
Targeting the PAI-1 Mechanism with a Small Peptide Increases the Efficacy of Alteplase in a Rabbit Model of Chronic Empyema
 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Animal Protocols
2.2. Ultrasonography
2.3. Metrics of Treatment Efficacy and Pleural Injury
2.4. Docking Site Peptide
2.5. ELISA for Quantitation of Antigens and PAI-1 Activity
2.6. Plasminogen Activating and Fibrinolytic Activity Assays
2.7. Histology
2.8. Immunofluorescence Staining and Imaging
2.9. Data Analysis and Statistics
3. Results
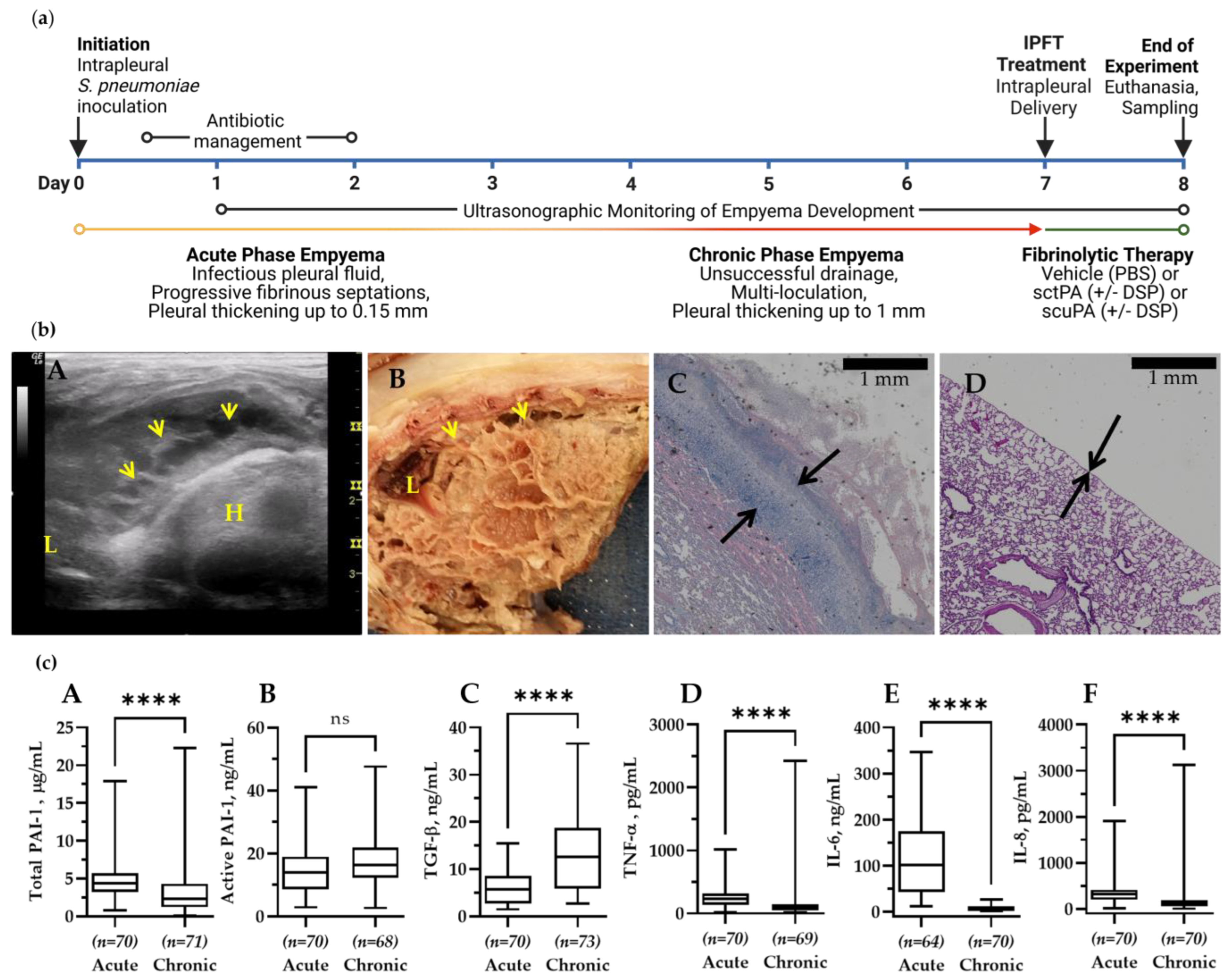
3.1. Chronic Infectious Pleural Injury in Rabbits Recapitulates Advanced-Stage Empyema in Humans
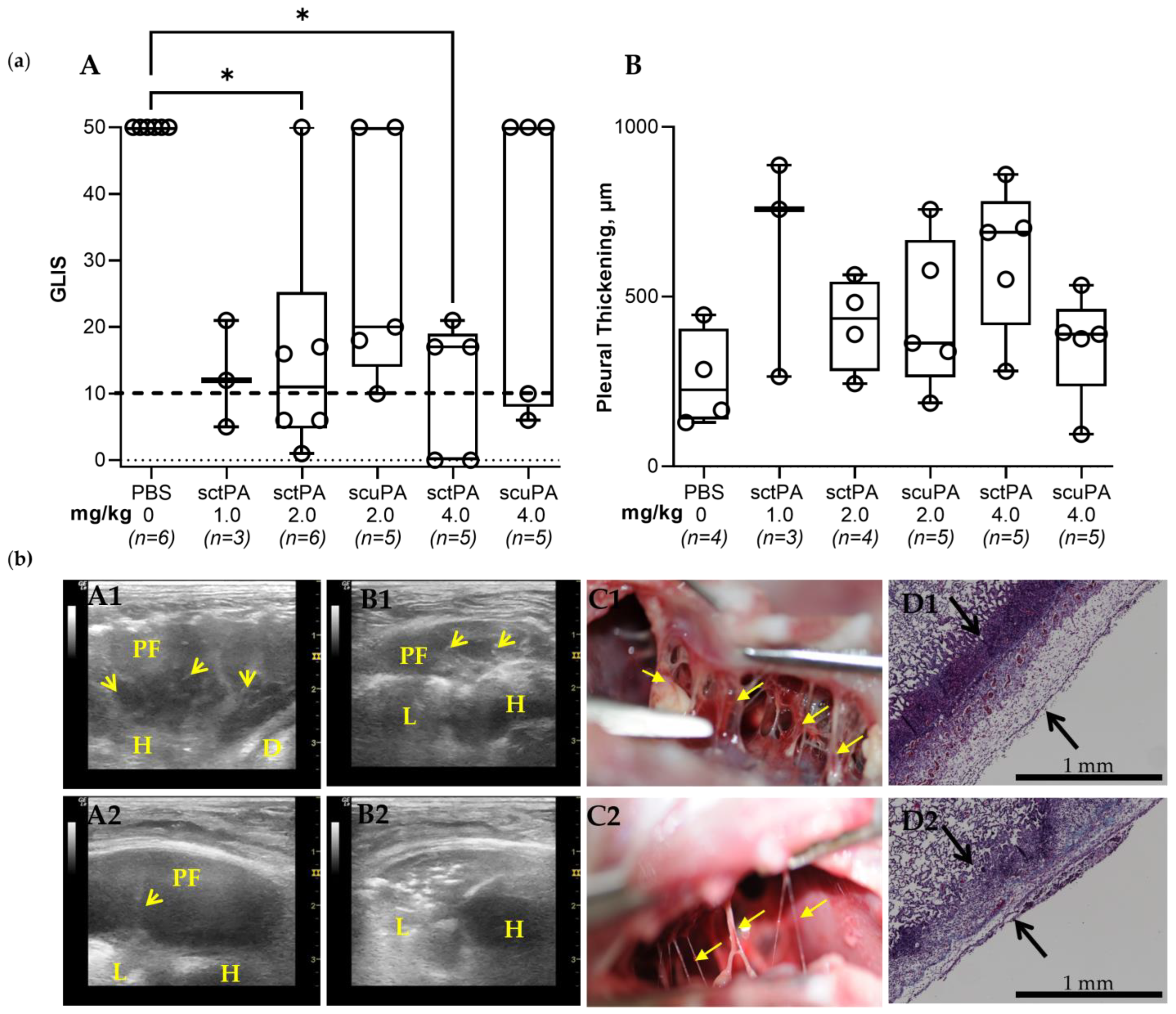
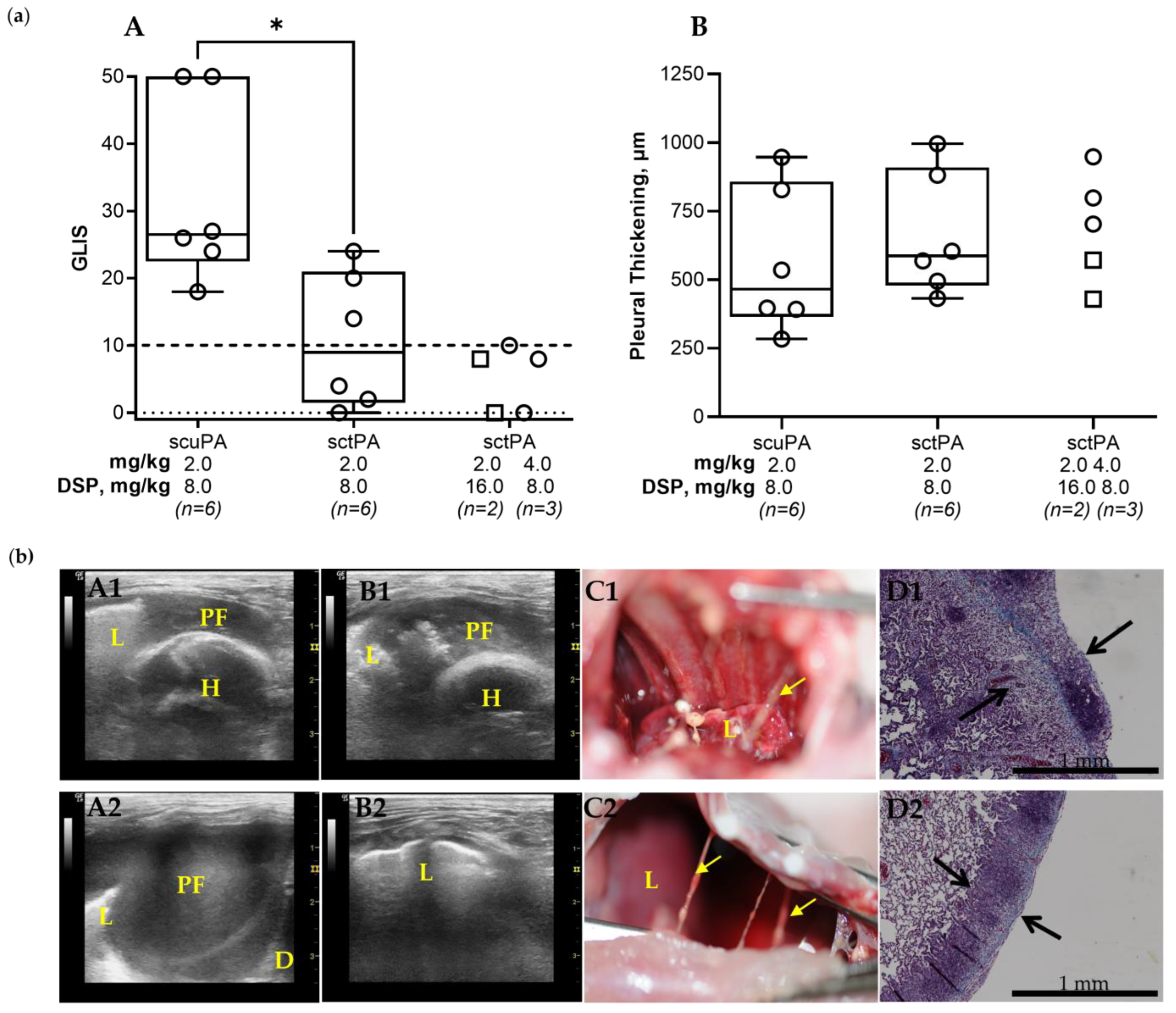
3.2. The Rabbit Model of Chronic Empyema Recapitulates the Decrease in the Efficacy of Fibrinolytic Therapy Observed in Humans with Advanced-Stage Empyema
3.3. DSP-Based PAI-1-Targeted Fibrinolytic Therapy Increases the Efficacy of sctPA in a Rabbit Model of Chronic Empyema
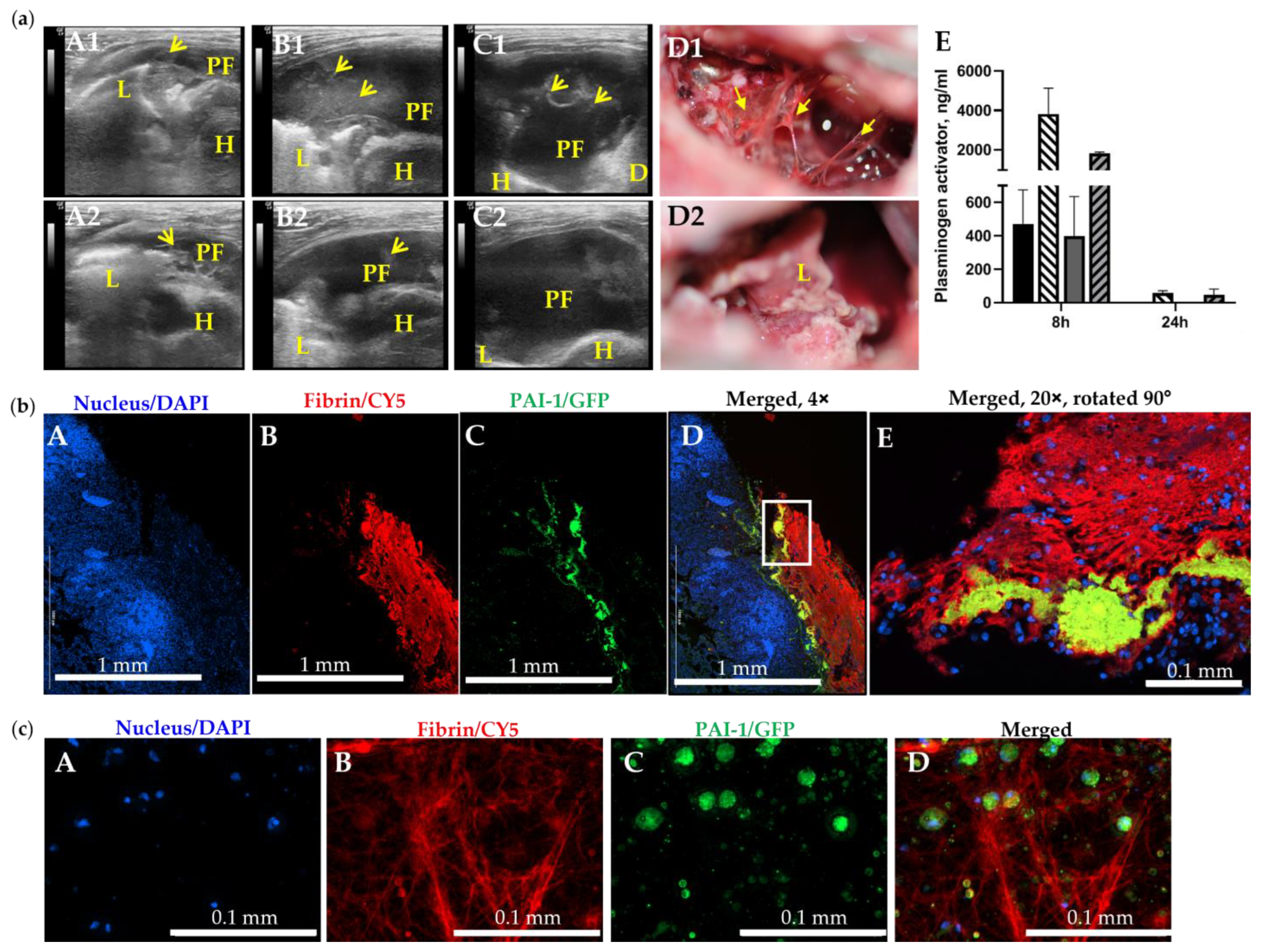
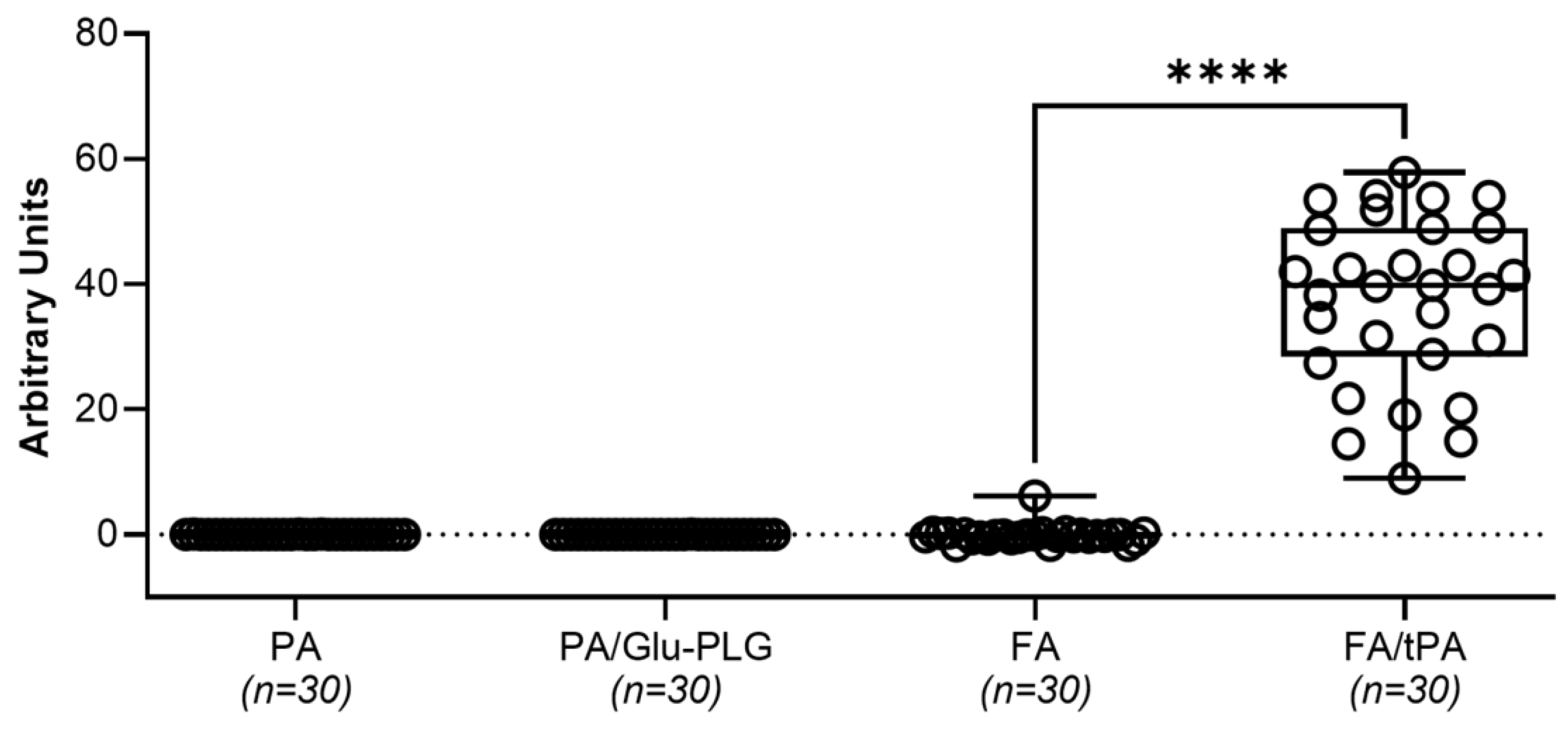
3.4. The Molecular Target, PAI-1, When Incorporated into a Fibrin Mesh, Contributes to the Failure of Fibrinolytic Therapy in Treatment of Chronic Empyema in Rabbits
4. Discussion
5. Conclusions
- Face and predictive validation of a novel model of chronic, advanced-stage empyema that closely recapitulates key physiological indicators seen in empyema in humans;
- PAI-1 is a valid molecular target in S. pneumoniae-induced empyema modeled in rabbits, which closely recapitulates the key characteristics of this disease in humans;
- Multiple injections of fibrinolysins could be tested in this model in order to develop and validate novel approaches to treatment of chronic empyema and expand treatment to patients who are not currently candidates for IPFT or surgery;
- A new form of the molecular target, active PAI-1 that is incorporated into a fibrin mesh could contribute to slow fibrinolysis and failure of IPFT in treatment of advanced-stage empyema;
- Preclinical development and testing of novel, low-dose PAI-1-TFT could result in innovative approaches to treating patients with advanced-stage, organizing pleural injury that fails drainage and is untreatable with surgery or high dose IPFT, as well as creating a foundation for translation to clinical trials.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pleural Disease | PAI-1 Antigen µg/mL | PAI-1 Activity ng/mL | TGF-β ng/mL | TNF-α pg/mL | IL-6 ng/mL | IL-8 ng/mL | Sample Size | References | |
|---|---|---|---|---|---|---|---|---|---|
| Rabbit | Acute Empyema | 5.18 | 16.93 | 12.68 | 174 | 65.54 | 0.25 | n = 64–70 | Figure 1c |
| Chronic Empyema | 0.92 | 15.53 | 18.76 | 70.87 | 1.15 | 0.12 | n = 69–73 | Figure 1c | |
| Human | Complicated Parapneumonic Effusion/Empyema | 0.70 | 40 ** | x | x | x | x | n = 163 | [32] |
| x | x | x | x | x | 4.74 | n = 7 | [74] | ||
| x | x | x | 1352 | 15 | x | n = 11 | [75] | ||
| 1.77 | 34.7 ** | x | 54 | x | 22.10 | n = 25 | [33] | ||
| 2 * | x | x | 30 * | 2.0 * | 6.0 * | n = 17 | [76] | ||
| 0.10 | x | 9.80 | 51.20 | x | x | n = 19 | [34] | ||
| 1.77 | x | x | 56.50 | x | 18.11 | n = 30 | [77] | ||
| x | x | x | 20.50 | x | 4.79 | n = 12 | [78] | ||
| x | x | x | x | x | 5.96 | n = 51 | [79] | ||
| 0.10 | x | x | x | x | 6.48 | n = 22 | [80] | ||
| x | x | 54.60 | x | x | 5.94 | n = 11 | [81] | ||
| 0.29 | x | x | x | x | x | n = 27 | [82] | ||
| x | x | x | x | x | 17.72 | n = 20 | [83] | ||
| 1.57 | x | x | 50.00 | x | x | n = 53 | [44] | ||
| Parapneumonic Effusion | 0.06 | x | 7.20 | 16.50 | x | x | n =11 | [34] | |
| x | x | x | x | 15.30 | 1.88 | n = 12 | [78] | ||
| x | x | x | 90.20 | 22.80 | x | n = 15 | [84] | ||
| 0.15 | x | x | 34.90 | x | x | n = 17 | [85] | ||
| Transudative Effusion | x | x | x | 495 | 0.58 | x | n = 17 | [75] | |
| 0.02 | 0.10 | x | 7 | x | 0.01 | n = 25 | [33] | ||
| x | x | x | x | 0.07 | 109 | n = 9 | [78] | ||
| x | x | x | 18.80 | 0.81 | x | n = 15 | [84] |




References
- Franklin, J.; Talwar, A.; Addala, D.; Helm, E.; Benamore, R.; Rahman, N.; Gleeson, F. CT appearances of pleural infection: Analysis of the Second Multi-centre Intra-pleural Sepsis Trial (MIST 2) cohort. Clin. Radiol. 2021, 76, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Finley, C.; Clifton, J.; Fitzgerald, J.M.; Yee, J. Empyema: An Increasing Concern in Canada. Can. Respir. J. 2008, 15, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Bender, J.M.; Ampofo, K.; Sheng, X.; Pavia, A.T.; Cannon-Albright, L.; Byington, C.L. Parapneumonic Empyema Deaths during Past Century, Utah. Emerg. Infect. Dis. 2009, 15, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Burgos, J.; Lujan, M.; Falcó, V.; Sánchez, A.; Puig-Asensio, M.; Borrego, A.; Fontanals, D.; Planes, A.M.; Pahissa, A.; Rello, J. The Spectrum of Pneumococcal Empyema in Adults in the Early 21st Century. Clin. Infect. Dis. 2011, 53, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Grijalva, C.G.; Zhu, Y.; Nuorti, J.P.; Griffin, M.R. Emergence of parapneumonic empyema in the USA. Thorax 2011, 66, 663–668. [Google Scholar] [CrossRef]
- Burgos, J.; Falcó, V.; Pahissa, A. The increasing incidence of empyema. Curr. Opin. Pulm. Med. 2013, 19, 350–356. [Google Scholar] [CrossRef]
- Bedawi, E.O.; Hassan, M.; Rahman, N.M. Recent developments in the management of pleural infection: A comprehensive review. Clin. Respir. J. 2018, 12, 2309–2320. [Google Scholar] [CrossRef]
- Godfrey, M.S.; Bramley, K.T.; Detterbeck, F. Medical and Surgical Management of Empyema. Semin. Respir. Crit. Care Med. 2019, 40, 361–374. [Google Scholar] [CrossRef]
- Taylor, M.D.; Kozower, B.D. Surgical Spectrum in the Management of Empyemas. Thorac. Surg. Clin. 2012, 22, 431–440. [Google Scholar] [CrossRef]
- Light, R.W. Pleural controversy: Optimal chest tube size for drainage. Respirology 2011, 16, 244–248. [Google Scholar] [CrossRef]
- Sogaard, M.; Nielsen, R.B.; Norgaard, M.; Kornum, J.B.; Schonheyder, H.C.; Thomsen, R.W. Incidence, length of stay, and prognosis of hospitalized patients with pleural empyema: A 15-year Danish nationwide cohort study. Chest 2014, 145, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Reichert, M.; Hecker, M.; Witte, B.; Bodner, J.; Padberg, W.; Weigand, M.; Hecker, A. Stage-directed therapy of pleural empyema. Langenbeck’s Arch. Surg. 2017, 402, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Reichert, M.; Pösentrup, B.; Hecker, A.; Schneck, E.; Pons-Kühnemann, J.; Augustin, F.; Padberg, W.; Öfner, D.; Bodner, J. Thoracotomy versus video-assisted thoracoscopic surgery (VATS) in stage III empyema—An analysis of 217 consecutive patients. Surg. Endosc. 2018, 32, 2664–2675. [Google Scholar] [CrossRef]
- Semenkovich, T.R.; Olsen, M.A.; Puri, V.; Meyers, B.F.; Kozower, B.D. Current State of Empyema Management. Ann. Thorac. Surg. 2018, 105, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Federici, S.; Bédat, B.; Hayau, J.; Gonzalez, M.; Triponez, F.; Krueger, T.; Karenovics, W.; Perentes, J.Y. Outcome of parapneumonic empyema managed surgically or by fibrinolysis: A multicenter study. J. Thorac. Dis. 2021, 13, 6381–6389. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.Y.; Bender, J.M.; Bard, J.D.; Trost, M.J.; Corden, M.H. Something Doesn’t Smell Right: When a Patient with Empyema Isn’t Responding to Guideline-Based Management. Hosp. Pediatr. 2016, 6, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Davies, C.W.H.; Kearney, S.E.; Gleeson, F.V.; Davies, R.J.O. Predictors of Outcome and Long-term Survival in Patients with Pleural Infection. Am. J. Respir. Crit. Care Med. 1999, 160, 1682–1687. [Google Scholar] [CrossRef] [PubMed]
- Khemasuwan, D.; Sorensen, J.; Griffin, D.C. Predictive Variables for Failure in Administration of Intrapleural Tissue Plasminogen Activator/Deoxyribonuclease in Patients with Complicated Parapneumonic Effusions/Empyema. Chest 2018, 154, 550–556. [Google Scholar] [CrossRef]
- Thommi, G.; Nair, C.K.; Aronow, W.S.; Shehan, C.; Meyers, P.; McLeay, M. Efficacy and Safety of Intrapleural Instillation of Alteplase in the Management of Complicated Pleural Effusion or Empyema. Am. J. Ther. 2007, 14, 341–345. [Google Scholar] [CrossRef]
- Abu-Daff, S.; Maziak, D.; Alshehab, D.; Threader, J.; Ivanovic, J.; Deslaurier, V.; Villeneuve, P.-J.; Gilbert, S.; Sundaresan, S.; Shamji, F.; et al. Intrapleural fibrinolytic therapy (IPFT) in loculated pleural effusions—Analysis of predictors for failure of therapy and bleeding: A cohort study. BMJ Open 2013, 3, e001887. [Google Scholar] [CrossRef]
- Ravaglia, C.; Ghirotti, C.; Puglisi, S.; Piciucchi, S.; Gurioli, C.; Fabbri, E.; Sultani, F.; Martinello, S.; Corso, R.M.; Maitan, S.; et al. Medical Thoracoscopy and Intrapleural Fibrinolytic Therapy for the Management of Pleural Empyema: A Cohort Study. Respiration 2023, 102, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Maskell, N.A.; Davies, C.W.; Nunn, A.J.; Hedley, E.L.; Gleeson, F.V.; Miller, R.; Gabe, R.; Rees, G.L.; Peto, T.E.; Woodhead, M.A.; et al. U.K. Controlled Trial of Intrapleural Streptokinase for Pleural Infection. New Engl. J. Med. 2005, 352, 865–874. [Google Scholar] [CrossRef]
- Farjah, F.; Symons, R.G.; Krishnadasan, B.; Wood, D.E.; Flum, D.R. Management of pleural space infections: A population-based analysis. J. Thorac. Cardiovasc. Surg. 2007, 133, 346–351.e1. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-C.; Chen, H.-Y.; Lin, J.-W.; Tseng, Y.-T.; Kuo, S.-W.; Huang, P.-M.; Hsu, H.-H.; Lee, J.-M.; Chen, J.-S.; Lai, H.-S. Acute thoracic empyema: Clinical characteristics and outcome analysis of video-assisted thoracoscopic surgery. J. Formos. Med. Assoc. 2014, 113, 210–218. [Google Scholar] [CrossRef]
- Thommi, G.; Shehan, J.; Robison, K.; Christensen, M.; Backemeyer, L.; McLeay, M. A double blind randomized cross over trial comparing rate of decortication and efficacy of intrapleural instillation of alteplase vs placebo in patients with empyemas and complicated parapneumonic effusions. Respir. Med. 2012, 106, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Thommi, G.; Shehan, C.J.; Mcleay, M.T. Fibrinolytics in Parapneumonic Effusions/Empyemas. Chest 2014, 146, e103–e104. [Google Scholar] [CrossRef]
- Ohara, G.; Iguchi, K.; Satoh, H. VATS and Intrapleural Fibrinolytic Therapy for Parapneumonic Empyema. Ann. Thorac. Cardiovasc. Surg. 2018, 24, 263–264. [Google Scholar] [CrossRef]
- Samancilar, O.; Akçam, T.I.; Kaya, S.O.; Ozturk, O.; Akcay, O.; Ceylan, K.C. The Efficacy of VATS and Intrapleural Fibrinolytic Therapy in Parapneumonic Empyema Treatment. Ann. Thorac. Cardiovasc. Surg. 2018, 24, 19–24. [Google Scholar] [CrossRef]
- Kermenli, T.; Azar, C. Can intrapleural alteplase treatment be an alternative to videothoracoscopic deloculation and decortication in pleural empyema? Wideochir. Inne. Tech. Maloinwazyjne 2021, 16, 580–586. [Google Scholar] [CrossRef]
- Townsend, A.; Raju, H.; Serpa, K.A.; Pruett, R.; Razi, S.S.; Tarrazzi, F.A.; Tami, C.M.; Block, M.I. Tissue plasminogen activator with prolonged dwell time effectively evacuates pleural effusions. BMC Pulm. Med. 2022, 22, 464. [Google Scholar] [CrossRef]
- Akulian, J.; Bedawi, E.O.; Abbas, H.; Argento, C.; Arnold, D.T.; Balwan, A.; Batra, H.; Uribe Becerra, J.P.; Belanger, A.; Berger, K.; et al. Bleeding Risk with Combination Intrapleural Fibrinolytic and Enzyme Therapy in Pleural Infection: An International, Multicenter, Retrospective Cohort Study. Chest 2022, 162, 1384–1392. [Google Scholar] [CrossRef]
- Philip-Joet, F.; Alessi, M.; Aillaud, M.; Barriere, J.R.; Arnaud, A.; Juhan-Vague, I. Fibrinolytic and inflammatory processes in pleural effusions. Eur. Respir. J. 1995, 8, 1352–1356. [Google Scholar] [CrossRef] [PubMed]
- Alemán, C.; Alegre, J.; Monasterio, J.; Segura, R.M.; Armadans, L.; Anglés, A.; Varela, E.; Ruiz, E.; De Sevilla, T.F. Association between inflammatory mediators and the fibrinolysis system in infectious pleural effusions. Clin. Sci. 2003, 105, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.-L.; Chen, C.-H.; Sheu, J.-R.; Chen, Y.-C.; Chang, S.-C. Proinflammatory Cytokines, Transforming Growth Factor-β1, and Fibrinolytic Enzymes in Loculated and Free-Flowing Pleural Exudates. Chest 2005, 128, 690–697. [Google Scholar] [CrossRef] [PubMed]
- van Mourik, J.; A Lawrence, D.; Loskutoff, D.J. Purification of an inhibitor of plasminogen activator (antiactivator) synthesized by endothelial cells. J. Biol. Chem. 1984, 259, 14914–14921. [Google Scholar] [CrossRef]
- Carrell, R.W.; Evans, D.L.; Stein, P.E. Mobile reactive centre of serpins and the control of thrombosis. Nature 1991, 353, 576–578. [Google Scholar] [CrossRef]
- Rahman, N.M.; Maskell, N.A.; West, A.; Teoh, R.; Arnold, A.; Mackinlay, C.; Peckham, D.; Davies, C.W.; Ali, N.; Kinnear, W.; et al. Intrapleural Use of Tissue Plasminogen Activator and DNase in Pleural Infection. N. Engl. J. Med. 2011, 365, 518–526. [Google Scholar] [CrossRef]
- Beckert, L.; Brockway, B.; Simpson, G.; Southcott, A.M.; Lee, Y.C.G.; Rahman, N.; Light, R.W.; Shoemaker, S.; Gillies, J.; Komissarov, A.A.; et al. Phase 1 trial of intrapleural LTI-01; single chain urokinase in complicated parapneumonic effusions or empyema. JCI Insight 2019, 5, e127470. [Google Scholar] [CrossRef]
- Komissarov, A.A.; Florova, G.; Azghani, A.; Karandashova, S.; Kurdowska, A.K.; Idell, S. Active α-macroglobulin is a reservoir for urokinase after fibrinolytic therapy in rabbits with tetracycline-induced pleural injury and in human pleural fluids. Am. J. Physiol. Cell. Mol. Physiol. 2013, 305, L682–L692. [Google Scholar] [CrossRef]
- Florova, G.; Azghani, A.; Karandashova, S.; Schaefer, C.; Koenig, K.; Stewart-Evans, K.; Declerck, P.J.; Idell, S.; Komissarov, A.A. Targeting of Plasminogen Activator Inhibitor 1 Improves Fibrinolytic Therapy for Tetracycline-Induced Pleural Injury in Rabbits. Am. J. Respir. Cell Mol. Biol. 2015, 52, 429–437. [Google Scholar] [CrossRef]
- Florova, G.; Girard, R.A.; Azghani, A.O.; Sarva, K.; Buchanan, A.; Karandashova, S.; DeVera, C.J.; Morris, D.; Chamiso, M.; Koenig, K.; et al. Precision targeting of the plasminogen activator inhibitor-1 mechanism increases efficacy of fibrinolytic therapy in empyema. Physiol. Rep. 2021, 9, e14861. [Google Scholar] [CrossRef] [PubMed]
- Komissarov, A.A.; Florova, G.; Azghani, A.O.; Buchanan, A.; Boren, J.; Allen, T.; Rahman, N.M.; Koenig, K.; Chamiso, M.; Karandashova, S.; et al. Dose dependency of outcomes of intrapleural fibrinolytic therapy in new rabbit empyema models. Am. J. Physiol. Cell. Mol. Physiol. 2016, 311, L389–L399. [Google Scholar] [CrossRef] [PubMed]
- Florova, G.; Azghani, A.O.; Karandashova, S.; Schaefer, C.; Yarovoi, S.V.; Declerck, P.J.; Cines, D.B.; Idell, S.; Komissarov, A.A. Targeting plasminogen activator inhibitor-1 in tetracycline-induced pleural injury in rabbits. Am. J. Physiol. Cell. Mol. Physiol. 2018, 314, L54–L68. [Google Scholar] [CrossRef] [PubMed]
- Bedawi, E.O.; Kanellakis, N.I.; Corcoran, J.P.; Zhao, Y.; Hassan, M.; Asciak, R.; Mercer, R.M.; Sundaralingam, A.; Addala, D.N.; Miller, R.F.; et al. The Biological Role of Pleural Fluid PAI-1 and Sonographic Septations in Pleural Infection: Analysis of a Prospectively Collected Clinical Outcome Study. Am. J. Respir. Crit. Care Med. 2023, 207, 731–739. [Google Scholar] [CrossRef]
- Karandashova, S.; Florova, G.; Azghani, A.O.; Komissarov, A.A.; Koenig, K.; Tucker, T.A.; Allen, T.C.; Stewart, K.; Tvinnereim, A.; Idell, S. Intrapleural Adenoviral Delivery of Human Plasminogen Activator Inhibitor–1 Exacerbates Tetracycline-Induced Pleural Injury in Rabbits. Am. J. Respir. Cell Mol. Biol. 2013, 48, 44–52. [Google Scholar] [CrossRef]
- Komissarov, A.A.; Florova, G.; Azghani, A.O.; Buchanan, A.; Bradley, W.M.; Schaefer, C.; Koenig, K.; Idell, S. The time course of resolution of adhesions during fibrinolytic therapy in tetracycline-induced pleural injury in rabbits. Am. J. Physiol. Lung. Cell. Mol. Physiol. 2015, 309, L562–L572. [Google Scholar] [CrossRef]
- Komissarov, A.A.; Mazar, A.P.; Koenig, K.; Kurdowska, A.K.; Idell, S. Regulation of intrapleural fibrinolysis by urokinase-α-macroglobulin complexes in tetracycline-induced pleural injury in rabbits. Am. J. Physiol. Cell. Mol. Physiol. 2009, 297, L568–L577. [Google Scholar] [CrossRef]
- Komissarov, A.A.; Florova, G.; Idell, S. Effects of Extracellular DNA on Plasminogen Activation and Fibrinolysis. J. Biol. Chem. 2011, 286, 41949–41962. [Google Scholar] [CrossRef]
- Tsovolou, E.-C.; Tzepi, I.-M.; Spyridaki, A.; Tsaganos, T.; Karagianni, V.; Menenakos, E.; Liakou, P.; Sabracos, L.; Zografos, G.; Giamarellos-Bourboulis, E.J. Effect of clarithromycin in experimental empyema by multidrug-resistantPseudomonas aeruginosa. Apmis 2014, 122, 68–75. [Google Scholar] [CrossRef]
- Shang, X.; Wang, D.; Miao, X.; Wang, X.; Li, J.; Yang, Z.; Pan, H. The oxidative status and inflammatory level of the peripheral blood of rabbits infested with Psoroptes cuniculi. Parasites Vectors 2014, 7, 124. [Google Scholar] [CrossRef]
- Alemán, C.; Porcel, J.M.; Alegre, J.; Ruiz, E.; Bielsa, S.; Andreu, J.; Deu, M.; Suñé, P.; Martínez-Sogués, M.; López, I.; et al. Intrapleural Fibrinolysis with Urokinase Versus Alteplase in Complicated Parapneumonic Pleural Effusions and Empyemas: A Prospective Randomized Study. Lung 2015, 193, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Chaddha, U.; Agrawal, A.; Feller-Kopman, D.; Kaul, V.; Shojaee, S.; Maldonado, F.; Ferguson, M.K.; Blyth, K.G.; Grosu, H.B.; Corcoran, J.P.; et al. Use of fibrinolytics and deoxyribonuclease in adult patients with pleural empyema: A consensus statement. Lancet Respir. Med. 2021, 9, 1050–1064. [Google Scholar] [CrossRef] [PubMed]
- Bédat, B.; Plojoux, J.; Noel, J.; Morel, A.; Worley, J.; Triponez, F.; Karenovics, W. Comparison of intrapleural use of urokinase and tissue plasminogen activator/DNAse in pleural infection. ERJ Open Res. 2019, 5, 00084-2019. [Google Scholar] [CrossRef] [PubMed]
- Corcoran, J.P.; Hallifax, R.; Rahman, N.M. Advances in the management of pleural disease. Expert Rev. Respir. Med. 2013, 7, 499–513. [Google Scholar] [CrossRef]
- Corcoran, J.P.; Rahman, N.M.; Psallidas, I. Management of Parapneumonic Effusions and Empyema. Semin. Respir. Crit. Care Med. 2014, 35, 715–722. [Google Scholar] [CrossRef]
- Thomas, R.; Francis, R.; Davies, H.E.; Lee, Y.G. Interventional therapies for malignant pleural effusions: The present and the future. Respirology 2014, 19, 809–822. [Google Scholar] [CrossRef]
- Ferreiro, L.; José, M.E.S.; Valdés, L. Management of parapneumonic pleural effusion in adults. Arch. Bronconeumol. 2015, 51, 637–646. [Google Scholar] [CrossRef]
- Koppurapu, V.; Meena, N. A review of the management of complex para-pneumonic effusion in adults. J. Thorac. Dis. 2017, 9, 2135–2141. [Google Scholar] [CrossRef]
- Komissarov, A.A.; Rahman, N.M.; Lee, Y.C.G.; Florova, G.; Shetty, S.; Idell, R.; Ikebe, M.; Das, K.; Tucker, T.A.; Idell, S. Fibrin turnover and pleural organization: Bench to bedside. Am. J. Physiol. Cell. Mol. Physiol. 2018, 314, L757–L768. [Google Scholar] [CrossRef]
- Idell, S.; Rahman, N.M. Intrapleural Fibrinolytic Therapy for Empyema and Pleural Loculation: Knowns and Unknowns. Ann. Am. Thorac. Soc. 2018, 15, 515–517. [Google Scholar] [CrossRef]
- Komissarov, A.; Idell, S. PAI-1 Drives Septation and Clinical Outcomes in Pleural Infection. Am. J. Respir. Crit. Care Med. 2023, 207, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Idell, S.; Florova, G.; Shetty, S.; Tucker, T.; Idell, R.; Koenig, K.; Azghani, A.; Rahman, N.M.; Komissarov, A. Precision-guided, Personalized Intrapleural Fibrinolytic Therapy for Empyema and Complicated Parapneumonic Pleural Effusions: The Case for The Fibrinolytic Potential. Clin. Pulm. Med. 2017, 24, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Wendler, A.; Wehling, M. Translatability scoring in drug development: Eight case studies. J. Transl. Med. 2012, 10, 39. [Google Scholar] [CrossRef]
- Madison, E.L.; Goldsmith, E.J.; Gerard, R.D.; Gething, M.J.; Sambrook, J.F.; Bassel-Duby, R.S. Amino acid residues that affect interaction of tissue-type plasminogen activator with plasminogen activator inhibitor 1. Proc. Natl. Acad. Sci. USA 1990, 87, 3530–3533. [Google Scholar] [CrossRef] [PubMed]
- Coombs, G.S.; Bergstrom, R.C.; Madison, E.L.; Corey, D.R. Directing sequence-specific proteolysis to new targets. The influence of loop size and target sequence on selective proteolysis by tissue- type plasminogen activator and urokinase-type plasminogen activator. J. Biol. Chem. 1998, 273, 4323–4328. [Google Scholar] [CrossRef] [PubMed]
- Armstead, W.M.; Riley, J.; Kiessling, J.W.; Cines, D.B.; Higazi, A.A.-R. Novel plasminogen activator inhibitor-1-derived peptide protects against impairment of cerebrovasodilation after photothrombosis through inhibition of JNK MAPK. Am. J. Physiol. Integr. Comp. Physiol. 2010, 299, R480–R485. [Google Scholar] [CrossRef] [PubMed]
- Armstead, W.M.; Riley, J.; Kiessling, J.W.; Cines, U.B.; Higazi, A.A.-R. PAI-1-derived peptide EEIIMD prevents impairment of cerebrovasodilation by augmenting p38 MAPK upregulation after cerebral hypoxia/ischemia. Am. J. Physiol. Circ. Physiol. 2010, 299, H76–H80. [Google Scholar] [CrossRef] [PubMed]
- Komissarov, A.A.; Declerck, P.J.; Shore, J.D. Protonation State of a Single Histidine Residue Contributes Significantly to the Kinetics of the Reaction of Plasminogen Activator Inhibitor-1 with Tissue-type Plasminogen Activator. J. Biol. Chem. 2004, 279, 23007–23013. [Google Scholar] [CrossRef]
- Himelman, R.B.; Callen, P.W. The Prognostic Value of Loculations in Parapneumonic Pleural Effusions. Chest 1986, 90, 852–856. [Google Scholar] [CrossRef]
- Temes, R.T.; Follis, F.; Kessler, R.M.; Pett, S.B.; Wernly, J.A. Intrapleural Fibrinolytics in Management of Empyema Thoracis. Chest 1996, 110, 102–106. [Google Scholar] [CrossRef]
- Gilbert, C.R.; Gorden, J.A. Use of intrapleural tissue plasminogen activator and deoxyribonuclease in pleural space infections: An update on alternative regimens. Curr. Opin. Pulm. Med. 2017, 23, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Karandashova, S.; Florova, G.; Idell, S.; Komissarov, A.A. From Bedside to the Bench—A Call for Novel Approaches to Prognostic Evaluation and Treatment of Empyema. Front. Pharmacol. 2021, 12, 806393. [Google Scholar] [CrossRef] [PubMed]
- Marudamuthu, A.S.; Shetty, S.K.; Bhandary, Y.P.; Karandashova, S.; Thompson, M.; Sathish, V.; Florova, G.; Hogan, T.B.; Pabelick, C.M.; Prakash, Y.S.; et al. Plasminogen Activator Inhibitor-1 Suppresses Profibrotic Responses in Fibroblasts from Fibrotic Lungs. J. Biol. Chem. 2015, 290, 9428–9441. [Google Scholar] [CrossRef] [PubMed]
- Ceyhan, B.; Özgün, S.; Çelikel, T.; Yalçin, M.; Koç, M. IL-8 in pleural effusion. Respir. Med. 1996, 90, 215–221. [Google Scholar] [CrossRef]
- Xirouchaki, N.; Tzanakis, N.; Bouros, D.; Kyriakou, D.; Karkavitsas, N.; Alexandrakis, M.; Siafakas, N.M. Diagnostic Value of Interleukin-1α, Interleukin-6, and Tumor Necrosis Factor in Pleural Effusions. Chest 2002, 121, 815–820. [Google Scholar] [CrossRef]
- Lin, F.-C.; Chen, Y.-C.; Chen, F.-J.; Chang, S.-C. Cytokines and fibrinolytic enzymes in tuberculous and parapneumonic effusions. Clin. Immunol. 2005, 116, 166–173. [Google Scholar] [CrossRef]
- Iglesias, D.; Alegre, J.; Aleman, C.; Soriano, T.; Armadans, L.I.; Segura, R.M.; Anglés, A.; Monasterio, J.; De Sevilla, T.F.; Ruiz, E. Metalloproteinases and tissue inhibitors of metalloproteinases in exudative pleural effusions. Eur. Respir. J. 2005, 25, 104–109. [Google Scholar] [CrossRef]
- Akarsu, S.; Kurt, A.N.C.; Doğan, Y.; Yilmaz, E.; Godekmerdan, A.; Aygun, A.D. The Differential Diagnostic Values of Cytokine Levels in Pleural Effusions. Mediat. Inflamm. 2005, 2005, 2–8. [Google Scholar] [CrossRef]
- Porcel, J.M.; Galindo, C.; Esquerda, A.; Trujillano, J.; Ruiz-González, A.; Falguera, M.; Vives, M. Pleural fluid interleukin-8 and C-reactive protein for discriminating complicated non-purulent from uncomplicated parapneumonic effusions. Respirology 2008, 13, 58–62. [Google Scholar] [CrossRef]
- Chung, C.-L.; Hsiao, S.-H.; Hsiao, G.; Sheu, J.-R.; Chen, W.-L.; Chang, S.-C. Clinical Importance of Angiogenic Cytokines, Fibrinolytic Activity and Effusion Size in Parapneumonic Effusions. PLoS ONE 2013, 8, e53169. [Google Scholar] [CrossRef] [PubMed]
- Saraya, T.; Ohkuma, K.; Watanabe, T.; Mikura, S.; Kobayashi, F.; Aso, J.; Nunokawa, H.; Honda, K.; Ogawa, Y.; Tamura, M.; et al. Diagnostic Value of Vascular Endothelial Growth Factor, Transforming Growth Factor-β, Interleukin-8, and the Ratio of Lactate Dehydrogenase to Adenosine Deaminase in Pleural Effusion. Lung 2018, 196, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Zentina, D.; Stukena, I.; Krams, A.; Lejnieks, A. PAI-1 Level Differences in Malignant Plural Effusion, Parapneumonic Pleuritis, and Cardiac Hydrothorax. Medicina 2019, 55, 567. [Google Scholar] [CrossRef]
- Yang, C.-Y.; Kuo, Y.-H.; Chen, M.; Wang, C.-L.; Shih, L.-J.; Liu, Y.-C.; Hsueh, P.-C.; Lai, Y.-H.; Chu, C.-M.; Wu, C.-C.; et al. Pleural cytokines MIF and MIP-3α as novel biomarkers for complicated parapneumonic effusions and empyema. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Kiropoulos, T.S.; Kostikas, K.; Oikonomidi, S.; Tsilioni, I.; Nikoulis, D.; Germenis, A.; Gourgoulianis, K.I. Acute phase markers for the differentiation of infectious and malignant pleural effusions. Respir. Med. 2007, 101, 910–918. [Google Scholar] [CrossRef]
- Gallego-Escuredo, J.M.; Gutierrez, M.D.M.; Diaz-Delfin, J.; Domingo, J.C.; Mateo, M.G.; Domingo, P.; Giralt, M.; Villarroya, F. Differential effects of efavirenz and lopinavir/ritonavir on human adipocyte differentiation, gene expression and release of adipokines and pro-inflammatory cytokines. Curr. HIV Res. 2010, 8, 545–553. [Google Scholar] [CrossRef]




| Minimal Effective Doses *, mg/kg | ||||||
|---|---|---|---|---|---|---|
| Model | Chemically Induced ** | Infectious Acute *** | Infectious Chronic | |||
| Treatment | Alone | PAI-1-TFT | Alone | PAI-1-TFT | Alone | PAI-1-TFT |
| sctPA | 0.145 | 0.073 | 2.0 | 0.25 | >4.0 | ≤2.0 |
| scuPA | 0.50 | 0.063 | 2.0 | 2.0 | >4.0 | >2.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Florova, G.; De Vera, C.J.; Emerine, R.L.; Girard, R.A.; Azghani, A.O.; Sarva, K.; Jacob, J.; Morris, D.E.; Chamiso, M.; Idell, S.; et al. Targeting the PAI-1 Mechanism with a Small Peptide Increases the Efficacy of Alteplase in a Rabbit Model of Chronic Empyema. Pharmaceutics 2023, 15, 1498. https://doi.org/10.3390/pharmaceutics15051498
Florova G, De Vera CJ, Emerine RL, Girard RA, Azghani AO, Sarva K, Jacob J, Morris DE, Chamiso M, Idell S, et al. Targeting the PAI-1 Mechanism with a Small Peptide Increases the Efficacy of Alteplase in a Rabbit Model of Chronic Empyema. Pharmaceutics. 2023; 15(5):1498. https://doi.org/10.3390/pharmaceutics15051498
Chicago/Turabian StyleFlorova, Galina, Christian J. De Vera, Rebekah L. Emerine, René A. Girard, Ali O. Azghani, Krishna Sarva, Jincy Jacob, Danna E. Morris, Mignote Chamiso, Steven Idell, and et al. 2023. "Targeting the PAI-1 Mechanism with a Small Peptide Increases the Efficacy of Alteplase in a Rabbit Model of Chronic Empyema" Pharmaceutics 15, no. 5: 1498. https://doi.org/10.3390/pharmaceutics15051498