
Genetic Variation in CYP2D6 and SLC22A1 Affects Amlodipine Pharmacokinetics and Safety


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design and Procedures
2.3. Pharmacokinetic Analysis
2.4. Safety
2.5. Genotyping
2.6. Phenotyping and Haplotyping
2.7. Statistical Analysis
3. Results
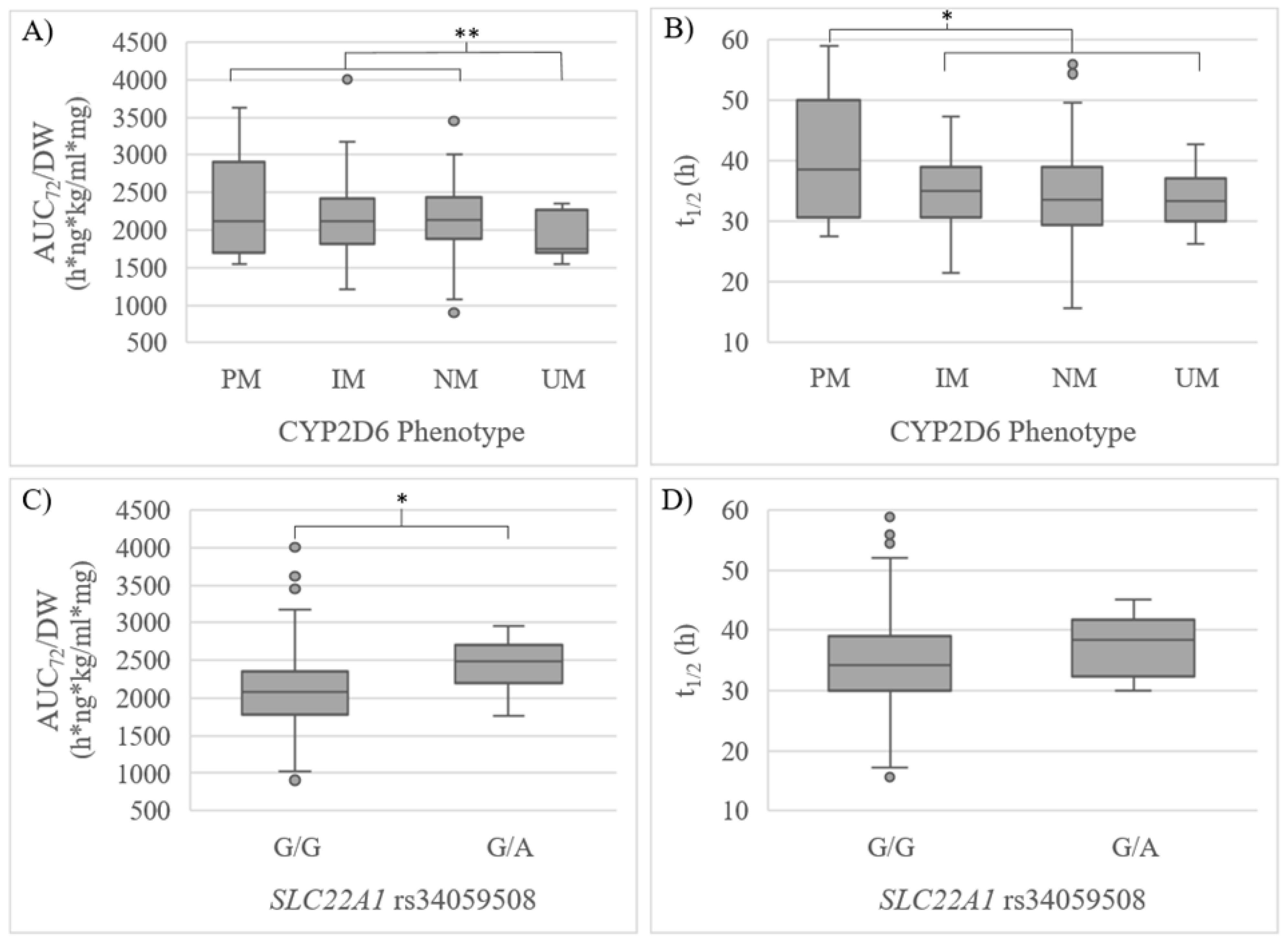
3.1. Pharmacokinetics
3.2. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robles, N.; Macias, J. Hypertension in the Elderly. Cardiovasc. Hematol. Agents Med. Chem. 2015, 12, 136–145. [Google Scholar] [CrossRef]
- Ostchega, Y.; Fryar, C.D.; Nwankwo, T.; Nguyen, D.T. Hypertension Prevalence Among Adults Aged 18 and Over: United States, 2017–2018. NCHS Data Brief. 2020, 364, 1–8. [Google Scholar]
- Jordan, J.; Kurschat, C.; Reuter, H. Arterial Hypertension. Dtsch. Ärztebl. Int. 2018, 115, 557–568. [Google Scholar] [CrossRef]
- Ananchenko, G.; Novakovic, J.; Lewis, J. Amlodipine Besylate. In Profiles of Drug Substances, Excipients and Related Methodology; Elsevier: Amsterdam, The Netherlands, 2012; Volume 37, pp. 31–77. ISBN 978-0-12-397220-0. [Google Scholar]
- Alvarez, J.C.; Mayer-Duverneuil, C.; Cappy, J.; Lorin de la Grandamison, G.; Knapp-Gisclon, A. Postmortem Fatal and Non-Fatal Concentrations of Amlodipine. Forensic Sci. Int. 2020, 316, 110555. [Google Scholar] [CrossRef] [PubMed]
- Meredith, P.A.; Elliott, H.L. Clinical Pharmacokinetics of Amlodipine. Clin. Pharmacokinet. 1992, 22, 22–31. [Google Scholar] [CrossRef] [PubMed]
- FDA Norvasc (Amlodipine Besylate) Label. Highlights of Prescribing Information. 2011. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/019787s047lbl.pdf (accessed on 10 November 2022).
- AEMPS Ficha Técnica AMLODIPINO CINFA 10 Mg Comprimidos EFG. 2022. Available online: https://cima.aemps.es/cima/dochtml/ft/65461/FichaTecnica_65461# (accessed on 20 November 2022).
- Rabah, F.; El-Naggari, M.; Al-Nabhani, D. Amlodipine: The Double Edged Sword: Amlodipine: The Double Edged Sword. J. Paediatr. Child Health 2017, 53, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Park, C.G. Is Amlodipine More Cardioprotective than Other Antihypertensive Drug Classes? Korean J. Intern. Med. 2014, 29, 301–304. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide Trends in Hypertension Prevalence and Progress in Treatment and Control from 1990 to 2019: A Pooled Analysis of 1201 Population-Representative Studies with 104 Million Participants. Lancet Lond. Engl. 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Suárez, C. Single-Pill Telmisartan and Amlodipine: A Rational Combination for the Treatment of Hypertension. Drugs 2011, 71, 2295–2305. [Google Scholar] [CrossRef]
- Zubiaur, P.; Mejía-Abril, G.; Navares-Gómez, M.; Villapalos-García, G.; Soria-Chacartegui, P.; Saiz-Rodríguez, M.; Ochoa, D.; Abad-Santos, F. PriME-PGx: La Princesa University Hospital Multidisciplinary Initiative for the Implementation of Pharmacogenetics. J. Clin. Med. 2021, 10, 3772. [Google Scholar] [CrossRef]
- Vijayananthan, A.; Nawawi, O. The Importance of Good Clinical Practice Guidelines and Its Role in Clinical Trials. Biomed. Imaging Interv. J. 2008, 4, e5. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. Available online: https://jamanetwork.com/journals/jama/fullarticle/1760318 (accessed on 20 November 2022).
- Aguirre, C.; García, M. Evaluación de la causalidad en las comunicaciones de reacciones adversas a medicamentos. Algoritmo del Sistema Español de Farmacovigilancia. Med. Clínica 2016, 147, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Belmonte, C.; Ochoa, D.; Román, M.; Saiz-Rodríguez, M.; Wojnicz, A.; Gómez-Sánchez, C.I.; Martín-Vílchez, S.; Abad-Santos, F. Influence of CYP2D6, CYP3A4, CYP3A5 and ABCB1 Polymorphisms on Pharmacokinetics and Safety of Aripiprazole in Healthy Volunteers. Basic Clin. Pharmacol. Toxicol. 2018, 122, 596–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CeGen-FPGMX Centro Nacional de Genotipado (CeGen-ISCIII). 2022.
- Desta, Z.; Gammal, R.S.; Gong, L.; Whirl-Carrillo, M.; Gaur, A.H.; Sukasem, C.; Hockings, J.; Myers, A.; Swart, M.; Tyndale, R.F.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2B6 and Efavirenz-Containing Antiretroviral Therapy. Clin. Pharmacol. Ther. 2019, 106, 726–733. [Google Scholar] [CrossRef] [Green Version]
- Scott, S.A.; Sangkuhl, K.; Stein, C.M.; Hulot, J.-S.; Mega, J.L.; Roden, D.M.; Klein, T.E.; Sabatine, M.S.; Johnson, J.A.; Shuldiner, A.R. Clinical Pharmacogenetics Implementation Consortium Guidelines for CYP2C19 Genotype and Clopidogrel Therapy: 2013 Update. Clin. Pharmacol. Ther. 2013, 94, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Theken, K.N.; Lee, C.R.; Gong, L.; Caudle, K.E.; Formea, C.M.; Gaedigk, A.; Klein, T.E.; Agúndez, J.A.G.; Grosser, T. Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clin. Pharmacol. Ther. 2020, 108, 191–200. [Google Scholar] [CrossRef]
- Goetz, M.P.; Sangkuhl, K.; Guchelaar, H.-J.; Schwab, M.; Province, M.; Whirl-Carrillo, M.; Symmans, W.F.; McLeod, H.L.; Ratain, M.J.; Zembutsu, H.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and Tamoxifen Therapy. Clin. Pharmacol. Ther. 2018, 103, 770–777. [Google Scholar] [CrossRef] [Green Version]
- DPWG. Annotation of DPWG Guideline for Quetiapine and CYP3A4. 2021. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166265421 (accessed on 1 November 2022).
- Birdwell, K.; Decker, B.; Barbarino, J.; Peterson, J.; Stein, C.; Sadee, W.; Wang, D.; Vinks, A.; He, Y.; Swen, J.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for CYP3A5 Genotype and Tacrolimus Dosing. Clin. Pharmacol. Ther. 2015, 98, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Ramsey, L.B.; Johnson, S.G.; Caudle, K.E.; Haidar, C.E.; Voora, D.; Wilke, R.A.; Maxwell, W.D.; McLeod, H.L.; Krauss, R.M.; Roden, D.M.; et al. The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1 and Simvastatin-Induced Myopathy: 2014 Update. Clin. Pharmacol. Ther. 2014, 96, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Gammal, R.; Court, M.; Haidar, C.; Iwuchukwu, O.; Gaur, A.; Alvarellos, M.; Guillemette, C.; Lennox, J.; Whirl-Carrillo, M.; Brummel, S.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for UGT1A1 and Atazanavir Prescribing. Clin. Pharmacol. Ther. 2016, 99, 363–369. [Google Scholar] [CrossRef]
- Campodónico, D.M.; Zubiaur, P.; Soria-Chacartegui, P.; Casajús, A.; Villapalos-García, G.; Navares-Gómez, M.; Gómez-Fernández, A.; Parra-Garcés, R.; Mejía-Abril, G.; Román, M.; et al. CYP2C8 *3 and *4 Define CYP2C8 Phenotype: An Approach with the Substrate Cinitapride. Clin. Transl. Sci. 2022, 15, 2613–2624. [Google Scholar] [CrossRef]
- Abad-Santos, F.; Novalbos, J.; Gálvez-Múgica, M.-A.; Gallego-Sandín, S.; Almeida, S.; Vallée, F.; García, A.G. Assessment of Sex Differences in Pharmacokinetics and Pharmacodynamics of Amlodipine in a Bioequivalence Study. Pharmacol. Res. 2005, 51, 445–452. [Google Scholar] [CrossRef]
- Ramamoorthy, A.; Pacanowski, M.; Bull, J.; Zhang, L. Racial/Ethnic Differences in Drug Disposition and Response: Review of Recently Approved Drugs. Clin. Pharmacol. Ther. 2015, 97, 263–273. [Google Scholar] [CrossRef]
- Zhou, Y.; Ingelman-Sundberg, M.; Lauschke, V. Worldwide Distribution of Cytochrome P450 Alleles: A Meta-Analysis of Population-Scale Sequencing Projects. Clin. Pharmacol. Ther. 2017, 102, 688–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, S.; Bell, E.C.; Zhang, Y.; Liang, D. Racial Disparity in Drug Disposition in the Digestive Tract. Int. J. Mol. Sci. 2021, 22, 1038. [Google Scholar] [CrossRef]
- Correa, R.; Harsha Tella, S.; Elshimy, G.; Davidson, J.A. The Status of Diabetes and Its Complications in Latin-American Population: A Review Article. Diabetes Res. Clin. Pract. 2020, 168, 108274. [Google Scholar] [CrossRef]
- Gonzalez-Bedat, M.; Rosa-Diez, G.; Pecoits-Filho, R.; Ferreiro, A.; García-García, G.; Cusumano, A.; Fernandez-Cean, J.; Noboa, O.; Douthat, W. Burden of Disease: Prevalence and Incidence of ESRD in Latin America. Clin. Nephrol. 2015, 83, 3–6. [Google Scholar] [CrossRef]
- Molden, E.; Åsberg, A.; Christensen, H. CYP2D6 Is Involved in O-Demethylation of Diltiazem: An In Vitro Study with Transfected Human Liver Cells. Eur. J. Clin. Pharmacol. 2000, 56, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Seeland, U.; Regitz-Zagrosek, V. Sex and Gender Differences in Cardiovascular Drug Therapy. In Sex and Gender Differences in Pharmacology; Regitz-Zagrosek, V., Ed.; Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2013; Volume 214, pp. 211–236. ISBN 978-3-642-30725-6. [Google Scholar]
- Abdoh, A.; Al-Omari, M.M.; Badwan, A.A.; Jaber, A.M.Y. Amlodipine Besylate–Excipients Interaction in Solid Dosage Form. Pharm. Dev. Technol. 2004, 9, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Costache, A.D.; Trawick, D.; Bohl, D.; Sem, D.S. AmineDB: Large Scale Docking of Amines with CYP2D6 and Scoring for Druglike Properties—Towards Defining the Scope of the Chemical Defense against Foreign Amines in Humans. Xenobiotica 2007, 37, 221–245. [Google Scholar] [CrossRef] [PubMed]
- Goswami, S.; Gong, L.; Giacomini, K.; Altman, R.B.; Klein, T.E. PharmGKB Summary: Very Important Pharmacogene Information for SLC22A1. Pharmacogenet. Genom. 2014, 24, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.C.; Khuri, N.; Liang, X.; Stecula, A.; Chien, H.-C.; Yee, S.W.; Huang, Y.; Sali, A.; Giacomini, K.M. Discovery of Competitive and Noncompetitive Ligands of the Organic Cation Transporter 1 (OCT1; SLC22A1). J. Med. Chem. 2017, 60, 2685–2696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saiz-Rodríguez, M.; Almenara, S.; Navares-Gómez, M.; Ochoa, D.; Román, M.; Zubiaur, P.; Koller, D.; Santos, M.; Mejía, G.; Borobia, A.M.; et al. Effect of the Most Relevant CYP3A4 and CYP3A5 Polymorphisms on the Pharmacokinetic Parameters of 10 CYP3A Substrates. Biomedicines 2020, 8, 94. [Google Scholar] [CrossRef]
- Bhatnagar, V.; Garcia, E.P.; O’Connor, D.T.; Brophy, V.H.; Alcaraz, J.; Richard, E.; Bakris, G.L.; Middleton, J.P.; Norris, K.C.; Wright, J.; et al. CYP3A4 and CYP3A5 Polymorphisms and Blood Pressure Response to Amlodipine among African-American Men and Women with Early Hypertensive Renal Disease. Am. J. Nephrol. 2010, 31, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Guo, C.; Pei, Q.; Tan, H.; Huang, Z.; Yuan, H.; Yang, G. Effects of Genetic Factors on the Pharmacokinetics and Pharmacodynamics of Amlodipine in Primary Hypertensive Patients. Biomed. Rep. 2015, 3, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Han, J.M.; Yee, J.; Chung, J.E.; Lee, K.E.; Park, K.; Gwak, H.S. Effects of Cytochrome P450 Oxidoreductase Genotypes on the Pharmacokinetics of Amlodipine in Healthy Korean Subjects. Mol. Genet. Genom. Med. 2020, 8, e1201. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Wen, G.; Lu, Y.; Wen, J.; Ji, Y.; Xing, X.; Li, Y.; Wen, J.; Yuan, H. CYP3A4*1G and CYP3A5*3 Genetic Polymorphisms Alter the Antihypertensive Efficacy of Amlodipine in Patients with Hypertension Following Renal Transplantation. Int J. Clin. Pharmacol. Ther. 2017, 55, 109–118. [Google Scholar] [CrossRef]
- Zuo, X.; Zhang, W.; Yuan, H.; Barrett, J.S.; Hua, Y.; Huang, Z.; Zhou, H.; Pei, Q.; Guo, C.; Wang, J.; et al. ABCB1 Polymorphism and Gender Affect the Pharmacokinetics of Amlodipine in Chinese Patients with Essential Hypertension: A Population Analysis. Drug Metab. Pharmacokinet. 2014, 29, 305–311. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Yung Chan, S.; Cher Goh, B.; Chan, E.; Duan, W.; Huang, M.; McLeod, H.L. Mechanism-Based Inhibition of Cytochrome P450 3A4 by Therapeutic Drugs. Clin. Pharmacokinet. 2005, 44, 279–304. [Google Scholar] [CrossRef]
- Zhou, S.-F. Drugs Behave as Substrates, Inhibitors and Inducers of Human Cytochrome P450 3A4. Curr. Drug Metab. 2008, 9, 310–322. [Google Scholar] [CrossRef]
- Kloner, R.A.; Sowers, J.R.; DiBona, G.F.; Gaffney, M.; Marilee, W. Sex- and Age-Related Antihypertensive Effects of Amlodipine. Am. J. Cardiol. 1996, 77, 713–722. [Google Scholar] [CrossRef]
- Soldin, O.P.; Mattison, D.R. Sex Differences in Pharmacokinetics and Pharmacodynamics. Clin. Pharmacokinet. 2009, 48, 143–157. [Google Scholar] [CrossRef] [Green Version]
- Sung, K.-C.; Oh, Y.-S.; Cha, D.-H.; Hong, S.-J.; Won, K.-H.; Yoo, K.-D.; Rha, S.-W.; Ahn, Y.-K.; Ahn, J.-C.; Jang, J.-Y.; et al. Efficacy and Tolerability of Telmisartan/Amlodipine + Hydrochlorothiazide Versus Telmisartan/Amlodipine Combination Therapy for Essential Hypertension Uncontrolled With Telmisartan/Amlodipine: The Phase III, Multicenter, Randomized, Double-Blind TAHYTI Study. Clin. Ther. 2018, 40, 50–63.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Düsing, R.; Waeber, B.; Destro, M.; Santos Maia, C.; Brunel, P. Triple-Combination Therapy in the Treatment of Hypertension: A Review of the Evidence. J. Hum. Hypertens. 2017, 31, 501–510. [Google Scholar] [CrossRef]
- Salam, A.; Atkins, E.R.; Hsu, B.; Webster, R.; Patel, A.; Rodgers, A. Efficacy and Safety of Triple versus Dual Combination Blood Pressure-Lowering Drug Therapy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Hypertens. 2019, 37, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- McDowell, S.E.; Coleman, J.J.; Ferner, R.E. Systematic Review and Meta-Analysis of Ethnic Differences in Risks of Adverse Reactions to Drugs Used in Cardiovascular Medicine. BMJ 2006, 332, 1177–1181. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Gene | Allele | SNPs Present in the Allele | Gene | Allele | SNPs Present in the Allele |
|---|---|---|---|---|---|
| CYP1A2 | N/A | rs2069514 | CYP2D6 | *3 | rs35742686 |
| N/A | rs762551 | *4 | rs3892097, rs1065852 | ||
| N/A | rs2470890 | *6 | rs5030655 | ||
| CYP2A6 | *9 | rs28399433 | *7 | rs5030867 | |
| CYP2B6 | *4 | rs2279343 | *8 | rs5030865 | |
| *5 | rs3211371 | *9 | rs5030656 | ||
| *6 | rs2279343, rs3745274 | *10 | rs1065852 | ||
| *7 | rs2279343, rs3745274, rs3211371 | *14 | rs5030865 | ||
| *9 | rs3745274 | *17 | rs28371706 | ||
| CYP2C8 | *2 | rs11572103 | *41 | rs28371725 | |
| *3 | rs10509681 | CYP3A4 | *2 | rs55785340 | |
| *4 | rs1058930 | *6 | rs46464389 | ||
| CYP2C9 | *2 | rs1799853 | *20 | rs67666821 | |
| *3 | rs1057910 | *22 | rs35599367 | ||
| CYP2C19 | *2 | rs4244285 | CYP3A5 | *3 | rs776746 |
| *3 | rs4986893 | *6 | rs10264272 | ||
| *4 | rs28399504 | SLC22A1 | N/A | rs12208357 | |
| *17 | rs12248560 | N/A | rs34059508 | ||
| ABCB1 | N/A | rs1045642 (C3435T) | N/A | rs72552763 | |
| N/A | rs2032582 (G2677A/T) | SLCO1B1 | *5 | rs4149056 | |
| N/A | rs1128503 (C1236T) | *15 | rs4149056, rs2306283 | ||
| ABCC2 | N/A | rs2273697 | *37 | rs2306283 | |
| ABCG2 | N/A | rs2231142 | N/A | rs4149015 | |
| UGT1A1 # | *80 | rs887829 |
| N | Age (Years) | Height (m) | Weight (kg) | BMI (kg/m2) | |
|---|---|---|---|---|---|
| Sex | |||||
| Men | 81 | 25.48 (5.06) | 1.77 (0.07) | 77.26 (10.00) | 24.58 (2.76) |
| Women | 79 | 27.79 (8.43) | 1.63 (0.06) * | 61.10 (7.85) * | 23.08 (2.80) * |
| Race | |||||
| Caucasian | 118 | 25.63 (6.00) | 1.71 (0.09) | 69.33 (11.73) | 23.60 (2.92) |
| Latin-American | 36 | 30.19 (9.10) *1 | 1.67 (0.11) | 68.83 (13.43) | 24.56 (2.72) |
| Other # | 6 | 24.67 (4.41) | 1.71 (0.10) | 71.08 (12.68) | 24.14 (2.34) |
| Clinical trial | |||||
| A | 22 | 26.05 (6.44) | 1.70 (0.12) | 66.85 (14.00) | 22.85 (2.88) |
| B | 20 | 23.90 (2.75) | 1.72 (0.09) | 68.37 (10.91) | 23.09 (2.99) |
| C | 4 | 30.00 (8.76) | 1.70 (0.16) | 77.93 (14.58) | 26.85 (2.45) |
| D | 25 | 27.64 (6.78) | 1.67 (0.08) | 65.90 (10.79) | 23.68 (2.84) |
| E | 16 | 25.56 (7.46) | 1.67 (0.09) | 64.73 (10.36) | 23.17 (2.34) |
| F | 31 | 26.81 (8.86) | 1.71 (0.08) | 72.16 (11.12) | 24.57 (2.90) |
| G | 25 | 27.64 (8.04) | 1.72 (0.10) | 71.45 (11.75) | 24.17 (2.54) |
| H | 18 | 27.43 (5.20) | 1.72 (0.12) | 72.29 (14.20) | 24.33 (3.22) |
| Total | 160 | 26.62 (7.01) | 1.70 (0.10) | 62.80 (12.09) | 23.84 (2.87) |
| N | AUC72/DW (h*ng*kg/mL*mg) | Cmax/DW (ng*kg/mL*mg) | tmax (h) | t1/2 (h) | |
|---|---|---|---|---|---|
| Sex | |||||
| Men | 81 | 2121.71 (467.12) | 65.39 (12.52) | 5.96 (1.29) | 35.89 (6.48) |
| Women | 79 | 2127.07 (520.90) | 63.72 (13.44) | 6.53 (1.58) * | 33.87 (6.98) |
| Race | |||||
| Caucasian | 118 | 2088.24 (514.93) | 64.74 (13.25) | 6.09 (1.46) *1 | 34.57 (7.52) |
| Latin-American | 36 | 2225.91 (412.95) | 63.76 (12.00) | 6.72 (1.26) | 35.81 (5.24) |
| Other | 6 | 2225.25 (457.01) | 66.09 (15.02) | 6.42 (2.33) | 35.65 (4.53) |
| Clinical trial | |||||
| A | 22 | 1887.51 (397.95) | 61.52 (12.27) | 6.30 (1.32) | 34.96 (7.83) |
| B | 20 | 2377.38 (619.04) | 71.67 (14.54) | 6.85 (1.18) | 40.19 (6.91) |
| C | 4 | 2223.35 (480.40) | 68.07 (12.55) | 6.25 (0.50) | 37.24 (5.24) |
| D | 25 | 2075.88 (355.09) | 63.62 (11.30) | 6.72 (1.30) | 33.07 (4.83) |
| E | 16 | 2095.49 (327.75) | 61.09 (8.87) | 6.47 (1.26) | 33.26 (5.64) |
| F | 31 | 2397.11 (517.72) | 70.20 (10.85) | 5.94 (1.67) | 35.61 (7.75) |
| G | 25 | 1951.39 (500.31) | 60.35 (15.01) | 5.22 (1.58) *2 | 33.63 (7.83) |
| H | 17 | 1965.30 (397.43) | 59.94 (12.82) | 6.59 (1.25) | 32.79 (4.38) |
| Co-administered drug | |||||
| Atorvastatin | 22 | 1887.51 (397.95) *3 | 61.52 (12.27) | 6.30 (1.32) | 34.96 (7.83) |
| Valsartan | 20 | 2377.38 (619.04) | 71.67 (14.54) | 6.85 (1.18) | 40.19 (6.91) *3 |
| Valsartan + HTZ | 45 | 2095.96 (350.46) | 63.11 (10.54) | 6.59 (1.23) | 33.51 (5.18) |
| Olmesartan + HTZ | 73 | 2143.91 (527.46) | 64.43 (13.62) | 5.84 (1.62) | 34.28 (7.16) |
| Total | 160 | 2124.35 (492.85) | 64.56 (12.97) | 6.24 (1.47) | 34.89 (6.98) |
| Genotype or Phenotype | N | AUC72/DW (h*ng*kg/mL*mg) | Cmax/DW (ng*kg/mL*mg) | tmax (h) | t1/2 (h) |
|---|---|---|---|---|---|
| CYP2D6 | |||||
| UM | 4 | 1971.00 (344.28) | 61.43 (7.83) | 5.63 (1.49) | 35.73 (4.63) |
| NM | 35 | 2106.89 (438.36) | 63.78 (13.11) | 6.19 (1.30) | 34.01 (6.23) |
| IM | 21 | 2166.75 (319.17) | 66.92 (10.74) | 6.12 (1.46) | 36.13 (4.13) |
| PM | 8 | 2307.66 (713.05) | 66.64 (12.15) | 5.94 (1.99) | 40.45 (10.87) *1 |
| SLC22A1 rs34059508 | |||||
| G/G | 66 | 2110.77 (428.73) | 64.38 (11.95) | 6.07 (1.39) | 35.19 (6.51) |
| G/A | 3 | 2638.62 (246.80) *2 | 72.35 (12.85) | 7.17 (2.02) | 40.69 (4.17) |
| CYP3A4 | |||||
| NM | 64 | 2128.17 (448.82) | 64.82 (12.23) | 6.09 (1.39) | 35.23 (6.70) |
| IM | 5 | 2231.76 (260.19) | 63.53 (9.51) | 6.40 (1.85) | 38.00 (2.10) |
| Genotype or Phenotype | N | AUC72/DW (h*ng*kg/mL*mg) | Cmax/DW (ng*kg/mL*mg) | tmax (h) | t1/2 (h) |
|---|---|---|---|---|---|
| CYP2D6 | |||||
| UM | 13 | 1905.21 (291.68) * | 60.59 (7.87) | 5.89 (1.31) | 33.68 (4.62) |
| NM | 87 | 2123.30 (497.73) | 64.41 (13.79) | 6.36 (1.36) | 34.64 (7.54) |
| IM | 48 | 2164.35 (485.10) | 66.08 (12.90) | 6.18 (1.66) | 34.84 (5.56) |
| PM | 8 | 2307.66 (713.05) | 66.64 (12.15) | 5.94 (1.99) | 40.45 (10.87) *1 |
| SLC22A1rs34059508 | |||||
| G/G | 152 | 2111.66 (492.69) | 64.44 (13.02) | 6.20 (1.46) | 34.78 (7.07) |
| G/A | 6 | 2442.42 (391.44) *2 | 69.05 (12.78) | 7.25 (1.75) | 37.63 (5.47) |
| CYP3A4 | |||||
| NM | 144 | 2111.68 (483.74) | 64.51 (13.02) | 6.19 (1.48) | 34.87 (6.98) |
| IM | 14 | 2316.87 (570.00) | 66.35 (13.22) | 6.82 (1.32) | 35.12 (7.69) |
| Variable | Category | N | ADR | Volunteers Affected | Significance |
|---|---|---|---|---|---|
| Sex | Men | 81 | Any ADR | 26 (32.1%) | puv = 0.024, pmv = 0.012, log OR = 2.327 |
| Women | 79 | 40 (50.6%) | |||
| Race | Caucasian | 118 | 41 (34.7%) | puv = 0.006, pmv = 0.031, log OR = 2.306 | |
| Latin-American | 36 | 20 (55.6%) | |||
| Other | 6 | 5 (83.3%) | |||
| Clinical trial | A | 22 | 6 (27.3%) | puv = 0.014 | |
| B | 20 | 3 (15.0%) | |||
| C | 4 | 0 (0.0%) | |||
| D | 25 | 14 (56.0%) | |||
| E | 16 | 7 (43.8%) | |||
| F | 31 | 16 (51.6%) | |||
| G | 25 | 14 (56.0%) | |||
| H | 17 | 6 (35.3%) | |||
| Co-administered drug | Atorvastatin | 22 | 6 (27.3%) | puv = 0.011 | |
| Valsartan | 20 | 3 (15%) | |||
| Valsartan + HTZ | 45 | 21 (46.7%) | |||
| Olmesartan + HTZ | 73 | 36 (49.3%) | |||
| Race | Caucasian | 118 | Headache | 29 (24.6%) | puv = 0.002, pmv = 0.001, log OR = 3.300 |
| Latin-American | 36 | 17 (47.2%) | |||
| Other | 6 | 5 (83.3%) | |||
| SLC22A1 rs34059508 | G/G | 153 | Thoracic pain | 0 (0.0%) | puv = 0.038 |
| G/A | 6 | 1 (16.7%) | |||
| SLC22A1 rs34059508 | G/G | 153 | Dizziness | 7 (4.6%) | puv = 0.038, pmv = 0.014, log OR = 10.975 |
| G/A | 6 | 2 (33.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soria-Chacartegui, P.; Zubiaur, P.; Ochoa, D.; Villapalos-García, G.; Román, M.; Matas, M.; Figueiredo-Tor, L.; Mejía-Abril, G.; Calleja, S.; de Miguel, A.; et al. Genetic Variation in CYP2D6 and SLC22A1 Affects Amlodipine Pharmacokinetics and Safety. Pharmaceutics 2023, 15, 404. https://doi.org/10.3390/pharmaceutics15020404
Soria-Chacartegui P, Zubiaur P, Ochoa D, Villapalos-García G, Román M, Matas M, Figueiredo-Tor L, Mejía-Abril G, Calleja S, de Miguel A, et al. Genetic Variation in CYP2D6 and SLC22A1 Affects Amlodipine Pharmacokinetics and Safety. Pharmaceutics. 2023; 15(2):404. https://doi.org/10.3390/pharmaceutics15020404
Chicago/Turabian StyleSoria-Chacartegui, Paula, Pablo Zubiaur, Dolores Ochoa, Gonzalo Villapalos-García, Manuel Román, Miriam Matas, Laura Figueiredo-Tor, Gina Mejía-Abril, Sofía Calleja, Alejandro de Miguel, and et al. 2023. "Genetic Variation in CYP2D6 and SLC22A1 Affects Amlodipine Pharmacokinetics and Safety" Pharmaceutics 15, no. 2: 404. https://doi.org/10.3390/pharmaceutics15020404