med. Biol. 2020, 46, 892–908. [Google Scholar] [CrossRef]
- Borden, M.A.; Dayton, P.A.; Slagle, C.; Walmer, R.W. Ultrasound Contrast Agents. In Molecular Imaging; Elsevier: Amsterdam, The Netherlands, 2021; pp. 639–653. ISBN 978-0-12-816386-3. [Google Scholar]
- Stride, E.; Segers, T.; Lajoinie, G.; Cherkaoui, S.; Bettinger, T.; Versluis, M.; Borden, M. Microbubble Agents: New Directions. Ultrasound Med. Biol. 2020, 46, 1326–1343. [Google Scholar] [CrossRef]
- Sennoga, C.A.; Kanbar, E.; Auboire, L.; Dujardin, P.-A.; Fouan, D.; Escoffre, J.-M.; Bouakaz, A. Microbubble-Mediated Ultrasound Drug-Delivery and Therapeutic Monitoring. Expert Opin. Drug Deliv. 2017, 14, 1031–1043. [Google Scholar] [CrossRef]
- Lammertink, B.H.A.; Bos, C.; Deckers, R.; Storm, G.; Moonen, C.T.W.; Escoffre, J.-M. Sonochemotherapy: From Bench to Bedside. Front. Pharmacol. 2015, 6, 138. [Google Scholar] [CrossRef]
- He, J.; Liu, Z.; Zhu, X.; Xia, H.; Gao, H.; Lu, J. Ultrasonic Microbubble Cavitation Enhanced Tissue Permeability and Drug Diffusion in Solid Tumor Therapy. Pharmaceutics 2022, 14, 1642. [Google Scholar] [CrossRef]
- Escoffre, J.-M.; Sekkat, N.; Oujagir, E.; Bodard, S.; Mousset, C.; Presset, A.; Chautard, R.; Ayoub, J.; Lecomte, T.; Bouakaz, A. Delivery of Anti-Cancer Drugs Using Microbubble-Assisted Ultrasound in Digestive Oncology: From Preclinical to Clinical Studies. Expert Opin. Drug Deliv. 2022, 19, 421–433. [Google Scholar] [CrossRef]
- Negishi, Y.; Endo-Takahashi, Y.; Maruyama, K. Gene Delivery Systems by the Combination of Lipid Bubbles and Ultrasound. DDT 2016, 10, 248–255. [Google Scholar] [CrossRef]
- Sirsi, S.R.; Borden, M.A. Advances in Ultrasound Mediated Gene Therapy Using Microbubble Contrast Agents. Theranostics 2012, 2, 1208–1222. [Google Scholar] [CrossRef]
- Rychak, J.J.; Klibanov, A.L. Nucleic Acid Delivery with Microbubbles and Ultrasound. Adv. Drug Deliv. Rev. 2014, 72, 82–93. [Google Scholar] [CrossRef]
- Tong, J.; Ding, J.; Shen, X.; Chen, L.; Bian, Y.; Ma, G.; Yao, Y.; Yang, F. Mesenchymal Stem Cell Transplantation Enhancement in Myocardial Infarction Rat Model under Ultrasound Combined with Nitric Oxide Microbubbles. PLoS ONE 2013, 8, e80186. [Google Scholar] [CrossRef]
- Toma, C.; Fisher, A.; Wang, J.; Chen, X.; Grata, M.; Leeman, J.; Winston, B.; Kaya, M.; Fu, H.; Lavery, L.; et al. Vascular Endoluminal Delivery of Mesenchymal Stem Cells Using Acoustic Radiation Force. Tissue Eng. Part A 2011, 17, 1457–1464. [Google Scholar] [CrossRef]
- Sun, T.; Gao, F.; Li, X.; Cai, Y.; Bai, M.; Li, F.; Du, L. A Combination of Ultrasound-Targeted Microbubble Destruction with Transplantation of Bone Marrow Mesenchymal Stem Cells Promotes Recovery of Acute Liver Injury. Stem Cell Res 2018, 9, 356. [Google Scholar] [CrossRef]
- Zhu, T.; Huang, X.; Peng, S.; Ye, Y.; Zhao, J. Ultrasound Targeted Microbubble Destruction Promotes the Therapeutic Effect of HUMSC Transplantation on Glaucoma-Caused Optic Nerve Injury in Rabbits. Trans. Vis. Sci. Tech. 2022, 11, 12. [Google Scholar] [CrossRef]
- Cui, H.; Zhu, Q.; Xie, Q.; Liu, Z.; Gao, Y.; He, Y.; Tan, X.; Xu, Y. Low Intensity Ultrasound Targeted Microbubble Destruction Assists MSCs Delivery and Improves Neural Function in Brain Ischaemic Rats. J. Drug Target. 2020, 28, 320–329. [Google Scholar] [CrossRef]
- Zhu, Q.; Xu, X.; Chen, B.; Liao, Y.; Guan, X.; He, Y.; Cui, H.; Rong, Y.; Liu, Z.; Xu, Y. Ultrasound-targeted Microbubbles Destruction Assists Dual Delivery of Beta-amyloid Antibody and Neural Stem Cells to Restore Neural Function in Transgenic Mice of Alzheimer’s Disease. Med. Phys. 2022, 49, 1357–1367. [Google Scholar] [CrossRef]
- Schoen, S.; Kilinc, M.S.; Lee, H.; Guo, Y.; Degertekin, F.L.; Woodworth, G.F.; Arvanitis, C. Towards Controlled Drug Delivery in Brain Tumors with Microbubble-Enhanced Focused Ultrasound. Adv. Drug Deliv. Rev. 2022, 180, 114043. [Google Scholar] [CrossRef]
- Song, K.-H.; Harvey, B.K.; Borden, M.A. State-of-the-Art of Microbubble-Assisted Blood-Brain Barrier Disruption. Theranostics 2018, 8, 4393–4408. [Google Scholar] [CrossRef]
- Wang, J.; Li, Z.; Pan, M.; Fiaz, M.; Hao, Y.; Yan, Y.; Sun, L.; Yan, F. Ultrasound-Mediated Blood–Brain Barrier Opening: An Effective Drug Delivery System for Theranostics of Brain Diseases. Adv. Drug Deliv. Rev. 2022, 190, 114539. [Google Scholar] [CrossRef]
- Unger, E.; Porter, T.; Lindner, J.; Grayburn, P. Cardiovascular Drug Delivery with Ultrasound and Microbubbles. Adv. Drug Deliv. Rev. 2014, 72, 110–126. [Google Scholar] [CrossRef]
- Qian, L.; Thapa, B.; Hong, J.; Zhang, Y.; Zhu, M.; Chu, M.; Yao, J.; Xu, D. The Present and Future Role of Ultrasound Targeted Microbubble Destruction in Preclinical Studies of Cardiac Gene Therapy. J. Thorac. Dis. 2018, 10, 1099–1111. [Google Scholar] [CrossRef]
- Chen, H.H.; Matkar, P.N.; Afrasiabi, K.; Kuliszewski, M.A.; Leong-Poi, H. Prospect of Ultrasound-Mediated Gene Delivery in Cardiovascular Applications. Expert Opin. Biol. Ther. 2016, 16, 815–826. [Google Scholar] [CrossRef]
- Wanigasekara, J.; de Carvalho, A.M.A.; Cullen, P.J.; Tiwari, B.; Curtin, J.F. Converging Technologies: Targeting the Hallmarks of Cancer Using Ultrasound and Microbubbles. Trends Cancer 2021, 7, 886–890. [Google Scholar] [CrossRef]
- Tu, J.; Zhang, H.; Yu, J.; Liufu, C.; Chen, Z. Ultrasound-Mediated Microbubble Destruction: A New Method in Cancer Immunotherapy. OTT 2018, 11, 5763–5775. [Google Scholar] [CrossRef]
- Li, H.; Zhang, Y.; Shu, H.; Lv, W.; Su, C.; Nie, F. Highlights in Ultrasound-Targeted Microbubble Destruction-Mediated Gene/Drug Delivery Strategy for Treatment of Malignancies. Int. J. Pharm. 2022, 613, 121412. [Google Scholar] [CrossRef]
- Han, Y.; Sun, J.; Wei, H.; Hao, J.; Liu, W.; Wang, X. Ultrasound-Targeted Microbubble Destruction: Modulation in the Tumor Microenvironment and Application in Tumor Immunotherapy. Front. Immunol. 2022, 13, 937344. [Google Scholar] [CrossRef]
- Ho, Y.-J.; Li, J.-P.; Fan, C.-H.; Liu, H.-L.; Yeh, C.-K. Ultrasound in Tumor Immunotherapy: Current Status and Future Developments. J. Control. Release 2020, 323, 12–23. [Google Scholar] [CrossRef]
- Omata, D.; Munakata, L.; Maruyama, K.; Suzuki, R. Ultrasound and Microbubble-Mediated Drug Delivery and Immunotherapy. J. Med. Ultrason. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Yang, Y.; Li, Q.; Guo, X.; Tu, J.; Zhang, D. Mechanisms Underlying Sonoporation: Interaction between Microbubbles and Cells. Ultrason. Sonochem. 2020, 67, 105096. [Google Scholar] [CrossRef]
- Deprez, J.; Lajoinie, G.; Engelen, Y.; De Smedt, S.C.; Lentacker, I. Opening Doors with Ultrasound and Microbubbles: Beating Biological Barriers to Promote Drug Delivery. Adv. Drug Deliv. Rev. 2021, 172, 9–36. [Google Scholar] [CrossRef]
- Qin, P.; Han, T.; Yu, A.C.H.; Xu, L. Mechanistic Understanding the Bioeffects of Ultrasound-Driven Microbubbles to Enhance Macromolecule Delivery. J. Control. Release 2018, 272, 169–181. [Google Scholar] [CrossRef]
- Kooiman, K.; Vos, H.J.; Versluis, M.; de Jong, N. Acoustic Behavior of Microbubbles and Implications for Drug Delivery. Adv. Drug Deliv. Rev. 2014, 72, 28–48. [Google Scholar] [CrossRef]
- Martinez, P.; Bottenus, N.; Borden, M. Cavitation Characterization of Size-Isolated Microbubbles in a Vessel Phantom Using Focused Ultrasound. Pharmaceutics 2022, 14, 1925. [Google Scholar] [CrossRef]
- Wischhusen, J.; Padilla, F. Ultrasound-Targeted Microbubble Destruction (UTMD) for Localized Drug Delivery into Tumor Tissue. IRBM 2019, 40, 10–15. [Google Scholar] [CrossRef]
- Chatterjee, D.; Sarkar, K. A Newtonian Rheological Model for the Interface of Microbubble Contrast Agents. Ultrasound Med. Biol. 2003, 29, 1749–1757. [Google Scholar] [CrossRef]
- Ja’afar, F.; Leow, C.H.; Garbin, V.; Sennoga, C.A.; Tang, M.-X.; Seddon, J.M. Surface Charge Measurement of SonoVue, Definity and Optison: A Comparison of Laser Doppler Electrophoresis and Micro-Electrophoresis. Ultrasound Med. Biol. 2015, 41, 2990–3000. [Google Scholar] [CrossRef]
- Shi, W.T.; Forsberg, F. Ultrasonic Characterization of the Nonlinear Properties of Contrast Microbubbles. Ultrasound Med. Biol. 2000, 26, 93–104. [Google Scholar] [CrossRef]
- Tan, J.-K.Y.; Pham, B.; Zong, Y.; Perez, C.; Maris, D.O.; Hemphill, A.; Miao, C.H.; Matula, T.J.; Mourad, P.D.; Wei, H.; et al. Microbubbles and Ultrasound Increase Intraventricular Polyplex Gene Transfer to the Brain. J. Control. Release 2016, 231, 86–93. [Google Scholar] [CrossRef]
- Fix, S.M.; Nyankima, A.G.; McSweeney, M.D.; Tsuruta, J.K.; Lai, S.K.; Dayton, P.A. Accelerated Clearance of Ultrasound Contrast Agents Containing Polyethylene Glycol Is Associated with the Generation of Anti-Polyethylene Glycol Antibodies. Ultrasound Med. Biol. 2018, 44, 1266–1280. [Google Scholar] [CrossRef]
- Tu, J.; Swalwell, J.E.; Giraud, D.; Cui, W.; Chen, W.; Matula, T.J. Microbubble Sizing and Shell Characterization Using Flow Cytometry. IEEE Trans. Ultrason. Ferroelect. Freq. Contr. 2011, 58, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Helfield, B.L.; Goertz, D.E. Nonlinear Resonance Behavior and Linear Shell Estimates for DefinityTM and MicroMarkerTM Assessed with Acoustic Microbubble Spectroscopy. J. Acoust. Soc. Am. 2013, 133, 1158–1168. [Google Scholar] [CrossRef]
- Chatterjee, D.; Sarkar, K.; Jain, P.; Schreppler, N.E. On the Suitability of Broadband Attenuation Measurement for Characterizing Contrast Microbubbles. Ultrasound Med. Biol. 2005, 31, 781–786. [Google Scholar] [CrossRef]
- Tu, J.; Guan, J.; Qiu, Y.; Matula, T.J. Estimating the Shell Parameters of SonoVue ® Microbubbles Using Light Scattering. J. Acoust. Soc. Am. 2009, 126, 2954–2962. [Google Scholar] [CrossRef]
- Gorce, J.-M.; Arditi, M.; Schneider, M. Influence of Bubble Size Distribution on the Echogenicity of Ultrasound Contrast Agents: A Study of SonoVue? Investig. Radiol. 2000, 35, 661–671. [Google Scholar] [CrossRef]
- Wu, S.-K.; Chu, P.-C.; Chai, W.-Y.; Kang, S.-T.; Tsai, C.-H.; Fan, C.-H.; Yeh, C.-K.; Liu, H.-L. Characterization of Different Microbubbles in Assisting Focused Ultrasound-Induced Blood-Brain Barrier Opening. Sci. Rep. 2017, 7, 46689. [Google Scholar] [CrossRef]
- Sarkar, K.; Shi, W.T.; Chatterjee, D.; Forsberg, F. Characterization of Ultrasound Contrast Microbubbles Using in Vitro Experiments and Viscous and Viscoelastic Interface Models for Encapsulation. J. Acoust. Soc. Am. 2005, 118, 539–550. [Google Scholar] [CrossRef]
- Sontum, P.C. Physicochemical Characteristics of SonazoidTM, A New Contrast Agent for Ultrasound Imaging. Ultrasound Med. Biol. 2008, 34, 824–833. [Google Scholar] [CrossRef]
- Landmark, K.E.; Johansen, P.W.; Johnson, J.A.; Johansen, B.; Uran, S.; Skotland, T. Pharmacokinetics of Perfluorobutane Following Intravenous Bolus Injection and Continuous Infusion of SonazoidTM in Healthy Volunteers and in Patients with Reduced Pulmonary Diffusing Capacity. Ultrasound Med. Biol. 2008, 34, 494–501. [Google Scholar] [CrossRef]
- Valdez, M.A.; Fernandez, E.; Matsunaga, T.; Erickson, R.P.; Trouard, T.P. Distribution and Diffusion of Macromolecule Delivery to the Brain via Focused Ultrasound Using Magnetic Resonance and Multispectral Fluorescence Imaging. Ultrasound Med. Biol. 2020, 46, 122–136. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, A.; Dalvi, S.V. Microbubble Formulations: Synthesis, Stability, Modeling and Biomedical Applications. Ultrasound Med. Biol. 2019, 45, 301–343. [Google Scholar] [CrossRef] [PubMed]
- Al-Jawadi, S.; Thakur, S.S. Ultrasound-Responsive Lipid Microbubbles for Drug Delivery: A Review of Preparation Techniques to Optimise Formulation Size, Stability and Drug Loading. Int. J. Pharm. 2020, 585, 119559. [Google Scholar] [CrossRef]
- Borden, M.A. Lipid-Coated Nanodrops and Microbubbles. In Handbook of Ultrasonics and Sonochemistry; Springer: Singapore, 2016; pp. 1075–1100. ISBN 978-981-287-277-7. [Google Scholar]
- Borden, M.A. Intermolecular Forces Model for Lipid Microbubble Shells. Langmuir 2019, 35, 10042–10051. [Google Scholar] [CrossRef]
- Lum, J.S.; Dove, J.D.; Murray, T.W.; Borden, M.A. Single Microbubble Measurements of Lipid Monolayer Viscoelastic Properties for Small-Amplitude Oscillations. Langmuir 2016, 32, 9410–9417. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Costello, M.J.; Duncan, P.B.; Needham, D. Mechanical Properties and Microstructure of Polycrystalline Phospholipid Monolayer Shells: Novel Solid Microparticles. Langmuir 2003, 19, 8455–8466. [Google Scholar] [CrossRef]
- Borden, M.A.; Longo, M.L. Oxygen Permeability of Fully Condensed Lipid Monolayers. J. Phys. Chem. B 2004, 108, 6009–6016. [Google Scholar] [CrossRef]
- Pu, G.; Longo, M.L.; Borden, M.A. Effect of Microstructure on Molecular Oxygen Permeation through Condensed Phospholipid Monolayers. J. Am. Chem. Soc. 2005, 127, 6524–6525. [Google Scholar] [CrossRef]
- Borden, M.A.; Kruse, D.E.; Caskey, C.F.; Shukui, Z.; Dayton, P.A.; Ferrara, K.W. Influence of Lipid Shell Physicochemical Properties on Ultrasound-Induced Microbubble Destruction. IEEE Trans. Ultrason. Ferroelect. Freq. Contr. 2005, 52, 1992–2002. [Google Scholar] [CrossRef]
- Garg, S.; Thomas, A.A.; Borden, M.A. The Effect of Lipid Monolayer In-Plane Rigidity on in Vivo Microbubble Circulation Persistence. Biomaterials 2013, 34, 6862–6870. [Google Scholar] [CrossRef] [PubMed]
- Borden, M.A.; Longo, M.L. Dissolution Behavior of Lipid Monolayer-Coated, Air-Filled Microbubbles: Effect of Lipid Hydrophobic Chain Length. Langmuir 2002, 18, 9225–9233. [Google Scholar] [CrossRef]
- van Rooij, T.; Luan, Y.; Renaud, G.; van der Steen, A.F.W.; Versluis, M.; de Jong, N.; Kooiman, K. Non-Linear Response and Viscoelastic Properties of Lipid-Coated Microbubbles: DSPC versus DPPC. Ultrasound Med. Biol. 2015, 41, 1432–1445. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-Y.; Chen, C.C.; Tung, Y.-S.; Olumolade, O.O.; Konofagou, E.E. Effects of the Microbubble Shell Physicochemical Properties on Ultrasound-Mediated Drug Delivery to the Brain. J. Control. Release 2015, 212, 30–40. [Google Scholar] [CrossRef]
- Borden, M.A.; Streeter, J.E.; Sirsi, S.R.; Dayton, P.A. In Vivo Demonstration of Cancer Molecular Imaging with Ultrasound Radiation Force and Buried-Ligand Microbubbles. Mol. Imaging 2013, 12, 357–363. [Google Scholar] [CrossRef]
- Chen, C.C.; Sirsi, S.R.; Homma, S.; Borden, M.A. Effect of Surface Architecture on In Vivo Ultrasound Contrast Persistence of Targeted Size-Selected Microbubbles. Ultrasound Med. Biol. 2012, 38, 492–503. [Google Scholar] [CrossRef]
- Borden, M.A.; Sarantos, M.R.; Stieger, S.M.; Simon, S.I.; Ferrara, K.W.; Dayton, P.A. Ultrasound Radiation Force Modulates Ligand Availability on Targeted Contrast Agents. Mol. Imaging 2006, 5, 139–147. [Google Scholar] [CrossRef]
- Borden, M.A.; Zhang, H.; Gillies, R.J.; Dayton, P.A.; Ferrara, K.W. A Stimulus-Responsive Contrast Agent for Ultrasound Molecular Imaging. Biomaterials 2008, 29, 597–606. [Google Scholar] [CrossRef]
- Chen, C.C.; Borden, M.A. The Role of Poly(Ethylene Glycol) Brush Architecture in Complement Activation on Targeted Microbubble Surfaces. Biomaterials 2011, 32, 6579–6587. [Google Scholar] [CrossRef]
- Kiessling, F.; Fokong, S.; Bzyl, J.; Lederle, W.; Palmowski, M.; Lammers, T. Recent Advances in Molecular, Multimodal and Theranostic Ultrasound Imaging. Adv. Drug Deliv. Rev. 2014, 72, 15–27. [Google Scholar] [CrossRef]
- Rudakovskaya, P.G.; Barmin, R.A.; Kuzmin, P.S.; Fedotkina, E.P.; Sencha, A.N.; Gorin, D.A. Microbubbles Stabilized by Protein Shell: From Pioneering Ultrasound Contrast Agents to Advanced Theranostic Systems. Pharmaceutics 2022, 14, 1236. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Dasgupta, A.; Qu, N.; Rama, E.; Kiessling, F.; Lammers, T. Strategies to Maximize Anthracycline Drug Loading in Albumin Microbubbles. ACS Biomater. Sci. Eng. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Ji, J.; He, X. Preparation of Ultrasound Microbubbles Crosslinked to Albumin Nanoparticles Packaged with Tissue-Type Plasminogen Activator Gene Plasmid and Method of in Vivo Transfection. JEP 2011, 24, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, M.J.; O’Brien, W.D.; Bernock, L.J.; Williams, H.R.; Hamilton, E.; Wu, J.; Oelze, M.L.; Culp, W.C. Production of Uniformly Sized Serum Albumin and Dextrose Microbubbles. Ultrason. Sonochem. 2012, 19, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.L.; Dhanaliwala, A.H.; Dixon, A.J.; Klibanov, A.L.; Hossack, J.A. Synthesis and Characterization of Transiently Stable Albumin-Coated Microbubbles via a Flow-Focusing Microfluidic Device. Ultrasound Med. Biol. 2014, 40, 400–409. [Google Scholar] [CrossRef]
- Upadhyay, A.; Dalvi, S.V. Synthesis, Characterization and Stability of BSA-Encapsulated Microbubbles. RSC Adv. 2016, 6, 15016–15026. [Google Scholar] [CrossRef]
- Lentacker, I.; De Geest, B.G.; Vandenbroucke, R.E.; Peeters, L.; Demeester, J.; De Smedt, S.C.; Sanders, N.N. Ultrasound-Responsive Polymer-Coated Microbubbles That Bind and Protect DNA. Langmuir 2006, 22, 7273–7278. [Google Scholar] [CrossRef]
- Upadhyay, A.; Dalvi, S.V.; Gupta, G.; Khanna, N. Effect of PEGylation on Performance of Protein Microbubbles and Its Comparison with Lipid Microbubbles. Mater. Sci. Eng. C 2017, 71, 425–430. [Google Scholar] [CrossRef]
- Ma, X.; Bussonniere, A.; Liu, Q. A Facile Sonochemical Synthesis of Shell-Stabilized Reactive Microbubbles Using Surface-Thiolated Bovine Serum Albumin with the Traut’s Reagent. Ultrason. Sonochem. 2017, 36, 454–465. [Google Scholar] [CrossRef]
- Liu, X.; Gong, P.; Song, P.; Xie, F.; Miller II, A.L.; Chen, S.; Lu, L. Fast Functionalization of Ultrasound Microbubbles Using Strain Promoted Click Chemistry. Biomater. Sci. 2018, 6, 623–632. [Google Scholar] [CrossRef]
- Narihira, K.; Watanabe, A.; Sheng, H.; Endo, H.; Feril, L.B.; Irie, Y.; Ogawa, K.; Moosavi-Nejad, S.; Kondo, S.; Kikuta, T.; et al. Enhanced Cell Killing and Apoptosis of Oral Squamous Cell Carcinoma Cells with Ultrasound in Combination with Cetuximab Coated Albumin Microbubbles. J. Drug Target. 2018, 26, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-H.; Liao, A.-H.; Chen, J.-H.; Chris Wang, C.-R.; Li, P.-C. Photoacoustic/Ultrasound Dual-Modality Contrast Agent and Its Application to Thermotherapy. J. Biomed. Opt. 2012, 17, 045001. [Google Scholar] [CrossRef] [PubMed]
- Liou, Y.-R.; Wang, Y.-H.; Lee, C.-Y.; Li, P.-C. Buoyancy-Activated Cell Sorting Using Targeted Biotinylated Albumin Microbubbles. PLoS ONE 2015, 10, e0125036. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Chen, S.-P.; Liao, A.-H.; Yang, Y.-C.; Lee, C.-R.; Wu, C.-H.; Wu, P.-C.; Liu, T.-M.; Wang, C.-R.C.; Li, P.-C. Synergistic Delivery of Gold Nanorods Using Multifunctional Microbubbles for Enhanced Plasmonic Photothermal Therapy. Sci. Rep. 2014, 4, 5685. [Google Scholar] [CrossRef]
- Porter, T.R.; Xie, F.; Knapp, D.; Iversen, P.; Marky, L.A.; Tsutsui, J.M.; Maiti, S.; Lof, J.; Radio, S.J.; Kipshidze, N. Targeted Vascular Delivery of Antisense Molecules Using Intravenous Microbubbles. Cardiovasc. Revascularization Med. 2006, 7, 25–33. [Google Scholar] [CrossRef]
- Liao, A.-H.; Wu, S.-Y.; Wang, H.-E.; Weng, C.-H.; Wu, M.-F.; Li, P.-C. Evaluation of 18F-Labeled Targeted Perfluorocarbon-Filled Albumin Microbubbles as a Probe for MicroUS and MicroPET in Tumor-Bearing Mice. Ultrasonics 2013, 53, 320–327. [Google Scholar] [CrossRef]
- Barmin, R.; Rudakovskaya, P.; Gusliakova, O.; Sindeeva, O.; Prikhozhdenko, E.; Maksimova, E.; Obukhova, E.; Chernyshev, V.; Khlebtsov, B.; Solovev, A.; et al. Air-Filled Bubbles Stabilized by Gold Nanoparticle/Photodynamic Dye Hybrid Structures for Theranostics. Nanomaterials 2021, 11, 415. [Google Scholar] [CrossRef] [PubMed]
- Maksimova, E.A.; Barmin, R.A.; Rudakovskaya, P.G.; Sindeeva, O.A.; Prikhozhdenko, E.S.; Yashchenok, A.M.; Khlebtsov, B.N.; Solovev, A.A.; Huang, G.; Mei, Y.; et al. Air-Filled Microbubbles Based on Albumin Functionalized with Gold Nanocages and Zinc Phthalocyanine for Multimodal Imaging. Micromachines 2021, 12, 1161. [Google Scholar] [CrossRef]
- Yoon, Y.I.; Pang, X.; Jung, S.; Zhang, G.; Kong, M.; Liu, G.; Chen, X. Smart Gold Nanoparticle-Stabilized Ultrasound Microbubbles as Cancer Theranostics. J. Mater. Chem. B 2018, 6, 3235–3239. [Google Scholar] [CrossRef]
- Chen, Z.; Chattaraj, R.; Pulsipher, K.W.; Karmacharya, M.B.; Hammer, D.A.; Lee, D.; Sehgal, C.M. Photoacoustic and Ultrasound Dual-Mode Imaging via Functionalization of Recombinant Protein-Stabilized Microbubbles with Methylene Blue. ACS Appl. Bio Mater. 2019, 2, 4020–4026. [Google Scholar] [CrossRef]
- Xiong, X.; Zhao, F.; Shi, M.; Yang, H.; Liu, Y. Polymeric Microbubbles for Ultrasonic Molecular Imaging and Targeted Therapeutics. J. Biomater. Sci. Polym. Ed. 2011, 22, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Dasgupta, A.; Koczera, P.; Schipper, S.; Rommel, D.; Shi, Y.; Kiessling, F.; Lammers, T. Drug Loading in Poly(Butyl Cyanoacrylate)-Based Polymeric Microbubbles. Mol. Pharm. 2020, 17, 2840–2848. [Google Scholar] [CrossRef]
- Estifeeva, T.M.; Barmin, R.A.; Rudakovskaya, P.G.; Nechaeva, A.M.; Luss, A.L.; Mezhuev, Y.O.; Chernyshev, V.S.; Krivoborodov, E.G.; Klimenko, O.A.; Sindeeva, O.A.; et al. Hybrid (Bovine Serum Albumin)/Poly (N-Vinyl-2-Pyrrolidone-Co-Acrylic Acid)-Shelled Microbubbles as Advanced Ultrasound Contrast Agents. ACS Appl. Bio. Mater. 2022, 5, 3338–3348. [Google Scholar] [CrossRef] [PubMed]
- Barmin, R.A.; Dasgupta, A.; Bastard, C.; De Laporte, L.; Rütten, S.; Weiler, M.; Kiessling, F.; Lammers, T.; Pallares, R.M. Engineering the Acoustic Response and Drug Loading Capacity of PBCA-Based Polymeric Microbubbles with Surfactants. Mol. Pharm. 2022, 19, 3256–3266. [Google Scholar] [CrossRef] [PubMed]
- Omata, D.; Maruyama, T.; Unga, J.; Hagiwara, F.; Munakata, L.; Kageyama, S.; Shima, T.; Suzuki, Y.; Maruyama, K.; Suzuki, R. Effects of Encapsulated Gas on Stability of Lipid-Based Microbubbles and Ultrasound-Triggered Drug Delivery. J. Control. Release 2019, 311–312, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Yin, M.; Zhu, S.; Liu, L.; Zhu, Y.; Wang, Z.; Xu, R.X.; Chang, S. Ultrasound-Mediated Destruction of Oxygen and Paclitaxel Loaded Lipid Microbubbles for Combination Therapy in Hypoxic Ovarian Cancer Cells. Ultrason. Sonochem. 2016, 28, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Eisenbrey, J.R.; Shraim, R.; Liu, J.-B.; Li, J.; Stanczak, M.; Oeffinger, B.; Leeper, D.B.; Keith, S.W.; Jablonowski, L.J.; Forsberg, F.; et al. Sensitization of Hypoxic Tumors to Radiation Therapy Using Ultrasound-Sensitive Oxygen Microbubbles. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 88–96. [Google Scholar] [CrossRef]
- Ho, Y.-J.; Chu, S.-W.; Liao, E.-C.; Fan, C.-H.; Chan, H.-L.; Wei, K.-C.; Yeh, C.-K. Normalization of Tumor Vasculature by Oxygen Microbubbles with Ultrasound. Theranostics 2019, 9, 7370–7383. [Google Scholar] [CrossRef]
- Liang, Z.; Chen, H.; Gong, X.; Shi, B.; Lin, L.; Tao, F.; Wu, Q.; Fang, M.; Li, H.; Lu, C.; et al. Ultrasound-Induced Destruction of Nitric Oxide–Loaded Microbubbles in the Treatment of Thrombus and Ischemia–Reperfusion Injury. Front. Pharmacol. 2022, 12, 745693. [Google Scholar] [CrossRef]
- Wang, C.; Yang, F.; Xu, Z.; Shi, D.; Chen, D.; Dai, J.; Gu, N.; Jiang, Q. Intravenous Release of NO from Lipidic Microbubbles Accelerates Deep Vein Thrombosis Resolution in a Rat Model. Thromb. Res. 2013, 131, e31–e38. [Google Scholar] [CrossRef]
- Kwan, J.J.; Kaya, M.; Borden, M.A.; Dayton, P.A. Theranostic Oxygen Delivery Using Ultrasound and Microbubbles. Theranostics 2012, 2, 1174–1184. [Google Scholar] [CrossRef] [PubMed]
- Reusser, T.D.; Song, K.-H.; Ramirez, D.; Benninger, R.K.; Papadopoulou, V.; Borden, M.A. Phospholipid Oxygen Microbubbles for Image-Guided Therapy. Nanotheranostics 2020, 4, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Luo, T.; Sun, J.; Zhu, S.; He, J.; Hao, L.; Xiao, L.; Zhu, Y.; Wang, Q.; Pan, X.; Wang, Z.; et al. Ultrasound-Mediated Destruction of Oxygen and Paclitaxel Loaded Dual-Targeting Microbubbles for Intraperitoneal Treatment of Ovarian Cancer Xenografts. Cancer Lett. 2017, 391, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Y.; Beguin, E.; Nesbitt, H.; Kamila, S.; Owen, J.; Barnsley, L.C.; Callan, B.; O’Kane, C.; Nomikou, N.; Hamoudi, R.; et al. Magnetically Responsive Microbubbles as Delivery Vehicles for Targeted Sonodynamic and Antimetabolite Therapy of Pancreatic Cancer. J. Control. Release 2017, 262, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.-H.; Cheng, Y.-H.; Ting, C.-Y.; Ho, Y.-J.; Hsu, P.-H.; Liu, H.-L.; Yeh, C.-K. Ultrasound/Magnetic Targeting with SPIO-DOX-Microbubble Complex for Image-Guided Drug Delivery in Brain Tumors. Theranostics 2016, 6, 1542–1556. [Google Scholar] [CrossRef]
- Liao, T.; Li, Q.; Zhang, Y.; Yang, Z.; Huang, Z.; Han, F.; Chen, X.; Yin, T.; Ren, J.; Sun, Q. Precise Treatment of Acute Antibody-Mediated Cardiac Allograft Rejection in Rats Using C4d-Targeted Microbubbles Loaded with Nitric Oxide. J. Heart Lung Transplant. 2020, 39, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Sonne, C. Differences in Definity and Optison Microbubble Destruction Rates at a Similar Mechanical Index with Different Real-Time Perfusion Systems. J. Am. Soc. Echocardiogr. 2003, 16, 1178–1185. [Google Scholar] [CrossRef]
- Hyvelin, J.-M.; Gaud, E.; Costa, M.; Helbert, A.; Bussat, P.; Bettinger, T.; Frinking, P. Characteristics and Echogenicity of Clinical Ultrasound Contrast Agents: An In Vitro and In Vivo Comparison Study: Comparison of Clinical Ultrasound Contrast Agents. J. Ultrasound Med. 2017, 36, 941–953. [Google Scholar] [CrossRef]
- McMahon, D.; Lassus, A.; Gaud, E.; Jeannot, V.; Hynynen, K. Microbubble Formulation Influences Inflammatory Response to Focused Ultrasound Exposure in the Brain. Sci. Rep. 2020, 10, 21534. [Google Scholar] [CrossRef] [PubMed]
- Sirsi, S.; Feshitan, J.; Kwan, J.; Homma, S.; Borden, M. Effect of Microbubble Size on Fundamental Mode High Frequency Ultrasound Imaging in Mice. Ultrasound Med. Biol. 2010, 36, 935–948. [Google Scholar] [CrossRef]
- Choi, J.J.; Feshitan, J.A.; Baseri, B.; Shougang, W.; Yao-Sheng, T.; Borden, M.A.; Konofagou, E.E. Microbubble-Size Dependence of Focused Ultrasound-Induced Blood–Brain Barrier Opening in Mice In Vivo. IEEE Trans. Biomed. Eng. 2010, 57, 145–154. [Google Scholar] [CrossRef]
- Samiotaki, G.; Vlachos, F.; Tung, Y.-S.; Konofagou, E.E. A Quantitative Pressure and Microbubble-Size Dependence Study of Focused Ultrasound-Induced Blood-Brain Barrier Opening Reversibility in Vivo Using MRI: FUS-Induced BBB Opening Reversibility. Magn. Reson. Med. 2012, 67, 769–777. [Google Scholar] [CrossRef] [PubMed]
- McMahon, D.; Hynynen, K. Acute Inflammatory Response Following Increased Blood-Brain Barrier Permeability Induced by Focused Ultrasound Is Dependent on Microbubble Dose. Theranostics 2017, 7, 3989–4000. [Google Scholar] [CrossRef]
- Song, K.-H.; Fan, A.C.; Hinkle, J.J.; Newman, J.; Borden, M.A.; Harvey, B.K. Microbubble Gas Volume: A Unifying Dose Parameter in Blood-Brain Barrier Opening by Focused Ultrasound. Theranostics 2017, 7, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Becerra, J.A.; Song, K.-H.; Martinez, P.; Borden, M.A. Microbubble Size and Dose Effects on Pharmacokinetics. ACS Biomater. Sci. Eng. 2022, 8, 1686–1695. [Google Scholar] [CrossRef] [PubMed]
- Bing, C.; Hong, Y.; Hernandez, C.; Rich, M.; Cheng, B.; Munaweera, I.; Szczepanski, D.; Xi, Y.; Bolding, M.; Exner, A.; et al. Characterization of Different Bubble Formulations for Blood-Brain Barrier Opening Using a Focused Ultrasound System with Acoustic Feedback Control. Sci. Rep. 2018, 8, 7986. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wu, S.; Li, L.; Wang, G.; Shen, W.; Xu, Y.; Liu, Z.; Zhuo, Z.; Xia, H.; Tan, K. Ultrasound-Targeted Stromal Cell-Derived Factor-1-Loaded Microbubble Destruction Promotes Mesenchymal Stem Cell Homing to Kidneys in Diabetic Nephropathy Rats. IJN 2014, 9, 5639–5651. [Google Scholar] [CrossRef]
- Metzger, K.; Vogel, S.; Chatterjee, M.; Borst, O.; Seizer, P.; Schönberger, T.; Geisler, T.; Lang, F.; Langer, H.; Rheinlaender, J.; et al. High-Frequency Ultrasound-Guided Disruption of Glycoprotein VI-Targeted Microbubbles Targets Atheroprogressison in Mice. Biomaterials 2015, 36, 80–89. [Google Scholar] [CrossRef]
- Yang, H.; Sun, Y.; Wei, J.; Xu, L.; Tang, Y.; Yang, L.; Zhang, X.; Lu, Y. The Effects of Ultrasound-Targeted Microbubble Destruction (UTMD) Carrying IL-8 Monoclonal Antibody on the Inflammatory Responses and Stability of Atherosclerotic Plaques. Biomed. Pharmacother. 2019, 118, 109161. [Google Scholar] [CrossRef]
- Chang, E.-L.; Ting, C.-Y.; Hsu, P.-H.; Lin, Y.-C.; Liao, E.-C.; Huang, C.-Y.; Chang, Y.-C.; Chan, H.-L.; Chiang, C.-S.; Liu, H.-L.; et al. Angiogenesis-Targeting Microbubbles Combined with Ultrasound-Mediated Gene Therapy in Brain Tumors. J. Control. Release 2017, 255, 164–175. [Google Scholar] [CrossRef]
- Fan, C.-H.; Ting, C.-Y.; Liu, H.-L.; Huang, C.-Y.; Hsieh, H.-Y.; Yen, T.-C.; Wei, K.-C.; Yeh, C.-K. Antiangiogenic-Targeting Drug-Loaded Microbubbles Combined with Focused Ultrasound for Glioma Treatment. Biomaterials 2013, 34, 2142–2155. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Gu, H.; Xu, Y.; Li, F.; Kuang, S.; Wang, Z.; Zhou, X.; Ma, H.; Li, P.; Zheng, Y.; et al. Targeted Antiangiogenesis Gene Therapy Using Targeted Cationic Microbubbles Conjugated with CD105 Antibody Compared with Untargeted Cationic and Neutral Microbubbles. Theranostics 2015, 5, 399–417. [Google Scholar] [CrossRef] [PubMed]
- Nederhoed, J.H.; Ebben, H.P.; Slikkerveer, J.; Hoksbergen, A.W.J.; Kamp, O.; Tangelder, G.-J.; Wisselink, W.; Musters, R.J.P.; Yeung, K.K. Intravenous Targeted Microbubbles Carrying Urokinase versus Urokinase Alone in Acute Peripheral Arterial Thrombosis in a Porcine Model. Ann. Vasc. Surg. 2017, 44, 400–407. [Google Scholar] [CrossRef]
- Wang, X.; Searle, A.K.; Hohmann, J.D.; Liu, A.L.; Abraham, M.-K.; Palasubramaniam, J.; Lim, B.; Yao, Y.; Wallert, M.; Yu, E.; et al. Dual-Targeted Theranostic Delivery of MiRs Arrests Abdominal Aortic Aneurysm Development. Mol. Ther. 2018, 26, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Pu, C.; Chang, S.; Sun, J.; Zhu, S.; Liu, H.; Zhu, Y.; Wang, Z.; Xu, R.X. Ultrasound-Mediated Destruction of LHRHa-Targeted and Paclitaxel-Loaded Lipid Microbubbles for the Treatment of Intraperitoneal Ovarian Cancer Xenografts. Mol. Pharm. 2014, 11, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.; Zhou, L.; Liu, P.; He, Y.; Tan, K.; Chen, Q.; Gao, Y.; Gao, Y. In Vivo Thrombolysis with Targeted Microbubbles Loading Tissue Plasminogen Activator in a Rabbit Femoral Artery Thrombus Model. J. Thromb. Thrombolysis. 2014, 38, 57–64. [Google Scholar] [CrossRef]
- Fan, C.-H.; Chang, E.-L.; Ting, C.-Y.; Lin, Y.-C.; Liao, E.-C.; Huang, C.-Y.; Chang, Y.-C.; Chan, H.-L.; Wei, K.-C.; Yeh, C.-K. Folate-Conjugated Gene-Carrying Microbubbles with Focused Ultrasound for Concurrent Blood-Brain Barrier Opening and Local Gene Delivery. Biomaterials 2016, 106, 46–57. [Google Scholar] [CrossRef]
- Woudstra, L.; Krijnen, P.A.J.; Bogaards, S.J.P.; Meinster, E.; Emmens, R.W.; Kokhuis, T.J.A.; Bollen, I.A.E.; Baltzer, H.; Baart, S.M.T.; Parbhudayal, R.; et al. Development of a New Therapeutic Technique to Direct Stem Cells to the Infarcted Heart Using Targeted Microbubbles: StemBells. Stem Cell Res. 2016, 17, 6–15. [Google Scholar] [CrossRef]
- Woudstra, L.; Meinster, E.; Van Haren, L.; Kay, A.M.; Koopman, M.; Belien, J.A.M.; Morrison, M.C.; Van Rossum, A.C.; Helder, M.N.; Juffermans, L.J.M.; et al. StemBell Therapy Stabilizes Atherosclerotic Plaques after Myocardial Infarction. Cytotherapy 2018, 20, 1143–1154. [Google Scholar] [CrossRef]
- Liu, Y.; Zhou, Y.; Xu, J.; Luo, H.; Zhu, Y.; Zeng, X.; Dong, F.; Wei, Z.; Yan, F.; Zheng, H. Ultrasound Molecular Imaging-Guided Tumor Gene Therapy through Dual-Targeted Cationic Microbubbles. Biomater. Sci. 2021, 9, 2454–2466. [Google Scholar] [CrossRef]
- Luo, W.; Wen, G.; Yang, L.; Tang, J.; Wang, J.; Wang, J.; Zhang, S.; Zhang, L.; Ma, F.; Xiao, L.; et al. Dual-Targeted and PH-Sensitive Doxorubicin Prodrug-Microbubble Complex with Ultrasound for Tumor Treatment. Theranostics 2017, 7, 452–465. [Google Scholar] [CrossRef]
- Zhang, L.; Sun, L.; Tang, Q.; Sun, S.; Zeng, L.; Ma, J.; Li, X.; Ge, H.; Liang, X. Cascade Drug Delivery through Tumor Barriers of Pancreatic Cancer via Ultrasound in Combination with Functional Microbubbles. ACS Biomater. Sci. Eng. 2022, 8, 1583–1595. [Google Scholar] [CrossRef]
- Beguin, E.; Gray, M.D.; Logan, K.A.; Nesbitt, H.; Sheng, Y.; Kamila, S.; Barnsley, L.C.; Bau, L.; McHale, A.P.; Callan, J.F.; et al. Magnetic Microbubble Mediated Chemo-Sonodynamic Therapy Using a Combined Magnetic-Acoustic Device. J. Control. Release 2020, 317, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.-H.; Ting, C.-Y.; Lin, H.-J.; Wang, C.-H.; Liu, H.-L.; Yen, T.-C.; Yeh, C.-K. SPIO-Conjugated, Doxorubicin-Loaded Microbubbles for Concurrent MRI and Focused-Ultrasound Enhanced Brain-Tumor Drug Delivery. Biomaterials 2013, 34, 3706–3715. [Google Scholar] [CrossRef]
- Wang, S.; Guo, X.; Xiu, W.; Liu, Y.; Ren, L.; Xiao, H.; Yang, F.; Gao, Y.; Xu, C.; Wang, L. Accelerating Thrombolysis Using a Precision and Clot-Penetrating Drug Delivery Strategy by Nanoparticle-Shelled Microbubbles. Sci. Adv. 2020, 6, eaaz8204. [Google Scholar] [CrossRef]
- Duan, L.; Yang, F.; He, W.; Song, L.; Qiu, F.; Xu, N.; Xu, L.; Zhang, Y.; Hua, Z.; Gu, N. A Multi-Gradient Targeting Drug Delivery System Based on RGD-l-TRAIL-Labeled Magnetic Microbubbles for Cancer Theranostics. Adv. Funct. Mater. 2016, 26, 8313–8324. [Google Scholar] [CrossRef]
- Dwivedi, P.; Kiran, S.; Han, S.; Dwivedi, M.; Khatik, R.; Fan, R.; Mangrio, F.A.; Du, K.; Zhu, Z.; Yang, C.; et al. Magnetic Targeting and Ultrasound Activation of Liposome–Microbubble Conjugate for Enhanced Delivery of Anticancer Therapies. ACS Appl. Mater. Interfaces 2020, 12, 23737–23751. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, S.; Deng, Z.; Li, L.; Tan, G.; Liu, X.; Zheng, H.; Yan, F. Ultrasound-Triggered Drug Delivery for Breast Tumor Therapy Through IRGD-Targeted Paclitaxel-Loaded Liposome-Microbubble Complexes. J. Biomed. Nanotechnol. 2018, 14, 1384–1395. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Huang, Q.; Wang, F.; Zhang, X.; Hu, J.; Tan, Y.; Huang, N.; Wang, Z.; Wang, Z.; Cheng, Y. Targeted ShRNA-Loaded Liposome Complex Combined with Focused Ultrasound for Blood Brain Barrier Disruption and Suppressing Glioma Growth. Cancer Lett. 2018, 418, 147–158. [Google Scholar] [CrossRef]
- Ingram, N.; McVeigh, L.E.; Abou-Saleh, R.H.; Maynard, J.; Peyman, S.A.; McLaughlan, J.R.; Fairclough, M.; Marston, G.; Valleley, E.M.A.; Jimenez-Macias, J.L.; et al. Ultrasound-Triggered Therapeutic Microbubbles Enhance the Efficacy of Cytotoxic Drugs by Increasing Circulation and Tumor Drug Accumulation and Limiting Bioavailability and Toxicity in Normal Tissues. Theranostics 2020, 10, 10973–10992. [Google Scholar] [CrossRef]
- Charalambous, A.; Mico, V.; McVeigh, L.E.; Marston, G.; Ingram, N.; Volpato, M.; Peyman, S.A.; McLaughlan, J.R.; Wierzbicki, A.; Loadman, P.M.; et al. Targeted Microbubbles Carrying Lipid-Oil-Nanodroplets for Ultrasound-Triggered Delivery of the Hydrophobic Drug, Combretastatin A4. Nanomed. Nanotechnol. Biol. Med. 2021, 36, 102401. [Google Scholar] [CrossRef]
- Liao, A.-H.; Chou, H.-Y.; Hsieh, Y.-L.; Hsu, S.-C.; Wei, K.-C.; Liu, H.-L. Enhanced Therapeutic Epidermal Growth Factor Receptor (EGFR) Antibody Delivery via Pulsed Ultrasound with Targeting Microbubbles for Glioma Treatment. J. Med. Biol. Eng. 2015, 35, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Zhang, Y.; Jin, X.; Chen, G.; Huang, Y.; Wu, D.; Li, G.; Shan, J.; Huang, P.; Chen, J. Concurrent Treatment with Anti-DLL4 Enhances Antitumor and Proapoptotic Efficacy of a γ-Secretase Inhibitor in Gastric Cancer. Transl. Oncol. 2018, 11, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Zhang, J.; Xu, M.; Zhang, L.; Tang, Q.; Chen, J.; Gong, M.; Sun, S.; Ge, H.; Wang, S.; et al. Ultrasound Microbubbles Mediated Sonosensitizer and Antibody Co-Delivery for Highly Efficient Synergistic Therapy on HER2-Positive Gastric Cancer. ACS Appl. Mater. Interfaces 2022, 14, 452–463. [Google Scholar] [CrossRef]
- Kim, D.; Lee, S.S.; Moon, H.; Park, S.Y.; Lee, H.J. PD-L1 Targeting Immune-Microbubble Complex Enhances Therapeutic Index in Murine Colon Cancer Models. Pharmaceuticals 2020, 14, 6. [Google Scholar] [CrossRef]
- Ma, Y.; Han, J.; Jiang, J.; Zheng, Z.; Tan, Y.; Liu, C.; Zhao, Y. Ultrasound Targeting of Microbubble-Bound Anti PD-L1 MAb to Enhance Anti-Tumor Effect of Cisplatin in Cervical Cancer Xenografts Treatment. Life Sci. 2020, 262, 118565. [Google Scholar] [CrossRef]
- Liu, Y.; Jiang, J.; Liu, C.; Zhao, W.; Ma, Y.; Zheng, Z.; Zhou, Q.; Zhao, Y. Synergistic Anti-Tumor Effect of Anti-PD-L1 Antibody Cationic Microbubbles for Delivery of the MiR-34a Gene Combined with Ultrasound on Cervical Carcinoma. Am. J. Transl. Res. 2021, 13, 988–1005. [Google Scholar] [PubMed]
- Li, X.; Khorsandi, S.; Wang, Y.; Santelli, J.; Huntoon, K.; Nguyen, N.; Yang, M.; Lee, D.; Lu, Y.; Gao, R.; et al. Cancer Immunotherapy Based on Image-Guided STING Activation by Nucleotide Nanocomplex-Decorated Ultrasound Microbubbles. Nat. Nanotechnol. 2022, 17, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Nan, Y.; Yuan, Y.; Gong, X.; Sun, Y.; Zhou, H.; Zong, Y.; Zhang, L.; Yu, M. Gas-filled Ultrasound Microbubbles Enhance the Immunoactivity of the HSP70-MAGEA1 Fusion Protein against MAGEA1-expressing Tumours. Mol. Med. Rep. 2018, 18, 315–321. [Google Scholar] [CrossRef]
- Jugniot, N.; Dahl, J.J.; Paulmurugan, R. Immunotheranostic Microbubbles (IMBs)—A Modular Platform for Dendritic Cell Vaccine Delivery Applied to Breast Cancer Immunotherapy. J. Exp. Clin. Cancer Res. 2022, 41, 299. [Google Scholar] [CrossRef]
- Chomas, J.E.; Dayton, P.; May, D.; Ferrara, K. Threshold of Fragmentation for Ultrasonic Contrast Agents. J. Biomed. Opt. 2001, 6, 141. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K.E.; Allen, J.S.; Dayton, P.A.; Chomas, J.E.; Klibaov, A.L.; Ferrara, K.W. Experimental and Theoretical Evaluation of Microbubble Behavior: Effect of Transmitted Phase and Bubble Size. IEEE Trans. Ultrason. Ferroelect. Freq. Contr. 2000, 47, 1494–1509. [Google Scholar] [CrossRef] [PubMed]
- Dayton, P.A.; Allen, J.S.; Ferrara, K.W. The Magnitude of Radiation Force on Ultrasound Contrast Agents. J. Acoust. Soc. Am. 2002, 112, 2183–2192. [Google Scholar] [CrossRef]
- Supponen, O.; Upadhyay, A.; Lum, J.; Guidi, F.; Murray, T.; Vos, H.J.; Tortoli, P.; Borden, M. The Effect of Size Range on Ultrasound-Induced Translations in Microbubble Populations. J. Acoust. Soc. Am. 2020, 147, 3236–3247. [Google Scholar] [CrossRef] [PubMed]
- Segers, T.; Kruizinga, P.; Kok, M.P.; Lajoinie, G.; de Jong, N.; Versluis, M. Monodisperse Versus Polydisperse Ultrasound Contrast Agents: Non-Linear Response, Sensitivity, and Deep Tissue Imaging Potential. Ultrasound Med. Biol. 2018, 44, 1482–1492. [Google Scholar] [CrossRef]
- Wang, S.; Unnikrishnan, S.; Herbst, E.B.; Klibanov, A.L.; Mauldin, F.W.; Hossack, J.A. Ultrasound Molecular Imaging of Inflammation in Mouse Abdominal Aorta. Invest. Radiol. 2017, 52, 499–506. [Google Scholar] [CrossRef]
- Rychak, J.J.; Klibanov, A.L.; Ley, K.F.; Hossack, J.A. Enhanced Targeting of Ultrasound Contrast Agents Using Acoustic Radiation Force. Ultrasound Med. Biol. 2007, 33, 1132–1139. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, P.; Liu, P.; Zhao, Y.; Gao, S.; Tan, K.; Liu, Z. Endothelial Adhesion of Targeted Microbubbles in Both Small and Great Vessels Using Ultrasound Radiation Force. Mol. Imaging 2012, 11, 58–66. [Google Scholar] [CrossRef]
- Wang, S.; Wang, C.Y.; Unnikrishnan, S.; Klibanov, A.L.; Hossack, J.A.; Mauldin, F.W. Optical Verification of Microbubble Response to Acoustic Radiation Force in Large Vessels with In Vivo Results. Investig. Radiol. 2015, 50, 772–784. [Google Scholar] [CrossRef]
- Frinking, P.J.A.; Tardy, I.; Théraulaz, M.; Arditi, M.; Powers, J.; Pochon, S.; Tranquart, F. Effects of Acoustic Radiation Force on the Binding Efficiency of BR55, a VEGFR2-Specific Ultrasound Contrast Agent. Ultrasound Med. Biol. 2012, 38, 1460–1469. [Google Scholar] [CrossRef]
- Gessner, R.C.; Streeter, J.E.; Kothadia, R.; Feingold, S.; Dayton, P.A. An In Vivo Validation of the Application of Acoustic Radiation Force to Enhance the Diagnostic Utility of Molecular Imaging Using 3-D Ultrasound. Ultrasound Med. Biol. 2012, 38, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Becerra, J.A.; Castillo, J.I.; Di Ruzza, F.; Borden, M.A. Monodispersity Increases Adhesion Efficiency and Specificity for Ultrasound-Targeted Microbubbles. ACS Biomater. Sci. Eng. 2023, 9, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Feshitan, J.A.; Chen, C.C.; Kwan, J.J.; Borden, M.A. Microbubble Size Isolation by Differential Centrifugation. J. Colloid Interface Sci. 2009, 329, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Segers, T.; Lassus, A.; Bussat, P.; Gaud, E.; Frinking, P. Improved Coalescence Stability of Monodisperse Phospholipid-Coated Microbubbles Formed by Flow-Focusing at Elevated Temperatures. Lab Chip 2019, 19, 158–167. [Google Scholar] [CrossRef]
- Segers, T.; De Rond, L.; De Jong, N.; Borden, M.; Versluis, M. Stability of Monodisperse Phospholipid-Coated Microbubbles Formed by Flow-Focusing at High Production Rates. Langmuir 2016, 32, 3937–3944. [Google Scholar] [CrossRef]
- Dhanaliwala, A.H.; Chen, J.L.; Wang, S.; Hossack, J.A. Liquid Flooded Flow-Focusing Microfluidic Device for in Situ Generation of Monodisperse Microbubbles. Microfluid. Nanofluid. 2013, 14, 457–467. [Google Scholar] [CrossRef]
- Khan, A.H.; Jiang, X.; Kaushik, A.; Nair, H.S.; Edirisinghe, M.; Mercado-Shekhar, K.P.; Shekhar, H.; Dalvi, S.V. Combining Ultrasound and Capillary-Embedded T-Junction Microfluidic Devices to Scale Up the Production of Narrow-Sized Microbubbles through Acoustic Fragmentation. Langmuir 2022, 38, 10288–10304. [Google Scholar] [CrossRef]
- Gañán-Calvo, A.M.; Gordillo, J.M. Perfectly Monodisperse Microbubbling by Capillary Flow Focusing. Phys. Rev. Lett. 2001, 87, 274501. [Google Scholar] [CrossRef] [PubMed]
- Garstecki, P.; Stone, H.A.; Whitesides, G.M. Mechanism for Flow-Rate Controlled Breakup in Confined Geometries: A Route to Monodisperse Emulsions. Phys. Rev. Lett. 2005, 94, 164501. [Google Scholar] [CrossRef]
- Anna, S.L.; Bontoux, N.; Stone, H.A. Formation of Dispersions Using “Flow Focusing” in Microchannels. Appl. Phys. Lett. 2003, 82, 364–366. [Google Scholar] [CrossRef]
- Wang, H.; Jiang, S.; Zhu, C.; Ma, Y.; Fu, T. Bubble Formation in T-Junctions within Parallelized Microchannels: Effect of Viscoelasticity. Chem. Eng. J. 2021, 426, 131783. [Google Scholar] [CrossRef]
- Dixon, A.J.; Dhanaliwala, A.H.; Chen, J.L.; Hossack, J.A. Enhanced Intracellular Delivery of a Model Drug Using Microbubbles Produced by a Microfluidic Device. Ultrasound Med. Biol. 2013, 39, 1267–1276. [Google Scholar] [CrossRef] [PubMed]
- Peyman, S.A.; Abou-Saleh, R.H.; McLaughlan, J.R.; Ingram, N.; Johnson, B.R.G.; Critchley, K.; Freear, S.; Evans, J.A.; Markham, A.F.; Coletta, P.L.; et al. Expanding 3D Geometry for Enhanced On-Chip Microbubble Production and Single Step Formation of Liposome Modified Microbubbles. Lab Chip 2012, 12, 4544. [Google Scholar] [CrossRef] [PubMed]
- Klibanov, A.L. Ultrasound Molecular Imaging of Cancer: Design and Formulation Strategies of Targeted Contrast Agents. In Molecular Imaging in Oncology; Schober, O., Kiessling, F., Debus, J., Eds.; Recent Results in Cancer Research; Springer International Publishing: Cham, Switzerland, 2020; Volume 216, pp. 319–336. ISBN 978-3-030-42617-0. [Google Scholar]
- Klibanov, A.L. Ligand-Carrying Gas-Filled Microbubbles: Ultrasound Contrast Agents for Targeted Molecular Imaging. Bioconjugate Chem. 2005, 16, 9–17. [Google Scholar] [CrossRef]
- Sambi, M.; Bagheri, L.; Szewczuk, M.R. Current Challenges in Cancer Immunotherapy: Multimodal Approaches to Improve Efficacy and Patient Response Rates. J. Oncol. 2019, 2019, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cruz, E.; Kayser, V. Monoclonal Antibody Therapy of Solid Tumors: Clinical Limitations and Novel Strategies to Enhance Treatment Efficacy. BTT 2019, 13, 33–51. [Google Scholar] [CrossRef]
- Hansel, T.T.; Kropshofer, H.; Singer, T.; Mitchell, J.A.; George, A.J.T. The Safety and Side Effects of Monoclonal Antibodies. Nat. Rev. Drug Discov. 2010, 9, 325–338. [Google Scholar] [CrossRef]
- Fares, C.M.; Van Allen, E.M.; Drake, C.G.; Allison, J.P.; Hu-Lieskovan, S. Mechanisms of Resistance to Immune Checkpoint Blockade: Why Does Checkpoint Inhibitor Immunotherapy Not Work for All Patients? Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 147–164. [Google Scholar] [CrossRef]
- Singh, S.; Hassan, D.; Aldawsari, H.M.; Molugulu, N.; Shukla, R.; Kesharwani, P. Immune Checkpoint Inhibitors: A Promising Anticancer Therapy. Drug Discov. Today 2020, 25, 223–229. [Google Scholar] [CrossRef]
- Rohaan, M.W.; Wilgenhof, S.; Haanen, J.B.A.G. Adoptive Cellular Therapies: The Current Landscape. Virchows Arch. 2019, 474, 449–461. [Google Scholar] [CrossRef]
- Fu, C.; Shi, G.; Liu, Y.-T. Manufacturing Anti-CD19 CAR-Tscm Cells for Immunotherapy Using Innovative Microbubble-Based Technologies for Precision Cell Processing. Blood 2021, 138, 3889. [Google Scholar] [CrossRef]
- Lustig, A.; Manor, T.; Shi, G.; Li, J.; Wang, Y.-T.; An, Y.; Liu, Y.-T.; Weng, N. Lipid Microbubble–Conjugated Anti-CD3 and Anti-CD28 Antibodies (Microbubble-Based Human T Cell Activator) Offer Superior Long-Term Expansion of Human Naive T Cells In Vitro. ImmunoHorizons 2020, 4, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Waldmann, T.A. Cytokines in Cancer Immunotherapy. Cold Spring Harb. Perspect. Biol. 2018, 10, a028472. [Google Scholar] [CrossRef]
- Berraondo, P.; Sanmamed, M.F.; Ochoa, M.C.; Etxeberria, I.; Aznar, M.A.; Pérez-Gracia, J.L.; Rodríguez-Ruiz, M.E.; Ponz-Sarvise, M.; Castañón, E.; Melero, I. Cytokines in Clinical Cancer Immunotherapy. Br. J. Cancer 2019, 120, 6–15. [Google Scholar] [CrossRef]
- Qiu, Y.; Su, M.; Liu, L.; Tang, Y.; Pan, Y.; Sun, J. Clinical Application of Cytokines in Cancer Immunotherapy. DDDT 2021, 15, 2269–2287. [Google Scholar] [CrossRef]
- Figueiredo, M.L.; Figueiredo Neto, M.; Salameh, J.W.; Decker, R.E.; Letteri, R.; Chan-Seng, D.; Emrick, T. Ligand-Mediated Targeting of Cytokine Interleukin-27 Enhances Its Bioactivity In Vivo. Mol. Ther.-Methods Clin. Dev. 2020, 17, 739–751. [Google Scholar] [CrossRef]
- Barua, A.; Yellapa, A.; Bahr, J.M.; Adur, M.K.; Utterback, C.W.; Bitterman, P.; Basu, S.; Sharma, S.; Abramowicz, J.S. Interleukin 16- (IL-16-) Targeted Ultrasound Imaging Agent Improves Detection of Ovarian Tumors in Laying Hens, a Preclinical Model of Spontaneous Ovarian Cancer. BioMed Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Malonis, R.J.; Lai, J.R.; Vergnolle, O. Peptide-Based Vaccines: Current Progress and Future Challenges. Chem. Rev. 2020, 120, 3210–3229. [Google Scholar] [CrossRef]
- Amara, S.; Tiriveedhi, V. The Five Immune Forces Impacting DNA-Based Cancer Immunotherapeutic Strategy. Int. J. Mol. Sci. 2017, 18, 650. [Google Scholar] [CrossRef]
- Saxena, M.; Balan, S.; Roudko, V.; Bhardwaj, N. Towards Superior Dendritic-Cell Vaccines for Cancer Therapy. Nat. Biomed. Eng. 2018, 2, 341–346. [Google Scholar] [CrossRef]
- Lin, M.J.; Svensson-Arvelund, J.; Lubitz, G.S.; Marabelle, A.; Melero, I.; Brown, B.D.; Brody, J.D. Cancer Vaccines: The next Immunotherapy Frontier. Nat. Cancer 2022, 3, 911–926. [Google Scholar] [CrossRef]
- Dewitte, H.; Van Lint, S.; Heirman, C.; Thielemans, K.; De Smedt, S.C.; Breckpot, K.; Lentacker, I. The Potential of Antigen and TriMix Sonoporation Using MRNA-Loaded Microbubbles for Ultrasound-Triggered Cancer Immunotherapy. J. Control. Release 2014, 194, 28–36. [Google Scholar] [CrossRef]
- Song, H.-W.; Lee, H.-S.; Kim, S.-J.; Kim, H.Y.; Choi, Y.H.; Kang, B.; Kim, C.-S.; Park, J.-O.; Choi, E. Sonazoid-Conjugated Natural Killer Cells for Tumor Therapy and Real-Time Visualization by Ultrasound Imaging. Pharmaceutics 2021, 13, 1689. [Google Scholar] [CrossRef]
- Navarro-Becerra, J.A.; Franco-Urquijo, C.A.; Ríos, A.; Escalante, B. Localized Delivery of Caveolin-1 Peptide Assisted by Ultrasound-Mediated Microbubble Destruction Potentiates the Inhibition of Nitric Oxide-Dependent Vasodilation Response. Ultrasound Med. Biol. 2021, 47, 1559–1572. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Becerra, J.A.; Caballero-Robledo, G.A.; Franco-Urquijo, C.A.; Ríos, A.; Escalante, B. Functional Activity and Endothelial-Lining Integrity of Ex Vivo Arteries Exposed to Ultrasound-Mediated Microbubble Destruction. Ultrasound Med. Biol. 2020, 46, 2335–2348. [Google Scholar] [CrossRef]
- Chen, H.; Brayman, A.A.; Evan, A.P.; Matula, T.J. Preliminary Observations on the Spatial Correlation Between Short-Burst Microbubble Oscillations and Vascular Bioeffects. Ultrasound Med. Biol. 2012, 38, 2151–2162. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Brayman, A.A.; Bailey, M.R.; Matula, T.J. Blood Vessel Rupture by Cavitation. Urol. Res. 2010, 38, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Armstrong, W.F.; Miller, D.L. Impact of Myocardial Contrast Echocardiography on Vascular Permeability: Comparison of Three Different Contrast Agents. Ultrasound Med. Biol. 2004, 30, 83–91. [Google Scholar] [CrossRef]
- Miller, D.L.; Lu, X.; Fabiilli, M.; Fields, K.; Dou, C. Frequency Dependence of Petechial Hemorrhage and Cardiomyocyte Injury Induced during Myocardial Contrast Echocardiography. Ultrasound Med. Biol. 2016, 42, 1929–1941. [Google Scholar] [CrossRef]
- White, P.J.; Zhang, Y.-Z.; Power, C.; Vykhodtseva, N.; McDannold, N. Observed Effects of Whole-Brain Radiation Therapy on Focused Ultrasound Blood–Brain Barrier Disruption. Ultrasound Med. Biol. 2020, 46, 1998–2006. [Google Scholar] [CrossRef]
- Sun, T.; Samiotaki, G.; Wang, S.; Acosta, C.; Chen, C.C.; Konofagou, E.E. Acoustic Cavitation-Based Monitoring of the Reversibility and Permeability of Ultrasound-Induced Blood-Brain Barrier Opening. Phys. Med. Biol. 2015, 60, 9079–9094. [Google Scholar] [CrossRef]
- Anderson, N.M.; Simon, M.C. The Tumor Microenvironment. Curr. Biol. 2020, 30, R921–R925. [Google Scholar] [CrossRef] [PubMed]
- Hernot, S.; Klibanov, A.L. Microbubbles in Ultrasound-Triggered Drug and Gene Delivery. Adv. Drug Deliv. Rev. 2008, 60, 1153–1166. [Google Scholar] [CrossRef] [PubMed]
- Jallinoja, V.I.J.; Houghton, J.L. Current Landscape in Clinical Pretargeted Radioimmunoimaging and Therapy. J. Nucl. Med. 2021, 62, 1200–1206. [Google Scholar] [CrossRef] [PubMed]





| Ligand Type | Ligand Species | Conjugation Chemistry | Microbubble Composition | Ultrasound Parameters | Animal/Disease Model | Reference |
|---|---|---|---|---|---|---|
| Protein | SDF-1α | EDC/sulfo-NHS | Shell: DSPC, DPPG, PEG4000-COOH Gas: C3F8 Diameter: 1–5 μm Dose: unknown | f = 4 MHz MI = 1.5 Time = 1.15 min | Rat/Diabetic nephropathy | [119] |
| GPVI-Fc | Avidin-biotin | MicroMarker™ Shell: Phospholipid Gas: C4F10/N2 Diameter: 2.3–2.9 μm Dose: 2.8 × 108 MBs/kg or 5.3 µL/kg MVD | f = 24 MHz Time = 2 min | Mouse/ Atherosclerosis | [120] | |
| Antibody | Aβ 1-42 | Avidin-biotin | Shell: DSPC, DPPA, PEG4000 Gas: C3F8 Diameter: 2.13 μm Dose: 5.8 × 108 MBs/kg or 2.9 µL/kg MVD | f = 3 MHz MI = 0.8 PRF = 50 Hz Time = 5 min | Mouse/Alzheimer’s disease | [20] |
| C4d mAb | Avidin-biotin | Shell: DPPC, DSPE-PEG-2000, -Biotin Gas: C3F8/NO Diameter: 0.96 ± 0.07 μm Dose: 5.8 × 106 MBs/kg or 0.003 µL/kg MVD | f = 13 MHz MI = 0.33 Time = 5 min | Rat/Heterotopic Heart transplant | [108] | |
| IL-8 mAb | Avidin-biotin | USphere™ Labeler Shell: Phospholipid Diameter: 1.8 μm Dose: 1.2 × 109 MBs/kg or 3.6 µL/kg MVD | f = 1 MHz MI = 1.5 Power = 5 W Time = 1 min | Rabbit/ Atherosclerosis | [121] |
| Ligand Type | Targeting Ligand | Therapeutic Molecule | Conjugation Chemistry | Microbubble Composition | Ultrasound Parameters | Animal/Disease Model | Reference |
|---|---|---|---|---|---|---|---|
| Antibody | VEGFR2 mAb | pHSV-TK | Avidin-biotin Electrostatic | Shell: DPPC, DPTAP, DSPE-PEG2000, -Biotin Gas: C3F8 Diameter: 1.1 ± 0.1 μm Dose: 1.8 × 1010 MBs/kg or 12.4 µL/kg MVD | f = 1 MHz PNP = 0.7 MPa PRF = 5 Hz Time = 2 min | Mouse/Glioma tumor | [122] |
| VEGFR2 mAb | BCNU | Avidin-biotin Hydrophobic | Shell: DPPC, DSPE-PEG2000, -Biotin Gas: C3F8 Diameter: 1.79 ± 0.13 μm Dose: 1.4 × 1010 MBs/kg or 41 µL/kg MVD | f = 1 MHz PNP = 0.7 MPa DC = 5% PRF = 5 Hz Time = 1 min | Rat/Glioma tumor | [123] | |
| CD105 | pEZ-M46-ES | Avidin-biotin Electrostatic | Shell: DPPC, Cholesterol, DSPE-PEG2000, -Biotin Gas: C3F8 Diameter: 1.44 ± 0.21 μm Dose: 1.3 × 1010 MBs/kg or 20.6 µL/kg MVD | f = 1 MHz PNP = 0.7 MPa DC = 50% I = 2 W/cm2 PRF = 5 Hz Time = 30 s | Mouse/Hind limb tumor | [124] | |
| RGD | Urokinase | Electrostatic | SonoVue Diameter: 1.5–2.5 μm Dose: 4.4 × 107 MBs/kg or 0.18 µL/kg MVD | f = 1.6 MHz MI = 1.1 PRF = 24 kHz Time = 10 min | Pig/Thrombosis | [125] | |
| VCAM-1 | miR-126 | Avidin-biotin | VisualSonics Target-Ready MBs Shell: Phospholipid Gas: C4F10/N2 Diameter: 1.5 μm Dose: 3.7 × 109 MBs/kg or 6.6 µL/kg MVD | f = 10 MHz MI = 0.66 I = 0.076 W/cm2 Time = 2.5 min | Mouse/Aortic Aneurysm | [126] | |
| Peptides | LHRa | Paclitaxel | Avidin-biotin Hydrophobic | Shell: DPPC, DSPE-PEG2000-Biotin Gas: C3F8 Diameter: 1.8 ± 0.2 μm Dose: 1.5 × 109 MBs/kg or 4.5 µL/kg MVD | f = 0.3 MHz I = 1 W/cm2 DC = 50% Time = 3 min | Mouse/Breast cancer | [127] |
| RGD | tPA | Amine Hydrophobic | Shell: DPPC, DSPC PEG-Amine Gas: C3F8 Diameter: 2.08 ± 0.93 μm Dose: 8.0 × 108 MBs/kg or 3.8 µL/kg MVD | f = 2 MHz MI = 1.4 I = 1.8 W/cm2 DC = 95% PRF = 15 Hz Time = 30 min | Rabbit/ Thrombolysis | [128] | |
| Vitamins | Folate | Paclitaxel | Hydrophobic | Shell: DPPC, DSPE-PEG2000-Folate Gas: O2 Diameter: 1.81 ± 0.04 μm Dose: unknown | f = 0.3 MHz I = 1 W/cm2 Time = 3 min | Mouse/Ovarian cancer | [105] |
| Folate | p-FLuc | Amide Electrostatic | Shell: DPPC, DPTAP, DSPE-PEG2000 Gas: C3F8 Diameter: 3.2 ± 0.1 μm Dose: 1.8 × 108 MBs/kg or 3.1 µL/kg MVD | f = 1 MHz PRF = 5 Hz PNP = 0.7 MPa Time = 1 min | Rat/ Glioma tumor | [129] |
| Targeting Ligands | Therapeutic Molecule | Conjugation Chemistry | Microbubble Composition | Ultrasound Parameters | Animal/Disease Model | Reference |
|---|---|---|---|---|---|---|
| CD90 Ab ICAM-1 Ab | Adipose-derived stem cells | Avidin-biotin | Shell: DSPC, PEG40S, DSPE-PEG2000, -Biotin Gas: C4F10 Diameter: 3.5 μm Dose: 9.3 × 107 MBs/kg or 2.1 µL/kg MVD | f = 1 MHz PNP: 0.1 MPa PRF = 1 kHz DC = 50% Time = 10 min | Rat/Myocardial Infarction | [130] |
| CD90 Ab ICAM-1 Ab | Adipose-derived stem cells | Avidin-biotin | Shell: DSPC, PEG40S, DSPE-PEG2000, -Biotin Gas: C4F10 Diameter: 3.5 μm Dose: 4.6 × 107 MBs/kg or 1 µL/kg MVD | f = 1 MHz PNP: 0.1 MPa PRF = 1 kHz DC = 50% Time = 1 min | Mouse/ Atherosclerosis | [131] |
| CCR2 Ab iRGD peptide | shAKT2 | Avidin-biotin, Electrostatic | Shell: DSPC, Stearic-PEI600, DSPE-PEG2000-iRGD-Biotin Gas: C4F10 Diameter: 1.32 ± 0.22 μm Dose: 5.3 × 109 MBs/kg or 6.3 µL/kg MVD | f = 1 MHz PNP: 1.2 MPa PRF = 1 kHz DC = 50% Time = 10 min | Mouse/Breast cancer | [132] |
| cRGD peptide Folate | Doxorubicin | Avidin-biotin | Shell: DSPC, DSPE-PEG2000, -Biotin Gas: C3F8 Diameter: 5.8 ± 2.1 μm Dose: 1.1 × 1010 MBs/kg or 1.1 mL/kg MVD | f = 10 MHz MI: 0.64 Time = 0.5 min | Mouse/Breast cancer | [133] |
| cRGD and cCLT1 peptide | Paclitaxel | Amide, Hydrophobic | Shell: DSPC, DSPE-PEG2000, -COOH Gas: SF6 Diameter: 1.59 ± 0.54 μm Dose: 1.0×1010 MBs/kg or 21 µL/kg MVD | f = 1 MHz MI = 1.17 DC = 10% I = 2.5 W/cm2 Time = 3 min | Mouse/Pancreatic cancer | [134] |
| Carrier | Type of Targeting | Therapeutic Molecule | Conjugation Chemistry | Microbubble Composition | Ultrasound Parameters | Animal/Disease Model | Reference |
|---|---|---|---|---|---|---|---|
| Nanoparticles | Magnetic | 5-fluorouracil Rose Bengal | Avidin-biotin | Shell: DBPC, DSPE-PEG2000, -Biotin Gas: O2 Diameter: 1–2 μm Dose: 7.0 × 109 MBs/kg or 12.3 µL/kg MVD | f = 1 MHz PNP = 0.85 MPa DC = 30% I = 3.5 W/cm2 PRF = 100 Hz Time = 3.5 min | Mouse/Pancreatic tumor | [106] |
| Magnetic | Doxorubicin | Amide | Shell: DSPC, DSPG DSPE-PEG2000, -Biotin Gas: C3F8 Diameter: 5.4 ± 1.1 μm Dose: 5.7 × 108 MBs/kg or 46.7 µL/kg MVD | f = 1 MHz PNP = 0.3 MPa DC = 30% I = 3.5 W/cm2 PRF = 1 Hz Time = 4 min | Rat/Glioma tumor | [107] | |
| Magnetic | Gemcitabine Rose Bengal | Avidin-biotin | Shell: DBPC, DSPE-PEG2000, -Biotin Gas: O2 Diameter: 1.9 ± 0.4 μm Dose: 5.4 × 109 MBs/kg or 19.5 µL/kg MVD | f = 1.17 MHz PNP = 0.7 MPa DC = 30% Time = 3.5 min | Mouse/Pancreatic tumor | [135] | |
| Magnetic | Doxorubicin | Electrostatic and hydrophobic | Shell: DSPC, DSPG DSPE-PEG2000, -Biotin Gas: C3F8 Diameter: 1.04 ± 0.01 μm Dose: 9.7 × 1010 MBs/kg or 56.8 µL/kg MVD | f = 0.4 MHz PNP = 0.325 MPa Power = 4 W PRF = 1 Hz Time = 1.5 min | Rat/Glioma tumor | [136] | |
| Magnetic | tPA | Electrostatic | Shell: SDS Gas: Air Diameter: 5.36 ± 1.44 μm Dose: 6.4 × 1010 MBs/kg or 0.50 µL/kg MVD | f = 18 MHz DC = 10% Time = 5 min | Mouse/ Thrombolysis | [137] | |
| Magnetic/ molecular | RGD | Amide | Shell: PVA Gas: Air Diameter: 1.37 μm Dose: 5.4 × 108 MBs/kg or 0.70 µL/kg MVD | f = 30 MHz Time = 10 min | Mouse/Colon cancer | [138] | |
| Liposomes | Magnetic | Doxorubicin | Maleimide | Shell: DPPC, DSPE-PEG2000-SPDP Gas: C3F8 Diameter: 4 μm Dose: 7.0 × 109 MBs/kg or 233 µL/kg MVD | f = 1 MHz DC = 30% I = 2 W/cm2 Time = 2 min | Mouse/Pancreatic tumor | [139] |
| Molecular: RGD peptide | Paclitaxel | Avidin-biotin | Shell: DSPC, DSPE-PEG2000, -Biotin Gas: C3F8 Diameter: 1.5 μm Dose: 1.1 × 1010 MBs/kg or 17.8 µL/kg MVD | f = 1 MHz DC = 1% PRF = 1 Hz Time = 2 min | Mouse/Breast cancer | [140] | |
| Molecular: NGR peptide | shBirc5 | Avidin-biotin | Shell: DPPC, Cholesterol DSPE-PEG2000-Biotin Gas: C3F8 Diameter: 2.90 ± 0.38 μm Dose: 2.1 × 1010 MBs/kg or 265.6 µL/kg MVD | f = 1 MHz DC = 50% Power = 1.84 W Time = 1–5 min | Rat/Glioma tumor | [141] | |
| Molecular: VEGFR2 Ab | Irinotecan | Avidin-biotin | MicroMarker™ Shell: Phospholipid Gas: C4F10/N2 Diameter: 1.5 μm Dose: 4.7 × 109 MBs/kg or 8.2 µL/kg MVD | f = 2.2 MHz PNP = 0.26 MPa PRF = 1 Hz Time = 4 min | Mouse/Colorectal cancer | [142] | |
| Nanodroplets | Molecular: VEGFR2 Ab | Combretastatin A4 | Avidin-biotin | Shell: DPPC, DSPE-PEG2000-Biotin Gas: C4F10 Diameter: 2.6 ± 1.5 μm Dose: unknown | f = 2.2 MHz PNP = 0.26 MPa PRF = 1 Hz Time = 5 s | Mouse/Colorectal cancer | [143] |
| Immunotherapy Modality | Therapeutic Molecule | Conjugation Chemistry | MicrobubbleComposition | Ultrasound Parameters | Animal/Disease Model | Reference |
| Monoclonal antibody | EGFR mAb | Avidin-biotin | Targestar™-SA Shell: Phospholipid Gas: C4F10 Diameter: 2.5 μm Dose: 3.6 × 109 MBs/kg or 29.7 µL/kg MVD | f = 400 kHz PRF = 1 Hz Power = 5 W Time = 3–4 min | Mouse/Glioma tumor | [144] |
| DLL4 mAb | Avidin-biotin | Targestar™-SA Shell: Phospholipids Gas: C4F10 Diameter: 2 μm Dose: 5.3 × 108 MBs/kg or 2.2 µL/kg MVD | f = 1 MHz DC= 50% I = 2 W/cm2 Time = 1.5 min | Mouse/Gastric cancer | [145] | |
| Trastuzumab mAb | NHS | Shell: DPSC, DSPE-PEG-2000-NHS, Cholesterol and pyropheophorbide Gas: SF6 Diameter: 1.654 ± 1.07 μm Dose: unknown | f = 1 MHz DC= 50% I = 2 W/cm2 Time = 5 min | Mouse/Gastric cancer | [146] | |
| Immune checkpoint inhibitors | PDL-1 mAb | NHS | Shell: DSPC, DSPE-PEG-2000-NHS. Gas: SF6 Diameter: 1.06 ± 0.31 μm Dose: 6.9 × 1010 MBs/kg or 43.3 µL/kg MVD | f = 1.1 MHz DC = 5% PRF = 100 Hz Time = 0.5 min | Mouse/Colon cancer | [147] |
| PDL-1 mAb and Cisplatin | Avidin-biotin Unbounded | Shell: DPSC, DSPE-PEG-2000, -Biotin Gas: C3F8 Diameter: 1.01 ± 0.14 μm Dose: 1 × 108 MBs/kg or 0.06 µL/kg MVD | f = 1 MHz DC = 50% I = 1W/cm2 PRF = 1 kHz Time = 1.5 min | Mouse/Cervical cancer | [148] | |
| PDL-1 mAb and miR-34a | Avidin-biotin Electrostatic | Shell: DSPC, DSPE-PEG-2000, DSPE-PEG-2000-Biotin, PEI-600 Gas: C3F8 Diameter: 0.940 ± 0.080 μm Dose: 4 × 109 MBs/kg or 1.7 µL/kg MVD | f = 18 MHz DC = 50% I = 1 W/cm2 Time = 1.5 min | Mouse/Cervical cancer | [149] | |
| Vaccine | CD11b mAb and CGAMP | Maleimide | Shell: DSPC, DSPE-PEG-2000, DSPE-PEG-5000-Maleimide Gas: C4F10 Diameter: 2.6 μm Dose: 1.4 × 109 MBs/kg or 13.1 µL/kg MVD | f = 1 MHz DC = 50% I = 4 W/cm2 Time = 2 min | Mouse/Breast cancer | [150] |
| HSP70-MAGEA1 | Electrostatic | Shell: Span 60 and Tween 80 Gas: SF6 Diameter: 6 μm Dose: 1.3 × 109 MBs/kg or 144.7 µL/kg MVD | MI = 0.75 | Mouse/Melanoma tumor | [151] | |
| Dendritic cell plasma membrane fragments | Hydrophobic | Shell: DPPC, DPPA, DSPE-PEG5000 Gas: C3F8 Diameter: 1.21 ± 1.0 μm Dose: 5 × 108 MBs/kg or 0.5 µL/kg MVD | f = 18 MHz MI = 0.75 Time = 5 min | Mouse/Breast cancer | [152] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navarro-Becerra, J.A.; Borden, M.A. Targeted Microbubbles for Drug, Gene, and Cell Delivery in Therapy and Immunotherapy. Pharmaceutics 2023, 15, 1625. https://doi.org/10.3390/pharmaceutics15061625
Navarro-Becerra JA, Borden MA. Targeted Microbubbles for Drug, Gene, and Cell Delivery in Therapy and Immunotherapy. Pharmaceutics. 2023; 15(6):1625. https://doi.org/10.3390/pharmaceutics15061625
Chicago/Turabian StyleNavarro-Becerra, J. Angel, and Mark A. Borden. 2023. "Targeted Microbubbles for Drug, Gene, and Cell Delivery in Therapy and Immunotherapy" Pharmaceutics 15, no. 6: 1625. https://doi.org/10.3390/pharmaceutics15061625