

Synergistic Combination of Irinotecan and Rapamycin Orally Delivered by Nanoemulsion for Enhancing Therapeutic Efficacy of Pancreatic Cancer
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation of Irinotecan/Rapamycin-Loaded LBSNENP
2.3. Characterization of Irinotecan/Rapamycin-Loaded LBSNENA
2.4. HPLC Instrumentation and Chromatographic Conditions
2.5. Simultaneous Analysis of Irinotecan, SN38, SN38 Glucuronide, and Rapamycin in the Biosample through Ultra-Performance Liquid Chromatography with Tandem Mass Spectrometry
2.6. In Vitro Release of Irinotecan and Rapamycin from LBSNENP
2.7. Cell Viability and Combination Effect Studies
2.8. In Vivo Pharmacokinetic Studies
2.9. Bioanalysis of the Blood Concentrations of Irinotecan, SN-38, SN38G, and Rapamycin
2.10. Tumor Inhibition Studies
2.11. Statistical Analysis
3. Results and Discussion
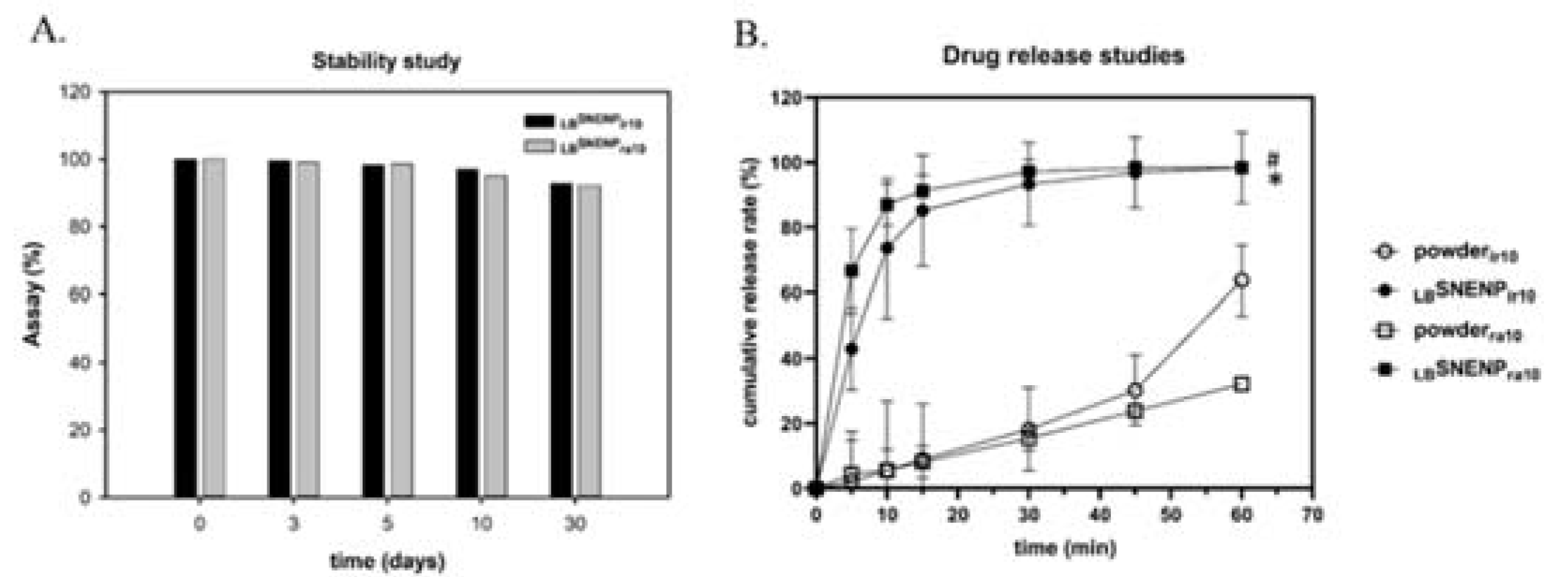
3.1. Characterization of LBSNENA
3.2. In Vitro Release of Irinotecan and Rapamycin from LBSNENP
3.3. Cell Viability and Combination Effect Studies
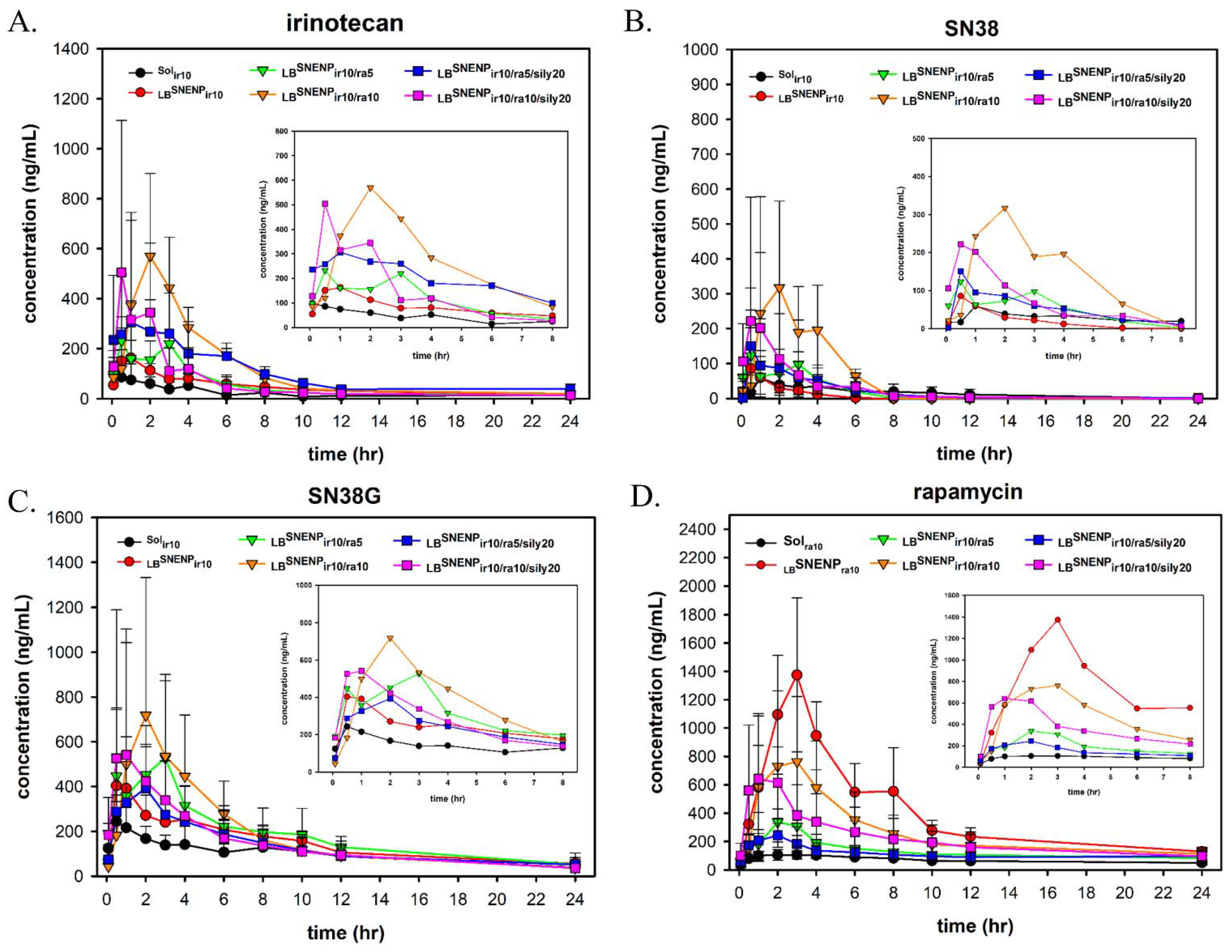
3.4. In Vivo PK studies
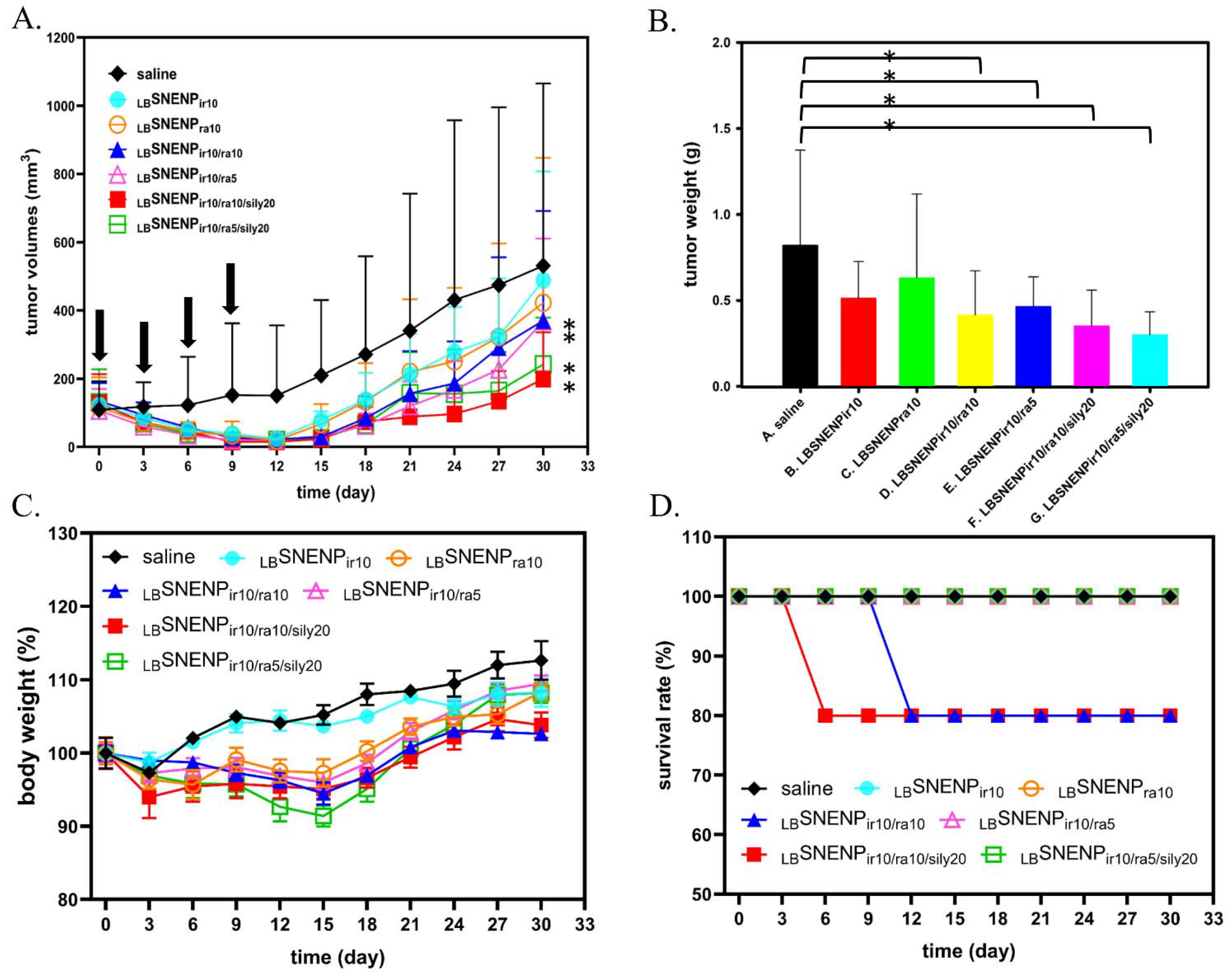
3.5. In Vivo Therapeutic Studies
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillen, S.; Schuster, T.; Meyer Zum Büschenfelde, C.; Friess, H.; Kleeff, J. Preoperative/neoadjuvant therapy in pancreatic cancer: A systematic review and meta-analysis of response and resection percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [Green Version]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.P.; Wu, C.Y.; Yeh, Y.C.; Shyr, Y.M.; Wu, Y.Y.; Kuo, C.Y.; Hung, Y.P.; Chen, M.H.; Lee, W.P.; Luo, J.C.; et al. Erlotinib is effective in pancreatic cancer with epidermal growth factor receptor mutations: A randomized, open-label, prospective trial. Oncotarget 2015, 6, 18162–18173. [Google Scholar] [CrossRef] [Green Version]
- Morran, D.C.; Wu, J.; Jamieson, N.B.; Mrowinska, A.; Kalna, G.; Karim, S.A.; Au, A.Y.; Scarlett, C.J.; Chang, D.K.; Pajak, M.Z.; et al. Targeting mTOR dependency in pancreatic cancer. Gut 2014, 63, 1481–1489. [Google Scholar] [CrossRef] [Green Version]
- Zhong, H.; Chiles, K.; Feldser, D.; Laughner, E.; Hanrahan, C.; Georgescu, M.M.; Simons, J.W.; Semenza, G.L. Modulation of hypoxia-inducible factor 1alpha expression by the epidermal growth factor/phosphatidylinositol 3-kinase/PTEN/AKT/FRAP pathway in human prostate cancer cells: Implications for tumor angiogenesis and therapeutics. Cancer Res. 2000, 60, 1541–1545. [Google Scholar]
- Forsythe, J.A.; Jiang, B.H.; Iyer, N.V.; Agani, F.; Leung, S.W.; Koos, R.D.; Semenza, G.L. Activation of vascular endothelial growth factor gene transcription by hypoxia-inducible factor 1. Mol. Cell Biol. 1996, 16, 4604–4613. [Google Scholar] [CrossRef] [Green Version]
- Büchler, P.; Reber, H.A.; Lavey, R.S.; Tomlinson, J.; Büchler, M.W.; Friess, H.; Hines, O.J. Tumor hypoxia correlates with metastatic tumor growth of pancreatic cancer in an orthotopic murine model. J. Surg. Res. 2004, 120, 295–303. [Google Scholar] [CrossRef]
- Liu, Y.; Feng, M.; Chen, H.; Yang, G.; Qiu, J.; Zhao, F.; Cao, Z.; Luo, W.; Xiao, J.; You, L.; et al. Mechanistic target of rapamycin in the tumor microenvironment and its potential as a therapeutic target for pancreatic cancer. Cancer Lett. 2020, 485, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Vaupel, P. The role of hypoxia-induced factors in tumor progression. Oncologist 2004, 9 (Suppl. 5), 10–17. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Defining the role of hypoxia-inducible factor 1 in cancer biology and therapeutics. Oncogene 2010, 29, 625–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou Khouzam, R.; Brodaczewska, K.; Filipiak, A.; Zeinelabdin, N.A.; Buart, S.; Szczylik, C.; Kieda, C.; Chouaib, S. Tumor Hypoxia Regulates Immune Escape/Invasion: Influence on Angiogenesis and Potential Impact of Hypoxic Biomarkers on Cancer Therapies. Front. Immunol. 2020, 11, 613114. [Google Scholar] [CrossRef]
- Pencreach, E.; Guérin, E.; Nicolet, C.; Lelong-Rebel, I.; Voegeli, A.C.; Oudet, P.; Larsen, A.K.; Gaub, M.P.; Guenot, D. Marked activity of irinotecan and rapamycin combination toward colon cancer cells in vivo and in vitro is mediated through cooperative modulation of the mammalian target of rapamycin/hypoxia-inducible factor-1alpha axis. Clin. Cancer Res. 2009, 15, 1297–1307. [Google Scholar] [CrossRef] [Green Version]
- Forster, R.E.; Tang, Y.; Bowyer, C.; Lloyd, A.W.; Macfarlane, W.; Phillips, G.J.; Lewis, A.L. Development of a combination drug-eluting bead: Towards enhanced efficacy for locoregional tumour therapies. Anticancer Drugs 2012, 23, 355–369. [Google Scholar] [CrossRef]
- Jannier, S.; Kemmel, V.; Sebastia Sancho, C.; Chammas, A.; Sabo, A.N.; Pencreach, E.; Farace, F.; Chenard, M.P.; Lhermitte, B.; Geoerger, B.; et al. SFCE-RAPIRI Phase I Study of Rapamycin Plus Irinotecan: A New Way to Target Intra-Tumor Hypoxia in Pediatric Refractory Cancers. Cancers 2020, 12, 3051. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Takeuchi, O.; Suzuki, Y.; Kitagawa, Y. Mechanisms of metformin’s anti-tumor activity against gemcitabine-resistant pancreatic adenocarcinoma. Int. J. Oncol. 2019, 54, 764–772. [Google Scholar] [CrossRef]
- Veltkamp, S.A.; Thijssen, B.; Garrigue, J.S.; Lambert, G.; Lallemand, F.; Binlich, F.; Huitema, A.D.; Nuijen, B.; Nol, A.; Beijnen, J.H.; et al. A novel self-microemulsifying formulation of paclitaxel for oral administration to patients with advanced cancer. Br. J. Cancer 2006, 95, 729–734. [Google Scholar] [CrossRef]
- Goodin, S. Oral chemotherapeutic agents: Understanding mechanisms of action and drug interactions. Am. J. Health Syst. Pharm. 2007, 64, S15–S24. [Google Scholar] [CrossRef]
- Sparreboom, A.; van Asperen, J.; Mayer, U.; Schinkel, A.H.; Smit, J.W.; Meijer, D.K.; Borst, P.; Nooijen, W.J.; Beijnen, J.H.; van Tellingen, O. Limited oral bioavailability and active epithelial excretion of paclitaxel (Taxol) caused by P-glycoprotein in the intestine. Proc. Natl. Acad. Sci. USA 1997, 94, 2031–2035. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Gursoy, R.N.; Lambert, G.; Benita, S. Enhanced oral absorption of paclitaxel in a novel self-microemulsifying drug delivery system with or without concomitant use of P-glycoprotein inhibitors. Pharm. Res. 2004, 21, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.C.; Cheng, W.J.; Lin, S.Y.; Hung, M.T.; Sheu, M.T.; Lin, H.L.; Hsieh, C.M. CPT11 with P-glycoprotein/CYP 3A4 dual-function inhibitor by self-nanoemulsifying nanoemulsion combined with gastroretentive technology to enhance the oral bioavailability and therapeutic efficacy against pancreatic adenocarcinomas. Drug Deliv. 2021, 28, 2205–2217. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.L.; Chen, L.C.; Cheng, W.T.; Cheng, W.J.; Ho, H.O.; Sheu, M.T. Preparation and Characterization of a Novel Swellable and Floating Gastroretentive Drug Delivery System (sfGRDDS) for Enhanced Oral Bioavailability of Nilotinib. Pharmaceutics 2020, 12, 137. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.M.; Wu, J.Y.; Chen, Y.C.; Su, Y.D.; Ke, W.T.; Ho, H.O.; Sheu, M.T. In situ formation of nanocrystals from a self-microemulsifying drug delivery system to enhance oral bioavailability of fenofibrate. Int. J. Nanomed. 2011, 6, 2445–2457. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.F.; Chen, Y.C.; Ho, H.O.; Huang, W.Y.; Sheu, M.T.; Liu, D.Z. Development and characterization of dilutable self-microemulsifying premicroemulsion systems (SMEPMS) as templates for preparation of nanosized particulates. Int. J. Nanomed. 2013, 8, 3455–3466. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.C.; Chen, Y.C.; Su, C.Y.; Hong, C.S.; Ho, H.O.; Sheu, M.T. Development and characterization of self-assembling lecithin-based mixed polymeric micelles containing quercetin in cancer treatment and an in vivo pharmacokinetic study. Int. J. Nanomed. 2016, 11, 1557–1566. [Google Scholar] [CrossRef] [Green Version]
- Su, C.Y.; Liu, J.J.; Ho, Y.S.; Huang, Y.Y.; Chang, V.H.; Liu, D.Z.; Chen, L.C.; Ho, H.O.; Sheu, M.T. Development and characterization of docetaxel-loaded lecithin-stabilized micellar drug delivery system (L(sb)MDDs) for improving the therapeutic efficacy and reducing systemic toxicity. Eur. J. Pharm. Biopharm. 2018, 123, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Pawarode, A.; Minderman, H.; O’loughlin, K.L.; Greco, W.R.; Baer, M.R. Rapamycin overcomes multidrug resistance (MDR) mediated by P-glycoprotein (Pgp), Multidrug Resistance Protein-1 (MRP-1), Breast Cancer Resistance Protein (BCRP) and Lung Resistance Protein (LRP) and synergizes with substrate drugs in MDR cells. Cancer Res. 2006, 66, 1270. [Google Scholar]
- Si, J.; Zhao, X.; Gao, S.; Huang, D.; Sui, M. Advances in delivery of Irinotecan (CPT-11) active metabolite 7-ethyl-10-hydroxycamptothecin. Int. J. Pharm. 2019, 568, 118499. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Wang, G.; Cao, Y.F.; Hu, C.M.; Yang, K.; Liu, Y.Z.; Zhang, C.Z.; Zhang, W.H.; Zhu, Z.T.; Sun, H.Z.; et al. Everolimus-inhibited multiple isoforms of UDP-glucuronosyltransferases (UGTs). Xenobiotica 2018, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Formulations | Drug | Oil (18%) | Co-Surfactant (24%) | Surfactants (58% SAA) | |||
|---|---|---|---|---|---|---|---|
| Composition | Irinotecan | Rapamycin | Capryol 90 | Propylene glycol | Lecithin | Tween 80 | Cremophor EL |
| LBSNENAbk | - | - | 0.182 g | 0.242 g | 0.198 g | 0.286 g | 0.092 g |
| LBSNENAir10 | 10 mg | - | 0.182 g | 0.242 g | 0.198 g | 0.286 g | 0.092 g |
| LBSNENAra10 | - | 10 mg | 0.182 g | 0.242 g | 0.198 g | 0.286 g | 0.092 g |
| Compounds | Formula | Parent m/z | Daughters m/z | Cone Volt. | Col. Energy |
|---|---|---|---|---|---|
| Irinotecan | C33H38N4O6 | 587.31 | 124.10 | 76 | 34 |
| SN38 | C22H20N2O5 | 393.21 | 349.14 | 70 | 26 |
| SN38G | C28H28N2O11 | 569.20 | 393.17 | 78 | 28 |
| Rapamycin | C51H79NO13 | 931.60 | 864.50 | 35 | 16 |
| Camptothecin | C20H16N2O4 | 349.14 | 305.15 | 52 | 22 |
| Ascomycin | C43H69NO12 | 809.51 | 756.49 | 48 | 22 |
| Dose | 1 g dd H2O | 1 g LBSNENP | ||||||
|---|---|---|---|---|---|---|---|---|
| Solir10 | Solra10 | LBSNENPir10 | LBSNENPra10 | LBSNENPir10/ra5 | LBSNENPir10/ra10 | LBSNENPir10/ra5/sily20 | LBSNENPir10/ra10/sily20 | |
| Irinotecan (mg/kg) | 10 | - | 10 | - | 10 | 10 | 10 | 10 |
| Rapamycin (mg/kg) | - | 10 | - | 10 | 5 | 10 | 5 | 10 |
| Silymarin (mg/kg) | - | - | - | - | - | - | 20 | 20 |
| Groups | |||||||
|---|---|---|---|---|---|---|---|
| Dose | Saline | LBSNENPir10 | LBSNENPra10, | LBSNENPir10/ra5 | LBSNENPir10/ra10 | LBSNENPir10/ra5/sily20 | LBSNENPir10/ra10/sily20 |
| Irinotecan (mg/kg) | - | 10 | - | 10 | 10 | 10 | 10 |
| Rapamycin (mg/kg) | - | - | 10 | 5 | 10 | 5 | 10 |
| Silymarin (mg/kg) | - | - | - | - | - | 20 | 20 |
| Sample | Droplet Size (nm) | PDI | Zeta Potential (mV) |
|---|---|---|---|
| LBSNENAbk | 149.3 ± 2.48 | 0.305 ± 0.043 | −7.32 ± 0.46 |
| LBSNENAir10 | 122.7 ± 1.84 | 0.212 ± 0.011 | −4.14 ± 0.24 |
| LBSNENAra10 | 120.8 ± 2.25 | 0.224 ± 0.010 | −8.20 ± 0.30 |
| Drug | Ratio | CI50 | |
|---|---|---|---|
| 24 h | 48 h | ||
| rapamycin:irinotecan | 0.3:1 | 0.11 | 0.02 |
| 0.5:1 | 0.16 | 0.01 | |
| 1:1 | 0.10 | 0.07 | |
| 2:1 | 0.28 | 0.01 | |
| rapamycin:SN38 | 0.3:1 | 0.20 | 0.01 |
| 0.5:1 | 0.21 | 0.04 | |
| 1:1 | 0.35 | 0.03 | |
| 2:1 | 0.23 | 0.04 | |
| irinotecan:silymarin | 1:1 | 0.69 | 0.01 |
| SN38:silymarin | 2:1 | 1.44 | 0.00 |
| 1:1 | 0.97 | 0.09 | |
| 2:1 | 0.84 | 0.14 | |
| Sol | LBSNENP | |||||
|---|---|---|---|---|---|---|
| Title | ir10 | ir10 | ir10/ra5 | ir10/ra10 | ir10/ra5/sily20 | ir10/ra10/sily20 |
| Cmax (ng/mL) | 106.4 ± 86.6 | 205.3 ± 86.6 | 349.7 ± 257.8 | 606.2 ± 283.6 | 360.1 ± 104.0 | 576.5 ± 497.0 |
| Tmax (h) | 1.2 ± 1.6 | 1.2 ± 0.8 | 2.1 ± 1.2 | 2.0 ± 1.0 | 2.0 ± 1.0 | 1.0 ± 0.9 |
| AUC0→∞ (ng·h/mL) | 553.2 ± 311.9 | 1097.6 ± 369.7 | 1250.7 ± 526.4 | 2747.1 ± 948.7 | 1962.6 ± 1137.9 | 1361.2 ± 744.6 |
| t1/2 (h) | 3.5 ± 1.1 | 2.8 ± 0.6 | 1.9 ± 0.3 | 2.1 ± 0.2 | 2.2 ± 1.1 | 2.2 ± 1.5 |
| FRB (%) | 100.0% | 198.4% | 226.1% | 496.6% | 354.8% | 246.1% |
| Sol | LBSNENP | |||||
|---|---|---|---|---|---|---|
| Title | ir10 | ir10 | ir10/ra5 | ir10/ra10 | ir10/ra5/sily20 | ir10/ra10/sily20 |
| Cmax (ng/mL) | 21.6 ± 3.4 | 141.6 ± 112.0 | 193.4 ± 112.2 | 357.7 ± 284.3 | 161.5 ± 125.0 | 202.0 ± 308.6 |
| Tmax (h) | 1.5 ± 0.7 | 0.8 ± 0.4 | 1.3 ± 1.4 | 1.5 ± 0.7 | 1.4 ± 0.8 | 1.0 ± 0.7 |
| AUC0→∞ (ng·h/mL) | 137.9 ± 99.1 | 209.4 ± 121.9 | 412.1 ± 220.2 | 1136.5 ± 815.9 | 502.6 ± 333.7 | 684.5 ± 553.1 |
| t1/2 (h) | 4.0 ± 2.1 | 1.9 ± 0.6 | 1.1 ± 0.2 | 1.1 ± 0.7 | 2.3 ± 1.6 | 1.2 ± 0.4 |
| FRB (%) | 100.0% | 151.8% | 298.8% | 824.1% | 364.5% | 496.4% |
| CE (%) | 37.3% | 28.5% | 49.3% | 61.9% | 38.3% | 75.2% |
| Sol | LBSNENP | |||||
|---|---|---|---|---|---|---|
| Title | ir10 | ir10 | ir10/ra5 | ir10/ra10 | ir10/ra5/sily20 | ir10/ra10/sily20 |
| Cmax (ng/mL) | 245.1 ± 117.1 | 454.5 ± 302.0 | 708.8 ± 318.5 | 985.7 ± 518.7 | 491.9 ± 204.0 | 789.2 ± 636.1 |
| Tmax (h) | 0.4 ± 0.2 | 0.7 ± 0.4 | 2.3 ± 0.6 | 2.3 ± 1.0 | 2.3 ± 1.3 | 1.2 ± 0.8 |
| AUC0→∞ (ng·h/mL) | 2369.0 ± 652.8 | 3546.7 ± 1014.1 | 3729.3 ± 172.6 | 4359.9 ± 2547.8 | 3262.7 ± 1472.8 | 4058.6 ± 1718.4 |
| t1/2 (h) | 5.2 ± 1.7 | 7.0 ± 2.1 | 5.1 ± 0.8 | 3.0 ± 0.4 | 4.7 ± 1.2 | 3.7 ± 0.7 |
| Sol | LBSNENP | |||||
|---|---|---|---|---|---|---|
| Title | ra10 | ra10 | ir10/ra5 | ir10/ra10 | ir10/ra5/sily20 | ir10/ra10/sily20 |
| Cmax (ng/mL) | 113.6 ± 26.4 | 1185.6 ± 604.2 | 747.4 ± 441.8 | 1107.1 ± 308.0 | 344.4 ± 37.6 | 1140.9 ± 863.7 |
| Tmax (h) | 3.3 ± 2.3 | 2.5 ± 0.7 | 2.3 ± 0.6 | 2.3 ± 1.0 | 1.8 ± 0.4 | 1.5 ± 0.6 |
| AUC0→∞ (ng·h/mL) | 1689.5 ± 176.1 | 7304.0 ± 4835.6 | 4308.2 ± 1970.9 | 6598.2 ± 1092.2 | 2767.6 ± 700.6 | 6499.4 ± 2306.1 |
| t1/2 (h) | 6.1 ± 3.9 | 4.3 ± 0.8 | 6.6 ± 1.9 | 3.4 ± 1.2 | 7.7 ± 4.4 | 4.8 ± 3.2 |
| FRB (%) | 100.0% | 432.3% | 255.0% | 390.5% | 163.8% | 384.7% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-H.; Chen, L.-C.; Cheng, W.-T.; Wei, P.-S.; Hsieh, C.-M.; Sheu, M.-T.; Lin, S.-Y.; Ho, H.-O.; Lin, H.-L. Synergistic Combination of Irinotecan and Rapamycin Orally Delivered by Nanoemulsion for Enhancing Therapeutic Efficacy of Pancreatic Cancer. Pharmaceutics 2023, 15, 473. https://doi.org/10.3390/pharmaceutics15020473
Liu Y-H, Chen L-C, Cheng W-T, Wei P-S, Hsieh C-M, Sheu M-T, Lin S-Y, Ho H-O, Lin H-L. Synergistic Combination of Irinotecan and Rapamycin Orally Delivered by Nanoemulsion for Enhancing Therapeutic Efficacy of Pancreatic Cancer. Pharmaceutics. 2023; 15(2):473. https://doi.org/10.3390/pharmaceutics15020473
Chicago/Turabian StyleLiu, Yu-Hsuan, Ling-Chun Chen, Wen-Ting Cheng, Pu-Sheng Wei, Chien-Ming Hsieh, Ming-Thau Sheu, Shyr-Yi Lin, Hsiu-O Ho, and Hong-Liang Lin. 2023. "Synergistic Combination of Irinotecan and Rapamycin Orally Delivered by Nanoemulsion for Enhancing Therapeutic Efficacy of Pancreatic Cancer" Pharmaceutics 15, no. 2: 473. https://doi.org/10.3390/pharmaceutics15020473